
Abstract
Conducting community-based participatory research (CBPR) is a complex endeavor, particularly when training non-academic community members. Though examples of CBPR training programs and protocols have been published, they often address a limited set of concepts and are tailored for university or medical school students. Here, we describe the process of developing an online CBPR training program for American Indian (United States) and Indigenous (Canada) community members to conduct multi-sited ethnographic dementia research. This program is unique in its breadth and depth, as our program covers CBPR theory, methods, practical research, and administrative skills. Significantly, this program centers Indigenous methodology, pedagogy, and processes such as two-eyed seeing, storywork, and decolonization approaches. Key to this training program is a “second-generation” approach which incorporates experiential knowledge from a prior community-based researcher and academic partners and is designed to develop CBPR capacity among community-based researchers and partnering communities. In this paper, we detail the experience of the first cohort of learners and subsequent improvement of the training materials. Unique challenges related to the specific research focus (dementia), population/setting (American Indian/First Nations communities), and technology (rural digital infrastructure) are also discussed.
Keywords
Introduction
Health research increasingly recognizes the unique contribution of community-based participatory research (CBPR), particularly in the study of health (in)equity and disparities. Key principles of CBPR as outlined by Israel et al. (1998) include: (1) recognizing the community as a unit of identity; (2) building on strengths and resources in the community; (3) facilitating collaborative partnerships in all phases of the research; (4) integrating knowledge and action for mutual benefit of all partners; (5) promoting a co-learning and empowering process that attends to social inequalities; (6) creating a cyclical and iterative process; (7) addressing health from both positive and ecological perspectives; and (8) disseminating findings and knowledge gained to all partners (Israel et al., 1998). A central feature of CBPR is the collaborative approach between community and academic research partners in conceptualizing, implementing, interpreting, and communicating research that is important to participating communities (Unertl et al., 2016). When working with American Indian and First Nations communities (hereafter referred to as “Indigenous” 1 ), additional ethical considerations must be incorporated, such as: (1) acknowledging historical experience with research and working to overcome the negative image of research; (2) recognizing Tribal sovereignty; (3) differentiating between Tribal and community membership; (4) understanding Tribal diversity and its implications; (5) planning for extended timelines; (6) recognizing key gatekeepers; (7) preparing for leadership turnover; (8) interpreting data within the cultural context; and (9) utilizing Indigenous ways of knowing (Laveaux & Christopher, 2009; Petrucka et al., 2012). These processes are strengthened with a “two-eyed seeing” approach, a concept introduced by Mi’kmaw Elders Albert and Muraena Marshall, which acknowledges the myriad ways of understanding the world (Martin, 2012). Two-eyed seeing and CBPR work in tandem to create an “ethical space” whereby researchers can “see with one eye the strengths of Indigenous ways of knowing and with the other eye the strengths of Euro-Western ways of knowing,” ultimately using both perspectives together (Vukic et al., 2012, p. 148). In this space, academic research partners must acknowledge their own limitations, address power dynamics (Belone et al., 2016), engage partner communities with humility, and understand the importance of place and knowledge tied to the land. Additionally, acknowledging the legacy of colonial policies, unethical research practices, and the resulting impacts on Indigenous peoples’ health and wellbeing is imperative. Decolonizing the research process and supporting data sovereignty and governance can help to address these concerns (Darroch & Giles, 2015; Tsosie, 2019).
Embedded within these principles are cyclical, iterative processes between academic and community partners that shift health research from being conducted on populations to being conducted with and/or by partner populations (Koster et al., 2012). Creating meaningful long term research partnerships involves open communication, working closely with Tribal and Indigenous partners, and community involvement and control over all aspects of the research process (Jacklin & Kinoshameg, 2008). Any research project must reflect community needs and uphold and respect cultural knowledge and ways of knowing.
