
Abstract
This article describes the innovative use of sequential focus groups (SFGs) with Indigenous adults living with type 2 diabetes. This use of SFGs has not been previously described in the literature. In our project, SFGs were used to explore Indigenous people’s experiences in managing their diabetes. Our research objective has been to elucidate deep understandings of these experiences in order to inform the development of continuing medical education curriculum with the aim of improving approaches to diabetes care for Indigenous people. Working in partnerships with Indigenous health organizations, we recruited four groups comprising participants from diverse Indigenous communities (two urban, two rural) in three provinces of Canada. We conducted a series of five focus groups (SFGs) with the same participants (6–8 participants) at each site for a total of 20 focus groups and 29 participants. Indigenous people living with type 2 diabetes were asked open-ended questions concerning their experiences with diabetes and diabetes care in primary health-care settings. Our findings concerning the use of SFGs for Indigenous health research draw on team member and participants’ reflections captured in facilitator field notes, memos from debriefing sessions, and focus group transcripts. The SFG approach enabled in-depth exploration of the complex, and at times sensitive, issues related to Indigenous people’s views on diabetes and their experiences of diabetes care. The repeated sessions facilitated comfort and camaraderie among participants, which led to insightful sessions filled with personal and emotional stories of living with diabetes, the impacts of colonization, and health-care experiences. Overall, the method fostered a deeper level of engagement, exploration, and reflection than a single-session focus group typically would. We suggest this adaptation of the traditional single-session focus groups would be applicable to a wide variety of research concerning sensitive health topics with vulnerable populations.
Keywords
What is Known:
Variations of focus groups, group interview methods, and talking circles have been used successfully in Indigenous health research for many years. Methods that allow for Indigenous ways of knowing and sharing information have been found to be consistent with decolonized approaches to health research. Although no studies using SFGs in Indigenous peoples could be identified, the relatively small number of studies reporting the use of sequential or serial focus groups (SFGs) in health research suggested that the repeated meetings would allow for the elucidation of deeper knowledge.
What this Paper Adds:
We believe this is the first paper to provide a detailed description of a SFG methodology in health research, and the first to report on the use of SFGs with Indigenous participants. The details provided in the paper concerning the process, potential benefits and considerations will help guide other researchers in the field and those interested in applying the SFG method in other contexts. The study demonstrates that SFGs are an appropriate and effective method to explore complex and sensitive health topics with Indigenous peoples. SFGs were found to be congruent with Indigenous approaches to knowledge sharing and can adequately respond to calls for decolonized and culturally appropriate methods for research involving Indigenous peoples.
Introduction
In this article, we describe the application of a sequential focus group (SFG) method in the context of Indigenous 1 health research. The method was developed and implemented in Canada as part of “Educating for Equity” (E4E). E4E is an international research collaboration involving teams in Canada, New Zealand, and Australia that explores how health professional education in Indigenous health can reduce disparities in chronic disease care and improve outcomes for Indigenous populations. The Canadian team has developed health professional curriculum on Indigenous diabetes care by engaging in primary research with Indigenous communities and organizations.
Health research with Indigenous populations in Canada is framed by specific guidelines established by Canada’s granting agencies in response to concerns raised over the last decade (Canadian Institutes of Health Research [CIHR], 2007; Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, & Social Sciences and Humanities Research Council of Canada, 2010). The rationale for such guidelines stems from an acknowledgment that Indigenous peoples are sometimes harmed by research (CIHR, 2007). These harms include appropriation of Indigenous knowledge for profit, secondary use of data without consent, misrepresentations of Indigenous ways of life, pathologizing or otherwise negatively representing communities and eurocentricity (Ermine, Sinclair, & Jeffery, 2004; Schnarch, 2004). The guidelines address key concerns to mitigate potential future harms such as around who owns, controls, has access to, and possesses research data (Schnarch, 2004). These policies suggest that health research conducted with Indigenous people be grounded in community-based participatory research (CBPR) methods creating opportunities for Indigenous communities, organizations, and participants to guide, own, and control the research process and outcomes to the extent possible or desired by Indigenous people. The intent of these policies is to protect Indigenous knowledge and representation by putting in place processes to facilitate participants’ and communities’ voices in the research and control over the collection and use of data. In essence, these policies promote a decolonized approach to research. Our work on E4E in Canada has been influenced by this context for Indigenous research and as such, we have structured our activities to ensure appropriate methodologies and inclusive processes.
Focus group and group interview methods have been used extensively in Indigenous health research, but we believe this is the first article reporting on the use of SFGs in this population. We define SFGs as a series of semi-structured interviews with a consistent small group of people coming together to gain deep insight into a topic by exploring questions about an issue with each other and a group facilitator over an established period of time. In this article, we will describe the innovative use of SFGs with Indigenous adults living with type 2 diabetes in three provinces across Canada. The purpose of the SFGs was to explore Indigenous people’s perspectives on and experiences living with diabetes in sufficient depth to allow us to build collective narratives that could serve as teaching cases. The vital role of storytelling derived from a long history of oral tradition among Indigenous peoples is increasingly being acknowledged in research with Indigenous communities. Struthers, Hodge, Geishirt-Cantrell, and Cora (2003), for example, describe the success of employing talking circles in a study of Native Americans’ experiences of type 2 diabetes, as this method was culturally familiar with participants and it encouraged the sharing of experiences through stories. The use of SFGs in our own study respects the narrative approaches that participants could potentially use to articulate their experiences. Hence, the repeated meetings ensured that there would be ample time for stories to unfold and to explore more in-depth people’s experiences than a single session would allow. The experiences shared were also used to ensure patients’ voices were captured in the development of an approach to care framework for health-care professionals working with Indigenous patients with type 2 diabetes.
