
Abstract
In this article, we describe a case study in which the method and approach to understanding internalizations of stigma may have both triggered and prompted suppressed memories and past trauma to reemerge. Drawing from trauma informed care approaches, we outline strategies to bear in mind for future studies.
In the midst of a massacre, in the face of torture, in the eye of a hurricane, in the aftermath of an earthquake, or even, say, when horror looms apparently more gently in memories that won't recede and so come pouring forth in the late night quiet of a kitchen, as a storyteller opens her heart to a story listener, re-counting hurts that cut deep and raw into the gullies of the self, do you, the observer, stay behind the lens of the camera, switch on the tape recorder, keep pen in hand? Are there limits of respect, piety, pathos that should not be crossed, even to leave a record? But if you can’t stop the horror, shouldn’t you at least document it?
-Ruth Behar, The Vulnerable Observer (Behar, 1997, p. 2)
Psychological trauma results from an event or a series of events and circumstances that are perceived as hurtful and/or threatening. Trauma effects are the lasting mental, physical, social, emotional and/or spiritual impacts on a person’s functioning and well-being (SAMHSA, 2014). It is nearly a universal experience among people with mental health or substance abuse disorders (SAMHSA, 2014). Given the harmful and long-lasting impact of trauma, many service organizations – especially those that help marginalized populations – have moved towards a model of trauma-informed care (TIC). Guided by TIC, agency staff are aware of and sensitive to trauma and its harms, and actively work to dismantle processes that may retraumatize (e.g., invasive procedures or questioning) the people that they help (SAMHSA, 2014).
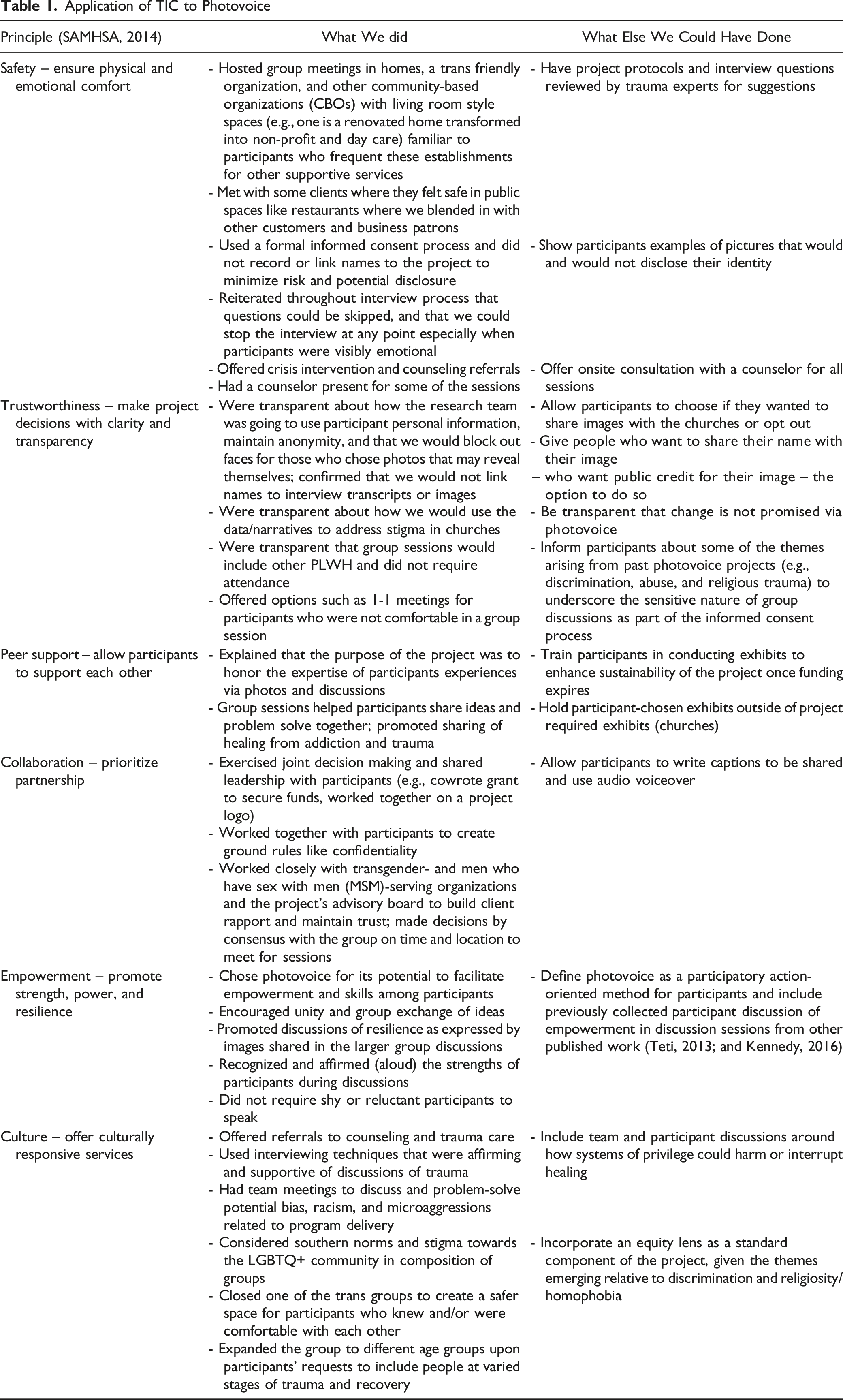
There are six principles of trauma informed care: (1) safety – setting and interactions promote safety; (2) trustworthiness – decisions are transparent with the goals of keeping or building trust with those served; (3) peer support – stories of peers are used in healing and recovery; (4) collaboration – shared power is a priority; (5) empowerment – strength and resilience are built upon; and (6) respect for cultural and historical issues – movement past bias, responsive to the racial, ethnic and cultural needs of those served (SAMHSA, 2014). A small number of people have begun to apply these principles to policy work (Bowen & Murshid, 2016) and research with marginalized communities (Isobel, 2021; Roche et al., 2020; Shimmin et al., 2017; Voith et al., 2020)
