
Abstract
Despite advocates for aesthetic forms of presentation in qualitative enquiry, for going beyond thin description, to share evocative forms of representation that resonate with that (Todres, 2008; Todres & Galvin, 2008), qualitative research in the health care field continues to favor conventional methods. This article adds to existing knowledge by articulating the innovative creation and value of aesthetic offerings in the unique form of visual maps to evoke the lived experience of being on an acute stroke unit, drawn from phenomenological interview findings. The maps helped embody the meaningful lived space and conveyed the complexity, spatiality, and holistic understanding being developed. They embodied the researcher’s involvement, position, and place as she imaginatively lived through the space of the acute stroke unit and proceed to invite others to join the dialogue. This article articulates the methodical alignment of creative mapmaking within three stages, for the development of phenomenological understanding, dialogue in-between, and ongoing life of dialogue for future projections toward practice and within the phenomenological project. This article illustrates the underutilized potential of mapmaking for the human sciences, understanding health care spaces, other meaningful lived spaces, and qualitative research methods.
Keywords
Introduction
A method is a way into one’s work. It is a way of going to work on one’s work, the making of a path that one follows into one’s work. When one designs a method, one is mapping out the journey that one will take from that place of not knowing one’s topic to that place of coming to know it. And, as with all other journeys, how one goes along the path informs what one will experience of the topos—the topic or place—where one arrives, and how one will experience it.
Mapping, mapmaking, and cartography are enmeshed with our social, historical, geographical, and scientific culture (Monmonier, 2007). From a health perspective, maps have predominantly been used as tools to define, label, categorize, and objectively record populations, diseases, and services. They can assist in visualizing health and sociodemographic profiles and health care needs from a geographical perspective (Samarasundera et al., 2012). Other studies have applied geostatistical continuous surface maps to estimate the spatial structure and variability of human immunodeficiency virus epidemics in South Africa and Tanzania, using routine health care facility data (Cuadros et al., 2018). In the field of qualitative research, maps are largely employed to present, organize, model, or analyze conceptual, categorical, and/or theoretical data. For example, concept maps have been used to compare and organize theoretical frameworks and approaches to guide a whole systems approach to integrated community-based primary health care (Steele Gray et al., 2018). Kokko and Lagerkvist’s (2017) hierarchical value maps presented the most important constructs and connections identified in their study that related to parents’ mental models about school sanitation and children’s well-being. Fuzzy cognitive maps were developed to demonstrate the strength of relationships between motivations for people participating in online communities in Galehbakhtiari and Hasangholi pouryasouri’s (2015) mixed methodology (which included a preliminary hermeneutic phenomenological study). Other researchers have explored how concept maps can assist in gathering qualitative research data (Wheeldon & Faubert, 2009). However, cartography and mapmaking come from a long tradition that has looked to garner the geographic world, provide order to the world (Wood, 1992) but also make sense of our place within it, traversing between the objective and subjective landscape of place (Karjalainen, 1999). Deep mapping and mapping of fictional and imagined spaces that draw on creative methodologies and literary and artistic mapping traditions are welcome developments in the human, geographical sciences that endeavor to produce artistically informed, sometimes unconventional representations of place (Dodge, 2017). This article addresses the methodical contribution of mapmaking as a development of a particular hermeneutic phenomenological study and their congruence with philosophical and methodological concerns. An extension of the maps beyond the confines of the present study context is also proposed.
The Study
The study in which the maps were created looked to provide phenomenological understanding of what being on an acute stroke unit was like for four stroke survivors and four health care practitioners who had experienced working in one of two acute stroke units in a health care Trust in the United Kingdom. In-depth interviews were analyzed using a hermeneutic phenomenological approach (Suddick et al., 2019).
The researcher adopted a basic-level phenomenological attitude 1 as she undertook detailed work within the hermeneutic circle. This meant working extensively with part and whole (Gadamer, 2004) and reflectively and intentionally attending to what was brought to consciousness and the manner in which it appeared (Giorgi, 1997). This was carried out for each participant until a detailed description of each individual’s comprehensive analysis was produced. Analysis across the collective whole from each perspective (stroke survivor and health care practitioner) was then undertaken.
