
Abstract
The aging cohort of persons living with human immunodeficiency virus (HIV) in Canada has reached a critical point, with nearly half now 50 years age or older. Older persons living with HIV have specific needs which can be effectively addressed by geriatric specialists. However, the recognition of HIV care as a domain of geriatrics is recent, resulting in a lack of clinical recommendations and modern care models for delivering geriatric care to this population. Virtual care has been demonstrated to reduce existing barriers to accessing HIV care in some populations but before it can be adapted to geriatric HIV care a critical first step is to acknowledge and understand disparities in socioeconomic circumstances, technology access and ability and cultural differences in experiences. This protocol marks the initial step in a comprehensive program of research aimed at co-designing, implementing, and evaluating culturally-appropriate virtual geriatric care for diverse older adults living with HIV. The study employs qualitative methods with older adults living with HIV to lay the groundwork, to inform the future development of a virtual model of geriatric care. We will explore the perspectives of diverse groups of older persons with HIV on (1) The value and necessity of culturally-tailored virtual interventions for geriatric HIV care; and (2) Recommendations on how best to engage older persons with HIV in the future co-design of a virtual model of geriatric HIV care. Ultimately, a more culturally-appropriate approach to care will foster a more inclusive and supportive healthcare system for all individuals affected by HIV including those who are aging. Researchers can utilize this research protocol to employ qualitative co-design and participatory methods with diverse older adults living with HIV.
Keywords
Background
Aging with HIV
Human Immunodeficiency Virus (HIV) is a chronic infection affecting approximately 75,500 Canadians (Medeiros et al., 2023) and 36.7 million people globally (Atuhaire, 2023). Due to advancements in antiretroviral therapy (ART), people with HIV are living longer, leading to a growing population of older adults (i.e.,
Persons aging with HIV often have more comorbidity (Aung et al., 2021; Schank et al., 2021; Zhao et al., 2020), social stigma (Brennan-Ing, 2019; Quinn et al., 2020; Sahoo et al., 2020), frailty (Falutz et al., 2021), and multimorbidity (i.e., the presence of multiple additional health conditions) (Collini & Mawson, 2023; De Francesco et al., 2020; Lorenz et al., 2021). The combination of these conditions adversely affects physical, social, and mental well-being (Balderson et al., 2013; Collini & Mawson, 2023; Fang et al., 2015); despite this, there are several healthcare system barriers to implementing services that help older persons with HIV optimize their health (Baim-Lance et al., 2022; Marshall & Cahill, 2022). Amongst these include the absence of evidence-based geriatric-HIV guidelines (Ballocca et al., 2016; O'Brien et al., 2014), poor access to telehealth and other modalities of virtual care (Baim-Lance et al., 2022), the intersectional stigma of HIV and ageism (Emlet, 2017; Grosso et al., 2023; Sangaramoorthy et al., 2017; Vance & Denham, 2008), intersectional challenges of race and gender identity and epidemiological variations of certain coexisting conditions (Deeks & Phillips, 2009; Mallipattu et al., 2014).
Previously, HIV care was typically managed by primary care (Rai et al., 2019) or infectious disease specialists (Lakshmi et al., 2018). Primary care providers have noted that teleconsultation to specialists improves confidence in caring for HIV (Waldura et al., 2013). As older persons with HIV age, specialized care provided by, or in consultation with, geriatric care specialists, including geriatricians and geriatric clinical nurse specialists) are healthcare professionals who specialize in providing comprehensive medical care and chronic illness management for older adults (Brañas et al., 2019), can address geriatric syndromes commonly present in older persons with HIV (Greene et al., 2015). Geriatric care specialists manage geriatric syndromes, provide comprehensive medication management, optimize quality of life, and promote healthy aging (Kokorelias et al., 2023). Through the development of tailored care plans and interdisciplinary collaboration, they can provide specialized expertise to enhance the overall well-being and outcomes of persons aging with HIV (Guaraldi et al., 2019).
Barriers to Geriatric Health Services
Worldwide, access to geriatric care in the general population is limited (Cheung et al., 2023). For instance, Canada, the study setting, has fewer than 400 certified geriatricians (.004% of physicians) and 1800 geriatric nurses (.0055% of registered nurses) (Krause et al., 2022).
