
Abstract
Storytelling is perennial to the human condition. We all tell stories and we all bear witness to the stories of others. According to narrative scholars, only certain stories are valorized in contemporary culture, while others go unrecognized. The inability to recognize ourselves and identities in contemporary cultural narratives can contribute to the silencing and muting of certain lives and voices. Young people with life-shortening conditions, such as cystic fibrosis (CF) and muscular dystrophy (MD), are rarely afforded the opportunity to have their stories heard and affirmed in contemporary cultural spaces. In this article, we reflect on the methodological process of engaging in a study known as “Telling My Tale,” that is, a storybook study featuring narratives and artwork by young people with CF and MD. Funded by the Social Sciences and Humanities Research Council of Canada, we critically reflect upon the methodological lessons, advances, and innovations we have learned, including theoretical musings, the process of exhibiting some of the artwork in a public art gallery, challenges faced along the way, analytical conundrums, and the role of technology in artistic creation for participants with limited hand function. In so doing, we hope to further methodological and theoretical development and innovation in narrative and artistic traditions to better center the voices, lives, tales, and experiences of young people with life-shortening conditions.
There is no greater agony than bearing an untold story inside you.
Review of the Literature
The literature on the use of visual storytelling for young people with chronic conditions is not extensive, thus necessitating our retrieval of literature from other populations. Furthermore, there does not seem to be a great deal of consensus on the name and description of this platform. Indeed, researchers simultaneously refer to visual storytelling in diverse ways (Valentine, 2008) as both methodology and method (Rice & Mundel, 2018). Furthermore, the use of both narrative and visual forms of storytelling, and narrating one’s illness experience, is categorized as arts-based research, narrative methodologies, visual methodologies, and visual storytelling (Valentine, 2008). In this methodological and reflective article, we employ the term visual storytelling to refer to the use of both visual and narrative platforms as a useful way in which to narrate and describe the experience of chronic illnesses in childhood.
Reflecting on the lesbian, gay, bisexual, transgender, and queer/questioning community, scholars comment on the critical role of narrative in forging a sense of identity and recognition in society (Rice & Mundel, 2018). For Valentine (2008), the ability to tell a tale—and be heard—is a critical issue of utmost importance. Indeed, he suggests that telling a story might be a form of life and death; loss and grief might result from the inability to tell a story. We make sense of the self in the context of the stories that we tell about our lives (Rice & Mundel, 2018). Closely related, storytelling is deeply tied to time and place in that the tales which we tell are firmly rooted within place, time, and relationality (LaMarre & Rice, 2016). The visual narrative, then, acts as a temporal bridge between the past, present, and future (Rich & Chalfen, 1999; Sairanen & Kumpulainen, 2014).
Valentine (2008) and Rice and Mundel (2018) also remind us not to fall capture to dominant modes of conventional storytelling, such as those that are characterized by a clear protagonist, trajectory of narrative arc, obstacle, and finite, uncomplicated conclusion. For James and Valentine (2008), it is important to recognize that some stories do not end, do not subscribe to these conventional and often simplistic plot lines. Despite an audiences’ need for closure, some stories remain unresolved. As noted below in our reflection section, it is critical to embrace the multiple and polyvocal ways that people tell stories, including those that do not conform to teleological endpoints (Gastaldo et al., 2018; Rice & Mundel, 2018).
Visual storytelling, according to Drew and colleagues, can also be thought of as a child and youth-centered approach. Despite efforts to make interview settings more comfortable for young people, Drew suggests that there is still a need for more methods that help to subvert child and adult structures in research settings (Drew et al., 2010). To better understand children’s lived experiences, the authors combined elements of photovoice and photovoice elicitation to explore what it is like for young people with CF, asthma, and diabetes to live with their chronic conditions. Although the authors did not report upon their findings, they suggest that visual storytelling makes evident elements of their lives that have not previously been discussed (Drew et al., 2010).
