
Abstract
The approval of the Spanish Law for the Regulation of Euthanasia in March 2021 entails a profound social change that has direct implications for professional practice at all levels of care. There is no information available about the experiences of the professionals participating in the process of implementing the law in our country, nor any guide as to what might represent good practices in euthanasia in the context of the Mediterranean countries. Due to the complexity of the concepts often associated with assisted dying processes (such as suffering, dignity and moral compass), it is essential that systematic and detailed research be conducted on how professionals understand their experiences of euthanasia, and that it be conducted during the initial stages. We intend to carry out a qualitative study with a constructionist orientation to gain insight to the social constructs underlying professionals’ initial experiences. It consists of a series of in-depth interviews conducted in two phases: the first being exploratory and the second phenomenological. Sampling will be purposive and substantiated and have the following variation criteria: profession, age, and gender. Participants will be recruited through the Guarantee and Review Commission of Catalonia, and the scope of the study is all of Catalonia. We expect the participation of 31 professionals. The research will be conducted by a multidisciplinary team with the direct participation of researchers from different levels of healthcare, university research centers and civil society through all phases of the study. The expected results are: (a) A detailed description of the experiences of the professionals involved in the implementation of the law; and (b) The identification of the foundations for a guide to good practices in euthanasia in the Mediterranean setting.
Keywords
Background
With the 2021 approval of the Organic Law for the Regulation of Euthanasia (LORE), Spain became the first Mediterranean country to decriminalize assisted dying (AD) (Organic Law 3/2021, 24 March, 2021). This new legal framework entails a significant social change that directly impacts healthcare professionals, who have thus been called upon to rethink their care practice (Busquet-Duran et al., 2022; Sandham et al., 2022; Regional Euthanasia Review Committees, 2021). There is extensive literature on the influence of the euthanasia process on those participating in it. Nurses describe it as a “serious and difficult process”, both on a practical and organizational level, as well as emotionally and morally (Denier et al., 2010). They report it being characterized by strong ambivalence (Bellens et al., 2020; Denier et al., 2009; Pesut et al., 2020). For their part, doctors may feel pressured (de Boer et al., 2019) and often report experiencing conflicting emotions (Evenblij et al., 2019). There are many ethical, legal, regulatory, clinical, personal, and political implications entangled in this new understanding of the medical practice. As with any major social change, there are a wide variety of arguments supporting maximalist positions (Altisent et al., 2021).
Death and dying are legally regulated, shared social phenomena. According to the canon of death, a good death is painless, taking place at home, swiftly, while sleeping or unconscious and surrounded by loved ones, having reached old age (Marí-Klose & Miguel, 2000) yet still enjoying some minimum standards of quality of life (Fernández et al., 2022). This does vary, of course, depending on the sociocultural framework in question, as can be clearly seen various pieces of legislation. Assisted dying has neither been regulated in the same way, nor does it include the same practices in Belgium, Holland and Oregon. Euthanasia is allowed in Belgium and Holland while physician-assisted suicide (PAS) is rare. Conversely, in Oregon, euthanasia is not allowed, but PAS is (Velasco Bernal & Trejo-Gabriel-Galan, 2022). In Spain, there is broad support for euthanasia. It dwindles however when PAS is laid on the table, thus suggesting that suicide in any form is banned from the collective imagination (Serrano-del-Rosal & Heredia-Cerro, 2018). On the other hand, in more traditionally liberal societies, PAS is accepted while euthanasia is not because supra-individual institutions (whether governmental or religious in nature) bend more to individual freedom (Serrano-del-Rosal & Heredia-Cerro, 2018). The fact that the term “suicide” does not appear in the LORE at any time is illustrative. Yet another example is that while nurses are recognized as professional evaluators and providers of assisted dying in Canada (Dierckx de Casterlé, 2006; Pesut et al., 2020), the LORE does not even mention the role of these professionals. Upon digging deeper into these sociocultural differences, it becomes clear that there are significant gender differences in how people face death (Yakimchuk, 2019). Women are more likely to provide advance directives and request that life-prolonging treatments be discontinued (Antolín et al., 2014; Fletcher et al., 2013; Saeed et al., 2018; Smets et al., 2012), while men are more greatly associated with continuous palliative sedation and euthanasia (van Deijck et al., 2013). This can be explained in part by differences in coping mechanisms as imposed by gender norms (Dalmau-Bueno et al., 2022; Gaston & Mitchell, 2005; Seifart et al., 2020; Skulason et al., 2014; Ullrich et al., 2019).