HIV stigma and ageism intersect and compound the challenges accessing HIV-specific geriatric care (Brown & Adeagbo, 2021; Grosso et al., 2023). HIV exceptionalism, defined as HIV care being distinctly unique from the management of other illnesses, may add to stigma surrounding persons aging with HIV seeking geriatric care for other age-related concerns (Burki, 2015). Intersectional demographics (race, sexual orientation, gender identity) and socioeconomic factors influence healthcare access and experiences for persons aging with HIV, and can be further barriers to accessing HIV-geriatric care. These factors may impact adherence to ART and failure to achieve viral suppression (Guaraldi & Rockwood, 2017) and other disparities in healthcare outcomes (Bietsch, 2022; Ecker et al., 2019; Williams et al., 2021). Health disparities among equity-deserving populations such as persons living with HIV have been further exacerbated during the COVID-19 pandemic (Alessi et al., 2023). In our work we will view, equity-deserving populations as older adults with intersecting identities, such as those who are racialized, newly immigrated, Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer or Questioning and additional sexual orientations and gender identities (2SLGBTQIA+), and/or precariously housed (City of Toronto, 2020; Koziel et al., 2021; Milaney et al., 2022). Thus, understanding and addressing these intersectional factors is crucial to ensuring equitable and inclusive healthcare access and improving the experiences of older persons living with HIV.
Virtual Models of Care
Virtual models of geriatric care are becoming increasingly common in the general population, and became more common and necessary during the COVID-19 pandemic (Merchant & Aprahamian, 2022). Virtual geriatric care can encompass various forms of telehealth (e.g., secure messaging) and telemedicine (e.g., video visits), with the terms often used interchangeably (Merchant & Aprahamian, 2022). Virtual care can be delivered synchronously in real-time (e.g., via videoconferencing) or asynchronously (e.g., via email), allowing for information sharing at convenient times (Merchant & Aprahamian, 2022). Virtual geriatric care may be an effective and efficient way to meet the needs of older adults when access to geriatric specialists is limited (Murphy et al., 2020). For example, a 2022 survey of older Canadians found that living in a rural community and being born outside of Canada were factors positively associated with the use of email and secure messaging of health issues. However, older adults with lower income and education levels may face barriers in accessing and utilizing more complex virtual care technologies (Yu & Hagens, 2022). The digital divide, defined as inequities in access and use of information and communication technologies, is more likely to affect older adults who are less likely to adopt new technologies and stop using technology with age (Abbey & Hyde, 2009). Additionally, barriers to digital health literacy, poor access to digital health, poverty, and poor engagement with technology are factors which can contribute to poor health outcomes (Crawford & Serhal, 2020).
Virtual care may help to overcome barriers faced by persons aging with HIV when seeking care, such as limited mobility, time constraints, financial limitations and transportation difficulties, especially for individuals residing in remote or underserviced areas (Lopez et al., 2021). Virtual care may help to reduce fear of judgment or discrimination due to the stigma associated with HIV by allowing individuals to access care and support services remotely in a more private environment (Yelverton et al., 2021). By providing remote access to care, virtual technologies can help overcome these obstacles and enable older adults to engage in HIV care services.
One-Size Doesn’t Fit All
An individualized approach to geriatric-HIV care is essential to adequately address unique healthcare needs and circumstances, such as the complexity of antiretroviral regimens, adherence, underlying comorbidity, mental health and the overriding elements of trauma and stigma (Brown & Adeagbo, 2021; Guaraldi et al., 2019). Despite its many advantages, virtually-delivered healthcare has not been universally beneficial and has worsened health inequality for some equity-deserving individuals (Alverson et al., 2008; Brown & Adeagbo, 2021) due to disparities in digital access and literacy, socioeconomic factors, and the lack of tailored support for certain populations (Baim-Lance et al., 2022; Labisi et al., 2022).
Summary of Preparatory and Pilot Research
This project is rooted in existing patient-oriented research (POR) initiatives within two academic health systems in Toronto, Ontario, Canada. To expand on our POR and fill service gaps identified by patients, this protocol represents the initial phase of a more comprehensive initiative to address the needs of individuals aging with HIV. While an evaluation of our model’s effectiveness is underway, our patient partners have expressed a strong interest in receiving care through virtual means. This research project serves as an initial step in the development of a comprehensive virtual geriatric-HIV program. Focused on co-design elements, the study aims to gather valuable insights and feedback from patient partners to inform the creation of a future virtual care model tailored to meet the psychosocial and medical needs of the geriatric population living with HIV. It is crucial to distinguish this project’s narrower scope, which addresses virtual care, from the broader initiative of enhancing geriatric support through the larger geriatric model.