The project’s formative theoretical model was postcolonial theory. While largely consistent with health equity and structural violence (Farmer, Nizeye, & Keshavjee, 2006), a postcolonial perspective emphasizes partnerships, is praxis-oriented, appreciates continuity between past and present health or health-care contexts, and acknowledges that research itself has the potential to colonize (Browne, Smye, & Varcoe, 2005). The overarching analytic model for the SFG method was phenomenology (Grbich, 2007), focusing on the common experiences of Indigenous people with diabetes. Writing on the use of phenomenological narrative interviews as a research method with Indigenous populations, Struthers and Peden-McAlpine (2005) propose that, “phenomenology provides a seamless link with Indigenous peoples and their culture, as it employs the natural inherent methods of oral tradition, narratives, and stories” (p. 1274). An explanatory model framework (Kleinman, 1980) was used to elicit the illness experience within a cultural context; an Indigenous social determinants framework was used to understand barriers and enablers to diabetes care (Reading & Wein, 2009); and participatory approaches were used to facilitate the inclusion and sharing of Indigenous knowledge (Castellano, 1993; Kovach, 2009, 2010; Petrucka, Bassendowski, Bickford, & Goodfeather, 2012).
Background
Indigenous health research
Much has been written on matters concerning the ethics of research with Indigenous peoples. Over the past 10–15 years, researchers have proposed various sets of principles to assist in developing ethical codes for conducting research with Indigenous peoples who is consistent with Indigenous worldviews and struggles for self-determination (Castellano, 2004; Kovach, 2009; Petruka et al., 2012; Tuhiwai Smith, 1999). Bartlett, Iwasaki, Gottlieb, and Mannell (2007) propose an Indigenous-oriented process framework for decolonizing research, which includes six distinct processes: rationalizing, enabling, facilitating, experiencing, accepting, and enacting. Others have written about the advantages and need for more CBPR (Jacklin and Kinoshameg, 2008; Cochran et al., 2008; Frerichs, Hassmiller Lich, Dave, & Corbie-Smith, 2016; Tobias, Richmond, & Luginaah, 2013). The National Aboriginal Health Organization (2007) developed principles around data ownership to help communities in their consideration of research proposals they receive. These are the principles of Ownership, Control, Access and Possession (OCAP™). These principles have recently been trademarked and sanctioned by the First Nations Information Governance Committee. Much of this aforementioned work is now captured in community-based and institutional ethics review processes and in the policies and guidelines of major health research funding bodies in Canada (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, & Social Sciences and Humanities Research Council of Canada, 2010). This trend is also evident in other nations that have a colonial relationship with Indigenous populations such as Australia (Laycock, Walker, Harrison, & Brands, 2011; National Health & Medical Research Council, 2003, 2005, 2010) and New Zealand (Health Research Council of New Zealand, 2010).
A small number of articles have attempted to elucidate how to incorporate Indigenous principles into the research process. Often foregrounded in these discussions of Indigenous principles in research are the importance of acknowledging the interconnectedness of people, things, ideas, and processes (Loppie, 2007); the need to build trusting relationships (Maar et al., 2011); maintaining accountability to these relationships (Wilson, 2008); and the value of storytelling as a mechanism for sharing, teaching, and healing (Struthers, Hodge, Geishirt-Cantrell, & Cora, 2003; Struthers & Peden-McAlpine, 2005).
Consistent with these principles, our decision to adopt an SFG approach was based on the following goals: fostering trust and building rapport with participants, allowing ample time for people’s personal stories to unfold and for sharing to occur, providing opportunities for reflection during and between sessions, and exploring in-depth people’s perspectives on the experience of living with diabetes.
SFGs in health research
In a chapter promoting innovation in the focus group method, Morgan, Fellows, and Guevara (2008) discuss the brief history of “repeated” or “reconvened” focus groups in the social sciences. It becomes evident from this review that a limited number of researchers in the social sciences have experimented with some form of repeated group interviews over the past 25 years. Our literature review revealed that the SFG method has rarely been used in health research. Using related search terms, such as repeated, serial, consecutive, or multiple focus groups, we found only one health study that employed a similar method to ours. In this study, the researchers conducted repeated focus group interviews with two groups of participants, where each group of the same participants attended five sessions, representing a total of 10 focus group sessions (Jonsson, Hallberg, & Gustafsson, 2002). They describe the milieu of the focus group sessions in their study as allowing for “multivocal conversations” (p. 336) and concluded that having repeated focus group meetings allowed the participants to “share their knowledge in a deeper way than if they had only met on one occasion” (pp. 336–337).