James and Valentine (2008) go onto suggest that telling a tale is particularly crucial for marginalized groups that lack a collective narrative in contemporary society. Indeed, if they are not permitted to tell their stories, the vicious cycle of silenced storytelling is perpetuated, increasing the risk that dominant groups might speak on their behalf (Valentine, 2008). Relatedly, according to Carla Rice, storytelling methods are extremely powerful and impactful, holding the potential for systemic change at many levels of influence (Rice & Mundel, 2018). Chronicling marginalized voices can help to work toward a more just future. Rice also reminds that much arts-based research stems from within activist communities seeking social justice (Rice & Mundel, 2018). Indeed, the arts can speak back to destructive societal structures, such as ableism or racism, by exposing powerful relations and generating counterhegemonic perspectives (Gastaldo et al., 2018; Lapum et al., 2012). Visual storytelling also promotes embodied, empathic, and relational encounters. Through the story, there is an entrance to a portal that allows one to see the world of the other (Bach, 2007) and to feel the impact of other’s stories in their own bodies. When stories are shared, they are often able to develop a deep resonance with the other (Bach, 2007)
While it falls under many names—and its place as methodology or method is somewhat unclear—visual storytelling is gradually becoming more extensively employed with marginalized young people, especially those facing long-term health conditions. While visual storytelling no doubt includes many methodological challenges related to feasibility and time, it can facilitate identity building and a sense of oneself in time and space. More critical scholars have encouraged embracing the polyvocality and multiplicity of storytelling, challenging people to suspend their need for easy closures (Galtaldo et al., 2018). Visual storytelling is considered to be a child- and youth-centered platform and is particularly well suited for those facing systemic disadvantage and oppression. Given the emotionally laden content that is often conveyed through storytelling, it is also one that promotes more embodied encounters. Below, we describe a visual storytelling study for young people living with CF and MD known as Telling My Tale.
Brief Overview of Telling My Tale
Drawing on visual narrative methodologies, Telling My Tale is a storybook study for young people living with CF and MD. Indeed, in our lab at the Holland Bloorview Kids Rehabilitation Hospital in Toronto, Canada, the study is colloquially termed the storybook study. CF and MD are very different illnesses. CF is a chronic and progressive multisystem illness. Although the cause of CF is known, there remains an ongoing search for a cure. The average age of survival has increased tremendously over the past several decades in Canada, to approximately 49 years (Stephenson et al., 2015). This is considered a great medical achievement from a global CF perspective since it is 10 years greater than the median age of survival in the United States. Despite these successes, most patients eventually succumb to respiratory failure and there appear to be sex-related patterns of survival. Female CF patients with CF-related diabetes have a slightly greater risk of death (Stephenson et al., 2015). In contrast, MD is a chronic and progressive neuromuscular condition characterized by the gradual loss of function and ability over time. In more advanced stages of neuromuscular degeneration, patients often lose independent ambulatory function (McMillan et al., 2010). Even though CF and MD are very different, there are similarities in these illness experiences with both conditions being chronic, progressive, and ultimately fatal. Further, both groups must grapple with the complexity and existential dilemma of a reduced lifetime (Gibson et al., 2009; Moola et al., 2012). Finally, both patient groups navigate exceedingly complex treatment regimens daily and have regular encounters with biomedical systems (Gibson et al., 2009; Moola et al., 2012). Patients with CF and MD lack societal and cultural narratives about what it means to be a young person with a chronic and progressive illness in culture. Therefore, the purpose of Telling My Tale was to explore how young people with MD and CF chronicle their life stories through art and written narratives. In so doing, we sought to (1) better understand the life experiences and stories of young people with CF and MD through original artwork and storytelling, (2) identify and analyze the narrative conventions that patients with CF and MD use to narrate their stories, (3) explore what themes and experiences these patients convey through art, (4) and contrast and compare CF and MD visual and written narratives.
Ethical approval for Telling My Tale was obtained by four academic hospitals in Southern Ontario. Multiple strategies were used for participant recruitment, including social media postings, word of mouth, clinic letters, clinician suggestion, and advertisements posted on websites. After obtaining informed consent and basic demographic information, art kits were mailed to all participants. In the art kit, participants were prompted to create at least one image and one written narrative per week. However, we informed participants that it was alright to also depart from the list of prompts and that they were free to flexibly engage with the content as they wished. In a few cases, participants with MD relied on technology to assist them with image creation due to limited hand function. The research coordinator phoned or e-mailed the participants on a weekly basis to discuss progress and to troubleshoot any errors. Participants often required slightly more time to complete their storybooks. On completion of the storybook, participants mailed them back to the hospital. After, participants complete a 2-hr semistructured interview about their visual narrative with the first author and research coordinator. Each participant also completed a lifeline activity to confirm central narrative points in their story. During the lifeline activity, participants walked the interviewers through their lives in chronological order, demarcating the major temporal epochs and milestones that were significant for them. Telling My Tale is still in progress, and the data have not been analyzed as yet. The research team is in the process of developing analytical frameworks and, with permissions, has exhibited some of the artwork already. At the end of this study, it is hoped that there will be a broader visual narrative for these patients to share their illness experiences in contemporary social life, thereby promoting greater recognition. In addition to a public art gallery to showcase youth’s artwork, we hope to create a collection of short stories by compiling a book for public education.
