
Abstract
Focus groups are becoming increasingly popular in research, especially in parent and child research. Focus group interviews allow participants to tell their own stories, express their opinions, and even draw pictures without having to adhere to a strict sequence of questions. This method is very suitable for collecting data from children, youths, and parents. However, focus group interviews must be carefully planned and conducted. The literature on focus group interviews with adult participants is extensive, but there are no current summaries of the most important issues to consider when conducting focus group interviews with children, youths, or parents. This article outlines the use of focus groups in child, youth, and parent research and the important factors to be considered when planning, conducting, and analyzing focus groups with children, youths, or parents.
Introduction
Qualitative research methods have an important role in social science and health-related research. In particular, focus groups and one-on-one interviews are state-of-the-art tools for the development of reliable and valid surveys and questionnaires (Baars, Chaplin, Koopmann, & DISABKIDS Group, 2006; Millward, 2012; Streiner & Normann, 2003). Within the fields of social science and health-related research, focus groups are an accepted qualitative research method because they enable the collection of in-depth data providing more details of the phenomenon under study (R. S. Barbour, 1999). Therefore, focus groups can be used in descriptive or interpretive phenomenology, provided philosophical underpinnings are presented (Bradbury-Jones, Sambrook, & Irvine, 2009).
Focus groups are used to collect data in participatory research, especially when involving young people (Bagnoli & Clark, 2010). In nursing research, focus groups have become increasingly popular (Happell, 2007; Webb & Kevern, 2001), and guidelines for conducting focus group interviews with adults are widely available. However, involvement of young people and small children is almost not addressed at all (Baars et al., 2006; Krueger & Casey, 2009; D. L. Morgan, 1993; Stewart & Shamdasani, 2014).
A focus group interview is described as “a carefully planned discussion designed to obtain perceptions on a defined area of interest in a permissive, non-threatening environment” (Krueger & Casey, 2009, p. 2).
Focus group interviews can be conducted with patients in hospitals, health-care professionals (Shaha, Wenzel, & Hill, 2011), healthy adults, youngsters, and even children as young as 4 or 5 years. This method can also be used with persons with disabilities such as visual or communication impairments (Decarlo, McGwin, Bixler, Wallander, & Owsley, 2012; Markham, van Laar, Gibbard, & Dean, 2009; Visagie, Loxton, Stallard, & Silverman, 2017) or people who have problems with writing or reading (Kennedy, Kools, & Krueger, 2001). Given the current Internet era, online synchronous and asynchronous focus groups are also feasible (Boateng et al., 2016; Krol, Sixma, Meerdink, Wiersma, & Rademakers, 2014; Tuttas, 2015; Zwaanswijk & van Dulmen, 2014). Electronic means facilitate the use of focus groups particularly with vulnerable populations such as, for example, Lesbian, Gay, Bisexual, Transgender and Queer (LGBTQ) teenagers or people with skin conditions. Participants are empowered to take part in group discussions without (physically) sitting in the same room and being visually exposed to the other participants. This anonymity makes it easier for the participants to share personal and sensitive information (Stover, 2012).
Focus groups can be used to create a safe peer environment for children. Focus groups can also avoid some of the power imbalances between researchers and participants, for example, those between an adult and a child in a one-on-one interview (Shaw, Brady, & Davey, 2011). Focus group interviews can elicit the perspective of youths. This method has been used in research with young people, for example, to analyze their experience of alcohol use (Demant & Järvinen, 2006), transition to adulthood (Brannen & Nilsen, 2002; Mello et al., 2009), to explore embarrassment as one of the often-ignored emotions of young people (vanTeijlingen et al., 2007) or sectarianism in Northern Ireland (Leonard, 2006). They are valuable for designing health programs in child and adolescent health-care research (Heary & Hennessy, 2002; Peterson-Sweeney, 2005; Wyatt, Krauskopf, & Davidson, 2008) and instruments to assess quality of care (Butt et al., 2009; Moran, Kelesidi, Guglani, Davidson, & Ford, 2012). However, it is essential to consider the specific characteristics of the target population. The purpose of this integrative literature review was to describe the use and the relevant factors related to conducting focus group interviews with children, youths, and parents.