As qualitative researchers, however, as Behar’s quote at the start of this manuscript signifies, we often delve deep into the inner most places and souls of historically disenfranchised populations (Behar, 1997). The approaches we use can discern rich experiences from participants. Yet, in doing so, we often also directly or unexpectedly ask participants about their traumatic experiences. What happens when the line of questions or method brings up hurtful memories or experiences from the past? As Behar notes, is it helpful enough to simply document this (Behar, 1997)? Should we do more to protect participants? Are we facilitating the healing process? In this article we describe a case study in which the method and approach to understanding internalizations of stigma may have both triggered and prompted suppressed memories and past trauma to reemerge. Drawing from TIC approaches, we outline strategies to bear in mind for future studies.
Participatory Research and Photovoice
Participatory research – or research that engages participants in research design and implementation decisions collaboratively, and that focuses on benefit to both the researchers and the participants, is aligned with some of the trauma informed principles (e.g., collaboration, empowerment, cultural relevance) (Cornwall & Jewkes, 1995). Yet there is a need to incorporate trauma informed practices more formally into research designs to protect marginalized participants (Roche et al., 2020).
Photovoice is a participatory method used to understand research participants’ lived experiences via photography. Participants typically use a camera to take pictures of images to identify and explore their perspectives about a given topic. These images are shared in small groups to facilitate shared knowledge, discussion, and problem-solving. Generally, exhibits of the participants’ work present their ideas with change makers and ultimately influence new policies or programs (Wang, 1999).
The method is often used among marginalized groups who desire and deserve more of a voice in the service programs designed to help them, or to explore difficult experiences that are hard to convey through words alone (Wang, 1999). It is not uncommon for such groups to have experienced trauma. Photovoice is appropriate for exploring difficult and traumatic issues because it can facilitate participant empowerment and provide a safe space for conversations to ultimately evoke individual reflection and community change. It also involves deep conversations about one’s lives; images can unearth traumatic experiences and discussions. And, although photovoice is an action method with intent to influence individual and or group change, there is no guarantee that this will happen (Sanon et al., 2014).