While geriatric care interventions (e.g., geriatrician consultation, geriatric-focused assessments) are potentially valuable in the care of older persons living with HIV and can improve health outcomes and quality of life (Sangarlangkarn & Appelbaum, 2020), they have low uptake by individuals (Butkus et al., 2020). Investigations into impactful and appropriate models of care for older persons living with HIV are limited. We conducted a systematic synthesis of existing models of geriatric HIV care to identify the key components and inform novel geriatric-HIV models of care within Canada (Kokorelias et al., 2023). Our review found that, while numerous models have been implemented with geriatricians taking on responsibilities ranging from consultation to leadership roles, no model considered the role of culturally-appropriate care. Moreover, none of the existing models were from Canada or delivered care in rural and remote communities (Kokorelias et al., 2023), despite people living in this setting being disproportionately impacted by HIV with increased frailty outcomes, and less treatment uptake and viral suppression (PHAC, 2020). A similar review explored the confidence of geriatricians in managing the care of older persons living with HIV and concluded their lack of comfort in dealing with intersecting identities (Jones & Barber, 2022). Thus, a critical step in reducing disparities in HIV-geriatric care is to understand intersectional differences in healthcare experiences. To elevate the perspectives of equity-deserving communities and gain a comprehensive understanding of their healthcare experiences and desires we will apply community-based research methods that engage community members as active participants in the research process.
Given the limited availability of dedicated virtual geriatric-HIV care models in Canada, despite the increasing aging HIV population and their distinct healthcare requirements, there’s an urgent demand to establish specialized virtual geriatric care models suited to this demographic’s specific needs.
This protocol outlines a participatory action research approach to create a more inclusive and comprehensive virtual care response for aging individuals with HIV, emphasizing the significance of incorporating their voices and perspectives into healthcare service development. Through a community-based approach, we aim to ensure that our services are aligned with the needs and preferences of those using them. By integrating virtual care and expanding the scope of geriatric services to meet the needs of those with lived experiences, we aim to enhance accessibility, reach, and quality of care for individuals aging with HIV, ultimately improving their overall health outcomes and well-being.
Positionality
The research team comprises Canadian researchers with experience in the study of HIV, and members with experience in equity-informed health care, health service research, and implementation science. Members include PhD-trained researchers, clinicians (physicians in geriatrics, family medicine and infectious diseases; occupational therapists; social workers), trainees (PhD and medical students), health service administrators and peer-researchers with lived experience. We have individuals in our team from various gender identities, sexual orientations, racial and ethnic backgrounds, and other dimensions of diversity.
Methods
Study Design
We aim to co-design and obtain foundational knowledge from older persons living with HIV to inform a culturally-appropriate virtual model of geriatric-HIV care. This study will use an Experience-Based Co-Design (EBCD) approach (Fox et al., 2022; Mulvale et al., 2016; Tran & Woo, 2022). EBCD is often used in health service research as a means to develop or enhance health services to improve the overall experiences of patients and their families by meaningfully engaging them in all aspects of improving healthcare services (Robert, 2013). In turn, EBCD approaches are an actionable way of ensuring services better meet the needs of end-users (Dimopoulos-Bick et al., 2018; Donetto et al., 2015; Robert, 2013). EBCD has been increasingly used to improve the services provided to individuals living with HIV (Eaton et al., 2022; Marent et al., 2018; Nixon et al., 2023), as well as older adults living with complex care needs (Lawless et al., 2022). By employing an EBCD approach, we aim to gain valuable insights that will inform the development of a new virtual geriatric-HIV model of care. Involving older persons with HIV in the design process ensures both model relevance and credibility, addressing their needs and preferences for a patient-centered approach (Goodrich, 2018).
