
Abstract
Moderate-to-severe hypoxic-ischemic encephalopathy (HIE) is a significant cause of neonatal mortality and permanent disability in surviving newborns. Therapeutic hypothermia (TH) is the only effective intervention to reduce these outcomes. Being a parent of these babies is a traumatic and strenuous event. To address these difficulties, parents need information and support. The aim of this article is to describe a qualitative methodological process followed to develop a guide for parents of a newborn with HIE receiving TH as an addendum to clinical practice guidelines. The guide based on the experience of parents of newborns with HIE is presented as 16 meaningful questions and a glossary. It provides information to parents about HIE, treatment and care, future outcomes, and coping strategies. The final version, in Spanish and English, has a didactic format with simple wording, parents’ verbatim queries, and illustrations made expressly for the guide. Furthermore, we think showing the methodological process we followed to develop the guide, detailing the difficulties that arose in doing so, and making the reflexivity of the researchers explicit may provide support for other teams undertaking similar projects. Likewise, this article illustrates in a practical way how the perspective of family can be incorporated into clinical practice guidelines.
Keywords
Introduction
Clinical practice guidelines (CPGs) are a set of recommendations regarding the care of patients with a specific clinical condition. They are developed from systematic reviews of evidence and an assessment of the risks and benefits of therapeutic alternatives. CPGs enable organization, evaluation, and grading of the available knowledge to facilitate sound clinical decision making by health care professionals and to improve patient choice (Steinberg et al., 2011).
The participation of actors such as users or families in the preparation of a CPG is recommended by the main CPG development groups including the National Institute for Health and Care Excellence (NICE) and Scottish Intercollegiate Guideline Network, but implementation in practice is scarce. For this reason, since 2000, these groups and other organizations such as the Guideline International Network Patient and Public Involvement Working Group have been developing various strategies to promote this methodology (Boivin et al., 2010).
In 2012, an interdisciplinary group of professionals from different Spanish university hospitals, under the auspices of GuiaSalud and with a grant from the National Health Service of Spain, began development of a CPG on the management of the newborn with perinatal hypoxic-ischemic encephalopathy (HIE) using grading of recommendations, assessment, development and evaluation (GRADE) methodology as the system to evaluate the quality of the evidence and to measure the strength of the recommendations (Del Río et al., 2015). Simultaneously, part of the team initiated a guide for parents of newborns with HIE needing treatment with therapeutic hypothermia (TH) to be included as an addendum to this CPG. The parents’ guide was designed as a tool to respond to the needs of families for information and support concerning their child’s hospitalization, based on the experience of families having undergone this situation (Herranz et al., 2014). Finally, in 2015, the CPG on perinatal HIE, including the parents’ guide, was published in Spanish and English (Working group Involved in the Development of Clinical Practices Guidelines, 2015).
Qualitative research allows us to understand the experience of people with regard to health–disease processes and the impact on their lives from their own perspective (Denzin & Lincoln, 1994). Evidence from the synthesis of qualitative studies, or primary studies, is a tool for integrating knowledge about people’s values, priorities, and preferences in CPG (Carroll, 2017; Tan et al., 2009).
The bibliographic review carried out to prepare the CPG revealed a lack of qualitative research on the phenomenon of study. To address this, we undertook a qualitative investigation to explore what families undergo during the hospitalization of an infant with HIE and identify the elements that the guide should contain from their perspective (Díaz Del Campo et al., 2011; Working Group of Patients Involved in the Development of Clinical Practices Guidelines, 2010). This article reports the methodological process followed to develop the guide for parents of a newborn with HIE and TH.
Background
HIE is an acute neurological dysfunction of variable severity that appears immediately after birth as a result of lack of oxygen and/or perfusion in the fetus or newborn (García-Alix, 2009). Moderate-to-severe HIE is an important cause of morbidity and mortality in the neonatal period and permanent disability in surviving newborns. The incidence of HIE presents significant from country to country for which statistics are available. The figures range between 1‰ and 6‰ of newborns in the countries with greater resources (Lawn et al., 2008), and it is estimated that up to 25% of newborns and 8% of deaths in children under 5 years of age are related to this clinical condition in countries with fewer resources (Eunson, 2015). In view of this, HIE is a relevant health problem worldwide.