Application of photovoice with CBPR partnership/project
In 2019, Snap Out Stigma (SOS) was implemented in Memphis, TN (Pichon et al., 2022). Thirty-five people living with HIV (PLWH) consented to take 5–10 pictures depicting internalizations of stigma, to discuss the photos in a large group setting, and to participate in one-on-one more intimate discussions with the two lead researchers. Participants’ photos were exhibited at the local health department, community agency providing support groups, community events during HIV Observance days (e.g., World AIDS Sunday, National Black HIV Awareness Day), health fairs, a Women and Girls Church Conference, and following Sunday worship services. Throughout the photovoice process, there were a few scenarios when the process brought up past trauma among participants.
Discrimination
Several of our aging population discussed a time when health care staff discriminated and disrespected Black PLWH and Black trans women at places of their employment (e.g., health clinics, social service agencies). For instance, during the sexual risk history taking assessment a participant said the provider left the door open to the examination room and spoke loudly for others nearby to hear. Other participants described how providers made accusations of some men having sexual relations with underaged minors. The participants reflected on being misgendered and gave examples of staff incorrect pronoun usage to refer to them. In several cases, these events happened years or even decades ago but the photovoice assignment prompted these memories and examples – See Figure 1. Discrimination
Abuse
Some participants also decided to revisit childhood homes where abuse occurred or places in the community where they sought shelter during periods of homelessness – See Figure 2. They discussed how they had not gone back to these physical environments in years but the photovoice exercise motivated them to return to the places to remind them of personal growth. Admittedly, some participants still were reconciling past trauma via group therapy and still working on moving forward from the past. Abuse
Religious trauma
Living in the U.S. Deep South, religious influence is embedded in the southern culture. Most participants were grounded in a faith tradition as a child and some shifted to no longer practicing due to personal harms from the church. One participant talked in great length about the sexual abuse taking place at their childhood church home. Images of a house, church, and tree were used to convey the participant’s story – See Figure 3. As an adult this person has never looked back. However, the photovoice experience prompted the participant to take photos of a time in their former years that shaped the internalizations of stigma relating to sexuality and struggles with substance abuse. Religious Trauma
Application of TIC to Photovoice
Conclusion
Our project demonstrates our research on the sensitive subjects of HIV stigma may be both cathartic and triggering for participants. We took many measures to increase the trauma sensitivity of the project: increased participant safety by holding meetings in spaces that seemed most comfortable and familiar; built trust through continual transparency; elevated the role of peer support and collaborative decision-making for project ground rules; ensured group discussions concentrated on participant strength and resilience; and refined group compositions in response to identified cultural needs of group members. Though we believe these trauma-sensitivities facilitated the successful commission of our project, we observed the need to more intentionally integrate further trauma responsiveness as part of Photovoice. For future Photovoice projects, we will also work with a trauma specialist during all stages of our work (i.e., to develop interview guides, engage participants in the project, and as part of group discussions in which participants are processing their experiences); further emphasize participant choice relative to if, how, and when their pictures/stories are shared; build on the role of peers by encouraging participants to consider holding their own exhibitions; and incorporate an equity lens as part of the project’s core so that participants are mentally prepared for discussions about privilege and trauma related to forms of discrimination.
A rich literature shows trauma is a pervasive experience among people living with HIV (PLWH). Therefore, our project illustrates one example of how psycho-educational projects and research for PLWH are likely equally as triggering as they are empowering. Consequently, we recommend HIV care providers and researchers consider how trauma-informed principles may be woven into projects as to maximize the empowerment participants experience while minimizing emotional difficulties.
ORCID iDs
Latrice C. Pichon https://orcid.org/0000-0002-2035-8267
Michelle Teti https://orcid.org/0000-0002-3943-3810
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was supported by funds provided by Gilead Sciences COMPASS (COMmitment to Partnership in Addressing HIV/AIDS in Southern States) Initiative, Southern AIDS Coalition Transformative Grant, and Dr. Pichon was the recipient of these funds. The funder did not contribute to the design of the study, implementation, or analysis and dissemination of the research.