Theoretical and Conceptual Frameworks
To guide to our co-design approach, the proposed study will adopt data collection suggestions for Experience-Based Co-Design Stages and Methods by Mulvale and colleagues (Mulvale et al., 2016). Our study will also be theoretically guided by intersectionality frameworks (Bauer et al., 2021; Museus & Griffin, 2011) and the Knowledge to Action Framework (KTA) such that we can shift our research knowledge into action and facilitate evidence uptake by health service administrators, healthcare professionals, and other stakeholders (Field et al., 2014; Graham et al., 2006). The framework is highly suitable for this objective because it encompasses two interconnected aspects of research that impact each other: knowledge creation (involving knowledge generation through research activities) and the action cycle (involving knowledge customization to meet the requirements of different audiences) (Field et al., 2014; Graham et al., 2006). Lastly, the Culturally-Competent Research Criteria for Methodological Areas (CCRCMA) guidelines will provide methodological guidance on the recruitment and retention of participants, measurement procedures, and dissemination of research findings (Casado et al., 2012).
Formation of a Community-Based Advisory Team
A community-based advisory team has been convened prior to the protocol development, such that they are engaged throughout the entire project. The advisory team consists of knowledge users (i.e., three administrators from non-profit community-based organization that deliver support to older persons with HIV [shelters, healthcare organizations, charity organizations, community centers], two older persons with HIV, and five clinicians working with older persons with HIV), policy-makers, and researcher team members. All team members will actively collaborate throughout the research process and be involved in key decision-making regarding the methodology. They will also play a significant role in data collection, analysis, and disseminating research findings. Members of the advisory team will meet with the principal investigators individually throughout the process to discuss their preferences for meetings and involvement, and to ensure flexible, yet meaningful engagement. By ensuring meaningful representation in the formation of our advisory team based on occupation, gender, and race, the panel can provide insights that reflect the diversity of perspectives and needs within the community and help to ensure participant involvement is not merely tokenistic or fragmented (Farrington, 2016; Smith & Dransfield, 2019).
Study Population
We will include older persons with HIV who meet specific eligibility criteria. Participants will be external to our advisory committee. To participate in the study, individuals must self-identify as HIV-positive, be 50 years of age or older, and reside in Ontario. This geographic specificity allows for a more targeted examination of the healthcare resources, available to older persons with HIV in these particular regions and is more likely to inform virtual care delivery that is specific to the researchers’ respective context. We will purposively seek as much as possible representation in the following areas to ensure diversity in perspectives: (a) sex and gender; (b) age; (c) ethnicity and race; (d) socioeconomic status; (e) prior usage of virtual geriatric care (yes or no); (f) geographical location – rural versus urban; (g) duration of time living with HIV; (h) non-English first language; and (i) level of educational attainment. We acknowledge that despite our best efforts, challenges such as resource constraints, participant availability, and category criteria may limit full coverage of each category. Nonetheless, we aim for diverse perspectives in this foundational study to inform broader research and gain insights into varied population complexities and needs.
Recruitment
To achieve a more comprehensive understanding of the research topic and to explore various lived experiences, we will use quota sampling (Moser, 1952) in conjunction with purposive sampling to ensure a more diverse sample representation, as to incorporate diverse voices and experiences. Purposive sampling involves actively seeking out and selecting participants who represent a range of diverse backgrounds and perspectives relevant to the research objectives (Suri, 2011). For our study, we will investigate intersectionality by actively seeking participation from individuals who identify with overlapping identities (e.g., racialized and low socioeconomic status) (Goldberg, 2008). Our advisory team will conduct community outreach at relevant community meetings and events to assist with recruitment and will recruit within their own networks and organizations. We are also conducting targeted recruitment through flyers at culturally diverse settings such as community-based organizations, religious institutions, and culturally-oriented events to ensure the inclusion of diverse populations (Casado et al., 2012). Additionally, we will utilize our advisory teams’ websites and social media platforms to promote the study, and continue to actively reach out to various gerontological and HIV organizations, including HIV clinics, geriatric clinics, and other healthcare facilities that serve older persons with HIV to reach potential participants who are already engaged in healthcare services in Ontario.
Phase 1
We anticipate recruiting 12–15 participants in phase one, but are prepared to conduct additional interviews beyond this if additional insights are needed to address the research objectives effectively (Fusch & Ness, 2015). This sample size is consistent with previous EBCD studies (Macdonald et al., 2023). The chosen sample size in this co-design study is based on the principle of data saturation, ensuring that a sufficiently diverse and representative group of participants is included to reach a point where new insights or design suggestions become redundant and additional participants are unlikely to contribute substantially to the findings (Braun & Clarke, 2021; Fusch & Ness, 2015).
