
Abstract
Evidence suggests that studies aiming to improve healthcare practice should be flexible and prioritise patient, family and clinician engagement. Video-reflexive ethnography (VRE), a form of qualitative research often employed in healthcare settings, is well-suited to these aims. VRE supplements ethnographic techniques with video-recordings of in situ practices, allowing practitioners to reflect on taken-for-granted practices. Its prioritisation of collaboration, affective entanglement, theory-driven analysis and flexibility – aligned with participatory and post-qualitative inquiry (PQI) – can facilitate reflexivity among researchers and participants for local practice improvement. Yet paradoxically, flexibility can hinder the predictability of impact, and demonstrating likely impact is crucial to securing research funding. This article offers practical advice to qualitative researchers facing this methodological challenge. Using three exemplars, we examine how differing onto-epistemological groundings, conceptualisations of participant engagement and researcher positionings affect the timing, predictability, scalability and transferability of each study’s impact. We show how prioritising affective engagement, flexible goals and collaboration can enable local healthcare practice improvement; prioritising theory generation via consultation can lead to traditional, more transferable, forms of impact. We share insights for researchers seeking to improve healthcare using methods inspired by PQI such as VRE. While predicting impact is fraught, optimising conditions for impactful VRE research can be accomplished by: foregrounding epistemology; prioritising affective engagement; aligning research and stakeholder goals; assessing timing and organisational readiness; and considering researcher and participant positioning.
Keywords
Introduction
To secure competitive funding, researchers across the globe are increasingly required to demonstrate the impact of their proposed research. Impact, drawing on the Organistion for Economic Cooperation and Development’s (OECD, 2009) definition, can be broadly conceptualised as contributions that research makes to society, beyond the academy. Fryis and colleagues (2019, p. 3) offer a list of the many different forms that impact can take: improvements in environmental health, quality of life, changes in industry or agency philosophy and practice, implementation or improvement in policy, improvements in monitoring and reporting, cost-savings to the economy or industry, generation of a higher quality workforce, job creation, improvements in community knowledge, better interpersonal relationships and collaborations, beneficial transfer and use of knowledge, technologies, methods or resources, and risk reduction in decision making.
In healthcare contexts, the focus of this paper, research impact includes improving practitioners’ working conditions, practices, standards of care and ultimately health outcomes (Morse, 2020, p. 6). This follows contemporary understandings of impact as ‘demonstrable and/or perceptible benefits to individuals, groups, organisations and society (including human and non-human entities in the present and future) that are causally linked (necessarily or sufficiently) to research’ (Reed et al., 2021, p. 2). It also aligns with progressive understandings of impact as responsive, relational and processual (Antoni & Beer, 2020). As such, it is about recognising participants and their contexts ‘as more than just sources of data and a potential academic paper, but as a collection of humans who are confronting very real challenges which require dedicated attention to overcome’ (183). It requires relationships and recognition of impact as a collective effort, rather than as alignment with an externally sourced definition.
Current evidence suggests that studies aiming to improve healthcare practice should adopt ‘flexible and locally appropriate goals’ (McHugh et al., 2020, p. 9) that prioritise engagement with (rather than research on) patients, families and clinicians, to accommodate the in situ intricacy of such work (Iedema et al., 2019; Leslie et al., 2014). Given its emphasis on complexity, entanglement and ongoing change, video-reflexive ethnography (VRE), as a ‘process methodology’ aligned with participatory and post-qualitative paradigms, is well-suited to such goals (Carlson et al., 2021, p. 154). Participatory methods are well known for transcending traditional divides between researchers and participants, favouring shared ownership, collaboration and within study social change (Bernard, 2000). Post-qualitative inquiry (PQI) is an emerging and ‘multiverse’ post-methodology that resists uniformity in favour of possibilities (Brown et al., 2021, p. 232) and questions the rigidity of dominant ‘conventionalist humanistic’ approaches to qualitative research (Carlson et al., 2021, p. 151), such as grounded theory, with prescribed sequential coding practices (St. Pierre, 2017, 2019, 2021). Instead, theory, plasticity and affective engagement are prioritised (Aagard, 2021; Carlson et al., 2021; Tesar, 2021). Post-qualitative forms of inquiry are disperse, taking many forms, such as the performative paradigm (Østern et al., 2021), arts-based research (Rousell, 2019), immersive cartography (Rousell, 2019) and VRE.
VRE supplements ethnographic techniques with video-recordings of in situ practices, allowing practitioners, patients and/or carers to collaboratively reflect on taken-for-granted practices (Iedema et al., 2013). Its prioritisation of principles rather than steps, affective entanglement, theory-driven analysis and flexibility – aligned with PQI – can facilitate shared reflexivity and local healthcare practice improvement (Iedema et al., 2019).