Only by understanding these different styles and traditions can a phenomenon such as assisted death be approached. It should be noted that there is evidence of non-medical AD practices in rural areas. One such example would be the “terminator” in Sardinia, a figure who ends the lives of those in agony (Murgia, 2020). AD used to be performed as a clandestine and illegal practice in Spain: an online survey completed by 390 nurses in Andalusia in 2010 revealed that 22.6% believed that cases of euthanasia had occurred and 11.4% believed assisted suicide had (Tamayo-Velázquez et al., 2012).
Criteria for eligibility for AD.

Legal steps for Assisted Dying.
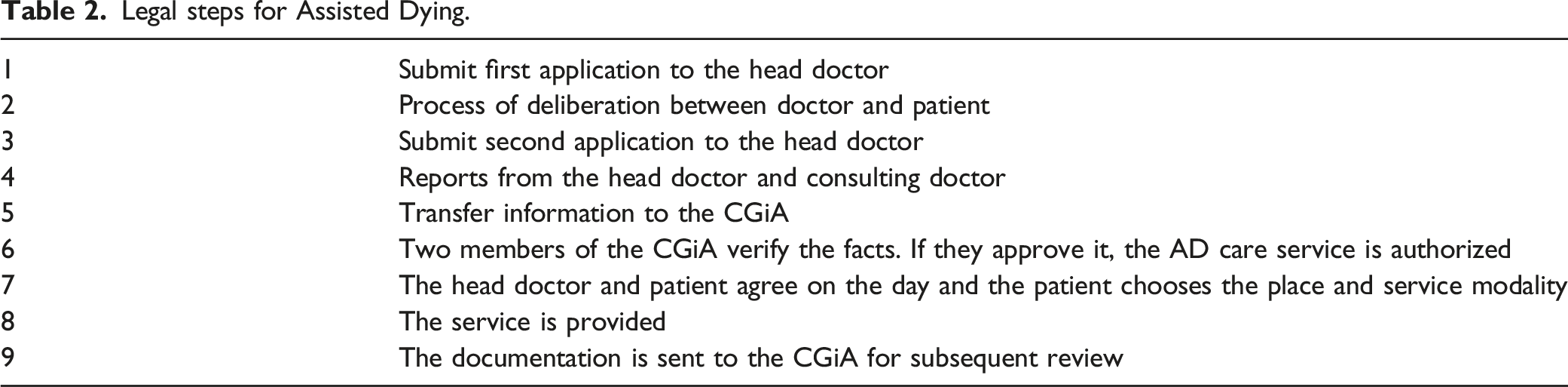
The Catalan model establishes a multidisciplinary CGiA and the creation of a euthanasia support office (the PRAM Office) and a network of regional references (Decree-law 13/2021, 2021; Departament de Salut. Generalitat de Catalunya, 2021). The CGiA is composed of three professionals from the field of medicine, three from law, two from nursing, one from psychology, one from social work and a representative of civil society. The PRAM Office performs the administrative functions necessary for the continuity and development of the CGiA’s remit. For their part, the regional, primary care and hospital references support the doctors and consultants responsible in both the procedure and the more administrative aspects.
Differences between natural and planned death.