Phase 2–3
We anticipate recruiting a maximum of 25 participants per phase, as consistent with existing co-design workshops in the context of HIV (Maestre et al., 2023). We will first give priority to participants who are already enrolled in Phase I of the study before recruiting additional individuals to reach 5 participants per workshop.
Data Collection
Data collection will happen in three described phases (see Figure 1). EBCD approach to Co-design.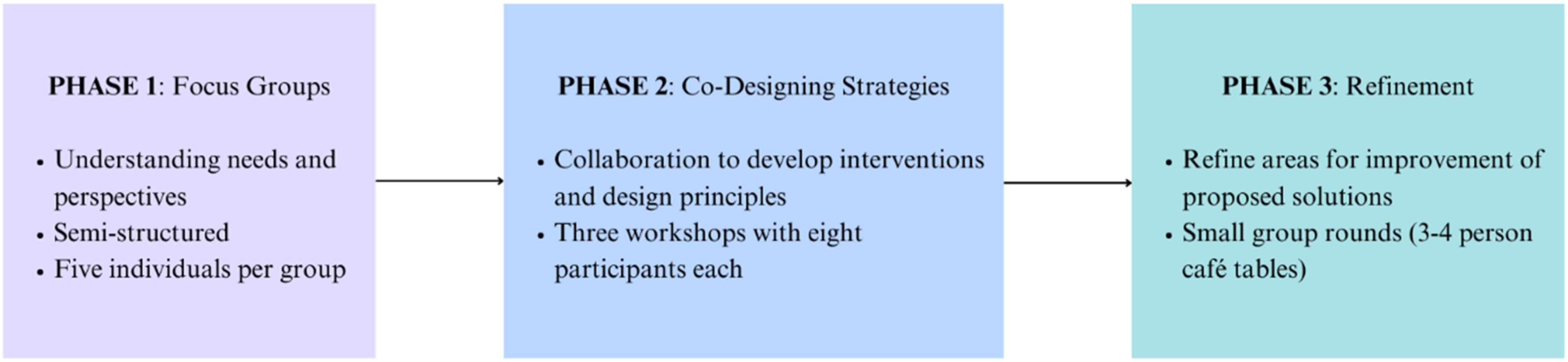
Phase 1: Focus Groups
The initial phase of ECBD focuses on understanding participants' needs and perspectives (Mulvale et al., 2016). We will use a qualitative descriptive approach (Sandelowski, 2000) to conduct semi-structured focus groups to capture feelings and experiences that participants have had at critical points during their healthcare journey. During this phase, we aim to gain a better understanding of experiences across the illness trajectory, as well as during transitions between care settings and different providers. Focus groups will be facilitated using a semi-structured discussion guide and involve approximately five individuals, for a total of approximately five focus groups. However, if individuals are interested in participating in phase one, but uncomfortable participating in a focus group, they can choose to conduct a one-on-one interview. Trained advisory team members will co-facilitate the focus groups/interviews with a member of the research team and contribute to developing the discussion guide that will ask participants to describe: (a) previous experiences providing, receiving, or facilitating care; (b) what their experience was like across the disease trajectory; (c) what their needs are related to receiving care and how they best desire these needs being met by geriatric care specialists; and (d) the priorities for virtual care and the implications for the development of virtual geriatric care for HIV populations. Following each focus group/interview, participants will also note if they wish to participate in phase two of data collection.
Participants will also be able to complete a demographic questionnaire noting various categories of self-identified lived experience, and perceived socioeconomic status. This questionnaire will be utilized to describe participants, contextualize interview/focus group findings, and inform targeted recruitment efforts to include individuals not captured in the study, so that their voices are represented in this work.
Within two days of each focus group/interview, the research assistant and facilitator will send a summary of the data collection event to the research team to help inform the planning of Phase 2.
Phase 2: Co-Designing Strategies (Dream and Design)
In the EBCD process, the next phase will be co-design events where participants collaborate to develop interventions and establish design principles for broader applications (Mulvale et al., 2016). Phase two of data collection will invite participants to take part in co-design workshops to design strategies to improve the existing geriatric care models and create an improved virtual care model that considers culturally appropriate care. This will be theoretically driven by a modified 3-D cycle of Appreciative Inquiry (Trajkovski et al., 2013; Van Wyk, 2015). The 3-D cycle of Appreciative Inquiry was selected as it is a strengths-based approach that focuses on leveraging and amplifying positive aspects of health care to foster growth, engagement, and sustainable change (Trajkovski et al., 2013).