Although reported uses of the SFG method in published studies is sparse, there are a few methodological discussion papers that highlight potential benefits of multiple focus groups, including increasing the reliability of the data (Betts, Baranowski, & Hoerr, 1996; Sim, 1998), assessing the extent to which data saturation has been reached (Flick, 1998), or eliciting a more in-depth understanding of the array of perceptions, beliefs, attitudes, and experiences held by participants (Krueger & Casey, 2009; Vaughn, Schumm, & Sinagub, 1996). Morgan et al. (2008) suggest that there is value in the continuity created with SFGs with the same individuals but caution that recruitment becomes more complex (p. 195). Much of the writing on the use of multiple focus groups centers on the suggested number of participants or the number of single focus groups that are needed in the same study in order to draw comparisons, achieve variation in sampling, or to yield diversity in the information provided. There is absence in the literature of discussions around what Lunt and Livingstone (1996) refer to as the standard “one-shot” design versus the adoption of an approach that favors repeat meetings. However, there is some evidence that serial or repeated one-on-one interviews are an effective approach for collecting longitudinal qualitative research data (Corden & Millar, 2007; Smith, Lister, & Middleton, 2004; White & Ariz, 2005). Serial interviews have been employed to study a range of health and health-care issues such as experiences of end-of-life care (Johnston, Milligan, Foster, & Kearney, 2012), the well-being of family caregivers of patients with lung cancer (Murray et al., 2009), the therapeutic impact of interviews on cancer patients (Colbourne & Sque, 2005), and the lived experience of patients with severe chronic obstructive pulmonary disease (Pinnock et al., 2011). Murray and colleagues (2009) propose that serial interviews are a “convenient and efficient approach to developing an ongoing relationship between the participant and researcher, thereby facilitating discussion of sensitive and personal issues while also allowing exploration of changing needs and experiences” (p. 958).
Reflecting on the standard approach to focus group research, Kitzinger and Barbour (1999) advocate for the need to move away from a “formulaic approach which fails to develop the full potential of this method” (p. 1). Elaborating on the utility of focus groups as a qualitative research tool nevertheless, they maintain that “focus groups are invaluable for examining how knowledge, ideas, story-telling, self-representation and linguistic exchanges operate within a given cultural context” (Kitzinger & Barbour, 1999, p. 5).
The extensive use of focus groups in Indigenous health research studies suggested to us that SFGs would be an appropriate method. All of the principal investigators had experience using focus group methods with Indigenous peoples in other projects. The project’s lead principal investigator had previous experience devising and implementing the SFG method with an urban Indigenous population. Still, the investigators carefully considered and reflected on the method and engaged in dialogue with the research sites concerning its acceptance and suitability. Some key guiding questions we considered included Does the research method foster trust and aid in developing rapport? Does it adhere to established ethical guidelines for working with Indigenous populations? Is it a culturally appropriate method? Does it reflect the principles of decolonizing research? Can it be used to support phenomenological and narrative approaches to data analysis?
Method
The study was carried out according to the established guidelines for ethical research with First Nations, Inuit, and Métis peoples in Canada. Research ethics approval was granted from each investigator’s university—University of Calgary (ID: E-23532), University of British Columbia (ID: H11-01408), Queen’s University (ID: FMED-244-10), and Laurentian University (ID: 2011-07-03) researchers. Research agreements were negotiated and agreed upon at each of the research sites. Agreements outlined accountability mechanisms and protocols for engagement and sharing of knowledge. These were approved by health directors and in some cases chief and council.
Several measures were put into place to ensure that our E4E research practices were inclusive of and informed by Indigenous perspectives, including the following: establishment of formal community partnerships, the creation of an advisory group that included Indigenous community members and health professionals, gathering feedback from Indigenous patients during a pilot focus group session, and the presentation of preliminary research findings to communities at public “member-check” sessions.
Site Selection
Communities involved in the research reflected our interest in balancing on-reserve and urban demographics and our preexisting research relationships.
Research involving Indigenous populations in Canada requires the consent of Indigenous communities as well as individual participants. Information letters about E4E were sent to five Indigenous community organizations that the investigators had existing relationships with in Ontario, Alberta, and British Columbia. All sites agreed to participate giving us two urban settings (Ontario and Alberta), two rural First Nation reserves (British Columbia and Alberta), and one remote First Nation (Ontario).
Development of the Focus Group Guide
The questions explored in each of the focus group sessions were developed by the investigators drawing on their own previous experience and an evaluation of published literature concerning Indigenous diabetes care experiences. The guide was developed to facilitate discussions around Indigenous experiences with diabetes over five sessions. The first focus group session drew on an explanatory model approach (Kleinman, 1980) to elicit Indigenous perspectives on diabetes and wellness. This approach is grounded in anthropological methodology, whereby eliciting how patients understand and explain their condition may reveal to a physician not only a patient’s knowledge of an illness, but a patient’s beliefs, social meanings, and expectations that can shape the clinical relationship. An Indigenous determinants of health model (Reading & Wein, 2009) informed subsequent focus group sessions as we explored spheres of influence in relation to diabetes management. Added to these was our postcolonial and health equity lens that influenced all sessions but most notably the fourth session concerning health-care experiences. The topics and a selection of questions are summarized in Table 1. While the process of question development was not conducted in partnership with the research sites, people with diabetes had an opportunity to review the questions and recommend changes during the pilot focus group session described in the following section.