Reflections and Challenges on the Methodological Process of Telling My Tale
Even though Telling My Tale is still in progress and will not be completed until 2020, we have already garnered several methodological insights, advances, innovations, and reflections along the way that may have relevance to the global community of qualitative researchers who employ visual storytelling approaches in their studies. These are discussed below.
Challenges With Recruitment
Unsurprisingly, we have noted several difficulties with recruitment. Indeed, difficulty with recruiting child and youth clinical populations has been well-documented in the literature (Burke et al., 2007). While the reasons are unknown, illness exacerbations and associating adverse experiences in the hospital with hospital-based research might serve to detract patients from enrolling in such studies. Through our various means of recruitment, including hospital partners, social media, and MD/CF websites, we have been in contact with 33 potential participants. However, of the 33 potential participants, we were only ultimately able to work with 13. In the footsteps of other researchers at our hospital, we have tried to overcome these barriers to recruitment by broadening the study demographics to include participants from all over Canada. Additionally, we have doubled our efforts to communicate with participants during the study. Depending on the communication needs of the particular patients, as well as research ethics requirements, we either call, text, or e-mail to maintain regular contact with them.
Additionally, our study has a significant arts-based component, including drawing and image-making on a weekly basis. The perception of “not being an artistic person” and the challenges associated with artistic creation might have also served as barriers to participation. Indeed, not seeing the self as an artist might be a notable barrier that requires further investigation. We have tried to overcome this impediment by letting participants know that there is no right or wrong way to engage in artistic creation and that we value all of their art pieces, regardless of their form and content. Thus far, this reassurance regarding artistic creation appears to be an effective way in which to encourage participants to engage in art-making. However, further efforts might be needed to destabilize and deconstruct the term “artist” in the future so that more participants see themselves as able to engage in arts-based research.
Since the study takes approximately 10 weeks to complete and requires some degree of work on a weekly basis, this might have appeared to be too arduous of a challenge for participants. We have tried to address some of these challenges by letting patients know that we will do our best to be flexible and to adapt the protocol based on their needs. For instance, almost all of our participants have experienced bouts of poor health or health-related exacerbations throughout the study protocol, resulting in numerous cancellations. When these health-related exacerbations occur, we make an effort to slow down and encourage the participant to resume the study when they feel able too. In this regard, we make efforts to be as flexible and adaptable as possible and attentive to participants’ daily medical and social realities. Although most of the participants have selected the hospital setting for data collection, we have tried to address this challenge by offering participants a range of study settings to participate in, such as home, community, and hospital contexts.
Interestingly, although we have faced challenges in reaching the consent phase of the study, those participants who did consent tended not to drop out and demonstrated excellent study adherence and loyalty. Thus, although we have faced upfront recruitment challenges, consenting participants have generally adhered to the study. However, the issue of recruitment challenges in pediatric populations is likely to continue to plague our field. Future researchers that use the Telling My Tale protocol should do their best to be flexible and to modify and adapt the protocol to the best of their abilities to meet the needs of participants. For an example of art from Telling my Tale, refer to Figure 1.
Sample of art from Telling my Tale.
Embracing Technology to Create Art
We initially suspected that participants would mainly use the visual arts to self-create their images in Telling My Tale and thus promoted drawing, coloring, and painting. None of our patients with CF have encountered any challenges with image creation thus far, even those with severely compromised lung function. However, a few of our participants with MD have severely compromised hand function. Initially, we envisioned assisting them with visual image creation by acting as conduits for their hands to bring their images to life. However, these participants showed an interest in using their own assistive technological devices—such as computers—to assist them with their image drawing work. For instance, one participant—Layla (code name)—used computer devices to create images of herself in a wheelchair or a wheel trans bus (Figure 2).

Sample of art from Telling my Tale.