In the first decade of this century, meta-analyses of clinical trials showed that TH, reducing brain temperature by 3–4 °C through cooling of the whole body or the head, is a safe and effective intervention to reduce the mortality and disability associated with HIE (Edwards et al., 2010; Jacobs et al., 2007; Shah, 2010; Tagin et al., 2012). Since 2005, TH has been progressively introduced into neonatal units worldwide to become established as the standard treatment for moderate-to-severe HIE in the newborn (Azzopardi, 2010; Blanco et al., 2011; Lemus-varela et al., 2016; NICE Interventional Procedure Guidance [IPG347], 2010; Peliowski-Davidovich et al., 2012).
The birth of a newborn with moderate-to-severe HIE is an emergency requiring urgent care in a neonatal intensive care unit (NICU). Generally, this implies the immediate transfer of the newborn to a hospital with a TH program and entails the separation of the family unit.
The emotional impact on the parents of a newborn hospitalized in the NICU, regardless of their health condition, has been explored in several systematic reviews. These reviews have revealed that parents experience stress, depression, guilt, and loss of control, among other emotions (Al Maghaireh et al., 2016; Cleveland, 2008; Obeidat et al., 2009).
Concerning the families of a newborn with HIE, during the development of the guide, we found no studies specifically exploring this situation. One year later, two Swedish studies (Heringhaus et al., 2013; Nassef et al., 2013) revealed that being a parent of a newborn with moderate-to-severe HIE is a strenuous process. Parents experience an initial shock due to the severity of the newborn’s condition, NICU admission, and family separation. Other factors such as fear of the baby’s death, uncertainty about the prognosis, and difficulty caring for a baby that may have sequelae act synergistically, causing feelings of sadness or hopelessness and engendering significant stress (Nassef et al., 2013). These circumstances intimidate parents, causing them to feel afraid to interact affectively with their child and to bond (Aagaard & Hall, 2008; Heringhaus et al., 2013; Nassef et al., 2013). Bonding is an adaptive resource, which is formed early and reciprocally between parents and children. It is essential for the child’s cognitive and emotional development, and it prepares parents for coping difficulties and contributes to fostering family mental health in the long term. To address these difficulties, parents need coping tools (Sullivan et al., 2011).
Several studies have documented the usefulness of information as a resource to help parents to situate themselves in reality to improve their control of the situation and to become empowered in decision-making. And because of this, it can potentially cushion stress and improve coping skills (Cleveland, 2008; Staniszewska et al., 2012; Wigert et al., 2013).
The information needs of parents in the NICU are complex (De Rouck & Leys, 2009; Harvey et al., 2013; Staniszewska et al., 2012), especially in the case of a newborn with HIE (Azzopardi, 2010; Working Group Involved in the Development of Clinical Practices Guidelines, 2015). The serious illness, the uncertainty and provisional nature of the news, coupled with the emotional vulnerability of the parents and the difficulty in assimilating and retaining information, combine to make the process of providing information a challenge for professionals (De Rouck & Leys, 2009; Harvey et al., 2013; Orzalesi & Aite, 2011).
Parents with a newborn in the NICU need the most current information about the disease, its treatment, and the care their child is receiving. They appreciate when this is honest, complete, and continuous. They need for it to be presented in simple language and positively value written resources (Brett et al., 2011; Janvier et al., 2014; Orzalesi & Aite, 2011).
Therefore, having a written guide for parents which provides specific information about HIE and TH, in a didactic format and drawn from the experiences of families who have undergone this same situation with their children, may be useful to respond to the information and fulfill the needs of parents of a newborn with HIE (Herranz et al., 2014). The objective of this article was to describe the methodological process followed in developing a guide for parents of a newborn with HIE and TH.
Approach to the Research Design
The experience of parents of a newborn with HIE who requires treatment with TH was a phenomenon of complex and unexplored nature at the time of the preparation of the parents’ guide. This led to the decision to conduct a phenomenological study based on the constructivist paradigm to explore and understand the experience of parents during the hospitalization of their child and to identify the elements that the guide should include (Morse, 2003).
The research design was constructed considering this as a process ranging from the conceptualization of the problem to the drafting of the findings (Creswell, 1998). Guidelines for conducting qualitative studies established by consolidated criteria for reporting qualitative research were followed (Tong et al., 2007). Our research team consisted of a psychologist, V.V. (PhD), a neonatal nurse, N.H.-R. (PhD St), both with knowledge and training in qualitative methodology, and two neonatologists, A.B. (PhD) and A.G.A. (PhD), with knowledge of and experience in quantitative and qualitative research. The researchers kept reflexivity in mind at the theoretical–practical and ethical levels during the duration of the investigation to identify how their attitudes could have an influence in the field and to argue transparently the decisions taken in the process (De La Cuesta-Benjumea, 2003). A continuous dialogue was established between the elements projected for research (before entering the field) and those that took place in the research process. This feedback allowed us to identify situations that made it necessary to reconsider elements of the project, molding the emerging design (Denzin & Lincoln, 1994), and also determining the need to use creative strategies such as the development of an ad hoc instrument to obtain the data (Janesick, 2001). This reflexivity was used as a tool to ensure the rigor, credibility, and internal validity of the research (Tracy, 2010), and it revealed how the researcher is an instrument in their own research (De La Cuesta-Benjumea, 2003).