To help address these considerations, we involve local community researchers in all aspects of research, from community engagement and outreach, data collection, analysis, and dissemination activities for various audiences. As insiders to their community, the community researchers are able to provide a deeper contextual lens to the research (Innes, 2009). Their understanding of community protocols and expectations are vital to the development of long-term research partnerships, as the community researcher often acts as a liaison between the community and research team. Simultaneously, being a part of a large research project with academic partners also brings a level of complexity to the insider/outsider role (Innes, 2009; Kerstetter, 2012; Pelzang & Hutchinson, 2018) since the university, as an institution, may be viewed with mistrust due to past unethical policies and research practices (Lee & Ahtone, 2020; Spier & Skoog, 1974). To support newly hired community researchers, our research team developed a CBPR training program that incorporates lessons and teachings from academic and community researchers (Chino & DeBruyn, 2006) in an effort to enhance research capacity at the community level.
This paper outlines the development of what we describe as a “second-generation” CBPR training program created for a multi-sited ethnographic research study titled ICARE (Indigenous Cultural Understandings of Alzheimer’s Disease and Related Dementias – Research and Engagement). We define second-generation CBPR training as a structured research training which incorporates experiential knowledge from prior community-based researchers and academic partners, that is designed to develop capacity among community-based researchers in order to implement research studies in their communities using a CBPR framework. ICARE partner sites include Tribal Nations in Minnesota, Wisconsin (United States) and First Nations in Ontario (Canada). We outline lessons learned to inform CBPR training for other university or community researchers. We highlight unique training needs that arise when researchers are members of participating communities. We also describe how this CBPR training attempts to build research capacity within Indigenous communities to help shift power differentials within research collaborations and build research capacity and infrastructure outside of the academy. Finally, we identify CBPR training issues that are specific to Alzheimer’s disease and related dementias (ADRD) research.
Methods
The Research Project and Sites
This CBPR training was developed for the ICARE project (NIH 5R56-AG62307-2) which is a qualitative, ethnographic exploration of the impact of ADRD in Indigenous communities across four research sites in the United States and Canada (Figure 1). Our research stance prioritizes a sustainable engagement model using CBPR approaches to establish community advisory councils and hire and train local community-based researchers at each site (Battaglia et al., 2019; Key et al., 2019). Community-based researchers do not require a background in research but are hired for their expertise and knowledge of their community. For this project we hired five new local, Indigenous community researchers in Minnesota, Wisconsin, and Ontario, and retained one community-based researcher (KP) from Ontario with over 15 years of experience working with the investigators (KJ and WW). Map of ICARE partner communities and research sites.
Ethical Considerations
We are describing the development of a CBPR training program with community-based researchers who were hired through the project, which took place prior to participant data collection, so ethical approval/informed consent was not sought. However, the ICARE project received ethics approval from the University of Minnesota (00013626), Manitoulin Anishinaabek Research Review Committee (2019-09), and Tribal Council Resolutions from partner sites.
Developing a Second-Generation CBPR Training Program
This second-generation CBPR training is a structured research training which incorporates experiential knowledge from prior community-based researchers and academic partners (Figure 2). Experiential knowledge is integral to this process and was informed and shaped (detailed more specifically below) by multiple authors. For instance, author KP is Anishinaabe Kwe from Wiikwemkoong Unceded Territory, Ontario, Canada, and has over 15 years of community-based researcher experience in addition to over 25 years of nursing experience. Author MB is Cree from George Gordon First Nation in Saskatchewan, holds a PhD in American Indian Studies, and has worked on CBPR-focused projects for over 10 years. KJ and WW are academic researchers in the area of Indigenous health and have over 50 years of combined experience. It is from these places of experience and knowledge that the CBPR training program was assembled. An overview of the development and implementation of a second-generation CBPR training program.
For this research project, we developed the content to support qualitative data collection for an ethnographic study of Indigenous cultural understandings of ADRD. The training incorporates Indigenous pedagogy through storytelling as an Indigenous educational theoretical model, understanding community culture and context, lessons learned, and past research experiences. The research team met on several occasions to refine the content, timing, and approach for the training.