VRE also shares an interest with participatory approaches in democratising scholarship (Batallan & Ritta, 2017; Dadich et al., 2018; Watson & Fox, 2018). Rather than blindly accepting that only researchers (who are typically part of the academy or university trained) are the sole bearers of the expertise required to design, conduct and report on research, participatory approaches and VRE both award primacy to a greater form of egalitarianism. They value and harness different types of knowledge from different sources – these include the participants who are often relegated to the position of research ‘subject’.
However, VRE is not synonymous with participatory methodology; it encompasses much more. Specifically, its four guiding principles – namely, exnovation, collaboration, reflexivity and care (Iedema et al., 2019) – are undergirded by myriad theoretical influences: from complexity theory to Dewey (1922), Foucault (1978), Latour (2004) and Flyvbjerg (2001). Participatory approaches tend to be more confined. For instance, while they necessarily involve care (to foster psychological safety) and collaboration, akin to VRE, they do not necessarily require exnovation or reflexivity. The former refers to ‘the attempt to foreground what is already present – though hidden or overlooked – in specific practices, to render explicit what is implicit in them’ (Mesman, 2011, p. 72). The latter is different from reflection and involves viewing, reviewing, imaging and reimagining practices (Iedema et al., 2019). As Iedema Iedema (2011, pp. i83–i84) explains: Reflection refers to the common practice of thinking back to an event and assessing it and our conduct in relation to it… Reflection is personal, focused and purposive… Reflexivity, in contrast, refers to our capacity to monitor and affect events, conducts and contexts in situ… unlike reflection, reflexivity is collaborative in nature, diffuse in focus, open-ended in purpose and immediate in effect.
While some of the challenges that vex participatory approaches have been addressed – like, substantiating its validity and impact (Burke, 2004; McTaggart, 1998; Operations Evaluation Department, 2004; Thiollent & de Toledo, 2012) – this is not necessarily the case for VRE. Thus, to extend extent literature on PQI, this article purposefully considers the impact of VRE, as VRE is ‘unpredictable’ (Messman et al., 2019, p. 4). The flexibility required hinders a researcher’s capacity to plan, articulate and demonstrate forecasted research engagement and impact with any certainty, which is crucial to securing funding in the current research climate.
This article considers the paradoxical challenge of designing and conducting research in healthcare that is both flexible and predictably impactful. It shows that ‘how we choose to do our research determines the product’ (Morse, 2020, p. 5): how goals and onto-epistemological positioning underpin engagement and impact possibilities. It offers practical advice for those planning studies in healthcare using VRE. In short, our thesis is that healthcare practice improvement impact using VRE can be facilitated by: reflecting on epistemology; prioritising deep affective engagement; aligning research and stakeholder goals; assessing organisational readiness; and considering researcher-participant positioning. To develop our thesis, we first provide a foundational background to the current research impact era, PQI and VRE. We then present and analyse the impacts achieved across three exemplar VRE studies, leaving readers with insights into how to design research to maximise impact using a flexible approach, like VRE, inspired by post-qualitative and participatory forms of inquiry.
Research Impact
Since the 1970s, research impact has slowly become a greater priority for national funding bodies (Fryir et al., 2019). Traditionally, it was assumed that supporting excellent research would lead to (un)predicted 1 impact within and beyond universities (Penfield et al., 2014). The focus was, accordingly, on measuring academic output, volume and quality. Over the past two decades, calls for accountability among health services have heightened (Joo et al., 2016); organisational decision-making – including decisions on the use of funds, particularly public funds – for research on health and healthcare now answers to a wider audience (Chalmers et al., 2014; Kass & Faden, 2018; Mietchen, 2014; Neyland, 2007; Sifry, 2011). Despite critiques that such practices skew funding towards studies that can predict impact, regardless of the potency of such impact (Iedema et al., 2019), grant proposals and government accountability mechanisms now require researchers to clearly indicate: how they will engage stakeholders; the potential impact of their study; as well as the scalability of the associated findings and wider impact (Dobrow et al., 2017; Edwards et al., 2016; Hanney et al., 2017; Milat et al., 2013; Penfield et al., 2014; van Bekkum et al., 2016).