Making of the Parents’ Guide
The process of constructing the guide for parents of a newborn with HIE and TH treatment was conducted in four stages. In the first preparatory stage, before entering the field, an ad hoc instrument was designed for data collection. In the second stage of immersion in the field, the data were collected, and in the third analytical stage, the decisions were made regarding the contents of the guide, which was then developed in the final stage. Figure 1 shows the flexible, reflexive, and circular process followed in the design of the guide.

Process followed in the design of the guide.
Stage 1: Before Entering the Field
The research team made an important discovery when they observed the emotional difficulty parents had in discussing their experiences during the first contact by telephone with them. At this moment, researchers began to consider parents as participants in “sensitive research” and, as such, at risk of experiencing emotional stress, derived from recounting painful elements of their experience during interviews (Sieber & Stanley, 1988). And they made the decision to replace the interview script with another resource to obtain the data using a visual instrument. The design of this instrument was developed in three stages.
(a) Development of a conceptual map. Following abductive reasoning (Given, 2008), the neonatal nurse, N.H-R., prepared a conceptual map to outline the path that a newborn with HIE and TH and their parents follow from birth (Vasilachis de Gialdino, 2006). Key elements that could be significant in characterizing the experience of a newborn and their parents from a complex and multidimensional perspective (disease, illness, and sickness) were identified and are illustrated in Figure 2. As illustrated in Figure 3, the conceptual map was a cross-sectional methodological tool with different applications to delineate the research project.
(b) Bibliographic review. The constructs identified in the conceptual map were considered descriptors to guide a systematized search of the bibliography (Grant & Booth, 2009). Searches were carried out in PubMed, PsycINFO, and CINAHL with the equations: hypoxic ischemic encephalopathy AND parents OR family; neonatal intensive care AND parents coping; family OR parents AND intensive care unit AND newborn; parenting AND intensive care nursing AND newborn; neonatal intensive care AND stress AND newborn.
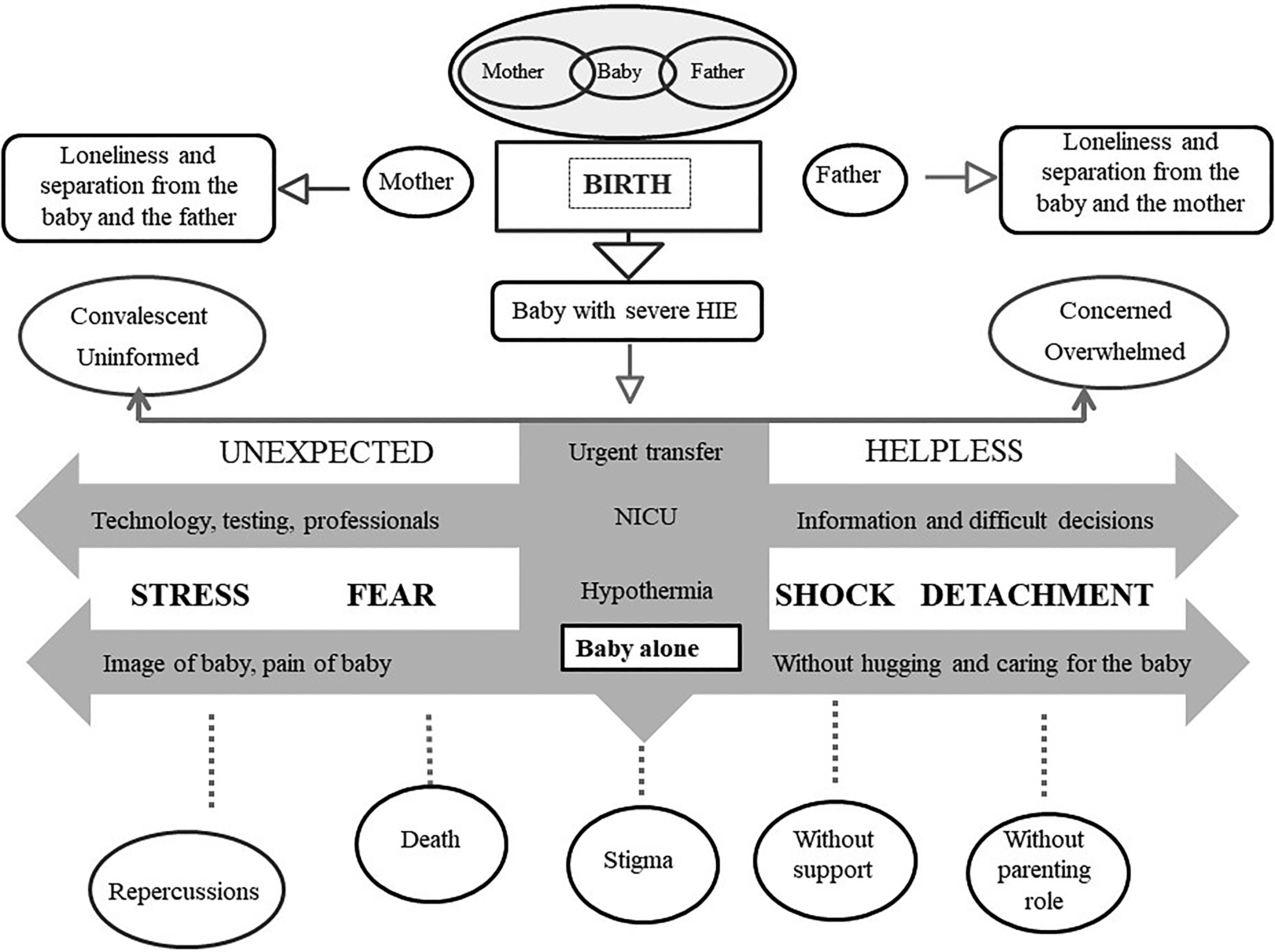
Experience of a newborn and their parents.

The conceptual map as a methodological tool.
Two of the researchers (V.V. and N.H.-R.) conducted a first reading of the abstracts of the items found and developed bibliographic records and a system of inclusion criteria for assessing the relevance of reading or rejecting the full articles. The articles read did not provide direct evidence about the experience of parents with a newborn with HIE and treatment with TH, but they did yield intermediate results such as the emotional experience of parents with a newborn in the NICU, effective interventions to foster the parental role, and coping strategies. These results allowed us to establish a system of theoretical categories and subcategories that illustrated thematic units that were used to develop the interview script.