Workshops will be half-day long (∼4 hours) and occur in-person and/or virtually, depending on the needs of participants. This will ensure that homebound participants are able to participate, as well as those with mobility concerns by minimizing the need for travel. Priority will be given to participants who participated in Phase 1, and we will also recruit additional individuals to allow for flexible participation. The number of workshops hosted will depend on the number of participants. We anticipate hosting a maximum of three workshops with ∼eight participants per workshop.
In this stage, participants will be asked to identify the existing strengths, positive experiences, and successful practices of existing geriatric-HIV care to gather stories and examples of excellence. Building on the discoveries made in the first stage, participants envision and articulate a desired future of geriatric-HIV care. Participants will be asked to collaboratively participate in the development of a novel model of care, including the identification of elements such as: modality (e.g., telephone, video), frequency (e.g., how often care should take place), and provider involvement (e.g., who needs to support different elements). Various methods will be used during this phase, including the “path of expression” method, whereby participants will be asked to visualize their ideal service experiences, express them to the group, and generate solutions to make the idealized experiences a reality (Mulvale et al., 2016). Other methods include open-group and small group discussions recorded on flipcharts or worksheets and utilizing visual tools such as concept mapping, mind mapping, or affinity diagrams to visually represent ideas, concepts, and relationships (Mulvale et al., 2016). Following each workshop, the research team will convene to discuss and reflect the lessons learned and recommendations. Members of the research team will meet with the advisory team during a separate meeting to share insights, and discuss logical solutions to any significant issues or challenges encountered. These meetings will inform subsequent workshops.
Phase 3: Refinement (Design)
In this stage, participants will be asked to design and plan the actions and initiatives needed to realize the envisioned future for virtual geriatric-HIV care. Participants from Phase 2 will be invited for Phase 3, but no new participants will be recruited. During this phase, the goal is to further develop and implement design principles to explore how the novel virtual care model and design principles can be implemented effectively (Mulvale et al., 2016). The focus of this stage is to continually improve the understanding of the ideal model of virtual geriatric-HIV care.
First, participants will be briefed on the proceedings of Phase 2 by a member of the research team and asked to comment further to ensure key ideas are captured. Next, participants will partake in a World Café, where participants partake in small-group rounds known as café tables with one question per round, allowing for dynamic conversations and interactions by promoting the cross-pollination of ideas as participants bring their diverse experiences and knowledge to the discussions (Fortin et al., 2019; Mulvale et al., 2016). Participants will partake in 3–4 in-person café tables, each with materials and information about the proposed solutions from Phase 2 (Banfield et al., 2022; Moran et al., 2023). As participants move across group discussions, they will explore what they like and dislike about the proposed solutions, areas for improvement, and what the program is missing (Fortin et al., 2019). Participants will also be asked to consider barriers and facilitators to implementation and uptake. During the last hour of the workshop, groups will present an overview of their discussions and elements of various models of care will be discussed to create unified set of recommendations for virtual geriatric-HIV care.
The co-design workshops will be led by a member of the advisory team with lived experience who will be trained how to facilitate co-design workshops and will be supported by a neutral, professional facilitator (i.e., consultant). Facilitators will encourage participants to actively listen, contribute their unique insights, and build upon the ideas shared by others. As such, the exact activities of the co-design workshops may change in order to meaningfully engage participants, and in turn, generate meaningful data (Mulvale et al., 2016). Certain members of the research team will be present during the workshops to provide support in secretarial and logistical duties. These responsibilities may include tasks such as probing participants for further insights or clarification and taking detailed notes of the discussions and activities. Research team members will be selected based on the recommendations of the advisory team and involve individuals trained in trauma-informed care and equity.
Data Analysis
All focus groups, interviews and workshops will be audio-recorded and professionally transcribed. As such, data will consist of audio-recordings, transcript, field notes, meeting notes as well as physical artifacts designed by participants.
The analysis team will involve the research team and self-selected members of the advisory committee. Data will be analyzed through a thematic content analysis (Anderson, 2007).