Summary of CBPR Training Modules, Learning Objectives, Exercises, and Examples.
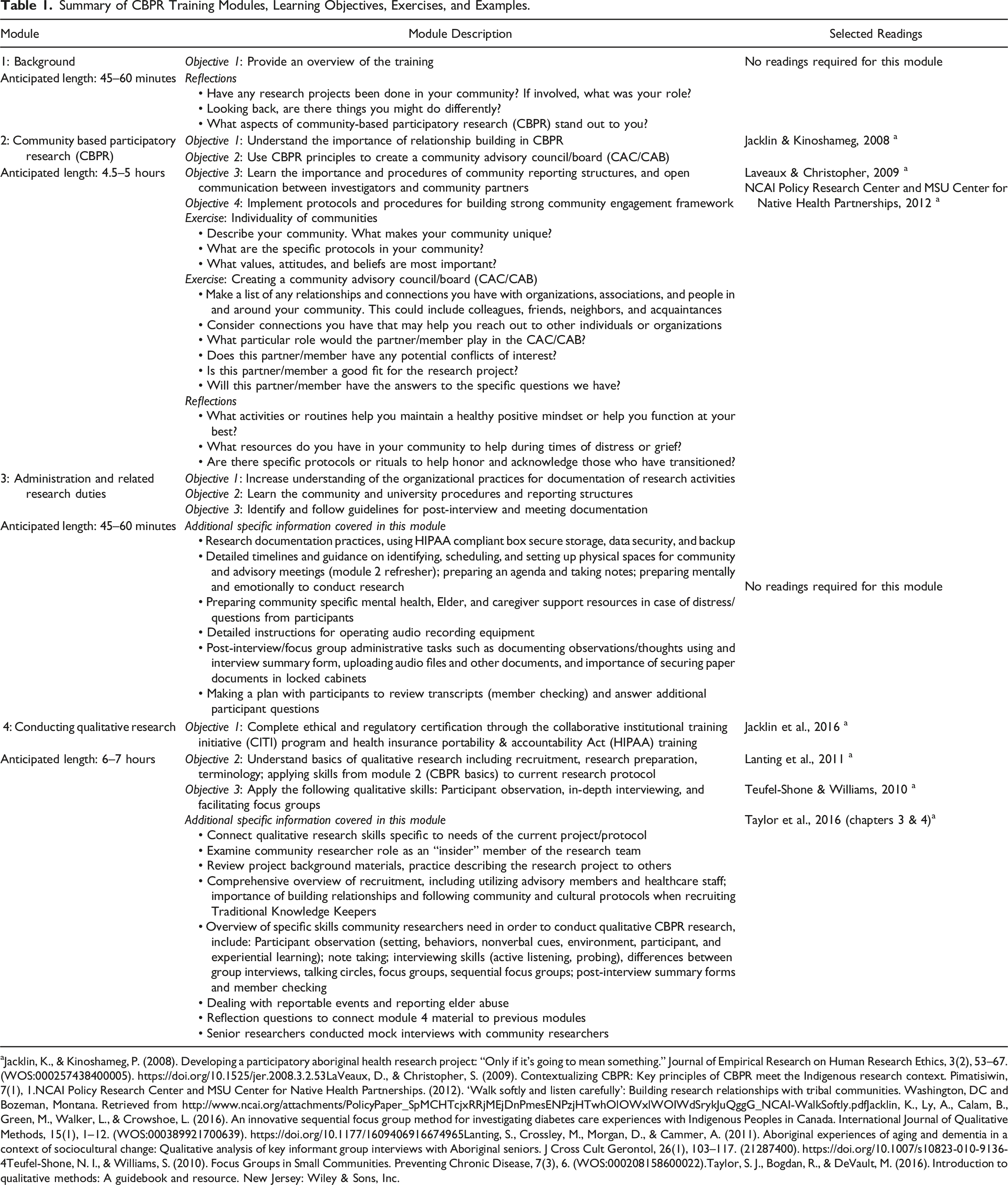
aJacklin, K., & Kinoshameg, P. (2008). Developing a participatory aboriginal health research project: “Only if it’s going to mean something.” Journal of Empirical Research on Human Research Ethics, 3(2), 53–67. (WOS:000257438400005). https://doi.org/10.1525/jer.2008.3.2.53LaVeaux, D., & Christopher, S. (2009). Contextualizing CBPR: Key principles of CBPR meet the Indigenous research context. Pimatisiwin, 7(1), 1.NCAI Policy Research Center and MSU Center for Native Health Partnerships. (2012). ‘Walk softly and listen carefully’: Building research relationships with tribal communities. Washington, DC and Bozeman, Montana. Retrieved from http://www.ncai.org/attachments/PolicyPaper_SpMCHTcjxRRjMEjDnPmesENPzjHTwhOlOWxlWOIWdSrykJuQggG_NCAI-WalkSoftly.pdfJacklin, K., Ly, A., Calam, B., Green, M., Walker, L., & Crowshoe, L. (2016). An innovative sequential focus group method for investigating diabetes care experiences with Indigenous Peoples in Canada. International Journal of Qualitative Methods, 15(1), 1–12. (WOS:000389921700639). https://doi.org/10.1177/1609406916674965Lanting, S., Crossley, M., Morgan, D., & Cammer, A. (2011). Aboriginal experiences of aging and dementia in a context of sociocultural change: Qualitative analysis of key informant group interviews with Aboriginal seniors. J Cross Cult Gerontol, 26(1), 103–117. (21287400). https://doi.org/10.1007/s10823-010-9136-4Teufel-Shone, N. I., & Williams, S. (2010). Focus Groups in Small Communities. Preventing Chronic Disease, 7(3), 6. (WOS:000208158600022).Taylor, S. J., Bogdan, R., & DeVault, M. (2016). Introduction to qualitative methods: A guidebook and resource. New Jersey: Wiley & Sons, Inc.
We further conceptualize second-generation CBPR training as highlighting the importance of capacity building. While “capacity” in CBPR work can be built in a number of ways (Lepore et al., 2021), the training described here builds research capacity in participating communities primarily vis-à-vis the community researchers. Capacity building involves developing the technical skills required for a specific research task and understanding the theoretical underpinnings of CBPR and ethnographic research. The training program is designed to prepare community researchers to engage in all stages of a research program and to be reflexive and comfortable challenging protocols. Capacity building also means utilizing and building upon existing knowledge in order to train future researchers, addressing sustainability and bi-directional knowledge needs (Hacker et al., 2012). To reiterate, we