(c) Design of an ad hoc photographic script. A script with 20 ad hoc photographs was produced as the main instrument for gathering the data and replacing the classic interview script. The use of photographs is a resource employed in qualitative research to evoke memory and facilitate the narrative of participants during data collection (Given, 2008). According to Sclater (2003), the photographs act as triggers that assist in connecting abstract ideas in specific situations and enable uncovering what is not normally discussed (Barone & Eisner, 2006; Sclater, 2003). In our study, it was a technique to generate a narrative around the themes associated with the images previously identified by the researchers.
The researchers, N.H.-R. and V.V., agreed on the content that the photographs should have in order to adequately represent the theoretical categories and subcategories that they wanted to explore according to the objectives of the research. For this purpose, they considered the information of the designed concept map (Figure 2) and that obtained in the bibliographic search. A third researcher, A.B., an expert on the subject, reviewed this process and enriched it with his contributions. All together examined how selected photographic themes were representative of theoretical categories and subcategories we sought to explore. Also, they designed the elements in content and form that the photographs should have. Table 1 illustrates the relationship between the photographic themes and the theoretical categories. The digital photographs were based on these topics and had been taken in the NICU of one of the participating hospitals by a professional photographer, following the precise instructions of researchers N.H.-R. and V.V. who accompanied him during the photo shoot. Signed consent was obtained from families whose babies appeared in the photographs. Finally, of the 30 photographs taken, N.H.-R., V.V., and A.B. selected 20 images that would make up the final photo script. The decision was made based on the richness of the elements of the photograph in showing the topics representative of theoretical categories and subcategories that were to be addressed in conjunction with the interview questions. This strategy allowed a broader understanding and a more holistic look at the experiences of the parents.
Photographic Themes and Theoretical Categories/Subcategories.

Note. HIE = hypoxic-ischemic encephalopathy; NICU = neonatal intensive care unit.
Stage 2: Access to the Field and Data Collection
Characteristics of participants and researchers, and settings
The study was carried out in two neonatal units of tertiary hospitals in Barcelona (Spain) between January 2012 and December 2014. The two units shared a hypothermia program and treat an average of 30 newborns per year.