Although some definitions of impact, such as Canada’s health solutions impact framework, include ‘knowledge production’ (Graham et al., 2012, p. 355), overall, the definitions are narrowly focused on changes outside of academia made possible through scholarly research. The United Kingdom’s Research Excellence Framework (REF), for example, echoes the OECD (2009) in highlighting the importance of impact as demonstrated by ‘an effect on, change or benefit to the economy, society, culture, public policy or services, health, the environment or quality of life, beyond academia’ (Higher Education Funding Council for England, n.d., para. 1). Following the REF and the Netherland’s social impact assessment methods for research and funding instruments (SIAMPI), which recognises the importance of ‘productive interactions’ between researchers and stakeholders as a precursor to impact (Royal Netherlands Academy of Arts and Sciences, n.d.), the Australian Government similarly requires researchers to demonstrate both ‘interaction [s] between researchers and research end-users outside of academia’ (engagement) and the ‘contribution that research makes to the economy, society, environment or culture’ (impact) (ARC, 2019, para. 8–9). Impact, however, is difficult to predict for projects aligned with non-linear methodological designs, such as PQI.
Post-Qualitative Inquiry
As a new form of scholarship, PQI encourages scholars to use theory as methodology (St. Pierre, 2021). Rather than coupling explanations on how and why phenomena occur (Sutton & Staw, 1995; Weick, 1995), with ‘way [s] to systematically solve the research problem’ (Kothari, 2004, p. 8), PQI challenges this distinction, melding the two. Said another way, theory and method are linked in all research paradigms and practices (Pink & Sumartojo, 2017), though this link is often overlooked (e.g. post-positivism) or takes a linear form (e.g. bracketing in phenomenology and grounded theory) (Glaser, 1992). PQI rejects the cautious relationship between theory and method that predominates (Aagaard, 2021), seeing it as one of many ‘leftovers from a positivist approach that still has tentacles into a (traditional humanist) qualitative research paradigm’ (Østern et al., 2021, p. 12). Instead, PQI ‘comes with no methodology at all, no pre-existing rules, processes, methods, categories, or “determining judgment”’ (St. Pierre, 2017, p. 1). In place of methodological fetishism, PQI prioritises affective encounters with discursive-material entanglements, to trace intensities and movements (Fullagar, 2017).
PQI presents clear opportunities. First, its methodological plurality supports theoretical advancement. The development of influential theory requires approaches that constructively provoke beliefs and assumptions, rather than merely identify gaps and issues, or problems with the knowledge-base – this is because this knowledge-base is largely situated on prevailing beliefs and assumptions, rather than counterviews (Alvesson & Sandberg, 2011; Masny, 2016). For instance, Alvesson and Kärreman (2007, pp. 1265–1266) argued for ‘the active mobilization and problematization of existing frameworks’ to develop theory. Unfettered from ‘determining judgment’ (Lyotard, 1984, p. 81), PQI has the elasticity to prod, provoke and problematicise what is (assumed to be) known. It urges researchers to ‘use theory to think with their data (or use data to think with theory)’ (Jackson & Mazzei, 2013, p. 261, original italics) to contest convention.
Second, because PQI starts with appreciation of subject-object, researcher-researched, human-nonhuman as ontologically entangled (Østern et al., 2021) – it helps to democratise scholarship. Rather than award primacy to conventional forms of knowledge – like empirical evidence – it recognises and embraces different forms of knowledge based in theory and affected bodies. It welcomes myriad data, views and experiences. The encompassing breadth of PQI directly responds to increased calls from funding bodies for engaged research (van Bekkum et al., 2016), research ‘committed to making a positive difference in the world’ through an ‘orientation to others’ (James, 2015, p. 8). While PQI shares this aim of effecting social change with many other qualitative approaches, it is relational ontology offers an opening to even broader forms of orienting towards others, knowledge creation and change.
Despite the opportunities afforded, PQI also presents challenges, particularly about its anticipated impact and the scalability of associated findings. Given its disperse and nebulous nature, it can be difficult to forecast or measure how research inspired by PQI will definitively lead to a ‘contribution… to the economy, society, environment or culture, beyond the contribution to academic research’ (ARC, 2018 n. p.). For instance, how might a PQ inquirer convince a funding body that the use of an post-methodological 2 approach demonstrates the sound use of limited (public) funds? As a critical response to conventional approaches to qualitative research, some interpret PQI as a-methodological (St. Pierre, 2019, 2021), others as a flexible hybrid of post-qualitative and conventional approaches (Brown et al., 2021), others still as a revised materialist, theory-informed and affective way of doing qualitative research (Carlson et al., 2021). Although PQI – as a post-methodology or process-methodology that merely offers tools for navigation (Carlson et al., 2021) – is useful in guarding against the ‘constraints of gold standard protocols’ and protecting the possibilities that such a ‘methodological multiverse’ affords – its flexibility resists prediction (Brown et al., 2021, p. 232). Similarly, it can be difficult to argue that research inspired by PQI will culminate with findings that will benefit others further afield, particularly at a national or an international scale. How might a research proposal, in which applicants ‘give up’ (Lather & St. Pierre, 2013, p. 630) established practices, convince those who hold the (public) purse-strings that others will benefit? The impact of research and scalability of the associated findings can be difficult to forecast and demonstrate in many studies, irrespective of research design – yet it is perhaps more so in PQI, which ‘encourages concrete, practical experimentation and the creation of the not yet instead of the repetition of what is’ (St. Pierre, 2019, p. 3, original italics).