The findings pointed toward how the lived and practiced space of the acute stroke unit was experienced meaningfully through how it held stroke survivors. The stroke unit was understood to hold the stroke survivors at a distance from their home, pre-stroke lifeworld, and the rest of the hospital. This meant that they experienced space and time to rest, recover, reflect, and think about how they would respond to the stroke. How this holding space was practiced by nurses and others (including their fellow stroke survivors) reflected a human response to human need and functioned to protect, sustain, and support the stroke survivors as they looked to deal with the significant vulnerabilities engendered by the stroke and by being in hospital. This holding space and the practices within it were intertwined with the stroke unit experienced as transitional space. Transition was either signified through its absence or by how the stroke survivors passively relinquished of themselves, actively, temporarily transformed, reasserted themselves, and/or recovered while they were on the stroke unit (Suddick et al., 2020).
The health care practitioners were understood to have appropriated the space of the acute stroke unit for their own self-actualization, for fulfilling their authentic project, experiencing a sense of belonging, and contributing meaningfully to others. This project-ed work was understood to be subject to the everyday challenges of life on the unit. A greater emphasis on process, time, technology, decision making, and fast through-put meant that three of the practitioners felt varying degrees of estrangement from their project and disrupted belonging in the place of the stroke unit. Fond remembrances of the past and a concern and lack of safety in the future (about what was going to happen, if the unit would close, and whether their jobs were safe) compressed their anxiety-laden present and meant they also felt displaced in time. Despite these concerns, the health care practitioners experienced the coexistence of thriving and surviving as they navigated the meaningful space of the acute stroke unit (see Suddick et al., 2019).
Methodology
Hermeneutic phenomenology offers access to embodied, humanly sensitive understanding about the lived-through experience that incorporates the existential, perceptual, and relational nature of experience that is integral to our being-in-the-world and making sense of ourselves, others, and the world around us (Finlay, 2011). This methodology drew on, but was not limited to, the following philosophical touchstones in relation to human being, the conditions through which we understand, and how understanding takes place: Existential and embodied phenomenology is concerned with understanding the world and what it is to be human. This understanding is not constrained by the limits of our rational consciousness but is encountered, lived through, sensed, felt, and revealed through intimate bodily being-in-the-world within and amongst other bodies (Todres, 2007; Wrathall, 2006) The deep, rich, fleshy understanding and meaning of everyday life are inseparable from the world in which we live (lifeworld) (Finlay, 2011). The lifeworld consists of existentials (incorporating temporality, spatiality, intersubjectivity, embodiment, mood, or emotional attunement) (Todres et al., 2007) and fractions (self-hood, sociality, embodiment, temporality, spatiality, project, discourse, and moodedness) (Ashworth, 2016; Husserl, 1970). The lifeworld is a shared, common ground, a universal horizon, all of us together, being in and having of the world (Husserl, 1970) where we are also situated (intersubjectively) with our own unique, dynamic perspective and horizon of understanding (Gadamer, 2004). The lifeworld, intersubjectivity, and horizons of understanding provide the conditions through which we can understand another (Gadamer, 2004) Understanding takes place hermeneutically through the ongoing, circular, interpretive dialogue
2
between part and whole perhaps life of dialogue
3
(Gadamer, 2008). Through extensive dialogue and rigorous play,
4
our horizon of understanding alters, fusing with that of another (Gadamer, 2008).
The purpose of this article is to explain why maps were created, how they were developed by the researcher from phenomenological findings, and to explore their value.
A Path Into the Work
The path into the work that provides the structure for this article represented three overlapping stages in the life of dialogue (Figure 1). The first stage addresses why the researcher created the maps and how understanding the lived space of the acute stroke unit was enhanced through their creation. The second avenue emerged when a dialogue within and between the maps pointed toward a shared, intersubjective understanding of human living. The third stage articulates the relevance of the maps within the ongoing life of dialogue and future, planned projections within the phenomenological project.

Evoking lived experience: Three stages in the life of dialogue.
A Call to Mapmaking
The initial call to mapmaking was in response to concerns around the development of phenomenological understanding and evoking meaningful lived experience. During the analysis, the researcher (K.S.) generated diagrams that signposted the findings thematically. However, they ineffectively conveyed the understanding in-process and did not offer the researcher, and those reading and engaging with the findings of the study an opportunity to dwell, be with that phenomenologically or allow the phenomenon to show itself as itself (Larkin et al., 2006). When articulating her inability to grasp the phenomenon to her research supervisors, K.S. would talk about landscapes, tectonic plates, and layers, all of which provided the initial prompt toward mapmaking. Responding to this call demanded an openness and letting go as K.S. moved from a position of demanding from the data to sensing what it demanded of her. Through the three stages articulated in this article, it became increasingly evident that it was no longer her will or the people that she talked to, rather the “law of the subject matter” that took on a life of its own (Gadamer, 2008, p. 66).