Method
A literature search was conducted in PubMed Central, ERIC, and PsycINFO with the search terms “focus groups/methods” or “focus groups/utilization.” Additionally, terms such as “child,” “youth,” “adolescent,” “parents,” “child health research,” “pediatric research,” “paediatric research,” “analysis,” and “child development” were used. Limits included publication dates within the last 10 years and English and German language publications. Reference lists, bibliographies, and books were hand searched, and books about focus group interviews and child development were included. The limit of 10 years was chosen as the inclusion of children as participants in research has changed during the past decade and therefore we found it relevant to look at the newest studies. Older studies from the reference lists were included if they added significant contents. Studies were included if there was a description of how the focus groups with children, adolescents, or parents were prepared and conducted. The literature search and the data extraction were conducted by the first author.
Results
One-hundred and twenty eligible articles were found. Figure 1 shows the flow diagram of the literature search. All articles were expert opinions. The articles were grouped in three categories: Article with focus groups or analysis of focus groups as main issue. Article where focus groups were used for data collection and details about the use of the method were described and discussed. Article where focus groups were used for data collection and at least one detail about the use of the method was described but not discussed.
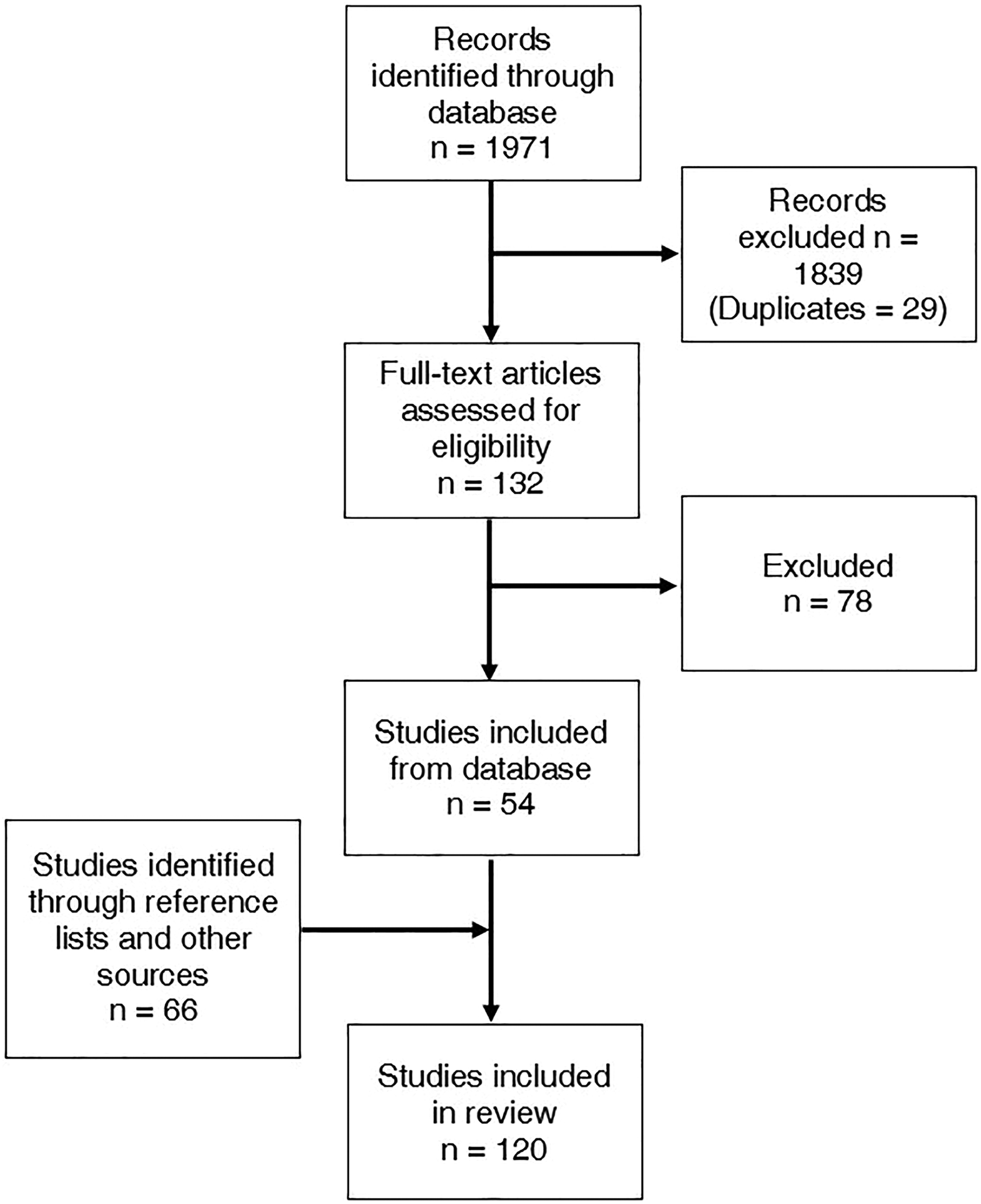
Flow diagram of literature selection process.
Most of the used articles were in Category A. Only 27 in Category B and 9 in Category C.
Preparation of Focus Groups
When preparing a focus group interview several issues have to be addressed. First, the participants have to be chosen. Inclusion and exclusion criteria need to be determined according to the research question, the number of participants per focus group needs to be defined, and the way these participants can be approached should be identified. Second, a questioning strategy and interview guide need to be prepared. Time and place of the interviews has to be determined as well as the length and number of interviews in total.
Table 1 provides an overview of basic points in planning and preparing focus groups. More details to preparing and conducting focus groups are elaborated in the following sections.
Selection of Participants