Sequential Focus Group Discussion Topics.

Pilot Focus Group
A pilot focus group was conducted to trial the interview guide. Since the actual focus groups would be held over five sessions, the interview guide was organized into five sections, representing a focused topic of discussion for each session (e.g., health-care experiences) and corresponding interview questions for each topic. Sample questions from each section of the full five-session interview guide were tested in this single pilot focus group.
Through the pilot focus group process, we were able to see where the interview guide required revision, test questions where we anticipated encountering problems, and observe the interaction between participants for clues about levels of comfort and engagement. The pilot resulted in slight modifications to questions for better clarity and clearer role definition for facilitators. We determined that the “definitional” questions we asked as a way of leading into a topic did not generate much response. As such, to make it more open-ended, questions such as “How do you define diabetes?” or “What is your definition of culture and tradition” were modified to “What is diabetes?” (Question 1) and “Do you think there is a relationship between “community” and diabetes?” (Question 9). Moreover, the latter question was modified specifically after observing that participants preferred the use of the term community to index their socially embedded and collective, yet locally specific, experiences rather than the more general term “culture.”
Recruitment
We recruited participants diagnosed with diabetes from Indigenous health organizations. The inclusion criteria for participant recruitment specified that participants were required to be Indigenous adults (≥18 years of age) living with type 2 diabetes, attend all five focus group discussion sessions, and speak English proficiently. Additionally, participants were required to have been receiving care from the same family physician over the past 12 months. We were interested in experiences of care that were grounded within an established relationship. We also hoped this would facilitate a more balanced exploration of their experiences of care; for example, this group would also more likely report positive aspects of relationships and care. We thought that unattached patients may not have similar experiences to draw from. The invitation for study participants was advertised in the communities and health organizations with the help of local staff. Participants meeting the criteria were urged to anonymously call our research staff for further information and to be prescreened for the inclusion criteria. All participants who volunteered for the study and met the criteria were enrolled in the study. While we were not aiming for demographic diversity in the composition of the focus groups, we wanted to ensure a balance of men and women whenever possible to allow for an analysis of potential gendered differences in the experience of diabetes for Indigenous people. In the end, our final sample included 11 men and 18 women ranging in age from 45 to 79 years.
Duration, Location, and Compensation
Vissandjée, Abdool, and Dupéré (2002) remark on how “participation in focus groups must be convenient, and researchers must consider the different daily lives of men and women to select appropriate times and venues” (p. 829). During the recruitment phase, we inquired with participants about proposed meeting venues, acceptability of the anticipated length of the session, preferred meeting times, any mobility limitations preventing individuals from easily attending the sessions, or other barriers such as transportation and child care needs. We made every attempt to reasonably accommodate participants.
Each participant received a CAD$50 honorarium for each session attended. Acknowledging both the Indigenous customary practice of offering food at social gatherings, and the time commitment required to attend the focus group sessions, we opted to also provide a light meal for participants.
Implementation
The SFGs were organized in partnership with our community partners. Sessions were held at the local health center or community friendship centers. SFGs were conducted between October 2011 and June 2012 in four out of the five participating sites. The remote First Nation site (Ontario) subsequently advised the investigators that one-on-one interviews would be more appropriate for their community due to concerns about sharing personal health information in a group setting. This resulted in a total of four groups of participants (one group per site), who we met with 5 times in SFG interviews over a 1 to 2-week period, representing a total of 20 focus group sessions in the overall study. Each focus group was comprised of 6–8 participants, for a total of 29 participants. At all but one site all participants were able to attend all five sessions. At one urban site, one participant misses the first session.
Facilitators were E4E research staff. Two facilitators were assigned to each research site. Both facilitators participated in all five sessions. At the start of the first session, the facilitators explained the purpose of the study and initiated the formal consent process including permission from participants to digitally audio-record the sessions for later transcription for the purposes of data analysis. Each focus group session lasted between 2.5 and 3.0 h and were semi-structured. Regular weekly meetings by teleconference with the entire E4E team were scheduled once data collection began to allow the research staff to debrief with each other and the investigators.
Community Member Checking
Member checking is described as the “most crucial technique for establishing credibility” (Lincoln & Guba, 1985, p. 314). According to Cho and Trent (2006), member checking is a process that should occur throughout the inquiry, where research findings are “played back” to participants to check for perceived accuracy and reactions. The SFG method allowed for this continual process of member checking to be embedded. At the start of every session, facilitators’ interpretations of the previous day’s discussion points were summarized and presented to participants to elicit their feedback and to check for accuracy. Participants were encouraged to reflect on their thoughts and feelings regarding the information shared in the last meeting.
A formal community member check occurred in each community 6–12 months post-SFG to present initial study findings to participants, health staff, and general community members for feedback. Participants from the focus groups were invited to attend the community member checks, and everyone was encouraged to bring family, friends, and other community members. Due to prior commitments, some participants were not able to attend, resulting in a lower turnout among original study participants than we were hoping for at all the sites. In one community for example, a death of a community member resulted in just one original participant attending the community member check session. In most communities, we found there were more health-care workers or general community members in attendance than participants (Table 2).