In order to select the participants, the records from a prospective study on HIE being carried out in these units were used (Alsina et al., 2017). The newborns were stratified according to the severity of HIE, the sequelae, and their age at the time. We performed an intentional sampling with the following criteria: Mothers and fathers of a newborn with HIE and TH who had survived the treatment and those who had an adequate command of Spanish. From the start of the TH program in 2010 to January 2012, 27 newborns met the inclusion criteria. Of the 21 families found, 9 (7 fathers and 9 mothers) agreed to participate in the study. Of the rest, 4 had no time availability and the remaining 8 refused to participate (4 were in the process of mourning the recent death of their children).
Contact with the families was facilitated by the coordinator of the TH program and made by one of the researchers (N.H.-R.) by telephone. In a preliminary conversation, the reason for the call was explained, and the parents were encouraged to participate; in a second call, the date and time of the meeting was arranged. Contact with the families revealed significant obstacles. On one hand, following the TH regionalization program, several families came from locations far from Barcelona, which complicated their participation. On the other hand, although at least 11 months had elapsed since treatment with HT, and even showing interest in participating in the research, some parents verbalized how difficult it was for them to recall the experience. In some instances, the investigator first received the news of the recent death of the baby during the telephone contact. Additionally, this emotional vulnerability of the families was confirmed when performing the first in-depth interview with a mother of a newborn with very serious sequelae. These circumstances were decisive in readjusting two elements of the design. First, we excluded those families who had children with very serious sequelae. Second, we decided to use the photographic script as a facilitator to conduct the interviews.
For this reason, only one in-depth interview was conducted with a Spanish mother of a newborn with HIE and very serious sequelae and two group interviews with families of children with moderate-to-severe HIE without major sequelae. Each focus group consisted of 15 participants (8 and 7, respectively), and in seven families, both parents were present. The families were middle class, of Spanish (11), Malian (2), and Colombian (2) nationality, and aged between 28 and 39 years old. Nine had university degrees, and six were secondary school graduates.
Ethical Considerations
The project (PIC108-13) was authorized by the clinical research ethics committee of the Sant Joan de Déu foundation affiliated with the University of Barcelona. The study was conducted in compliance with the ethical requirements set out in the Declaration of Helsinki (World Medical Association, 2013). Voluntary participation and confidentiality of data were ensured in accordance with European Union Directive 95/46/CE.
Data Collection
The focus group interviews were conducted in a building outside the hospitals in the period between May and June 2013. Beforehand, families were informed of the study objectives and the confidentiality of the data as well as the possibility of discontinuing their participation at any time. All participants agreed and signed the informed consent.
The interviews were moderated by two researchers: V.V., a psychologist who did not know any of the participants, streamlined conducting of the interviews, and a neonatal nurse (N.H.-R.), who knew some of the participants, supported in the collection of field notes as an observer. The sessions lasted 60–80 min, and were audio-taped, transcribed verbatim, and accompanied by field notes. The photographic script was the instrument used to obtain the data. Like other authors, the researchers took into account several special considerations when they planned how to conduct the focus group on sensitive topics (Dempsey et al., 2016). V.V. used the photographic script flexibly as a guide to facilitate meaningful discussion between the researcher and participants, allowing free flow of conversation. Rapport development was the key to facilitating the discussion of sensitive topics. The order of the 20 photographs was adjusted according to the difficulty of the subject and the speech of the parents in each focus group. Researchers considered the vulnerability of the families, and they were very careful to ensure parents were appropriately supported and could put off the topic till later or stop the discussion at any time for a break, switching off the audio recorder or terminating the interview if the parents became upset. The interviews began with an open-ended question of the type: “How does this image make you feel?” and “What does this picture suggest to you?” until all the images had been viewed and all the proposed topics addressed. These broad questions allowed us to explore the experience of each participant in a flexible manner. At the time of data collection, the age of the children ranged from 11 to 24 months. During the interviews, all parents had active participation and provide detailed and rich information about how they felt during the hospitalization of their newborn and what were their information and support needs. Once the focus group session ended, V.V. and N.H.-R. dedicated their efforts to creating a space, where participants could alleviate difficult emotions by providing relief and accompaniment. Likewise, as other authors have pointed out, we believe that participants see the interviews as an outlet to express intense emotions and reflect on the course of an illness (Lowes & Paul, 2006; McGrath, 2003), and the use of photographs has helped parents remember (Guiven, 2008).
In addition, in the weeks after the focus groups, N.H.-R. made telephone contact with families to explore their emotional state. Communication tools such as active listening, assertiveness, and empathy were used to provide emotional support to families. This contact allowed us to detect the usefulness of telephone conversations as a strategy to accompany parents who are facing the upbringing of a newborn who has had a moderate-to-severe HIE. In this regard, a proposal was made for families included in the TH program to have protocolized telephone contact in the future.