Participants are typically selected using either purposive or convenience sampling (Stewart & Shamdasani, 2014). In purposive sampling, the researcher chooses individuals who fulfil inclusion criteria corresponding to the objectives of the study. The participants need to have some experience with the study topic, be within the appropriate age range, or have similar psychosocial characteristics (R. Barbour, 2018; Krueger & Casey, 2009; Rabiee, 2004).
In convenience sampling, persons who are conveniently accessible and have experience with the study topic are invited to participate in the study. Typically, school classes, religious communities, youth groups, or groups of parents who are meeting regularly are representative of such participants (Dupper, Forrest-Bank, & Lowry-Carusillo, 2015). The first step in participant selection is determining whether candidates meet the predetermined inclusion criteria (e.g., age, gender, and place of residence; Hinojosa et al., 2014; Krueger & Casey, 2009).
With children, significant differences in communication styles and knowledge levels are noted at various ages (Baars et al., 2006; C. D. Clark, 2011; Doherty & Hughes, 2013; Feldman, 2011). It is important to consider that not all children develop in a linear way. Their development also depends on the culture and social stratum they belong to. Children should not be perceived as “small adults.” They are active social beings with their own social relationships and meanings (Hendrick, 2015; Prout & James, 2015). Thus, children can be valuable partners in focus groups.
Children as young as 4–5 years old are capable of participating in focus groups provided the methodology is adjusted accordingly. Using playful group activities instead of conversation can facilitate the participation of younger children (Cammisa, Montrone, & Caroli, 2011; Greene & Hogan, 2005). Children in kindergarten and first grade are able to discuss their opinions with each other. They are beginning to understand metaphors (Stites & Ozcaliskan, 2013). At the age of 6, children can provide brief accounts of their thoughts and preferences. Preschoolers start to form friendships. Their behavior with their friends will differ from their behavior with children who are familiar but not friends (Damon, Lerner, Kuhn, Siegler, & Eisenberg, 2008). They understand symbolic functions, meaning that they can, for example, use the word car and understand what is meant without having a car standing in front of them, and they understand that a toy car represents a real car (Feldman, 2011).