Health, illness and death are social constructs with deep-rooted meanings and symbolism. In our setting, AD is a new, little known or studied phenomenon with a strong subjective burden. It is therefore appropriate to conduct research with a social constructionist perspective and qualitative methodology to better understand these emerging meanings in the current Catalan context since: 1. Death and dying bear an enormous subjective burden. A qualitative study conducted among Dutch doctors objectifies the tension that may arise between the doctor’s own opinions on death and dying and the patient’s preferences (Ten Cate et al., 2017). Quantitative studies have demonstrated that the reasons for requesting euthanasia are strictly subjective (pointless suffering and loss of dignity) (Jansen-van Der Weide et al., 2005), that the desire to advance death is related to spiritual and psychosocial discomfort (Busquet-Duran et al., 2021; Stolz et al., 2017; Van Den Berg et al., 2021), and that the greatest challenge reported by doctors regarding euthanasia is assessing whether or not the suffering expressed by the patient is unbearable (Buiting et al., 2008). In our setting, nearly 10% of patients with advanced cancer receiving palliative care verbally express the desire for AD (Busquet-Duran et al., 2021; Güell et al., 2015). 2. AD involves meanings created by the people, groups and community involved which, in turn, are embedded in a set of social relationships and a specific sociopolitical context. For example, different religions vary in how they deal with this process (Sobrevia & Torradeflot, 2014), and the European Association for Palliative Care is openly against it (Kelly et al., 2020). It is necessary to understand the perceptions, meanings, and behaviors of the various actors involved. Accordingly, Timoty Quill studied the limits professionals set when it comes to meeting patients’ perceived needs, as well as their moral compass (Quill, 2018), given the deep displacement of values (Beuthin et al., 2018; Dholakia et al., 2022; Lavoie et al., 2015; Stevens, 2006). One qualitative study shows the difficulty that Dutch doctors experience when they go from being seen as caregivers involved in the patient’s health to simple interpreters of the law, facing requests for euthanasia based on non-medical reasons (Snijdewind et al., 2018), such as mental health issues (Evenblij et al., 2019; Pronk et al., 2021; Verhofstadt et al., 2022) or when the patient is not competent at the time of the request (Kouwenhoven et al., 2015; Variath et al., 2022). 3. The participation of professionals directly involved in the phenomenon is essential. A systematic review of mixed studies concludes that euthanasia decision-making should be framed within the patient-professional-family triad (Roest et al., 2019) and that the approach to shared decision-making should be more contextualized (Gómez-Vírseda et al., 2020). Another recent qualitative study conducted in Canada shows how the legal possibility of AD leads to profound changes in expectations and how palliative care units work (Gómez-Vírseda et al., 2020). Ultimately, the aim is to understand the experience in order to design intervention programs that take it into account and incorporate self-care for the professionals involved. Although AD is requested in few cases (Emanuel et al., 2016), it can have a huge impact on professionals (Kelly et al., 2020).
In Spain, news stories are being published about how both patients and family members, as well as professionals, are dealing with the euthanasia process (Macpherson, 2021, October 28). One recent study points to the need for training and emotional support for healthcare professionals (López-Matons et al., 2021). However, we are not aware of any research that offers systematically collected evidence or data on the experiences of professionals involved in euthanasia in Spain or on what good practices should look like for euthanasia in Mediterranean countries.
Explanation and Justification of Method
Aim
This study aims to analyze and understand the full range of experiences and implications of health professionals when providing care to someone who chooses AD, as well as to identify the foundations for good practices in this area.
Specific Aims
• Analyze the main ethical dilemmas of health professionals in Catalonia participating in the provision of AD. • Understand professional and personal experiences related to the implementation of the euthanasia process in Catalonia. • Identify and define key elements for good practices from the perspective of the professionals involved in the AD process during the first year of implementation in Catalonia.
Method
We propose an exploratory qualitative study with a constructionist focus, based on a series of in-depth interviews with professionals involved in the euthanasia process (Eatough & Smith, 2008; Langdridge, 2007). The study period is from June 2022 to June 2024 in Catalonia.
Recruitment and Participant Selection
The study population comprises health professionals involved in the euthanasia process. The exclusion criterion is having serious emotional trauma (diagnosed or otherwise) that makes reliving traumatic experiences unadvisable.
Participants will be recruited and selected using snowball as well as maximum variation sampling (Moser & Korstjens, 2018) as regards the sample criterion of involvement in the process of implementing the law. Recruitment will be performed in agreement with and through the CGiA of Catalonia. Moreover, the final selection of participants will be done taking into account the variables of professional profile, gender and age. Selection will be purposive, substantiated, and deliberate to collect a wide diversity of experiences and implications linked to the phenomenon under study. To this end, participants in the exploratory interviews will be asked to suggest any profile or individuals they consider should be included in a second phase sample. Also, professional profile (medicine, nursing, psychology, pharmacy, social work, administrative support and law), setting (hospital, primary care, impatient rehabilitation facility, administration), sector (public, private), area (urban, rural), region (Barcelona, Girona, Tarragona, Lleida), experience (satisfactory, non-satisfactory) will be considered segmentation criterion, and the following variables will be taken into account as sample variation criteria: age, gender (including non-binary), and religion. An estimated sample of 31 participants is expected, distributed throughout the field work as follows:
Phase 1: Exploratory
Five in-depth interviews with key informants: These would be participants belonging to the CGiA of Catalonia since they represent most of the professional profiles involved in the process (medicine, nursing, social work, psychology and law) and have an overall view of the implementation of the law throughout the whole territory. These interviews would be aimed at identifying the main elements to consider in subsequent interviews, corroborating the various professional profiles to be interviewed, and gaining access to them for the following phases.