Community Member Check Attendance.
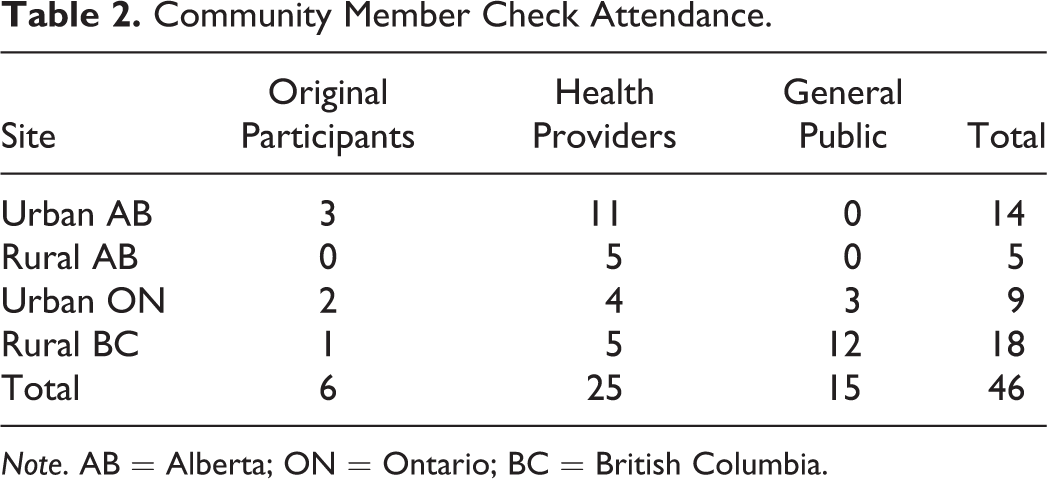
Note. AB = Alberta; ON = Ontario; BC = British Columbia.
These member checking sessions lasted approximately 2 h and included a light meal. A formal presentation was given by the team followed by participant feedback.
Results
The SFG methodology was successful in providing a data set that allowed us to proceed with phenomenological analysis leading to collective lived experiences of diabetes and diabetes care at each of the sites. We were able to collect data in all of the domains deemed important at the onset with sufficient depth. The data was used to create complex instructional cases grounded in the experiences of Indigenous people living with diabetes.
The research did not include a formal evaluation of the effectiveness or appropriateness of the SFG method in Indigenous settings. Our findings here draw on reflections of the project team and comments captured in the focus groups transcripts made by participants. An overview of the benefits, possible limitations, and considerations is summarized in Table 3.
Benefits, Limitations, and Considerations in the Use of Sequential Focus Groups.
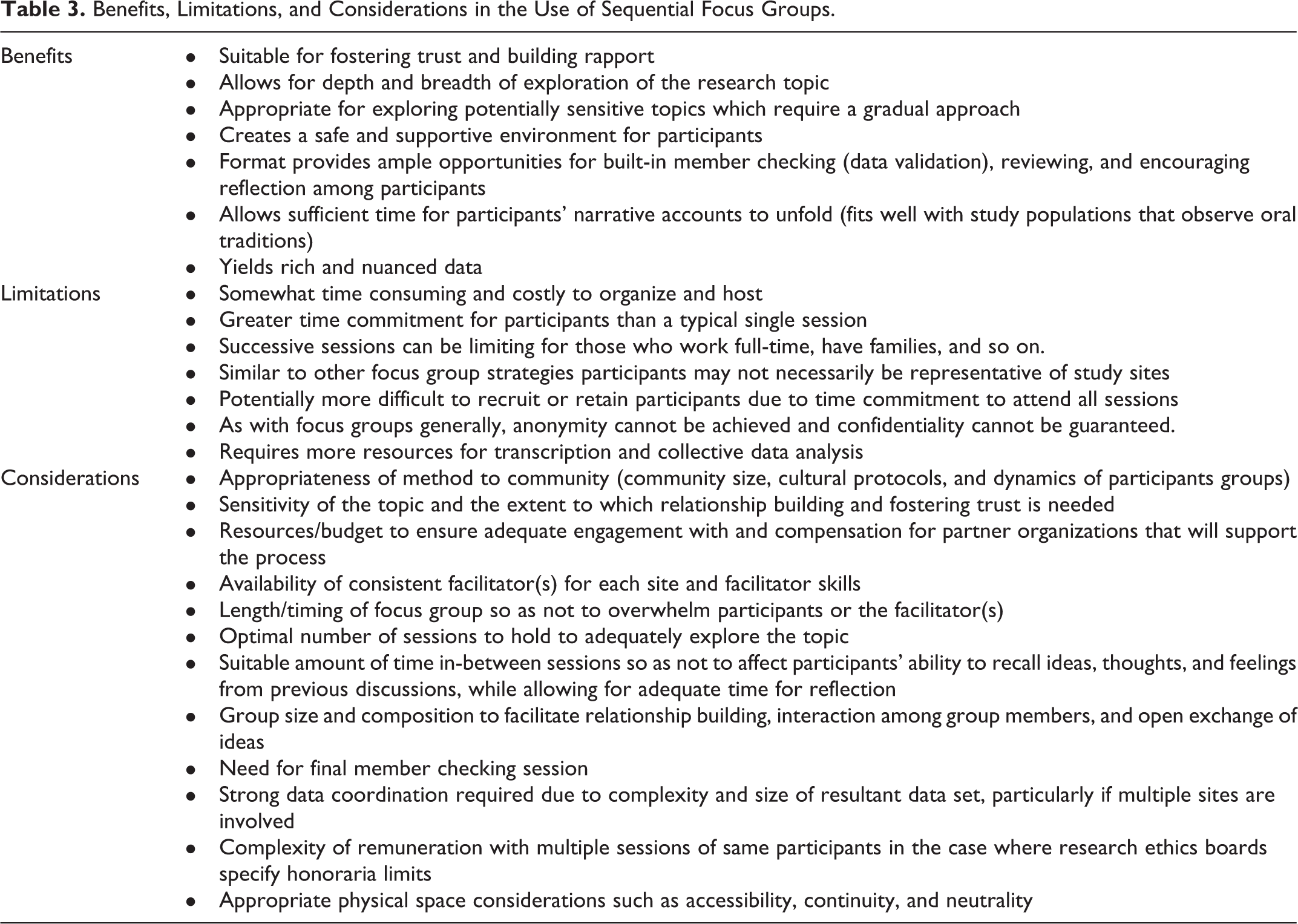
Upon reviewing facilitator field notes, memos from debriefing sessions, and focus group transcripts, we saw indicators suggesting that this data collection technique is a valuable, effective, and promising research method for exploring in-depth Indigenous people’s perspectives on diabetes in most community settings. Notes indicate that it allowed for a gradual building of trust and rapport, which resulted in the candid sharing of personal stories, thoughts and feelings, and ultimately yielded a richness of data that likely would not have been possible to achieve in a typical single-session focus group interview.
Building Trust and Rapport
A common theme recorded in the facilitators’ notes was the increasing comfort of participants with each subsequent meeting. As participants became more comfortable, less prompting by facilitators was needed, more casual conversation between participants was noted, and it took less time at the start of later sessions to delve into discussion. At one of the sites the facilitators debriefing notes indicated that during the first two sessions participants spoke in general terms about how diabetes affected people’s lives rather than relating back to personal experiences. It was not until Day 4 of the debriefing notes that the facilitators begin to note greater levels of comfort and willingness to share personal experiences: I felt like today was the first time that they really started going into the territory of their attitudes, you know some of their personally held beliefs and attitude and beliefs and stuff around diabetes, particularly around the discussion with the issue of fear and not wanting to fear something because of the belief that you might contract the illness. And that was good for me, I thought that was lacking in the conversations earlier.