For the researcher, apprehending the phenomenon occupied the focus of her attention. But in the phenomenological hermeneutic project, this is never the end of the work. Although acute stroke units have been built as places with specific locales, settings, and structures, the phenomenological findings showed that it is people who give them meaning and bring them to life. People need to dwell in the structures and spaces they create and making the maps provided an opportunity to ask them to do so. Kirova and Emme (2006) used photographs to develop fotonovela with immigrant children that contributed to the development of phenomenological understanding and visually represented the phenomenon of interest. When shown to other children, the fotonovela were felt to hold evocative power, embody the stories linguistically and visually, and offer multiple ways to engage with the understanding produced (Kirova & Emme, 2006). In this study, the maps as a living text (in a similar fashion to fiction, poetry, sculpture and graphic art) were created to offer immediacy and impact of evocative expression about how the acute stroke unit was meaningfully lived through, as well as one that could be revisited and explored from different vantage points (Willis, 2004). Congruent with this, the final stage of this article will address future plans for the maps beyond the confines of the study in which they were produced.
Going to Work on Mapmaking: The Process of Creating Maps
Mapmaking began with numerous sketches (e.g., Figures 2 and 3). With respect to the phenomenological insights emerging from the analysis of phenomenological interviews, K.S. considered absence, presence, background, foreground, the arrangement and structure of the space, its topographical form, alongside relationships, connections, orientations, positioning, scale, signs, and language used. Describing the whole process is not possible. Key examples are provided to explain how the maps were created, support their contribution to understanding, and offer sufficient context to encounter them effectively.

Sketching the experience of being a health care practitioner on an acute stroke unit.

Sketching the stroke survivor experience of being on an acute stroke unit.
Transitioning from sketching to creating the maps graphically using a multistage process (Ascension of Cartographers’ Guild, n.d.) and Adobe illustrator™ software (Figure 4A–D) was undertaken when the researcher felt a sense of resonance and grasping of meaning (albeit tentative and indefinite). This was congruent with the epistemological open-ended nature of understanding and knowledge adopted in the study. It also reflected how the maps were used to contribute to the ongoing analysis and development of understanding that remained in-play and in-process throughout their creation.

Example steps in creating the stroke survivors map. A. Drawing the landmass and shading the sea. B. Working with topography through shading. C. Demarcating territories in the stroke unit landscape. D. Assigning colors to mark out territories.
Mapmaking began by constructing the landscape, seas, and water ways (Figure 4A–D). Symbols, graphics, phrases, and words were inserted (where possible the participants’ own) with color, scale, format, and placement considered in relation to the understanding emerging. To illustrate, during the analysis of the stroke survivors’ accounts, the acute stroke unit as a meaningful place became manifest. This and the fact that it was the focus of the study led to the acute stroke unit being represented on the map as the central landmass (Figure 5). Other specific places and locales (home, Accident & Emergency (A & E), other wards, the community rehabilitation unit) also emerged and were designated as additional land masses, albeit smaller or incomplete. “Home” was envisaged as a large fertile continent mostly located beyond the map. Considering home in this way contributed to more comprehensive understanding. Home was understood as particularly meaningful as it was the place where the stroke survivors began their narrative, where they left, where their pre-stroke lifeworld was located and where they returned. Considering where it was positioned on the map also helped point toward the stroke survivors’ not-at-homeness in the remainder. Through creating the map and working with the spaces in it, the researcher also began to understand how the stroke unit functioned to hold the stroke survivors apart from their home, pre-stroke lifeworld, the hospital, and “other wards.”

The map of stroke survivors lived through experience of being on an acute stroke unit.