These technological advancements and technologically aided image creations were unanticipated and both fascinating and innovative from a methodological perspective. In retrospect, the assumption that every participant would be able to engage in drawing and illustration may have been an ableist assumption that guided the research (Penketh, 2017). Furthermore, had we assisted participants in image creation by acting as their “hands,” we may have unwittingly reinforced the notion of disability as a passive entity (Kuppers, 2001) that lacks artistic agency and license (Penketh, 2017). Indeed, we have learned that extreme variation within one diagnostic category has a great impact on the ability to create art.
In the future, we will make an effort to better employ our critical faculties when designing research protocols so as not to make assumptions about art-making ability. Although the definition of art has been contested historically (Duncum, 2001), we also hope to broaden and expand our definition of what art is to better include technologically enhanced or technologically driven artistic creation as well. Understanding participants’ technological resources needs during the consent phase of the study might also better prepare the team to anticipate art-making requirements as well. We encourage future researchers who take up our protocol to employ broad, inclusive, and liberal definitions of what art is and how it is produced (Figure 3).

Example of using technology to create art in the context of reduced hand function.
Challenges With Visual Analysis
Although we are still deeply embedded within the data collection phase of Telling My Tale, many qualitative pioneers suggest that data analysis and collection are hand in glove, with each informing the other in an iterative process (Gabrium et al., 2012). Consequently, the emerging data analysis should serve to prompt further lines of inquiry during data collection. Thus far, we have noted analytical challenges with the interpretation of visual data. Indeed, analytical challenges during visual data interpretation have been noted by other scholars such as Gastaldo et al. (2018). Most researchers often omit discussions about data analysis or, rather, do not analyze the visual data at all. Alternatively, authors often combine visual data analysis approaches. Thus far, we have found that the analysis of visual materials is poorly described in the existing literature with little in the way of analytical guidance. Although we have not yet chosen our visual analytical approach, we will most likely combine a few approaches to develop a visual analysis template. For example, Gillan Rose’s analysis of visual data is perhaps the most well-known approach, involving both inductive and deductive analysis. Sweet and Escalante in Gastaldo et al. (2018) has advanced a three-phase approach that begins with collaborative meaning-making between the participant and the researcher (Phase 1). In Phase 2, composition, semiology, and discourse analysis occurs to better understand each work of art. Interpretation is based on the location of the object, presenting symbols, as well as the oral and the written narrative. Similarly, Espinoza in Gastaldo et al. (2018) has advanced a three-dimensional, two-phase approach that begins with an analysis of the oral and written narrative. A graphic analysis of the work is then undertaken as well as a projected layer of analysis in which symbol products are analyzed (Gastaldo et al., 2018). Although we have not yet undertaken our visual analysis, we anticipate that this will be layered with challenges. We are committed, however, to not omitting this critical phase and, rather, to explicitly describing and explaining our analytical framework. Thus far, we are blending elements of Rose’s compositional analysis and semiotic analysis including color, size, orientation, expressive content, use of light, signifier, referent, and signified (Rose, 2001).
Managing Issues of Representation and Interpretation in Visual Data
Furthermore, as recommended by several arts-based researchers, we are exercising great caution and care over representational and interpretive issues (Knowles & Cole, 2008). We will engage in a formal visual analysis in the next few months. We will try to reduce interpretive conundrums by asking participants to interpret their images during the interview. This will hopefully better ensure that assumptions do not guide the interpretation of the artwork. In this regard, we employ great care and caution before interpreting images on behalf of the participants (Knowles & Cole, 2008).