In the following section, the challenges that surround PQI are taken up – notably, its capacity to demonstrate engagement, impact and the scalability of associated findings – with reference to VRE. Opportunities are proposed for strengthening how VRE and perhaps other forms of research inspired by PQI might demonstrate engagement and impact. However, reflecting PQI’s critique of rigid methodologies, the insights provided are not intended to be prescriptive directions for VRE or PQI, but grounds to progress understanding to advance (post-)methodological decision-making for improved impact and effectiveness.
Video-Reflexive Ethnography and Impact
VRE is both a methodology and a process methodology. As a methodology, VRE combines ethnographic techniques (e.g. extended participant observation, interviewing) with the analysis of video-recordings of in situ practices with participants during reflexive sessions to elicit collaborative insight (Iedema et al., 2013; Mesman et al., 2019). Used largely within healthcare (Iedema et al., 2019), this visual methodology makes largely ‘invisible’, mundane everyday practices ‘visible’ to practitioners (Dadich et al., 2018, p. 1206). By drawing on the ‘affective effect of practitioners watching video footage of their own practice’, VRE reflexively invokes transformation in the complex and messy space of healthcare (Iedema & Carroll, 2015, p. 69). Thus, VRE can be conceptualised as a flexible methodology that aims to not just describe, but foster learning, readiness for change and healthcare practice improvement 3 (Carroll & Mesman, 2018; Iedema et al., 2013). Especially in the context of patient safety, VRE has inspired quality improvements through revised local practices (Higher Education Funding Council for England, n.d.). Consistent with the democratising principles of PQI, VRE aligns ethically with participatory research, which resists objectification in favour of working with participants in a trusting relationship to encourage transformation (Carroll, 2009; Carroll et al., 2008; Collier & Wyer, 2016; Dadich et al., 2018).
Philosophically and theoretically, VRE is a process methodology responding to the PQI shift towards ‘more dialogic, evolving methodologies’ (Juhasz et al., 2009, p. 322) that capitalise on researcher capacity to affect and be affected (Mesman et al., 2019; Wyer et al., 2017). Rather than a pre-defined procedure, as a process methodology, VRE is responsive – to the emerging research context and in the theoretical tools employed (Carlson et al., 2021). VRE ‘privilege [s] co-accomplished sense-making’ over traditional approaches that favour the researcher’s expertise above the researched (Iedema & Carroll, 2010, p. 73). It prioritises ‘being present’ through affective engagement with participants and the research process, rather than generalisable ‘knowledge production’ or a ‘step-by-step methodology’ (Iedema & Carroll, 2015, pp. 68, 71). However, in practice, VRE is varied (Iedema et al., 2019). As a post-paradigmatic approach to research, it draws on multiple epistemologies (Olson et al., 2020), from an interpretivist appreciation of practices as socially co-constructed to a critical appreciation of power as ubiquitous and a participatory commitment to prioritising change in researching with (rather than on) participants (Iedema et al., 2019; Lincoln et al., 2013).