This suggests that the method did provide the research team with a more in-depth understanding of the participant’s values and experiences as suggested by Krueger and Casey (2009) and Vaughn, Schumm, and Sinagub (1996). Most notably, was the extent to which participants began to open up and share personal stories of their experiences with health care and the challenges of living with diabetes and also the pain and suffering caused by experiences of residential schools. Facilitators noted in a debriefing session on Day 3 that, “It was quite…that was a really rich conversation around people’s experiences of residential school without us having to pry.” Another noted, “It sort of came up organically. The link between the residential school and food now and food then, I thought was very strong.” Facilitators were surprised by participants’ willingness to share such deeply personal accounts, given the sensitive nature of the latter topic. In the end, we interpreted this candidness as a reflection of participants’ level of comfort with the setting and process of the SFGs. Also, we believe that participants appreciated the opportunity to share their stories in a safe environment and to have their voices heard. During the fifth and final session at one of the sites, a participant shared, “I thought that I was the only one who felt this way.”
Healing and Empowerment
An unexpected outcome was participants reporting that the level of sharing that occurred during the SFGs contributed to their own healing: For me I’d like to say it’s been really helpful…because out there you’re not really as sharing as you would in this kind of environment. So, it really brings a lot of healing…because we’re all sharing a lot here. Just having this focus group, it really brought my realisation of the seriousness of the illness. And, you know, [I liked] the sharing…and, to me, to verbalise what I went through with this illness, it really helped me, this group. It made me realise a lot of stuff.
Participants also appeared to enjoy and value the communal aspect of the focus groups. Many people emphasized the importance of taking collective action to prevent diabetes in their community; hence, coming together to discuss common experiences of diabetes was viewed as an important and proactive way of encouraging change. The following comment made by one of the participants demonstrates how the sharing of stories concerning individual diabetes experiences fostered a realization of the social determinants that have affected them collectively and the need to act on this knowledge: Everybody sits down and let’s share stories, maybe because we can learn from [each other]…. We have to put our, all our thoughts together to make it work…. You know…we went through a lot of stress here on the reserve. Not only for diabetes, cancer, alcoholism, residential schools. You know, we’ve learned a lot of how we solve some of these things…and we have to work together.