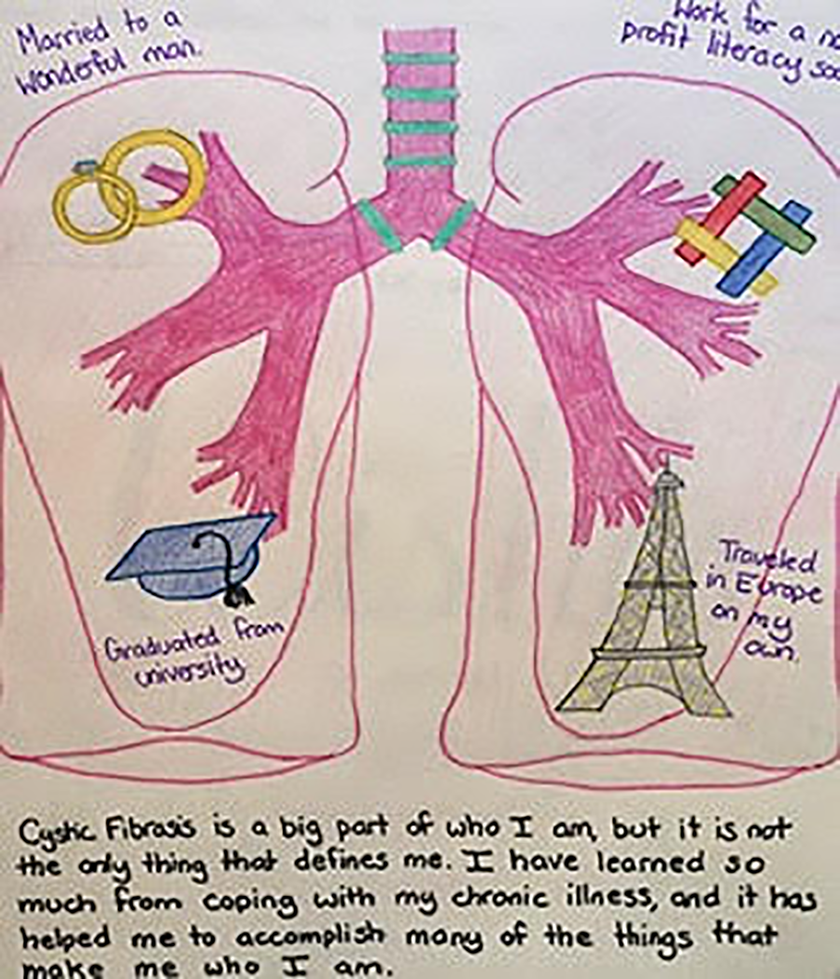
Paying Attention to Literal and Metaphorical Content
In a related vein, we are trying to be very attentive to participants’ use of both literal and metaphoric content. As described by Bagnoli (2009) and Moola et al. (2015), the participants appear to create images that convey both literal and symbolic components of their health and illness experiences. For example, as depicted below, Gretta draws herself walking along a road toward a distant future. A graduation cap is in her hand. The road is not safe, and she can easily fall off. The dress she is wearing is a wedding gown to convey her desire to one day meet a lifelong partner. Although her destination point is unclear, she explained that it represents an educational institute where she hopes to one day complete a university degree without constant health-related challenges that impede her progress (Figure 4). This is just one example of participants’ engagement both with the literal and the symbolic realms (Bagnoli, 2009). We hope to carefully attend to both meanings throughout the study.

Example of an image from Telling my Tale that contains both literal and metaphorical content.
Generating Novel and Unanticipated Information
The ability to generate novel and unanticipated information and knowledge that is worthy of new discoveries and exploration through arts-based research (Rolling, 2015) is a benefit inherent to this tradition. Although none of these were areas of inquiry on our interview guide, the participants appear to be using their artwork to convey gendered relationship experiences, struggles at college and University, as well as changes to the body and the self through the organ transplant process. While it is important not to perpetuate heteronormative assumptions in research agendas, here, young women with CF are recounting gendered relational experiences, characterized by great difficulty disclosing their health status to, in this case, the men that they expressed they wanted to have romantic relationships with. Through their artwork, they display an array of complex emotional experiences, characterized by an effort to protect both the self and the other through nondisclosure. “Pushing partners away” appears to be a common pattern that participants use to ward off the potential relational losses that they might experience if they become intimate with others. Further, almost all of our participants have used their art to convey great challenges while attending college and university. Despite seeking educational assistance from student accessibility services, many of our participants ultimately had to terminate their studies due to the inability to manage both coursework and health-related challenges. As university educators, this surprising finding has been deeply troubling, especially since many of these young people appear to have developed school-related anxiety or phobia in the wake of leaving. Invariably, our research team is recognizing that more structural support is needed at postsecondary institutions for these participants. Finally, unbeknownst to the research team before the study, a few of the participants have revealed through art-making that they have received double-lung transplants. They are using their artwork to convey profound phenomenological experiences with the body, while also illustrating Valentine’s (2008) conceptual postulate about the need to embrace uneasy and messy stories without simple teleological and finite endpoints. Indeed, these stories are unfinished and are almost marked by three lives
Exhibition Design as Knowledge Translation?