According to Jerome Bruner’s social theory (McLeod, 2018), important cognitive changes take place between 7 and 8 years of age (Doherty & Hughes, 2013). Children’s language ability improves. Between 7 and 11 years, children begin to use logic to solve problems. Children are able to judge their own abilities and to compare them with others, and they develop self-esteem. Membership in particular groups becomes more important (Damon et al., 2008; Doherty & Hughes, 2013; Feldman, 2011). Their ability to control their attention improves (DeHart, Sroufe, & Cooper, 2004). By the end of middle childhood (age 10), children are adept at conveying their thoughts and feelings to one another (DeHart et al., 2004). They become involved in social activities in and out of school, but mostly with others of their own gender. Girls construct their own rules and social codes and discuss them with each other, but boys avoid talking about relationships (Doherty & Hughes, 2013). Children recognize the importance of shared values and social understanding, and friends are expected to be loyal to one another (Damon et al., 2008; DeHart et al., 2004; Feldman, 2011). They also become able to understand what other children are thinking (DeHart et al., 2004). Conversations show more “give and take” as children actually start responding to each other (Feldman, 2011).
At 12 years and older, children show an increased ability to engage in abstract reasoning, verbal and mental problem-solving, and decision-making using deductive logic (Vaughan & Litt, 1990). Their language and memory capabilities increase (Feldman, 2011). Adolescents begin to think and reason abstractly, and their self becomes increasingly differentiated (Damon et al., 2008; Feldman, 2011). Their memory capacity grows, and their ability to divide their attention between different stimuli at the same time improves. They start thinking hypothetically. They know more about the world, and their memory capacity grows. Adolescents’ new cognitive abilities enable them to imagine what others think about them (Feldman, 2011).
Grouping children according to age rather than familiarity with other members of the focus group can therefore be essential to group dynamics and discussion. However, children may feel safer and more willing to express their opinion if group members are familiar to them (Fielden, Sillence, & Little, 2011; Hoppe, Wells, Morrison, Gillmore, & Wilsdon, 1995; McGarry, 2015). Children typically strive to make peers understand their thoughts and feelings, and they also attempt to understand other children’s perspectives. Because of children’s efforts to achieve mutual understanding, adults who are “listening in” have a unique opportunity to discover the meaning of events from the children’s perspective and to study their behavior in action (Kennedy et al., 2001).
In addition to age, gender can influence the compatibility of children in a group. Gender differences might arise in groups containing older children and teenagers or in discussions of gender-specific topics (Fielden et al., 2011; Heary & Hennessy, 2002; Kennedy et al., 2001). For older children and teenagers, interest in the opposite sex and differing interests, desires, and attitudes can negatively affect group dynamics in mixed-gender teenager groups (Heary & Hennessy, 2002). It is recommended to hold single-gender focus groups with teens who are not familiar with one another and whose ages differ by less than 2 years to obtain more diverse opinions and elicit fruitful conversations (Daley, 2013).
Not only can the gender of the group participants influence the responses of the focus group participants but so can the gender of the focus group moderator. Depending on the study topic, a moderator with the same gender as the group members in single-gender groups can be advantageous (Daley, 2013; Yager, Diedrichs, & Drummond, 2013).
Parents appreciate opportunities to share their own stories. Therefore, focus groups are highly recommended to obtain parents’ views of a service (Teare & Smith, 2004). Special arrangements might have to be made if parents attend the interviews together with their children. Additional assistance may be needed to keep the children occupied during the interviews (Hjalmhult, Glavin, Okland, & Tveiten, 2014; Patterson & Kelly, 2005).