The two seas were meaningful but more abstract spaces, not wholly bounded within geographical place. The sea of “vulnerability and disruption” was located off the north east coast of the stroke unit territory, between the unit and home. This signified the stroke survivors’ disruption from their pre-stroke lifeworld (interspersed in the sea at darkened, deeper sections of water). Orientated on the northern aspect of the map, the “hospital/health care sea” looked to evoke how the hospital/health care space included different ways of thinking about and being “in hospital” that were intertwined with the stroke survivors’ acute stroke unit experience. This involved the spatial practice of being a patient, a sense of diminished control and agency, being processed and moved from place to place while also grateful and appreciative for what the space represented and did to help them.
Within the acute stroke unit territory, the two different but interconnected spaces were arranged. Holding space was placed on the eastern side and portrayed as barren to reflect the significant challenges the stroke survivors experienced as they dealt with the vulnerability and disruption from the stroke, being in hospital, and how basic and fundamental their human, holding needs were because of this. Red text was used to represent the vulnerability, disruption, threat, and concern they experienced. Black text signified what the holding space provided and what this meant. The location of words was also considered. For example, “powerlessness,” “loss of control,” and “helplessness” were signified within the stroke survivors’ experience of being on the unit as embedded and encountered within the hospital space, but also as a result of the stroke. These phrases were therefore placed on the map near the shoreline with the “hospital/health care sea” as well as the sea of vulnerability and disruption (Table 1 also addresses the “coast of intimacy and distance”).
An Example of How Mapmaking Contributed to the Hermeneutic Process and Phenomenological Understanding.
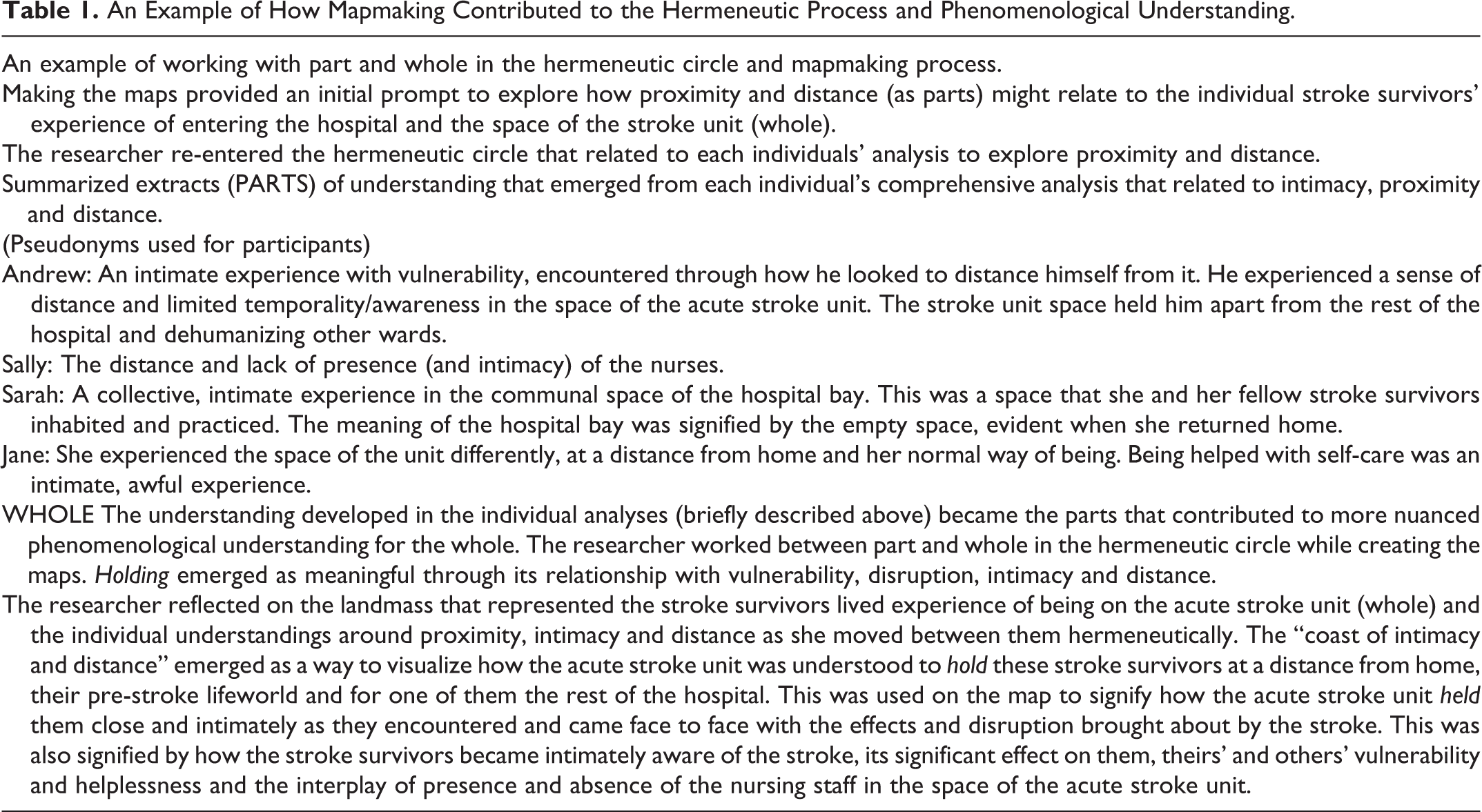
While creating the map, the researcher tried to represent transitional space similarly to holding space by focusing on spatial practices. This unsuccessful attempt provided a prompt to reenter the hermeneutic circle, which in turn bought forth the idiographic nature of the stroke survivors’ transition experience and that these transitions were in fact intertwined with “self.” The final iteration of the map thereby showed the transitional space orientated around a lake that represented the self-related concerns and associated transitions that emerged within the stroke survivors’ experience of being on the unit (i.e., sustaining self, passive relinquishing of self, utility of self, recovery, reassertion and re-emergence of self and transformation of self). Rivers and streams extended from the lake into the surrounding territories. All of the above aimed to represent the western part of the stroke unit as a landscape of fertile growth and transition that signified how the stroke survivors looked to survive, transition, and/or recover in meaningful ways.
While creating the maps, K.S. would take the findings and each individual account and ensure that she could trace, position, and argue how these understandings were represented on the map. Congruent with hermeneutic principles, when this understanding felt impartial or incomplete, she would return to the hermeneutic circle and develop the findings, individual analyses, and maps in a circular, iterative way. In this vein, creating the maps meant being immersed, attentive, questioning, and interrogative. It extended the reflection and dialogue within the hermeneutic circle so that phenomenological understanding could be grasped and made present.
Stage 1—How Mapmaking Contributed to Hermeneutic and Phenomenological Understanding