Phase 2: Phenomenological insight
In this phase, sample size will be determined by data saturation. The initial plan is to conduct 26 in-depth, iterative interviews. Although there is a tendency to opt for even smaller samples in phenomenological studies to avoid generating a general cacophony that obscures the richness of each participant’s voice (Bartholomew et al., 2021), this study has an exploratory focus of the phenomenon and a broad approach to the category of “professional”. It is therefore necessary to include a wide diversity of profiles and, simultaneously, anticipate the possibility of interviewing participants more than once (Malterud et al., 2016). We thus hope to capture a holistic and dense description of the experience of professional involvement in the euthanasia process. In any case, the interviews will be conducted sequentially so that the principles of qualitative research (flexibility, openness and iteration) can be implemented and the point of data saturation can be clearly and rigorously established.
The initial plan is to conduct seven medicine, seven nursing, three psychology, two pharmacy, three social work, two administrative support and two legal interviews. Two subphases are foreseen: a. The first includes the seven professional profiles identified to gain a general perspective of the main themes structuring the experience of professionals. b. And the second phase includes the remaining interviews, until reaching the discourse variation sought out and data saturation.
Data Handling
Experiences, opinions and perceptions will be collected through semi-structured, in-depth interviews. Informed consent will be obtained. Audio will be recorded with a digital voice recorder and the data will be stored locally. The interview questions are aimed at establishing a dialogue from which in-depth and contextualized information can be extracted, without inciting or forcing answers (Additional file 1).
The interview scripts will be approved by the research team and tested and revised during the first phase of the study. Modifications and corrections will be made as necessary; the results of these first interviews will not be dismissed. The interviews will be transcribed, eliminating any identifying traces, and transferred to the Atlas.ti Web software for qualitative analysis (which can be worked on collaboratively). Participants from the first phase will be invited to contact the researchers for a second interview if they have more to contribute.
The interviews will last approximately 40–90 minutes and will be conducted at the participants’ workplace or in a room at the Barcelona Medical Association.
The project is expected to last 22 months, with varying involvement of the participating entities and coordinated by the Principal Investigator and his research group, with the support of a contracted professional technician with advanced knowledge of qualitative methodologies.
Project chronogram.
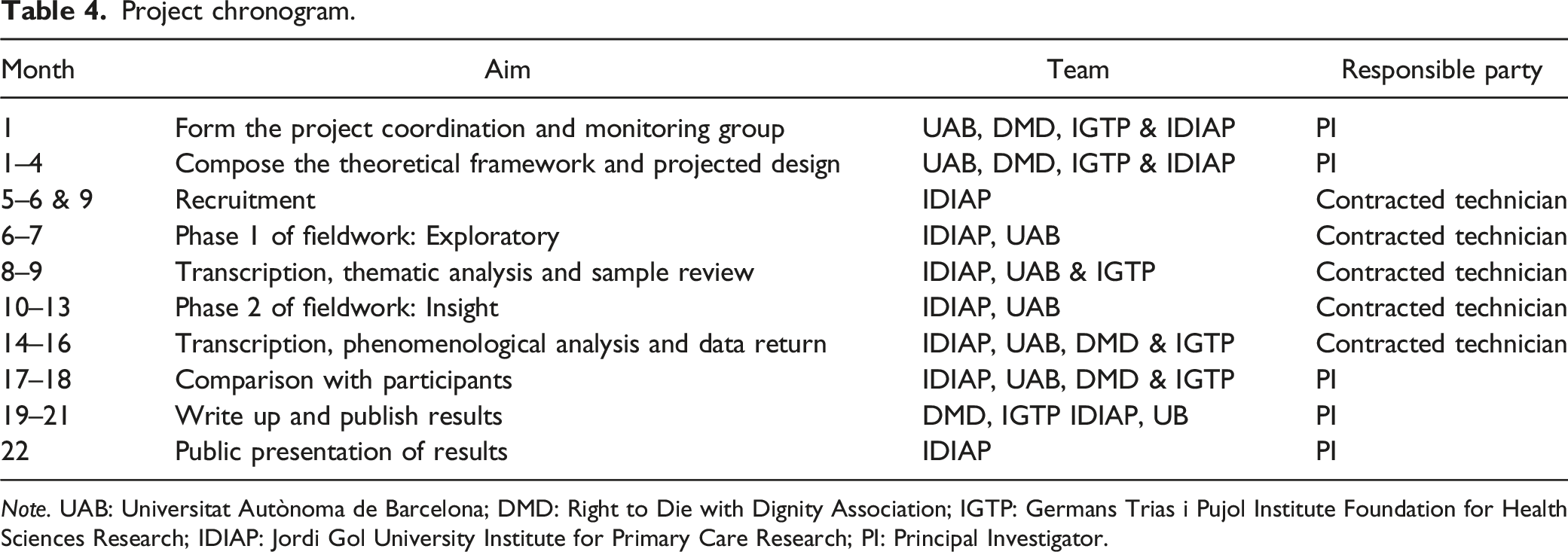
Note. UAB: Universitat Autònoma de Barcelona; DMD: Right to Die with Dignity Association; IGTP: Germans Trias i Pujol Institute Foundation for Health Sciences Research; IDIAP: Jordi Gol University Institute for Primary Care Research; PI: Principal Investigator.
Data Analysis
In the first phase, a reflective thematic analysis based on Braun and Clarke will be conducted (Braun & Clarke, 2006). In the second phase, the standard interpretative phenomenological analysis procedure will be followed (Pietkiewicz & Smith, 2014; Willig, 2008): 1. Multiple readings of the transcription and making notes 2. Identification of emerging themes 3. Clustering the themes