consider our approach a second-generation model because the training incorporates the knowledge and experience of a senior community researcher (KP) who has worked with the investigators (KJ and WW) on Indigenous community-based research for over 15 years. KP represents the first-generation CBPR expert for this specific research (ADRD-focused) and communities, who is now mentoring new and emerging Indigenous community researchers in a similar research topic in new geographic and cultural sites.
Lastly, we incorporate a trauma-informed approach, recognizing that potential participants (both community participants and community researchers) may have experienced interpersonal trauma(s) and/or intergenerational trauma(s) that may continue to impact the broader family unit and community as a whole (Browne et al., 2011; Haskell & Randall, 2009; Krieg, 2009; Mussell et al., 2006). Tujague and Ryan (2021) suggest that “[r]ecognising the role that historical and other traumas play in Indigenous people’s communities and lives is a prerequisite for respectful and safe practice.” A trauma-informed approach is widely used in health and social service settings, and we felt it was especially important to incorporate in this research training due to the longstanding impacts of colonization, genocide, and intergenerational, historical trauma among the populations we collaborate with (Gone et al., 2019). The U.S. Department of Health and Human Services Substance Abuse and Mental Health Services Administration (SAMHSA) guidelines for a trauma-informed approach outline that our program should realize the widespread impact of trauma and understand paths for recovery; recognize the signs and symptoms of trauma in clients, families, staff, and others working with the program; and respond by integrating knowledge about trauma into policies, procedures, and practices in order to actively resist re-traumatization. SAMHSA further highlights six key principles of a trauma-informed approach: (1) safety, (2) trustworthiness and transparency, (3) peer support, (4) collaboration and mutuality, (5) empowerment, voice and choice, and (6) cultural, historical, and gender issues (Substance Abuse and Mental Health Services Administration, 2014). We posit these key principles are synergistic and complimentary with the principals of CBPR. Additionally, the research team incorporated examples, resources, and supports for community researchers who may experience compassion fatigue and vicarious trauma from conducting research within one’s own community, which is one of many important considerations when conducting “insider” research (Brayboy and Deyhle 2000; Heslop et al., 2018).