Discussion
Iteration and Reflection
The inherently iterative process of SFGs proved to be highly congruent with our phenomenological approach. As Srivastava and Hopwood (2009) comment: The role of iteration, not as repetitive mechanical task but as a deeply reflexive process, is key to sparking insight and developing meaning. Reflexive iteration is at the heart of visiting and revisiting the data and connecting them with emerging insights, progressively leading to refined focus and understandings. (p. 77)
The final community member checks occurred between 6 months and 1 year after the initial SFG sessions. The group composition was quite different than that of the SFGs which an overrepresentation of health-care workers at the community member checks. For the most part these sessions validated our analysis rather than contributing to it. Since the participants in these sessions were diverse and did not only represent the patient perspective, we placed greater value on the built-in member checking during the SFGs. We found that health-care workers may agree with the themes presented but would add new information from their perspective. In one case, for example, the health-care workers put a greater emphasis on patient responsibility over access to resources. In hindsight, these sessions would have better served as knowledge translation events rather than member checks.
Regular weekly meetings with the entire project team also facilitated reflexivity by allowing the research staff and investigators to debrief. These larger team debriefings were an important early part of the iterative process in our qualitative inquiry.
Decolonizing Research
Determining the extent to which our method approximated a decolonizing methodology is less straightforward. Nevertheless, our reflections have led us to the conclusion that the research we carried out is but one example of a myriad of ways to conduct research with Indigenous peoples from the standpoint and goal of decolonization. Our study provides an example of a decolonizing method insofar as the relational aspects of our research were always foregrounded (Chilisa, 2012). This emphasis on the relational aspects of research is what led us to adopt an SFG method which we believed would allow us to build trust and rapport more effectively with participants. Moreover, the postcolonial lens employed in this study shaped all aspects of our research and ensured that our methodological approach and processes were informed by the goals and principles of decolonizing research. Our research team members are both Indigenous and non-Indigenous which provided opportunities for multiple ways of understanding the world to be incorporated into the process.
Storytelling and narrative approaches are viewed as appropriate approaches to research with Indigenous peoples (Kovach, 2010; Struthers & Penden-McAlpine, 2005) The use of SFGs in our own study, respected the narrative approaches that participants could potentially use to articulate their experiences. The repeated meetings ensured that there would be ample time for stories to unfold in an increasingly comfortable environment.
We recognize that our overall approach did not facilitate a truly community-based participatory process which would have involved community partners at every step along the way (Jacklin and Kinoshameg, 2008), although the SFG method required us to work in close partnership with local agencies. Because of the national scope of the project, we instead chose to work in partnership with an advisory group comprising stakeholders. We note that the incorporation of a community-based approach throughout each stage may have resulted in better inclusion of multiple Indigenous worldviews.
Considerations in the Use of SFGs
The SFG method presents opportunities for researchers to conduct research into topics that may be potentially sensitive, require more in-depth exploration, or necessitate gradual rapport building when it is not feasible to work longitudinally with participants. The description of our use of this method should not be read as a prescriptive “how to” guide to conducting SFGs. Rather, it indicates how this method was a viable and culturally acceptable data collection technique for the particular communities that we worked with and given the specific contextual (relational and practical) factors in place, such as preexisting relationships with communities, project timeline, and research budget. It is noteworthy that one of our community partners did not view focus group methods as appropriate for them. Needless to say, researchers interested in employing the SFG method ought to carefully consider both the general benefits and limitations of this technique as well as the specific circumstances in which this model would be applied (see Table 3). For example, how the method may need to be tailored in different studies to take into account potentially important and culturally sensitive dynamics pertaining to gender, class, age, ethnicity, role in the community, and education.
Gender
During the planning stages of this study, we contemplated holding additional single-gender focus group sessions at each site but were not able to proceed due to time and financial restraints. Our observations during the SFGs suggest that this could have yielded further valuable data and provided insight into how SFGs influence gender dynamics. At one First Nation site in our study, for example, there were more women than men (six and two, respectively), and this resulted in a dynamic where the women were relatively more vocal than the men. At another site, however, despite having an equal number of men and women in the same group, it was most often the case that the women would defer to the men whenever a new topic of discussion was introduced. It was only after the male participants had ample opportunity to share their views that women would then offer their opinions. Holding additional single-gender focus group sessions could have allowed us to see how women’s level of comfort with participation in the SFGs changed under different conditions and potentially elucidated more gender-specific diabetes experiences.
Time and resources
An important and practical criterion to consider is the temporal aspect of conducting SFGs. Most research is constrained by time and money, thus planning the optimal number of consecutive sessions to hold or the suitable amount of time in-between sessions is important. The latter consideration is especially significant, given that time lapses between sessions may affect participants’ ability to recall ideas, thoughts, and feelings from previous discussions. Our consultations revealed that participants preferred the sessions be held in a short time frame (within a 1 to 2-week period). They did not view this as too onerous or tiring, as we had thought, and the sessions benefited from the discussions being fresh in participants’ memory. This allowed for easier recall or review of discussion points and, most importantly, more seamless development of rapport and relationship building among the group.