Questioning Strategies and Interview Guides
For children, concrete questions phrased in simple language should be used throughout the focus group (Lund, Helgeland, & Kovac, 2016; Sandberg et al., 2017). Particularly, younger children may have difficulty understanding excessively general or vague questions. Questions starting with “what” or “how” are preferred to questions starting with “why” or to questions requiring “yes” or “no” answers. Using prompts such as “What does everyone else think?” “Do others have different thoughts?” “Tell me more” or “How interesting” can improve the flow of a discussion, especially with shy individuals (Lund et al., 2016). Expressions such as “Great!” “Terrific!” or “Cool!” should be avoided because they may discourage the child from telling the parts of the story that are less cool (Fargas-Malet, McSherry, Larkin, & Robinson, 2010). Questions should not be repeated, as children might think their first answer was somehow wrong and then change their response. Long pauses before responding should not be interrupted (Lund et al., 2016). If young children become excited and begin talking simultaneously, it may be useful to address each participant by name (Gibson, 2007; Kennedy et al., 2001). Using nonverbal feedback such as nodding or raising the eyebrows in surprise can help shy children feel secure (Lund et al., 2016). To better understand a child’s intended meaning, participatory techniques, such as role-playing scenarios, can be helpful (M. Morgan, Gibbs, Maxwell, & Britten, 2002). For focus groups with parents, semistructured and open-ended questions about their experiences or opinions can facilitate the discussion (Aylaz, Yılmaz, & Polat, 2012).
When planning the interview guide, it is important to keep the purpose of the study in mind. The questions should be phrased in a way to elicit responses that lead to discussion (Krueger & Casey, 2009). Pretesting the interview guide is recommended (R. Barbour, 2018; Millward, 2012).
By adhering to the guide, the moderator can address all the relevant topics and issues during the group discussion, but it should still be flexible enough to pursue unanticipated yet relevant issues that may arise during the discussion (Wong, 2008). For example, when examining the reasons for sedentary rather than active behavior in kindergarteners, Cammisa, Montrone, and Caroli (2011) found that not only the environment of the kindergarten but also the parents’ and teachers’ fears that the children could get hurt when playing outside were important considerations.
At the end of a focus group, adult participants are often asked to summarize the discussion. Small children’s cognitive skills are generally not sufficiently developed to perform such an analytical activity (Kennedy et al., 2001). Instead, the moderator should review any comments from the group to ensure that they have been understood correctly (Kennedy et al., 2001). An additional way to raise points that the participant did not want to bring up in front of the group (e.g., writing notes) should be offered (Coyne & Carter, 2018).
Timing
The timing of the interview should be appropriate for all group members (Beyea & Nicoll, 2000). With children in particular, the time of day must be carefully planned because fatigue and restlessness typically occur at the end of the day, and children might need to complete homework in the evenings (Kennedy et al., 2001). Weekends, especially Saturday afternoons, or lunchtimes are preferred (Dowling, 2014; Kennedy et al., 2001). For parents, different times of the day and different days of the week for participating in the focus group interview should be offered. Focus groups may even need to be held at night when working parents are involved (Mandinach & Miskell, 2017). Parents of a sick child may have difficulty finding someone to care for the child during the session, especially if special care is required. In a survey conducted by Teare and Smith (2004), parents overwhelmingly preferred to attend focus groups while their child was in the hospital.
Parents of school-age children should be able to attend a focus group while school is in session, but if the focus group is held after school, the children should be supervised, for example, by their teachers (Baker-Henningham, 2011; Gregg, Rugg, & Stoneman, 2012). Parent and child focus groups could also be planned in parallel (Sommer et al., 2017).
Setting
The best place to conduct a focus group interview is culture-specific and should be carefully considered. Settings need to take into account the specific needs of the participants (i.e., healthy or sick children, youths, or parents). The best place for focus groups will differ between healthy schoolchildren or sick children or their parents. When children are involved, safety must be ensured, for example, whether the children can visit the bathroom on their own or whether an adult has to accompany them should be clarified (C. D. Clark, 2011; Kennedy et al., 2001). It is essential that the place is familiar and accessible to the children and their families (Lúcio, 2015; Neely-Barnes, Graff, Roberts, Hall, & Hankins, 2010; Sandberg et al., 2017). M. Morgan, Gibbs, Maxwell, and Britten (2002) recommend holding focus groups with children in an informal nonschool-like setting, such as at a community center. However, Cammisa et al. (2011) and Chan, Lam, and Shae (2011) recommend implementing focus groups in classrooms with teacher involvement. It is argued that teachers are important familiar adults. Their presence contributes to avoid any shyness among the children that may occur in an unknown environment. Children appear to be more attentive and serious in school-like rather than a home-like settings (Kennedy et al., 2001). Children and youths could be given a choice where they prefer the focus group interview to take place (Coyne & Carter, 2018; Kuchah & Pinter, 2012). When conducting focus groups with sick or chronically ill children, a hospital setting might discourage group discussion by emphasizing the patient–professional relationship (Gibson, 2007).