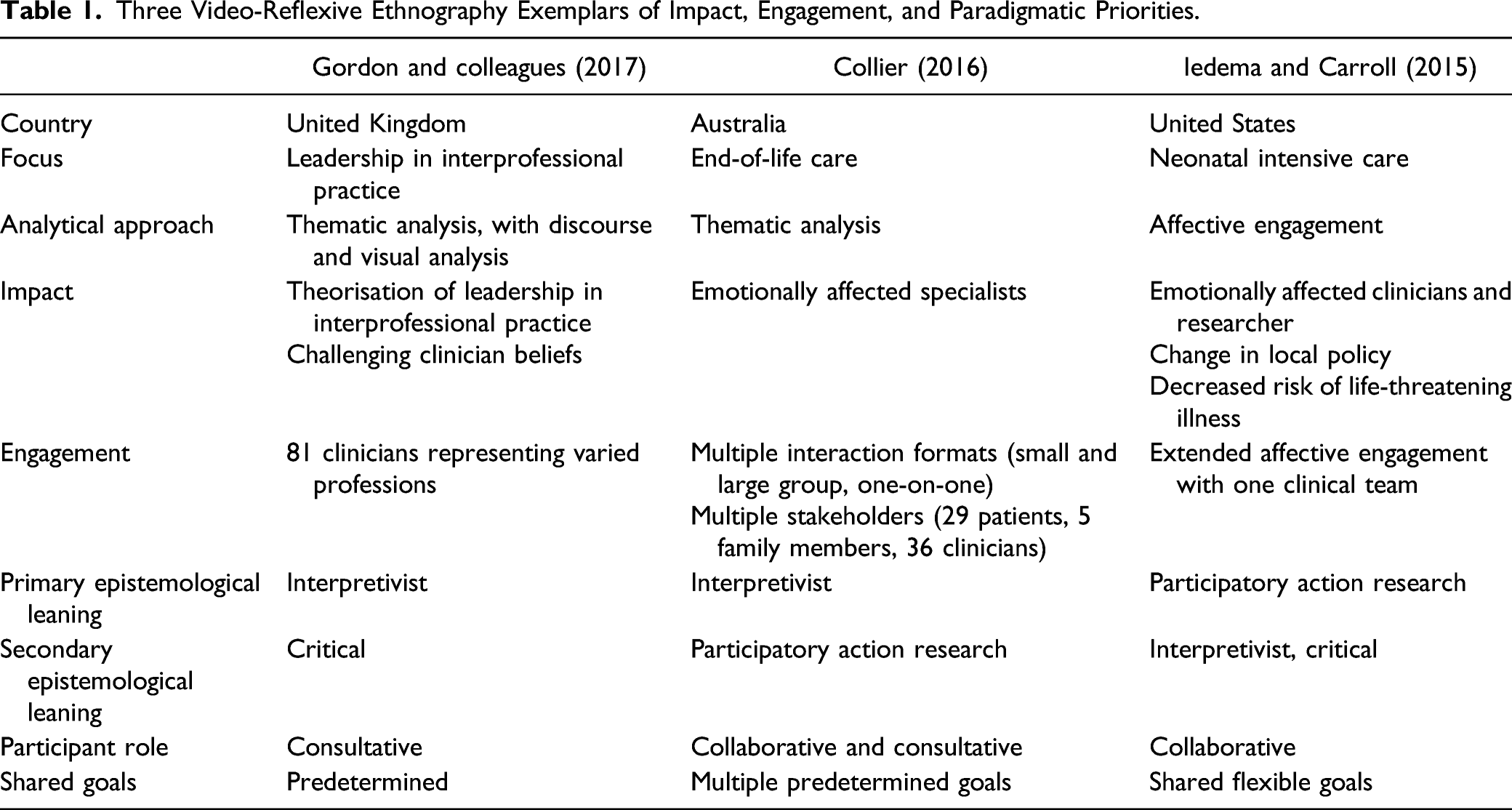
Three Video-Reflexive Ethnography Exemplars of Impact, Engagement, and Paradigmatic Priorities.
Video-Reflexive Ethnography Study 1
Gordon and colleagues (2017, p. 1101) used VRE to ‘capture the complexity of leadership’. They studied interprofessional practice at two UK clinical sites and interrogated filmed interactions between clinicians using thematic analysis, drawing on discourse and visual analysis, to understand how leadership was enacted in interprofessional healthcare. Videos revealed the ‘minutiae of interactions’ (Gordon et al., 2017, p. 1117). Their analysis theorised common features of ‘influential acts of organising’ (Fairhurst & Uhl-Bien, 2012, p. 1050) and highlighted the importance of the control of materials, such as computers and patient notes, when negotiating and renegotiating leadership. Reflexive sessions served to challenge clinician beliefs about leadership practices and offered clinicians an opportunity to contribute to analysis – ‘using video-reflexivity provided formal accountability for our own analysis and provided rich opportunity for the co-construction of meaning, which served to enrich our study findings’ (Gordon et al., 2017, p. 1118). VRE was largely used as a traditional approach to interpretivist data collection. Affect and participatory principles were low-lighted, while the capacity of VRE to be a visual methodology for transferrable theorisation was emphasised.
Video-Reflexive Ethnography Study 2
Acknowledging the limitations of ‘tickbox approaches’ to improve end-of-life care within hospitals, Collier (2016, p. 11) capitalised on VRE’s emotional potentiation: the capacity to affectively engage participants considering their practices so they are able to stand outside and reconsider them (Iedema, 2021). Combining interpretivist and participatory research goals with an indigenous ethics framework (Collier & Wyer, 2016), Collier supplemented ethnographic techniques – participant observation, interviewing and thematic analysis – with videoing, and viewed the videos of patients, families and staff with participants for their reflections (Collier, 2016). The focus of these data was participant understandings of care. She edited the video-recordings into thematic video-clips and presented these to stakeholders within the hospital over the course of four reflexive sessions, inviting critical responses.