Stage 3: Analytical Stage and Decision-Making Regarding the Contents of the Guide
To adapt to the exploratory and descriptive profile of the study, V.V. and N.H.-R. performed an inductive content analysis. They did the analyses separately and then met to discuss their findings and agreeing on the final themes. This focused on describing the parents’ experiences and identifying their information and support needs. A systematic process was followed for identifying, coding, and categorizing textual data obtained in the interviews in order to reveal a priori patterns of hidden meaning, considering what is said, who says it, and how it is said (Mayring, 2000). Analysis began with an initial reading of the data performed to understand the overall meaning of the data and obtain the first units of meaning. A second careful reading allowed the first inductively generated codes to be established and classified according to the aims of the investigation. The codes were grouped according to similarity criteria and differences and grouped into categories and these into further subcategories. Ultimately, memos were written to refine the analysis (Elo & Kyngas, 2008). After that, N.H.-R. and V.V. compared their analyses. Deliberation regarding positioning and labeling of categories and subcategories was carried out until consensus was reached establishing credibility. The one-off differences were settled with the participation of the rest of the research team to increase trustworthiness. The data obtained in the first focus group identified the central issues and were enriched with the data obtained in the second. Data saturation was reached when no new themes emerged in the second focus group, considering that the study aims to identify core issues in data and to capture explicit concrete codes (Hennink et al., 2019).
Guided by the study objectives and the thematic units present in the photographic script, a map of categories and subcategories was developed, which in turn was transformed into the thematic index of the parents’ guide. This process was agreed upon in several sessions with the other researchers of this project. As an example, Table 2 illustrates the process followed to transform the information needs category with its subcategories into questions for the parents’ guide.
Example of Transformation of Information Needs Category and Subcategories Into Questions for the Parents’ Guide.
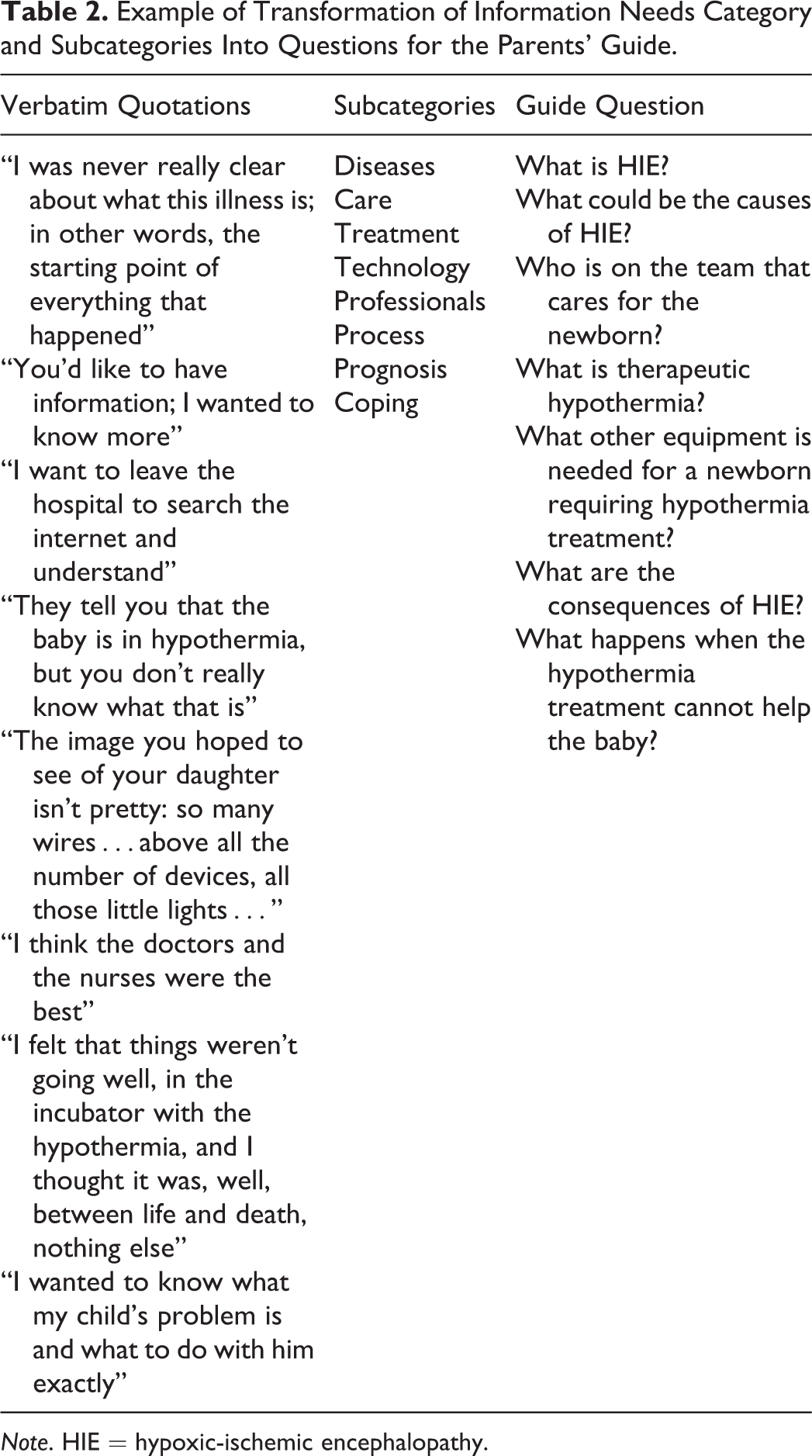
Note. HIE = hypoxic-ischemic encephalopathy.