Parents feel comfortable in a location previously known from counselling or prior meetings (Buus, Caspersen, Hansen, Stenager, & Fleischer, 2014; Calvete et al., 2014; Heary & Hennessy, 2002). The premises of a grammar school with an additional room for the children of attending parents are also considered a suitable venue (Patterson & Kelly, 2005). Kennedy (2001) also suggests churches and shopping malls besides the already mentioned community settings.
Length and Quantity of Interviews
The length of the interviews depends on the age of the participant. Table 1 gives an overview on how long the interviews in each age range can be. For the amount of interviews, a rule of the thumb is to conduct three or four focus groups and then assess whether saturation has been reached. Saturation describes the point at when there is repetition of themes, and additional interviews will not provide any new information (Krueger & Casey, 2009; Parker et al., 2012; Prior & Van Herwegen, 2016; Wong, 2008).
Overview of Main Points for the Preparation of a Focus Groups Interview With Children and Youths.

Ethical Issues
Ethical considerations in conducting focus groups with children, youths, and parents do not differ from guidelines for other qualitative research. Focus groups need the approval from an institutional review board. That means that the proposal including the details of the study has to be submitted for review to ensure that the standards of human subject research are met (C. D. Clark, 2011; Krueger & Casey, 2009). The participants of the study must be informed about the advantages and risks of the study, that study participation is voluntary, that they can quit at any time and that the contents of the interviews and the research data are treated as strictly confidential.
For every study, consent from the participants is mandatory. When participants provide informed consent, it is assumed that they have received adequate information regarding the study, understood the information, and still voluntarily choose to participate (Heary & Hennessy, 2002; Lebet, Fineman, Faustino, & Curley, 2013; Polit & Tatano Beck, 2008). Information and consent form need to be easily understandable (Cocks, 2006; Griffiths, Stenner, & Hicks, 2014; Shaw et al., 2011). For children, the overall research goal is not always easy to understand. To simplify information about the research, the description of the study procedures could be supported with pictures or dialogues held with the children to be sure, they understand the purpose of the study and their role in a focus group interview (C. D. Clark, 2011).
As smaller children cannot consent, the concept of “assent” is frequently used. Cocks (2006) defines “assent” as a verbal or nonverbal confirmation that participants have grasped “the relationship between the researched and the researcher,…trust within that relationship and acceptance of the researchers presence” (p. 257). The regulations depend on the countries or states where the study is conducted. In the United States, teenagers under 18 years assent, over 18 years they consent (U.S. Food and Drug Administration, 2015a). In European countries, young people from the age of about 14 years can consent, smaller children assent also ( European Parliament v. Council of the European Union, 2014). For studies where the participants have not reached the age of majority, permission from parents or legal guardians is mandatory (Peterson-Sweeney, 2005). Depending on the internal review board, consent from one or both parents is required. If one parent is the only legal guardian, confirmation may be necessary when giving consent to the study. The ethical review board will specify steps to take in case one of the parents has given consent, but the other is unavailable (Nelson et al., 2013; U.S. Food and Drug Administration, 2015a, 2015b). There are several templates of assent and consent forms available in the Internet, for example, on the site of the World Health organization (2017).