The emotional affect was consistent – ‘without exception, specialists spoke of “being moved”’ (Collier, 2016, p. 8). The emotional entanglement afforded through the videos ranged from mild surprise to more intense anger and guilt. Specialists described surprise, for example, when patients and families positioned themselves as knowledge holders in videos, impressing healthcare workers with the extent to which they understood their diagnosis, prognosis and overall circumstances (Collier & Wyer, 2016). In other reflexive sessions, emotions were more intense and controversial: on one occasion an attendee expressed concern that I was complicit in exposing healthcare workers to unnecessary harm by provoking guilt for those employed in a ‘broken’ healthcare system. On another occasion… a physician suggested…. That people’s visual narratives were clearly not representative of the majority of the patients and families (Collier, 2016, p. 9).
The feelings of disquiet in the critiques presented in Collier’s article might be necessary precursors to practice change in end-of-life care; a diverse body of scholarship suggests affect and emotion are necessary precursors to change (Ahmed, 2015; Holmes, 2004; Montgomery, 2008; Olson et al., 2017). Strong emotional reactions, Collier (2016, p. 10) concordantly argues, are required to ‘unsettle habitual ways of being’. In this study, VRE was valued for its affective intensity and local specificity. Collier emphasised the potential for VRE to provoke strong emotions relevant to practice improvement. Although practice changes were not discussed, she emphasised their potential because of the emotional entanglement afforded through VRE.
Video-Reflexive Ethnography Study 3
Iedema and Carroll (2015) employed VRE within a neonatal intensive care unit (NICU) in the USA. Rather than ‘privileging some analytic endpoint’, they prioritised collaborative presence – affectively and reflexively (p. 68) – an approach described elsewhere as ‘affect-as-method’ VRE (Carroll & Mesman, 2018). Shared presence between the researcher and clinicians through VRE enabled them to be collectively ‘moved to act’ (Iedema & Carroll, 2015, p. 68). For instance, Carroll’s fieldnotes described NICU clinicians working to help a disadvantaged, young mother who had given birth to a severely ill, premature baby. The mother did not produce enough breastmilk for her baby, and the neonatologist was reluctant to prescribe formula because of the baby’s condition and the risk of necrotising enterocolitis: a potentially deadly infection. The NICU had a policy of supplying 360 mls of donor human breastmilk without charge; after that, families were required to pay. However, as Carroll articulated, ‘turning to the infant’s mother to provide money for the infant’s donor milk was not a possibility, she could not afford to buy her own lunch, let alone the medical costs associated with her infant’s hospital admission’ (Iedema & Carroll, 2015, p. 69). Carroll felt moved by the helplessness of the mother and clinicians, as did the clinicians when they watched the video-recordings. ‘As the clinicians watched the footage… they realised… the current donor milk policy… went against “the organisation they wanted to be”’ (Iedema & Carroll, 2015, p. 69). Through VRE, the ‘researchers and researched agree [d]… that specific matters matter sufficiently for them to warrant action’ (Iedema & Carroll, 2015, p. 72). After the clinicians lobbied for change, unlimited amounts of breastmilk became available to NICU patients where the mother’s supply was insufficient. Here, VRE was practiced as shared presence, characterised by the potential to affect and be affected. Local quality improvement and improved health outcomes, achieved through the decreased risk of neonatal death, were provoked through shared presence, emotions and relational enactment.
Analyising Video-Reflexive Ethnography’s Varied Impacts
VRE – as both a methodology and a process methodology – aligns with PQI’s treatment of bodies, materials and texts as affectively intertwined (Fullagar, 2017; Iedema et al., 2019). The flexibility inherent to such an approach makes predicting impact impossible. Indeed, none of the outcomes described in the case studies, bar study one’s contribution to theory, was predictable (Wyer et al., 2017). This highlights the challenge of employing research practices that draw on PQI, such as VRE, to demonstrate future impact. Given these difficulties, we analyse here the three studies employing VRE.
Evidently, VRE assumes many forms, some more aligned with PQI than others. Conceptualisations of engagement vary from breadth to affective depth; approaches to participation range from collaboration to consultation; and impact includes definitive local change through to historical outcomes in the form of academic contributions. Drawing on our three case studies, in this section, we analyse how some elements of VRE are foregrounded and others backgrounded, with differing effects. Specifically, we ask questions about impact, scalability, engagement, goals and positioning. In answering these questions, we identify insights for researchers seeking to achieve the interconnected goals of engagement, impact and scalability using VRE (highlighted below in bold): foreground epistemology, prioritise affective engagement, bring research and stakeholder goals into alignment, consider timing, and reflect on researcher and participant positioning.