Resources need to be a consideration when considering the SFG method. The customary costs of honorariums, food, and space rental are all elevated by the number or repeated sessions that are included. Perhaps less obvious is the need for adequate support for data analysis and management. The five sessions at four sites resulted in considerable qualitative data to transcribe, code, and analyze. The national and distributed nature of our team added to the complexity. Our team used QSR NVivo 9 (a qualitative data software analysis program, QSR International Pty Ltd., Version 9, 2010) as a data management tool. Each research site required an independent site license and training on the program. Overall project management was key to the amalgamation and distribution of the data to the investigators for consideration and discussion. Several teleconferences were required to work through the analysis. Intensive team retreats at a central location would have eased this process but were not included in the original budget.
Facilitation
Also central to the building of trust and rapport among the group was the involvement of the same facilitators for each of the five sessions. This demonstrated an equal commitment to the process on the part of the research team. We also note a benefit in using existing research staff to conduct the focus groups. These staff had been hired based on their experience working with Indigenous populations and were aware of the goals of the project. Their involvement in many aspects of the project including research design, the development of data collection tools, and data analysis ensured better overall continuity in the data collection and analysis process.
Recruitment and retention of participants
Morgan et al. (2008) suggest that repeated focus group sessions can impact recruitment and retention of participants due to the time commitment required. Participants often have other priorities that make it difficult to commit to multiple sessions. Our recruitment strategy became highly personalized after initial contact was made by the potential participants. Working closely with the partner organizations and participants on scheduling was a significant factor in ensuring retention. Research assistants had many discussions with participants and local health-care staff to determine the best dates and time of day for them. Our protocol also included transportation when it was needed as well as a full meal during the sessions. These considerations made accessing the sessions easier and perhaps provided some incentive to attend. We offered an honorarium to acknowledge the value of participant’s time and knowledge. Importantly, we did not withhold payment to the end of the process but instead opted to compensate group members CAD$50 at the end of each session they attended. This was done to recognize the commitment they made to the project that day regardless of the participant’s ability to return to the next session. We did not find that recruitment or retention was an issue at our sites. Just one participant across all sites was not able to participate in one of the five sessions. The strategy also helped to ensure that the final sample of participants at each site were diverse—sessions could be held in the evenings to accommodate those who were employed; and transportation, food, and honorariums made it possible for those with fewer resources to participate.
Conclusion
The use of SFGs in health research has not yet received any attention in the literature. In light of this gap, we sought to describe this approach and our experience with it as a promising method for qualitative inquiry with Indigenous peoples.
The SFGs employed in our study allowed us to explore Indigenous people’s perspectives on living with diabetes and their views on diabetes care. Based on the 20 focus group discussions we held with a total of 29 participants from four Indigenous communities across Canada, we believe that the SFG method can be a culturally congruent and viable data collection technique for research with Indigenous peoples.
Our findings of participants’ experiences with the research process are congruent with what Jonsson, Hallberg, and Gustafsson (2002) reported in their study using SFGs which indicated that the research method enabled participants in their study to “share their knowledge in a deeper way than if they had only met on one occasion” (p. 336). Our experience shows that participants were engaged in the research process and openly shared their knowledge. The SFGs method provided participants the time needed to share their stories and, in the process, they felt more empowered as they learned more about diabetes from others in the group and actively took part in providing suggestions for the improvement of diabetes care. The fact that some of the groups ended up feeling that they could collectively act on what they had discussed in the sessions suggest that the SFG method is appropriate for CBPR designs.
We believe that our successful experience with the SFG method is owing to a number of factors. First, this approach respects and acknowledges the importance of a narrative tradition in Indigenous communities; hence, the repeated meetings provided ample time for storytelling and the sharing of personal experiences with diabetes. Second, this method allowed us to gradually build rapport with participants and to foster trust, which increased people’s level of comfort within the group such that we were able to explore sensitive topics. Last, the method yielded rich and reliable data because it provided participants time between sessions to reflect on discussion points, which were then revisited in each session. This built-in data validation process was indeed highly valuable and a unique feature of the SFG method.
In summary, this data collection technique should be considered a viable approach if the research program requires in-depth exploration of complex, interconnected, and potentially sensitive topics. There is need for increased attention to issues of culturally appropriate qualitative research methods for studies involving Indigenous peoples. Although much has been written about the broader ethical shift to research orientations that emphasize the value of CBPR, and the need to acknowledge Indigenous research principles, there is still a paucity of literature that describes the process, benefits, or limitations of specific methodological designs in qualitative research with Indigenous peoples. This article provides an example of how SFGs were successfully used in research with Indigenous adults living with type 2 diabetes.
Footnotes
Acknowledgments
We would like to thank our research partners and the E4E Advisory Committee for their support, guidance and participation and our E4E research team who facilitated and supported the SFGs: Tiina Liinamaa, Sarah Elliott, Tanu Gamble, Elaine Laflamme, Elaine Boyling, and Joanne Parker. Thank you to Katelynn Viau for her assistance preparing the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Institutes of Health Research funded this study through the International Collaborative Indigenous Health Research Partnership grant (#IDP-103986, Grant number: RT735835), in partnership with the Health Research Council of New Zealand, and the Australian Government National Health and Medical Research Council.