As focus group participation requires a certain effort, incentives to motivate participation and/or compensations can be offered to children, youths, and parents (Hinojosa et al., 2014). Participants may incur financial and emotional costs to participate, including childcare, traveling, staying inside on a beautiful day, and apprehension about discussing sensitive topics (C. D. Clark, 2011; Krueger & Casey, 2009). The most common incentive with youths or parents is monetary reimbursement, which is advantageous because participants immediately recognize its value. Incentives can also be gifts such as food, snacks, or a full meal. Parents might appreciate respite care for their children during the interview instead of incentive payment (Neely-Barnes et al., 2010). However, the type of incentive must be adequately described in advance to avoid disappointment. Reimbursement of children can assume the form of a gift certificate or voucher (Dowling, 2014; Kennedy et al., 2001; M. Morgan et al., 2002). Online gift certificates are popular with teenagers as they can purchase items from the Internet without having to go to a store (Efken, 2002). Gibson (2007) suggests asking children of a similar age what they believe is the most effective incentive to participate in a study.
Investigators should be aware that monetary incentives can influence an individual’s willingness to participate in the study and so have to insure themselves that they are not putting pressure on the participants when deciding to participate or not (Seymour, 2012). Incentives in research are forbidden in certain countries; therefore, researchers should inquire with the local ethics committee to determine what is permissible.
Conducting Focus Groups
Role of the Moderators
The success of the focus group partially depends on the moderator. Conducting focus groups requires a great deal of talent, skill, and knowledge regarding group dynamics, communication techniques, and the strategies most useful for the study (Beyea & Nicoll, 2000; Greene & Hogan, 2005; Krueger & Casey, 2009). Moderators need an excellent ability to make all participants feel welcome as part of the group to promote meaningful exchange (Beyea & Nicoll, 2000; Prior & Van Herwegen, 2016). Ideally, two individuals conduct the focus group together, with one as the moderator and the other as a notetaker and assistant (Beyea & Nicoll, 2000; Krueger & Casey, 2009; Prior & Van Herwegen, 2016; Shaha et al., 2011). The focus group assistant manages the technical equipment, observes group dynamics, and takes field notes (Bender & Ewbank, 1994; Drahota & Dewey, 2008; Krueger & Casey, 2009; M. Morgan et al., 2002). In focus groups with children, a third person is recommended to attend to children who may want to leave the focus group before it ends or to accompany them to the bathroom when needed.
There are specific challenges to interviewing children. They can be inattentive or slow in their responses, they may lose interest, or they may withdraw from an adult who is too dominant. For younger children, the novelty and presence of unknown adults can lead to anxiety. Therefore, attention to these details is essential. Facilitating a balanced discussion can be challenging for moderators (Hoppe et al., 1995). The moderator has to find a way to reach the children to establish an equal footing. He should adjust his or her vocabulary to the child’s level (C. D. Clark, 2011). A child-friendly demeanor, including patience, warmth, humor, and flexibility, is an ideal characteristic of a moderator (Kennedy et al., 2001). To balance between directing and facilitating responses, the moderator should relinquish “control” to ensure that children are able to share their unique insights on their own terms (Kennedy et al., 2001; Moffat, Dorris, Connor, & Espie, 2009). Interactive performance in focus groups with adolescents can help to overcome discomfort and shyness (Norris, Aroian, Warren, & Wirth, 2012). Alternatively, an older teen can conduct the group. It is, however, important to provide the teen moderator with special instructions and considerable practice prior to the focus group (C. D. Clark, 2011; Coyne & Carter, 2018; Krueger & Casey, 2009). To better empathize with teens, moderators need to know the “world” of the teenagers. This may include the music they listen to, the Internet sites they visit, what is trendy at the moment, which series or movies are popular, and so on (Efken, 2002). Kuchah and Pinter (2012), Lund, Helgeland, and Kovac (2016), and Berggren et al. (2017) spent time with the participants doing confidence-building activities such as playing sports or games or just participating in their daily life in kindergarten prior to the interviews.