Impact: Timing and Scale
Our first questions consider the impacts 4 afforded through the three VRE case studies, the temporal nature of VRE impact, and its scalability. The researcher’s role as videographer, video-editor, co-researcher and change facilitator is necessarily short-lived; projects and funding are never without end dates. Thus, we ask what impacts are evident; what impact follows project completion; and is there scope for impact further afield?
The outcomes stemming from the critical and interpretivist approach to study one, where participatory principles were low-lighted, was largely academic and presumed – publications theorising leadership in interprofessional practice – aligned with historical conceptualisations of impact as something that would eventually result from contributions to the academy (Penfield et al., 2014). As the results focussed on theory generation, the magnitude of the study’s effect beyond the academy is uncertain. Broad dissemination could see the theory inform future health education programs, beyond the research sites – however, this is a probable rather than a certain and predictable impact. While study two similarly did not describe an immediate impact on healthcare practice, the heightened emotions might facilitate future impact (Holmes, 2004; Montgomery, 2008; Olson et al., 2020). Collier argues that the study fostered clinicians’ readiness for change, aligned with arguments that affect and discomfort are necessary for new ways of seeing and doing (Boler & Zembylas, 2003; Iedema, 2021). In study three, impact can be identified clearly as a change in policy and practice, with quantifiable health benefits: a decreased risk of necrotising enterocolitis and associated decrease in neonatal mortality risk. Although impact was contained to the NICU, there is scope – through future projects – for similar quality improvement elsewhere. Regarding scalability, it is possible that, through broader dissemination, all three studies might inform policy and practice, further afield – however, the emphasis on local context in studies two and three complicate transferability.
The contrasts presented here in impact and scalability largely reflect differences in the epistemological leanings across the case studies. As a post-paradigmatic methodology (Olson et al., 2020), VRE draws its assumptions and principles from more than one research paradigm (Iedema et al., 2019; Lincoln et al., 2013). As such, and despite VRE’s alignment with PQI (Iedema et al., 2019; Wyer et al., 2017), there is the capacity for VRE scholars to prioritise more traditional, researcher-driven priorities – aligned with the interpretivist and critical paradigms – or participatory priorities that attend to local contexts and practices. This serves as an important reminder; in VRE study planning, foreground epistemology. VRE studies aligned with participatory principles might be more likely to achieve impact through healthcare practice improvement. Critical and interpretivist assumptions support more traditional researcher and participant relationships that foster traditional research outputs, such as theorisation disseminated through scholarly publications.
Conceptualising Participant Engagement
Our second focus is on engagement: how can researchers’ gage participant engagement? In the first study, as previously noted, the approach was largely academic. Clinician engagement was demonstrated by contributing to, rather than co-directing, the analysis. The means of evaluating participation was implicitly numerical: a detailed description of all 81 participants suggests one approach – counting participants across different levels of hierarchy. Yet conceptualising engagement in this way might favour shallower forms of participation that do not prioritise relational entanglement and might not foster in situ or broader practice changes.
Conversely, in studies two and three, engagement was indicated by emotional effect, with participants feeling moved to act. In the second study, patients’ emotionally charged stories regarding end-of-life care flexibly shaped the research purpose. Extended description of encounters with participants – ethnographic, filmed, small group, one-on-one and large group – suggests another benchmark for judging engagement: breadth in interaction. Conceptualising engagement in this way allowed myriad voices to potentially direct the research. However, the range of stakeholders might limit the effect of engagement to emotional entanglements.
In the third study, the researchers’ and clinicians’ shared affective responses defined participant engagement and the research impact: decreased risk of necrotising entercolitis and infant death through increased availability of breastmilk. The shared presence illustrated in study three offers yet another marker of engagement – the affective depth of the interactions between researcher and participants. Measuring engagement as affect and prioritising shared presence with a small group of participants, fostered their strong contributions as relationally entangled co-researchers. Although affect is a dynamic phenomenon that is said to elude the measurement and predictability often required by funding bodies (Collier & Wyer, 2016), we argue that VRE researchers should prioritise affective engagement in VRE study design to facilitate local impact.
Participant/Researcher Goals and Positioning
Our final questions relate to positioning and challenge the participatory principles of VRE (more than PQI): how do research goals and researcher positioning affect impact? Are participants always best-placed to recognise opportunities to reconceptualise or change their practices?