To ensure the analytical process is rigorous, the researchers will triangulate their work, independently reading each interview as transcribed verbatim from audio recordings and then sharing their codifications with each other to reach a consensus. Lastly, the interviewees will participate in triangulation (member checking) both individually and at a collaborative analysis workshop, where a narrative summary of their stories will be presented for comparison and validation.
Rigor
The interviewers will use established qualitative standards to ensure reliability and rigor, in accordance with Thorne et al. (2004). The research team will approve the scripts, drawing on the external and expert perspective of the institutions participating in the project. It should be noted that describing the experiences inevitably involves the perspective of the research team, which is clearly positioned in favor of facilitating the exercise of this new right. Therefore, it will be necessary to manage the biases of those in a dual position: researcher and member of the study population. Credibility will be enhanced by asking participants to review the preliminary findings and involving them in the analysis and creation of proposals and documents.
Ethics
All the researchers and collaborators undertake to strictly observe the Declaration of Helsinki. Participants must sign an informed consent form and will be identified exclusively by code. Only the data controller will have access to the list of participant names, date of inclusion and study codes. All the information obtained will be treated confidentially, in compliance with Spanish Organic Law 3/2018, of December 5, on personal data protection and guarantee of digital rights, and Regulation (EU) 2016/679 of the European Parliament and of the Council, of 27 April 2016, on the protection of natural persons with regard to the processing of personal data and on the free movement of such data (GDPR): 1. Identification of the data and the subjects processing them: Qualitative data (opinions, etc.) will be obtained from interviewees voluntarily once consent has been granted and in the context of the interview. If, in the course of the conversation, data that may identify the participants be provided, the research team will anonymize them by removing them from the file using an audio editing program (Audacity) or replacing them with pseudonyms or generic categories (for example, “city”) when transcribing the interview. If the transcription is commissioned to people outside the research team, they will be provided with the pseudo-anonymized data and a confidentiality agreement will be signed. 2. Identification and legitimate basis of the data processing: The variables required to conduct the study will be obtained directly from the project participants with their consent, in accordance with the provisions of articles 6.1.a) and 9.2.a) of the GDPR. 3. Data processing tools: Data will be stored locally on the computers of the health centers and on the Cercles platform of the Government of Catalonia. Transcriptions and coding will be performed with locally installed software. 4. International data transfers: International data transfers are not foreseen. 5. Identification of processing that may pose a significant risk to the rights and freedoms of research participants: No processing that may pose a risk to the rights or freedoms of the participants will be applied. The interviews will be recorded and transcribed but the content of the recordings will be stored securely (password protected and accessible only to members of the research team) for 2 years, at which point it will be deleted. Participants will be able to review their interview transcripts.