Finally, the research team is currently thinking about the role of exhibition design and gallery showcasing as a knowledge mobilization activity for Telling My Tale. After obtaining consent, in November 2018, art from the Telling My Tale study was showcased in a gallery opening at the Holland Bloorview Kids Rehabilitation Hospital. The purpose of the gallery was to use art as a platform for voice to generate critical conversations about illnesses in childhood in contemporary culture. The gallery was extremely well attended by hospital staff, patients and families, and the broader Toronto community with approximately 180 people visiting over the course of 1 week. The gallery received very positive comments in our comment box with people stating that the work was thought-provoking and emotional. Attendees’ emotional response to the artwork speaks to the capacity for arts-based research to generate corporeal and visceral responses for audiences, such as empathy and resonance (Gastaldo et al., 2018). As well, participants whose work was showcased in the gallery suggested that it resulted in a sense of pride and ownership. As curators, it was touching to watch the participants observe others engaging with their artwork. To showcase their sense of pride, they often asked their parents or their care workers to photograph them next to their artistic creations in the gallery. While exhibition design and gallery showcase is far from neutral and has a troubled history of negating the experiences of marginalized groups (Dodd et al., 2004), the research team is currently considering it as a knowledge mobilization activity for the Telling My Tale study. In addition to the healing impact of art galleries on patient’s lives (Camic & Chatterjee, 2013), it has begged us to consider what it means to elevate young people with chronic illnesses to culturally esteemed roles in contemporary cultures such as artist and curator (Figures 5 and 6).
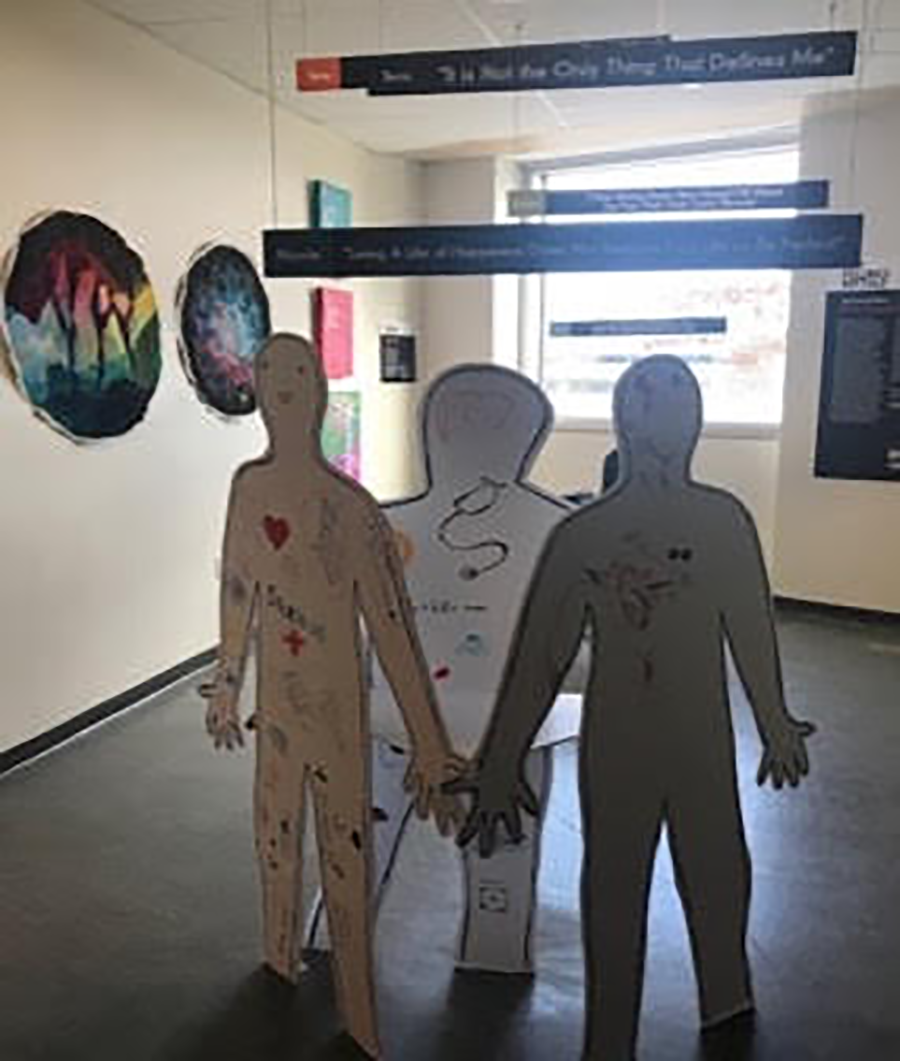
Picture of the gallery.