Emergent understanding and meaning were enriched by mapmaking. As KS played with placement, orientation, and movement between spaces in the stroke survivors’ map, her thinking regarding the acute stroke unit as a lived and practiced space embedded within the hospital/health care space and its relationship with the space of home emerged. As explained in the preceding section, she began to apprehend the interplay between the disruption brought about by stroke and the experience of being on the stroke unit (in meaningful holding and transitional forms). Creating the map proffered a sense of how the spaces related, how stroke survivors moved between and from them, as well as the orientation of self, intimacy, and distance (Table 1) and their meaningful spatial relation.
Mapmaking also assisted in grappling with the complex, temporal, relational, experiential nature of being on an acute stroke unit that became manifest through the health care practitioners’ analysis (Figure 6).

A map of the experience of being a health care practitioner on an acute stroke unit.
In contrast to how the stroke survivors’ map developed, K.S. went through numerous unsuccessful attempts at mapping the health practitioners’ experience. Reflecting on why the phenomenon was hard to grasp helped K.S. become aware of her preoccupation with the health practitioners’ descriptions of their practice and the change and transition they were experiencing. In the phenomenological attitude and working within the hermeneutic circle, K.S. reflected on the practitioners’ claims and concerns, aspirations and objectives, and the discord and harmony intertwined in their accounts. She continued sketching and playing. She began to expand her thinking toward the belonging and authenticity they experienced through their work and how this reflected a meaningful life project that was important for their own authenticity, development, and human realization. The next iteration involved developing the map and associated understanding further by considering the challenges and vulnerabilities the practitioners experienced and how these were meaningfully signified (see Figure 2 for a work-in-progress map). This included reflecting on the relevance of They and resolving how to include the temporal and spatial aspects of their experience. Creating the final iteration of the map (Figure 6) began from the nexus of their work as existential project (represented as the uppermost, central landmass). How this work was challenged, eroded, or threatened from numerous directions was evoked through the tides, seas, and currents their work was exposed to. The They continent was orientated on the map so that it projected into the “sea of change and development” encroached toward their “work as existential project” and was placed near to the land mass that signified their “disrupted sense of belonging” and the “concernful currents” they experienced in relation. This reflected how They were understood to control, shape, drive, and demand the health care practitioners in part, relinquish aspects of their meaningful work. Further insight emerged as K.S. orientated the compass to capture the health care practitioners’ surviving and thriving and the temporal, spatial, and “forming and forging” currents. Throughout this process, K.S. became more attuned to the health care practitioners’ lived experience and her horizon of understanding altered. She began to understand that their meaningful experience encompassed the totality of the map as the health care practitioners navigated and lived through the complex, dynamic space of the unit on a minute by minute, day-to-day basis. Congruent with this, the map provided a sense of what Lefebvre (1991) considered the hyper-complexity of social space: “embracing as it does individual entities and peculiarities, relatively fixed points, movements, and flows and waves—some interpenetrating, others in conflict, and so on” (p. 88). Creating the map pointed toward the produced space 5 of the acute stroke unit for more nuanced understanding (Suddick et al., 2019). This signified the complex interplay between how the health care practitioners lived the space through their actions, practice, and living situations and conceived the ways they needed to practice and nature of “acute stroke unit space” they wished to produce. The researcher began to understand how the meaningful lived, practiced, and conceived stroke unit space, as well as their sense of being authentic practitioners and human beings, were in the process of being eroded and engulfed by an abstract, conceived space. This abstract space represented the changing stroke unit, planned and structured around guidelines and policies, concerned with process, efficiency, and economy, and understood to be controlled by They (management and unnamed others in power).