The training was developed to be delivered virtually and asynchronously. Format development reflected different start dates for the community researchers, distances between research sites (>600 miles at its furthest), and a desire to have the training flexible enough to respond to changing research needs. KP’s narratives were recorded and edited into shorter video vignettes for inclusion in the training modules. Modules are stored on the University of Minnesota Box Secure Storage system, a HIPAA compliant cloud-based file storage and collaboration service.
Piloting the Training Program
The piloting of the CBPR training program involved a cohort of five community researchers from four different Indigenous communities. All community researchers identify as women with three being over the age of 60 and two between the ages of 30 and 39. They had various levels of post-secondary education, ranging from some college or an associate degree to graduate degrees, specializing in finance, social work, and education. Two of the community researchers had previous research experience, with one of the two having qualitative research experience. Information about ADRD, including culturally safe dementia health promotion materials, was provided to the community researchers prior to the training program. Authors KP, WW, MB, and NL were constantly available to community researchers for questions, role play practice, and feedback. A large group debriefing session with the authors and community researchers was held in October 2019. Additional large group meetings were held after the community researchers completed initial interviews to discuss challenges that arose and opportunities to improve the training.
By January 2020, all community researchers started data collection and were conducting in-person qualitative interviews. This changed in March 2020 with COVID-19 and all in-person research activities were stopped. Weekly virtual meetings between community researchers and the research team continued. The pandemic created a need to develop additional training resources focused on facilitating individual interviews virtually and by phone, with subsequent sequential focus groups held virtually via Zoom (Jacklin et al., 2016). These additional training resources were completed by May 2020. Weekly community researcher meetings were used to practice mock interviews and facilitate focus group discussions. Community researchers practiced setting up secure Zoom meetings, recording meetings, and helping participants with troubleshooting technology.
Results
Community researchers shared verbal feedback via weekly team and one-on-one meetings with MB and KP regarding the time it took to complete the training, challenges associated with technology, redefining/acclimating to their roles, and the complexity of learning the traditions and language of academia. MB, KP, and NL debriefed after each meeting and took comprehensive notes to help inform the training process. In the following sections, we will describe these challenges, how the team addressed them, and lessons learned that will impact future iterations of the training program.
Training Took Longer Than Anticipated
All five community researchers were able to complete the required trainings. However, the learners differed in the amount of support required from the senior researchers and senior community researcher. Some community researchers requested one to two debriefing sessions after each module, and others met with a senior researcher twice total after completing all the CBPR modules. The research team anticipated the training modules would take between 14-16 hours to complete; however, the training took much longer, with community researchers reporting taking between 2 and 8 weeks to complete them on a part-time basis (20 hours a week). One community researcher reported it took her 41 hours to complete the CBPR training modules and an additional one to four weeks to complete the university required CITI program (Collaborative Institutional Training Initiative) and HIPAA (Health Insurance Portability and Accountability Act) training.
Training may have taken longer than originally expected because none of the community researchers had formal research backgrounds or training. While this was known and previous research experience was not a prerequisite for the position, in practice this necessitated more time than anticipated for tasks that are highly conceptual. For example, explaining what research is and what it entails, orientation to their role as a researcher, and extensive time devoted to self-reflection questions found in the modules, which were completed both individually and communally at debriefing meetings.