Regarding research goals, studies one and two could be interpreted as having predetermined goals, while study three’s goals seemed more flexible, responsive to the affective effect of viewing the videos. Improving healthcare practice – a goal with widespread appeal (Howell et al., 2017) – has been the broad aim of several VRE projects that have stimulated quality improvement (Gilbert et al., 2020), some with relevance beyond the research site (Iedema et al., 2013). Research goals related to more contentious issues, such as interprofessional practice (Gordon et al., 2017) and ‘good’ end-of-life care (Collier, 2016), might not attract widespread support. The extent to which meaningful engagement and impact is achievable via VRE might depend on alignment between the research goal(s) and those of stakeholders.
Thus, we argue that VRE scholars should prioritise flexibility, and align research and stakeholder goals. They should ask: does the study reflect a shared aspiration across stakeholders, be they researchers, clinicians, health service managers, patients or family members; why or why not; and what are the associated effects? We also advise VRE researchers to consider timing. An organisation committed to change, but not yet clear on how, might be primed to benefit from VRE.
Regarding researcher positioning, it was clear from all three studies that a shared profession between the researchers and participants might also help to foster ‘trustful entanglement’ (Carroll et al., 2008, p. 389). However, this must be considered with reference to the research goal(s). Both Gordon et al. (2017) and Carroll (Iedema & Carroll, 2015), for example, drew on their clinical experiences to understand the realities of working within a health service. Yet, given Gordon’s focus on distributive leadership (rather than patient safety), some clinicians might have felt threatened by her positioning, particularly those who feared losing authority and autonomy to interprofessional decision-making (Baker et al., 2011). The studies considered in this article also collectively suggest that researcher values, be they explicit (Gordon et al., 2017) or implicit (Collier, 2016; Iedema & Carroll, 2015), are central to VRE. Thus, like so many before us (Carroll, 2009; Carroll & Mesman, 2018; Finlay, 2002), we advise VRE researchers to consider researcher positioning, in reference to the goals of the research. As is suggested within scholarship on participatory research, shared positioning and values – which will vary depending on the research context and goals (e.g. professional background or expertise, status within the healthcare hierarchy, gender) – might foster the trust and affective entanglements needed to achieve impact (Batallan & Rita, 2017; Bernard, 2000; Burke, 2004; Thiollent & de Toledo, 2012; Watson & Fox, 2018).
In response to our final question – are participants always best-placed to recognise opportunities to reconceptualise or change their practices? – this was certainly the case in study three. This insight, supported by scholarship on participatory research more broadly, suggests the need to consider participant positioning, as well as researcher positioning (Battallon & Rita, 2017; Bernard, 2000). Clinicians were valued as experts on the ‘taken-as-given practices and associated understandings’ that imbued their work (Iedema & Carroll, 2010, p. 71). The practitioners, as co-researchers, were moved to act, but also well-positioned to determine the local actions needed. Yet in study one, participants might not have been well-placed to recognise opportunities for self-change. The clinicians held ‘deeply entrenched values, beliefs and practices in relation to healthcare leadership as hierarchy’, ‘inhibit [ing] the cultural shift towards distributed patterns of leadership’ (Gordon et al., 2017, p. 1117). In this study, the researchers were valued as experts in leadership; participants were positioned as subjects – not co-researchers – in need of ideological emancipation, aligned with critical paradigm research goals. The appropriateness of this approach can be defended, based on the study focus – it was built on the premise that new forms of leadership need to be studied, enacted and embraced if interprofessional healthcare is to be successful. For this end, the researchers might be well-placed as knowledge experts and change agents, though this might limit participant-driven local change.
Concluding Remarks
Demonstrating impact is crucial to securing research funding, yet flexible, non-linear in situ research that prioritises participant engagement is argued to be more effective at improving healthcare practice. Such flexibility, which necessarily accommodates for contextual complexity, eludes the impact prediction required by national funding bodies. This article offers reflections on the challenges of forecasting impact in VRE. As a methodology and process methodology, VRE is geared ‘toward inventing practices that do not yet exist’ (Lather, 2014, p. 8). Using three studies as exemplars, we illustrated the breadth of ways that VRE has been interpreted and applied – to varied affect/effect. Despite the unpredictability of research practices which foreground theory and relationality, we have argued that the potential of VRE to demonstrate impact hinges on key considerations regarding the alignment of goals and positioning. In essense, to help VRE researchers improve the likelihood of positively impacting healthcare practice improvement, we suggest: foregrounding epistemology; prioritising affective entanglement; aligning research and stakeholder goals; considering timing; and considering researcher and participant positioning.
Footnotes
Acknowledegments
We wish to thank the Australian Consortium for Social and Political Research Incorporated (ACSPRI) organising committee for inviting us to speak on this topic, Mr Morgan Dudley for his support as an RA in finalising this manuscript for peer review, and our colleagues within the International Association for Video-Reflexive Ethnography (VREIA) for their ongoing collegiality and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.