As articulated here, and similarly to how others have implemented art and poetry, mapping functioned to analyze, represent knowledge, and evoke lived experience (Capous-Desyllas & Bromfield, 2018; Öhlen, 2003). However, as well as providing the researcher with ongoing opportunities to practically engage with her own thinking, the accounts of others and the phenomenon reflectively (Gauntlett & Holzwarth, 2006; Radley & Taylor, 2003) mapmaking was distinct in demanding extensive work with part and whole. Creating the maps thereby extended the dialogue and hermeneutic process, allowing the researcher to play, enter, dwell, and explore the phenomenon through the maps. The maps required her to work visually and hermeneutically with part and whole through the very nature of their construction. They are an embodied representation of the imaginative journey toward the phenomenon which these landscapes flesh out.
Embodied, Phenomenological Re-presentation
Creating the maps was underpinned by the phenomenological endeavor to engage with, bring forth the awakening and sharing of presences (Galvin & Todres, 2012), and “make visible what has not previously been seen” (Lindberg et al., 2016, p. 7). In doing so, the maps helped the researcher understand the lived experience in an embodied way. They successfully embodied the phenomenological understanding of place (space) as any “environmental locus that gathers human experiences, actions, and meanings spatially and temporally” (Seamon, 2013, p. 150) and time, as the maps were made in time and spoke about the past from which they grew and the future to which they point (Wood, 1992). Their creation aesthetically valued and fleshed out the humanity of the experience as they embodied the intricacies and thickness of living and hermeneutic understanding which is relationally alive, open but also ongoing and unfinished (Todres, 2008). The maps provide a sense of the meaning, complexity, texture, and holistic nature of being on an acute stroke unit. Through their inability to be fully grasped, they also keep thinking open and in play.
Embodiment in map form was important to evoke the meaningful lived space of the stroke unit and to present that which is beyond pure mental conceptualization. This methodology acknowledges the epistemological and ontological significance of language and dialogue. However, verbal and written language can only take understanding so far, and creating the maps assisted in employing a visual and spatial language that was congruent with the phenomenological insights emerging. Re-presenting what being on the acute stroke unit was like as an evocative, embodied, living text was also important to convey a seeing-more-than representation (Christensen, 1997) and nonrepresentational speaking, where resonance and re-sounding can abide (Galvin, 2019). Resisting objective, categorization, or a standard, normative presentation, they encouraged and enhanced the researchers’ embodied sensing. Creating the maps reflected a more fundamental transition to be with and “enjoin the other” “into the resoundings of the flesh” (Churchill, 2012, p. 8). As such, they demanded the researcher dwell within each person’s experiential account and phenomenologically feel, attend, and grasp the meaningful lived experience of being on an acute stroke unit. Through the maps embodied and nonrepresentational nature, we propose that they also invite the viewers’ engagement, dwelling, and sensing as a potential path to insight, knowing, and seeing differently.