Technical Issues
Four of the five community researchers used Tribal government or health center office space to complete online trainings and participate in debriefing meetings. One community researcher had more flexibility to work from home and had a relatively stable Internet connection. Even if a stable Internet connection was accessible, problems with multiple hosting platforms posed a related challenge. For example, our initial CBPR training program materials were stored on Box Secure Storage (https://www.box.com/). Accessing the Box platform from three different community Tribal government servers meant that firewall issues were frequent and ultimately deemed prohibitive. Google Drive was used for systems that could not interface with Box. Switching to Google Drive solved the compatibility issues, but streaming video content from Google Drive was not possible and required learners to download the entire CBPR training package prior to use. In addition, learners that did not have a Google account were required to create one, resulting in multiple email addresses, usernames, and passwords to keep track of. To address technology issues, new hires are given a USB flash drive containing all training materials during employee onboarding. This relatively lower tech solution solved issues related to limited connectivity and unstable connections for the training modules, but not for the CITI or HIPAA training that requires learners to complete the modules through an online format.
Another technical aspect of the training program was the introduction of professional grade audio recording equipment. We were aware that the equipment used to audio record interviews would be unfamiliar to most, if not all, community researchers. Previous research projects have demonstrated the necessity for practice with the equipment. This was emotionally challenging and stressful to some learners and required additional time and training demonstrations to address. For example, some learners expressed fear of deleting audio recordings or pushing the wrong button and not starting the recording. The research team reiterated the importance of the post-interview/focus group documentation and written reflective interview summary in cases where an interview was not audio recorded. Future iterations of the training modules will include video demonstrations on how to use the audio recorders.
Addressing New Identities and Secondary Trauma
Few of the community researchers had worked in research-related occupations in the past. In addition to learning a new profession’s technical language (see subsequent section), learners had to shift the way in which they thought about their role in the community, particularly how the role of “community researcher” differs from other identities such as employee, family member, neighbor, boss, friend, or any other role they hold in their community. While some community researchers had prior training and skills in interviewing, not all did. This left many feeling as though they were ill-prepared to ask highly personal questions of the research participants. During this training period, learners experienced a wide range of emotions including fear of disappointing university partners, self-doubt, low self-efficacy about their ability to perform their duties, and embarrassment or frustration with the need to learn the traditions and language of academia. The senior researchers reminded the learners that these are very common reactions expressed during CBPR training and that the research team was there to support them in their journey.
A related concern to adjusting to their new role as community researcher was exposure to secondary trauma. A wide variety of care workers, including but not limited to nurses, therapists, counselors, social workers, physicians, and other healthcare professionals, are at increased risk of secondary trauma characterized by fatigue, burnout, and symptoms similar to post-traumatic stress reactions (Armes et al., 2020). Secondary trauma occurs after repeated exposure to patient or client trauma histories and has been documented with care workers exposed to recollections of discrimination (Giordano et al., 2020) and can lead to compassion fatigue (Powell, 2020).
Recognizing that community researchers could be exposed to participant descriptions of early childhood trauma from residential school experiences, a variety of adult trauma experiences, and racial discrimination and bias, self-care was intentionally addressed in the training. The training encouraged thorough preparation before interviews (e.g., being rested, having a clear mind, being in a good mental space to conduct an interview) and comprehensive debriefing after interviews (e.g., sharing positives aspects/challenges of interview with the other researchers). In their community researcher role, learners were encouraged to be mindful of confidentiality at the community level while also acknowledging that participants may share information that is sad, traumatic, or simply not known to anyone else in the community. As such, videos and reflection points were included to help learners pre-plan self-care. In the debriefing sessions, community researchers found the videos featuring real-life experiences and tips from the senior community researcher to be most helpful in mitigating secondary trauma. Once all sites started the interviews, weekly (and later bi-weekly) community researcher meetings were held to further debrief and build a supportive cohort.