Stage 4: Writing the Guide
Finally, as shown in Table 3, the contents that structure the guide were explained in 16 meaningful questions organized around four elements: the ABCs of HIE, treatment and care, outcome and help, and from A to Z.
Thematic Content of the Guide.

The drafting of the text was done jointly by V.V., N.H.-R., and A.B. Subsequently, several debriefing sessions were held with the CPG coordinator to refine the text until arriving at its final version. A relevant aspect was that the parents participating in the qualitative research received the guide draft in the mail and had the opportunity to contribute to the text.
The narrative structure followed a question–answer format with simple and instructional wording, avoiding technical terms as much as possible. To facilitate understanding of the information, a glossary was included with 41 words of biomedical jargon used in the NICU. Additionally, to support the contents of the guide, we included cross-referenced textual phrases of parents who participated in the study detailed in this article and specific illustrations made expressly for the guide (Working group Involved in Development Guide for Mothers and Fathers, 2015).
Why Do We Need This Kind of Tool in Clinical Practice With Families?
The CPG on perinatal HIE addresses a health problem of great importance due to the serious consequences for the child’s health and the overwhelming impact it has on families and society (Working Group Involved in the Development of Clinical Practices Guidelines, 2015). Incorporating a parent’s guide, developed from their own perspective, into a CPG aims to respond to the information and support needs of the families of newborns with HIE during the hospitalization of their child. Reaching this objective facilitates compliance with an essential right of the patient/family and potentially improves the quality and practical application of the CPG (Working Group of Patients Involved in the Development of Clinical Practices Guidelines, 2010). Involving users and families in the preparation of informational materials included in the CPG makes these more relevant and comprehensible for the families (Díaz Del Campo et al., 2011). Also, a recent systematic review proposed, by way of recommendation (moderate evidence), using these informational materials as strategies to reduce the anxiety and stress experienced by families of a patient in the intensive care unit (Davidson et al., 2017).
The stress the parents of these children experience can evolve into the form of chronic stress and prolonged mourning. This emotional dysfunction can alter the development of parent–infant bonding and hinder the already complex upbringing of a child with chronic health problems and special care needs (Lemmon et al., 2017). The situation negatively impacts family dynamics, the psychological health of caregivers, and the anguish of families (Al Maghaireh et al., 2016; Cleveland, 2008; Mesman et al., 2013).
Recent studies have shown that in addition to TH and the care the infant receives in the NICU, other factors such as the role of parents during child-rearing can affect the health outcomes of the newborn in the long term (Lemmon et al., 2016). The positive attitude of the family toward facing the disease and actively participating in rehabilitation therapies and follow-up programs for their children can be decisive in optimizing their neurodevelopment and well-being (Natarajan et al., 2014).
From these findings, it is clear that the outcomes of parents and children are reciprocally linked and that promoting the emotional well-being of parents can aide both. In this sense, as concluded by the systematic review by Al Maghaireh and colleagues (2016), it is a priority to implement strategies aimed at providing the instrumental and emotional support necessary to minimize the emotional impact on the family and encourage better coping.
The guide shown in this article falls within this objective. As various studies suggest, information is a priority for the parents of a seriously ill newborn to the extent of being considered by them as a coping strategy. Parents who feel informed participate better in decision-making and are encouraged to participate in the care of their children, essential elements for bonding and empowering. However, for the information to be effective, it must respond to their needs (Brett et al., 2011; Cleveland, 2008; De Rouck & Leys, 2009; Ignell Modé et al., 2014; Smith et al., 2012).