Stage 2—The Dialogue Within and Between Horizonal Landscapes
The second stage emerged when the dialogue within and between the maps took on a life of its own. Throughout Stages 1 and 2, the maps created an opportunity for communication and dialogue with critical others, first with the research team and later inviting a wider audience to join (i.e., colleagues, students, and health care practitioners). In this vein, each of the maps creatively represented their own form of gestalt
6
and prompt to dialogue about the lived, living space of the stroke unit: The map image is a synthesis of spatially and temporally registered gestalten, each a synthesis in its own right; and to pretend that this whole is no more than the sum of its parts, or that we can do no more than recommend a certain alignment of their priorities, is to reduce our concept of the map to that of a diagram. No degree of thematic constriction can silence the conversation among map signs. The map models the world as an interplay of systems and presents it to us as a multi-voiced analogue, with harmonies and dissonances clearly discernible.…(Wood, 1992, p. 140) This strife which is brought into the rift-design, and so set back into the earth and fixed in place, is the figure [Gestalt]. The createdness of the work means: the fixing in place of truth in the figure. Figure is the structure of the rift in its self-establishment. The structured rift is the jointure [Fuge] of the shining of truth. (Heidegger, 2002, p. 38)
Stage 3—Mapping a Path Toward Practice
The third stage articulates the relevance of the maps within the ongoing life of dialogue for future projections toward practice. Mapping and mapmaking are part of the everyday as a way to make human being in the world shareable (Wood, 1992). We aim to share the maps with stroke survivors and practitioners so that the research can be translated into practice. We envisage that their embodied form will open up thinking, reflection, elicit personal connection, and offer more complex knowing that can translate to health providers’ own thinking, knowing, and ways of practicing (Galvin & Todres, 2011). Congruent with Gadamer (2004) and the aesthetic–hermeneutic significance of art, not necessarily about what is familiar, instead that which leads to knowing more, differently and (historic) self-understanding (Gadamer, 2004). Art as the “world presented in play of presentation does not stand like a copy next to the real world but is that world in the heightened truth of being” (Gadamer, 2004, p. 132).
The maps are unique in their ability to present an incredible amount of information, proffering a sense of holistic understanding on a single page (Wood, 1987). They anchor to place and space and embody the relational and complex nature of the lived experience. At the same time, they offer an otherness: “like shining a light which increases the reader’s sense of contact with this phenomenon without fully possessing it” (Todres, 2007, p. 49).
The maps thereby evoke a presence in between, that moves and is toward (Galvin & Todres, 2012). In doing so, they stand on our shared humanity but also creatively open up a space in-between self and other. They offer a different restructuring which is other than what the viewer expects or perhaps knows; they claim their attention, call for interaction, and encourage dialogue and engagement with the embodied understanding in map form from each viewers’ history, narrative, and perspective. This resonated with the researchers’ motivation to ask those that view the maps to encounter, wander, and navigate the lived space of the acute stroke unit, and extend an invitation to think, play, dialogue, and consider what each may project toward: “This is the very point of the map, to present us not with the world we can see, but to point toward a world we might know” (Wood, 1992, p. 12).
We aim to present the maps in lay publications as well as workshops and a range of gatherings. After a brief contextual introduction, we will invite people to view the maps and talk about them. What they think about the maps will be discussed alongside the findings of the study, with a particular focus on the participants’ voices that provided the maps’ foundations. We will ask those involved to consider what they feel is and is not relevant to them, their practice (where applicable), stroke services, and those involved in stroke unit provision.
For some people, the maps may provide a sense of resonance, recognition, and remembrance. However, we acknowledge that the maps will speak and pose questions to those that encounter them in different ways, some entirely different from the original manner in which the researcher intended. That is the nature of the map. Likewise, if the viewer is lost, dismisses, or sees nothing in the map, there is still something to be said of, or something to be done with the map. To encourage embodied engagement and further exploration of the meaningful experience of being on a stroke unit from different vantage points, and similarly to Kirova and Emme (2006), we also intend to use the maps as a backdrop for others to revise, reword, sketch over, or modify, thereby exploring the possibility and utility of a reimagining of the maps presented here.