Learning the Traditions and Language of Academic Research
Community researchers were confronted with the need to understand a new set of academic traditions and complex terminology. The community researchers came from various occupational fields, each with their own ways of gathering knowledge and communicating with one another about their previous work. Stepping into the community researcher role exposed them to technical language related to dementia, geriatric medicine, qualitative research, and ethics. Some learners, including those with advanced degrees, reported needing a dictionary to make their way through the CITI and HIPAA trainings and required readings. Thus, the challenge was not a matter of level of education, but rather the unique characteristics of very different occupational fields.
Adapting to Community and Research Needs
Working with communities requires flexibility and the ability to adapt to what the community needs. The beginning of the COVID-19 pandemic brought research to a standstill for several months. During that time, the team worked closely with community researchers to better understand the needs of each community and assisted with providing COVID-19 support and educational materials as they became available. The community researchers met weekly to share information and think of ways to engage and support each other and their communities.
Conducting virtual interviews and sequential focus groups required additional training on how to best use the Zoom platform, while keeping the participant engaged and paying attention to non-verbal cues. Many practice sessions were conducted before the community researchers were comfortable in continuing with any of the interviews. Often, the community researcher held a pre-interview practice session with participants to help them become familiar with Zoom. Both MB and NL were involved in the virtual sequential focus groups for technical support, recording observations, and facilitating debriefing sessions with community researchers.
Building Reciprocal Relationships and Reflexive Learning to Increase Researcher Confidence and Capacity
Frequent community researcher meetings built a safe space for feedback, questions, and to identify if further training or support was needed. Group meetings strengthened camaraderie, support, and rapport amongst the community researcher team, which ultimately supports the CBPR principle of “giving back” when community researchers use their transferable skills within and for their community. Meetings provided space for all team members to acknowledge and respect the strengths that each team member brings, allowing all researchers to learn from each other. With varied age ranges, geographic distances, and research experiences among the community researchers, meetings provided space for bi-directional knowledge exchange on multiple levels, including generational, experiential, and geographical.
Recommendations Based on Our CBPR Training Experience
Given the many lessons learned during this CBPR training module development process, we outline specific recommendations and future directions. Overall, the importance of frequent contact between community researchers and senior researchers is paramount in providing adequate CBPR training. Ongoing communication and support from senior researchers is needed throughout the entire training process and for the duration of the project. In this specific instance, meetings addressed everything from technical issues to discussions of the community researcher’s role and potential secondary traumas. Peer-support among the community researchers naturally emerged and became an important support system during their training. Additionally, we recommend that training programs allot more time for check-ins, self-reflection questions, and debrief sessions. We did not initially include enough time and space for these important discussions, but quickly pivoted to add more to the training program.
Community researchers, with little to no previous research experience, cannot simply complete a PowerPoint training and be expected to begin interviewing participants with a high level of research confidence. While the training modules explore self-awareness and reflexivity as a researcher, some community researchers may not be fully aware of the impact of research until they are immersed in interviewing and analysis, which may include personal trigger points or trauma. Depending on researcher identities, experiences, and research topics, they may be affected at varying levels. Emphasis on self-care and providing a safe space for the team to support each other is key.
Additionally, while our CBPR training program addressed core components of a CBPR approach and qualitative research practices, it became clear that more information was needed specific to ADRD. For instance, just as the community researchers needed to become acquainted with the language and traditions of academic research, it was also necessary to explore and understand the biomedical language and understandings around ADRD. We have addressed this in our research project, as one example, by having supplemental meetings and training to address best practices for interviewing people living with ADRD and mitigating distress. We recommend that other researchers also build in disease specific training to best prepare community researchers for understanding the disease state and its impact on participants.