In a recent study, parents of a newborn with HIE verbalized needing individualized information about the disease, treatment, care, and prognosis and having difficulty organizing, assimilating, and recalling information. They pointed to the empathic communication of professionals using simple language as essential to better understand information and mitigate their fear. They also valued written materials as instrumental resources to aide in the understanding of information, to facilitate recall, and to transmit to other family members (Lemmon et al., 2016). In other populations, such as parents of preterm infants, written informational resources have been shown to be effective in reducing anxiety and stress in families (Davidson et al., 2017; Galarza-Winton et al., 2013; Melnyk et al., 2006).
In this sense, although the whole family can benefit from the guide, we believe that it may be especially useful to fathers because frequently, and due to the clinical situation of the mother, they are the first to receive information, face decision-making alone, and even transmit this information to other family members (Lemmon et al., 2016). As revealed by Ignell Modé and colleagues (2014), managing these issues is very difficult for fathers, and it puts their parental role to the test. Early, adequate, and comprehensible information increases their security and sense of control over the situation.
Moreover, one aspect to note is the potential contribution of this guide to helping in the transmission of information to families in a unified and homogeneous way, thus improving communication among them. This element is important since informing families in a crisis context is difficult for professionals (Ignell Modé et al., 2014; Janvier et al., 2014). Parents frequently complain of receiving fragmented and heterogeneous information from professionals, which is perceived as an obstacle to establishing a relationship of trust and collaboration (Lemmon et al., 2016; Wigert et al., 2013).
The main strength of this guide is that it is based on the experiences of parents of newborns with HIE and adapted to the needs of the families. The content responds to the significant issues identified by parents in the qualitative research carried out. The didactic and user-friendly question–answer format, written in simple language, supported by a glossary, accompanied by specific illustrations and verbatim quotations of the families, is also adapted to their priorities. In addition, parental involvement was essential to help in rephrasing questions, refining language, and eliminating common expressions in medical jargon such as “cooled infant,” which carries a negative emotional burden. And as suggested by some authors, parents played a significant role in the dissemination of the guide in digital format through patient associations and virtual communities, clearly facilitating its practical application (Boivin et al., 2010).
Finally, we have shown the methodological process followed to prepare the guide, detailing each stage of the qualitative research carried out and how the practical limitations flexibly molded the design, providing transparency and rigor. Making the reflexivity of the researchers visible enables following their sequence as an activity immersed in the research process. A central element of this was considering parents as participants in sensitive research and, as such, at risk of experiencing emotional stress as a result of recounting painful elements of their experience during interviews (Sieber & Stanley, 1988). This led to profound methodological changes such as replacing the conventional interview script with one with images and excluding participants whose children had very serious sequelae.
Limitations
The preparation of this guide was carried out with the participation of families whose infants did not have serious sequelae. The absence of such families, given their fragile emotional state, may be considered a limitation of this guide. Another limitation is that, given the importance of the cultural context in a study of this nature, the guide may not be applicable in other contexts without proper adaptation. Further, it would be desirable to evaluate the impact of this guide on families and its usefulness for health practitioners.
Conclusion
This guide is a tool to provide instrumental and emotional support to parents of newborns with HIE during the hospitalization of their child. Its goal is to empower parents and provide resources for resilience to the challenges posed by parenting in a context of chronic illness.
Presenting the process of developing the guide illustrates in a practical way how the perspectives of patients and their families can be incorporated into a CPG. This is a relevant issue, as it is a fundamental pillar of evidence-based practice and family-centered care, but its practical application is still infrequent and experience in carrying it out is limited. This article can provide support for other teams wishing to conduct similar projects.
Footnotes
Authors’ Note
This study was part of the PhD dissertation of N.H.-R. The content of this article has not been published before except as a brief abstract in the proceedings of a scientific meeting.
Acknowledgments
We would like to express our gratitude to the families who participated unselfishly in the preparation of this guide. We would also like to thank Dr. Krauel for his meaningful drawings and the CPG team for all the enthusiasm they put into the collaboration with us.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Parents’ guide was part of the Spanish National Health System Clinical Practice Guideline on perinatal hypoxic-ischemic encephalopathy. Funding was received for the development of it from the Institute of Health and the Health Quality and Assessment Agency of Catalonia. It has been funded by the Spanish Ministry of Health, Social Services, and Equality (PIC-108-13).