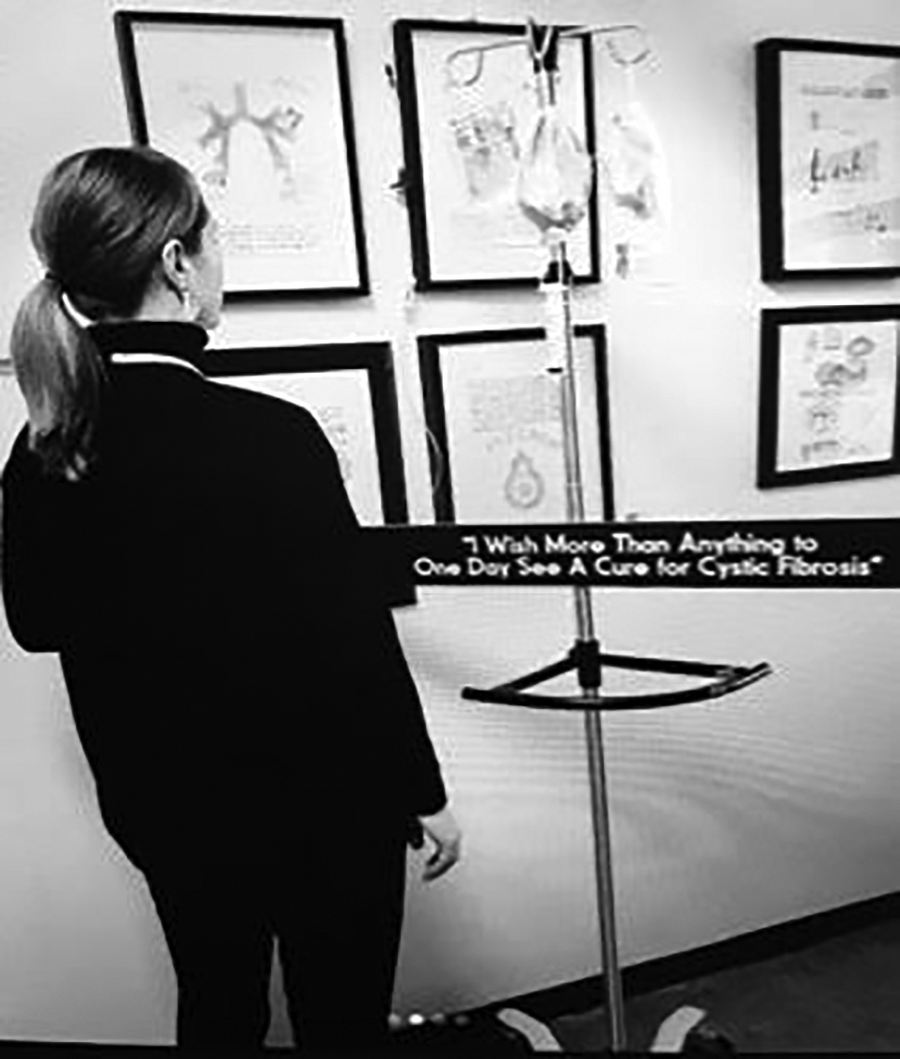
Picture of a student viewing the gallery
Conclusion
According to Valentine, the inability to tell one’s story—and to recognize one’s storied experiences in culture—can lead to a sense of loss and existential dread (Valentine, 2008). When there are no words available in culture to anchor our experiences to others, we are unable to recognize ourselves as viable subjects and the vicious cycle of untold storytelling continues unabated. The storied experiences of young people with life-shortening conditions in Canada, such as CF and MD, are largely untold in culture. Alternatively, medical experts and other outsiders have spoken on their behalf, thus increasing the risk of storied misconceptions and the perpetuation of stereotyped experiences (Valentine, 2008). In this article, the methodological reflections and innovations were chronicled during a SSHRC-funded visual storytelling study known as Telling My Tale. In so doing, the researchers grappled with some of our own methodological and reflexive conundrums. We hope that others will take up, adapt, and modify the Telling My Tale protocol to better attend to the dropped narrative threads of other young people living with chronic and progressive illnesses in contemporary culture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Social Sciences and Humanities Research Council of Canada—Insight Development Grant, in 2016 (SSHRC-IDG).