Phase 1
Data analysis and collection will occur concurrently, with the analysis team fully immersed in the dataset. As transcripts are produced, each team member will assign colors to text segments conveying similar concepts, forming distinct codes. A codebook will be developed based on team discussions and integration of inductive and deductive codes (informed by the KTA framework). A research assistant will apply the codebook to transcripts using NVivo software, with regular meetings with principal investigators (Maher et al., 2018). Coded data will be shared among the team, who will identify themes through individual comparisons and refine them through team meetings (Anderson, 2007; Braun & Clarke, 2006). The analysis team will engage the research and advisory team for input, and participant perspectives will be compared across different identities. A thematic map will aid in examining code-theme relationships, iteratively refining until consensus on final themes is reached. The research team will capture compelling and actionable ideas to inform Phase 2.
Phase 2 and Phase 3
As co-design also typically utilizes reflexive thematic content analyses to identify, analyze, and report patterns within the data, including artifacts and field notes (Braun & Clarke, 2019), the process used for Phase 1 will be used for Phase 2 and Phase 3. We will modify the thematic analysis approach to consolidate and present the data gathered from each series of workshops. The findings from the Phase 2 workshop will be shared in Phase 3.
Ethics
This study acknowledges risks tied to sensitive healthcare topics like aging and HIV, addressing them via thorough consent discussions and flexible participation (e.g., offering 1:1 interviews and withdrawal options). Emotional well-being will be prioritized, utilizing relationship building, an advisory member with shared experiences, and trained clinicians available to provide trauma-informed support. Data confidentiality will be maintained through restricted access, de-identified transcription, encrypted data sharing, and pseudonyms. Participants will also be equitably compensated in accordance with co-produced guidance for patient engagement (SPOREA, 2022). Lastly, while our research team possesses extensive experience in various aspects related to people aging with HIV, the use of an advisory panel throughout the entire research process, will prioritize creating a supportive and respectful research environment that considers the physical, cognitive, emotional, and social aspects of participants and community partners. This study has been submitted to a research ethics board and all participants will be required to sign an informed consent form.
Rigor
We will employ rigorous data collection and analysis methods, including audio recording, verbatim transcription, and the use of peer-researchers to ensure the accuracy and credibility of the data. The research process will also involve analytical insights to guide further data collection and purposeful sampling (Charmaz & Thornberg, 2021). By including diverse perspectives and experiences, we will also enhance the transferability of our findings (Slevin & Sines, 1999). Credibility will be ensured by aligning the interpretation of the data with the participant experiences in their own words through direct quotes (Charmaz & Thornberg, 2021). Multiple analysts will be involved, bringing varied perspectives to our analysis and reducing the risk of bias associated with analysis based on single individuals. We will leverage our advisory committee to ensure that our interpretations and findings with larger groups, institutions, and individual lives (Charmaz & Thornberg, 2021). Lastly, we will actively engage in reflexivity throughout the research process by reflecting on our positionality/subjectivities and critically examining our own biases, assumptions, and preconceptions in order to enhance the transparency of our work (Clancy, 2013).
Conclusion
This research protocol is the initial step in addressing unique aging and HIV-related care needs for older Canadians, particularly through virtual geriatric care. By engaging with older adults from diverse backgrounds and employing qualitative methods, the research seeks to understand the value and necessity of tailored HIV virtual-care interventions for geriatric care. This research protocol represents the initial step in a comprehensive program of research aimed at co-designing, implementing, and evaluating equity-informed virtual geriatric care for diverse older persons living with HIV in Ontario, Canada. The findings will offer methodological guidance for future researchers interested in co-designing health services, ultimately improving the quality of care and well-being of individuals aging with HIV. Findings from this foundational work will be disseminated in academic journals, conferences and through public workshops and lectures.
Footnotes
Acknowledgements
The authors acknowledge the insights of their advisory committee members who are key decision-making partners in our project and will be integral to the success of this project, for sharing their invaluable opinions and knowledge.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the AGE-WELL Network of Centres of Excellent (NCE) (AW-CAT-2023-03) Inc and the Canadian Frailty Network’s (CFN) Catalyst Funding Program in Healthy Aging. The AGE-WELL NCE and CFN are funded by the Government of Canada through the Networks of Centres of Excellence program.