Further Considerations
A map will embody the interests of its author and show this, but not that: Even to point is always to point…somewhere; and this not only marks a place but makes it the subject of particular attention that pointed there instead of…somewhere else. The one who points: author, mapmaker; the place pointed: subject, location; the particular attention: the aspect attended to, the theme—nothing more is involved (and nothing less) in any map. (Wood, 1992, p. 24)
This article, as much as it can, looks to lay bare how mapmaking occurred, how the maps were brought to life, and the potential contribution of mapmaking as an evocative and meaningful form of re-presentation. In creating these maps, the researcher has pointed, directed, and turned her gaze and hopefully others toward the acute stroke unit as meaningfully experienced. The maps and the intertwined phenomenological understandings that emerged were brought forth as a result of the researchers’ attentive and extensive dwelling and reflection on what was meaningful, how meaning was signified, and how her horizon of understanding changed and altered as it fused with the horizonal perspective of each person who took part and each collective horizonal perspective (stroke survivors and health care practitioners). As such, this article recognizes the maps as a re-presentation and embodiment of the meaningful lived space of the acute stroke unit brought to the researcher’s consciousness, and not to be mistaken for the horizon and consciousness of another or an objective depiction of the world (Wood, 1987). Congruent with the hermeneutic process, their creation does not exclude other directions that could have been imaginatively evoked or projected toward.
For her own purposes, the researcher wanted to produce something creatively and was encouraged to do so by her supervisors. However, it is important that the map and how it was created were congruent methodologically and that the researchers’ authority as mapmaker did not overshadow the voices of participants (Simons & McCormack, 2007) or the phenomenon. This article has articulated how it was in fact the subject matters’ authority that dominated and was determinative throughout the process of their creation.
It is the person who views the map that does its work, and like with other creative forms, contrary to their aim, they could provoke rather than evoke (Galvin & Todres, 2012) or fail to resonate (Simons & McCormack, 2007).
Cartography and mapmaking traverse an expansive field of practice encompassing science and art, between recording and objectifying the “real world” and developing literary, imagined (Caquard, 2011), fictive, and fantasy worlds. In this study, mapmaking contributed to the study’s epistemological and ontological concerns and brought forth what being-in-the-world, through being-in-the-acute stroke unit was like. Aligned with the above, mapmaking offers underutilized potential for human sciences, understanding health care spaces, narrative storying, and qualitative research methods.
Conclusions
Aesthetic offerings in the unique form of maps were created to evoke the lived experience of being on an acute stroke unit. This was congruent with the philosophical and methodological framework (existentialism, hermeneutics, the sensing body, and affective concerns), and the understanding developed from the narratives of the stroke survivors and health practitioners involved. Mapping offered a path to more comprehensive understanding, ensured that the complex, holistic meaning developed from the research study was expressed, and that justice was done to both the accounts of those involved and emergent phenomenon. They provided an offering that gathered up the messages, signs, symbols, images, scales, and emblems entangled in the map, and in doing so made a coherent and purposeful proposition (Wood, 1992). They are an embodied, living text that allowed the phenomenon to be made present (Willis, 2004).
This article articulates how mapmaking was fulfilled, how it aligned with the study’s concerns, contributed to development of understanding, emergence of the phenomenon and extended the life of dialogue. The maps were an opportunity to dwell and interrogate the interpretation further, a way of creating a space that could be encountered, experienced, lived through, and taken onward. We propose that similar novel ways of working with the development of understanding and re-presentation of findings can be rigorous methods for presencing, embodying, and laying bare the holistic, complex nature of human living so that it can be encountered in meaningful ways and translated to practice.
Maps are invitations. We can read them, read with them, draw and redraw them, use them, share them, add and alter them, enter into them. As representations, they are always partial, always incomplete, and yet they always offer us more than what is held there on paper alone. Maps begin a story. They send us off on new journeys, set our feet moving and our minds racing. Maps inform us and they encourage wonder. Maps give us guidance and direction, and show us the range of a territory, but they can only ever suggest a greater whole. The rest is up to you. (Lewis-Jones, 2018, p. 237)
Footnotes
Author's Note
Pirjo Vuoskoski is now affiliated with Faculty of Sport and Health Sciences, University of Jyväskylä, Seminaarinkatu 15, 40014 Jyväskylän yliopisto, Finland.
Acknowledgment
The authors thank Paul Johnson for his invaluable assistance with Adobe Illustrator™.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Brighton provided a small grant that supported the completion of the study. No grant from any funding agency was received.