We follow the ethical criteria for medical research proposed by Emanuel: scientific and social interest, scientific validity, fair subject selection, a favorable risk-benefit ratio, independent review, informed consent and respect for subjects (Berenguera-Ossó et al., 2014; Emanuel et al., 2000).
Discussion
Expected Results
We expect to identify key themes such as: 1. Positive reinforcement from within the profession by providing comprehensive care, championing patient choice and supporting a good death as defined by the patient. 2. A pioneering and innovative spirit and a sense of involvement and belonging in responding to the many emerging questions posed by the new legislative scenario. 3. A clear personal, ethical, and emotional impact related to the underlying values and practice of AD.
In terms of good practices, the following aspects may stand out: 1. The importance of technical and pharmacological skills 2. The need for good communication skills 3. The importance of teamwork and coordination between care levels 4. The need for specific psychological support 5. The need to create safe spaces for ethical and moral debate.
Transferability, Applicability And Opportunity Of The Proposal
The results will be transferable to the entire Mediterranean region and, especially, the other autonomous communities of Spain, where the law has been implemented in very different ways. For example, in the first year of implementation, 60 applications were accepted in Catalonia, while only 11 were accepted in Andalusia, a region with one million more inhabitants (Linde, 2022; Sanz, 2022).
At the level of healthcare, the results may contribute to the collective construction of good practices to understand and provide AD (Pesut et al., 2020) and help remodel and empower the practice of palliative care, from a systemic understanding revolving around death and dying (Sallnow et al., 2022).
At the level of training, the emotional and ethical nature of AD will have to be fundamentally addressed. The results will have implications for mandatory minimum education and could become the basis for developing training packages based on experience and co-design.
Professional and institutional leaders will need to be at the forefront to ensure that professionals understand and feel prepared to respond to the situations that patients and their families present, bearing in mind that dynamic changes are likely to occur as different aspects of the legislation are questioned (Carnevale, 2013; Vargas-Celis & Concha-Méndez, 2019).
At the policy level, our findings will likely suggest that we need to continue to advocate for patient choice at the end of life, promoting compassionate, informed and non-judgmental patient care, while making a major effort to improve access to quality palliative care and adequate support for the staff involved in implementing it.
In addition to scientific publications and congresses, we plan to disseminate the results to various professional, patient and citizen associations, as well as through press releases, the media, and policy briefs.
Lastly, the methodology and results may serve as a basis for future research since they paint a picture of the initial situation.
Supplemental Material
Supplemental Material - Implementation of Assisted Dying in Catalonia: Impact on Professionals and Development of Good Practices. Protocol for a Qualitative Study
Supplemental Material for Implementation of Assisted Dying in Catalonia: Impact on Professionals and Development of Good Practices. Protocol for a Qualitative Study in Maria Verdaguer, Núria Vallès-Peris, Xavier Busquet-Duran, Eduard Moreno-Gabriel, Patricia Beroiz, Antonia Arreciado Marañón, Maria Feijoo-Cid, Miquel Domènech, Lupicinio Íñiguez-Rueda, Glòria Cantarell and Pere Torán-Monserrat in International Journal of Qualitative Methods
Footnotes
Author Notes
Two of the authors, Xavier Busquet-Duran and Patricia Beroiz are references for euthanasia in their area of work, the first in primary health care and the second in a third-level hospital. Glòria Cantarell was president of the DMD Association and is currently the vice president.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project was awarded a grant from the Strategic Plan for Research and Innovation in Health (PERIS) 2016-2020, aimed at primary care research, of the Department of Health of the Government of Catalonia, ref. SLT021/21/000046. The funder is not involved in designing aspects of the study, but the study proposal underwent competitive peer review through a formal peer-review process.
Ethical Approval
Ethics approval for the study has been received by the IDIAP Jordi Gol Independent Ethics Committee (IEC/IRB). Project ID: 22/094-P. Participants who have been recruited for this study have provided consent in writing.
Data Availability
The datasets used and analyzed during the study will be available from the corresponding author upon reasonable request.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.