Senior researchers should also become adept in assessing community researcher learning through a developmental framework to identify what each community researcher needs to build capacity and confidence. Since the subjective experience of the community researcher will change as they become more immersed in the process of CBPR, consistent, ongoing support is needed after formal training. For example, as community researchers immerse themselves in the research project, challenges may present themselves, necessitating “refresher courses” or “booster training sessions” to revisit training. Reviewing modules after community researchers have been in the field will allow them to apply and learn from their lived experiences. Reviewing modules can facilitate a strong support system between community researchers, thereby reducing any feelings of isolation and increasing resilience.
Finally, administrative research duties should be explicitly addressed and include technological components (e.g., audio recording equipment usage). These aspects are not typically discussed in qualitative literature yet are an integral part of training community-based researchers and was one of the areas community researchers found the most challenging.
Limitations
This paper describes a CBPR training program with a relatively small number of community-based researchers, which will need further refinement and verification with future community researchers. If and when the CBPR training program is more widely distributed, our team could benefit from an evaluation and/or pre-/post-assessment distributed to trainees.
Conclusion
This paper outlines the process of creating and implementing a second-generation CBPR training program for Indigenous community-based health researchers in the United States and Canada. Several considerations were particularly important in working with this population, including incorporating Indigenous pedagogy, technology/Internet considerations, incorporating a trauma-informed approach, providing ample space for meetings and debriefings with senior researchers, and building rapport and support among the cohort of learners.
There are notable examples of successful training programs in CBPR within Indigenous communities (Jernigan et al., 2015; Maar et al., 2018; Teufel-Shone et al., 2018; The Examining Community-Institutional Partnerships for Prevention Research Group, 2006; Whitesell et al., 2020, 2020). However, only a select few explicitly work to enhance community members’ theoretical understanding of CBPR or work to promote and build CBPR researcher capacity within Indigenous communities. Additionally, while the value of teaching CBPR theory to even those with advanced degrees is highlighted and encouraged (Maar et al., 2018), these publications do not specifically outline a curriculum for training community members on how to collect data within their community using CBPR approaches and qualitative interview skills. In this paper, we have outlined the content of each training module allowing other CBPR researchers to build upon and adapt our curriculum for their specific needs. The components and modules outlined in this CBPR training can be adapted to a wide variety of contexts and further specialized to accommodate community and researcher needs.
One important finding was the difficulty which community researchers had in accessing CITI and HIPAA trainings, underscoring a technological divide between community members and researchers, and highlights a place where university/academic systems should work to better support CBPR efforts. At its most basic level, asking community members to complete extensive online training modules assumes a stable and functional Internet connection. This is an assumption that cannot be met in many rural communities (Pant & Hambly Odame, 2017; Vogels, 2021), including Tribal communities (Kruger, 2019).
Ultimately, this research fills an important gap in providing a culturally affirmative guide for implementing community-based training and building community research capacity. It highlights community-based training as an integral component of CBPR, a methodology particularly suited to address and reduce health disparities in underserved Indigenous communities in the United States and Canada. The CBPR training described here builds upon past research and training to create a reciprocal, second-generation CBPR model that prioritizes Indigenous knowledge and experiences.
Footnotes
Acknowledgments
We acknowledge that the University of Minnesota Duluth is located on the traditional, ancestral, and contemporary lands of Indigenous people. The University resides on land that was cared for and called home by the Ojibwe people, before them the Dakota and Northern Cheyenne people, and other Native peoples from time immemorial. Ceded by the Ojibwe in an 1854 treaty, this land holds great historical, spiritual, and personal significance for its original stewards, the Native nations and peoples of this region. We recognize and continually support and advocate for the sovereignty of the Native nations in this territory and beyond. By offering this land acknowledgment, we affirm tribal sovereignty and will work to hold the University of Minnesota Duluth accountable to American Indian peoples and nations. We would like to acknowledge the community researchers who helped to shape this program: January Johnson, Collette Pederson, Lois Strong, Marlene Summers, and Rhonda Trudeau. We would also like to thank former Memory Keepers staff members Jessica Chiovitte and Andrine Lemieux for their contributions to the training.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institutes on Aging of the National Institutes of Health under award number 1R56AG062307. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.