Seating the Participants
Seating participants at a round or oval table is recommended, as this setup allows them to see and hear each other (Beyea & Nicoll, 2000; Wong, 2008). Smaller children might prefer to sit in a circle on the floor (Greene & Hogan, 2005; M. Morgan et al., 2002). It can be helpful to seat more assertive children, youths, or parents near the moderator and quieter individuals across from the moderator. With this seating arrangement, more outspoken participants can be given nonverbal cues, such as the moderator turning slightly away from them, and the moderator can maintain better eye contact with shy participants to encourage them to talk (Krueger & Casey, 2009). Because of the spontaneous nature of children’s responses, failure to document relevant comments due to technical problems, such as low audio-tape sound quality, is likely. Occasionally, an individual child’s behavior, such as silence due to shyness or an inability to focus, can limit the participation of the entire group or challenge the moderator’s skills (C. D. Clark, 2011; Kennedy et al., 2001).
Introduction and Arrangements
Parents can feel reluctant to leave their child at a focus group. Therefore, moderators should introduce the parents and provide sufficient time for them to become acquainted with the environment. Parents need important information reiterated such as the time to collect their child (Gibson, 2007). Should parents continue to feel reluctant in leaving the child at the focus group, additional arrangements are needed. In some situations, the presence of caregivers or parents is appropriate or even necessary. If the child is afraid to stay alone or in the case of the participation of a disabled child, the presence of caregivers or parents can be beneficial. These children may also have specific communication or support needs requiring the presence of a caregiver or parent. In this case, the attending caregiver or parent needs to be coached carefully about their role within the focus group. The moderator should then ensure that these caregivers or parents keep their neutral role and do not attempt to influence or interpret the participants’ responses (Shaw et al., 2011).
Moderators should welcome the participants, restate the purpose of the focus group, establish rules for group behavior, and take note of any special arrangements (Wong, 2008). The moderator must make sure that all exchanged information stays in the group. If the participants do not know each other, a pseudonym name or not using names at all can be helpful (Krueger & Casey, 2009).
Children can be asked whether they want to suggest any other rules (Griffiths et al., 2014; M. Morgan et al., 2002). In focus groups with children, moderators are recommended to introduce themselves with their first name and accept being addressed informally. This step will help children perceive their relationship with the moderator as more informal than their relationship with their teachers (Cammisa et al., 2011; Gibson, 2007; M. Morgan et al., 2002). The children should be informed that they do not need to raise their hand to talk and that they can ask to go to the bathroom (M. Morgan et al., 2002).
Using icebreakers can make it easier for children to start the discussion (Coyne & Carter, 2018; Coyne, Hayes, & Gallagher, 2009; Daley, 2013; Fielden et al., 2011; Greene & Hogan, 2005; Griffiths et al., 2014; McGarry, 2015; Moffat et al., 2009). This may involve something simple, such as making and wearing their own name badges, drawing pictures, or listening to themselves speak on tape. Each participant, including the moderators, should have an opportunity to share some information about themselves, such as their age and primary interests. Activities like these can help children feel relaxed and provide each child the opportunity to contribute to the focus group.
Besides questions, other ways of engaging children before or during an interview are needed. The focus group should not stick to conversation alone (C. D. Clark, 2011). Moderators of focus groups with children should integrate seeing, touching, and moving about. Such activities may include to ask children to list things, rate items, sort or draw pictures, create mind maps or flowcharts, dream, or use their imagination (Berggren et al., 2017; Cammisa et al., 2011; C. D. Clark, 2011; Davies & Robinson, 2010; Krueger & Casey, 2009; Moffat et al., 2009). Ronen, Rosenbaum, Law, and Streiner (2001) had good success using playdough as a research tool. Playing with toys has a positive and relaxing effect on children (M. Morgan et al., 2002). Flash movies could be used as vignettes when doing focus groups with sensitive topics, for example, child abuse (Chan, Lam, & Shae, 2011).
Young people may hesitate to talk to each other. This can be addressed by actively involving them in the research, for example, by planning different activities for other kids and then to discuss what they like best about each activity (Krueger & Casey, 2009; M. Morgan et al., 2002) or developing a campaign including a slogan or drafting an advertisement for a special topic (Colucci, 2007). They could be asked about their opinion on a topic like how to prevent bicycle accidents or about risk factors to obesity (L. Clark, 2009). Having a meal together can help in getting to know the group before the focus group starts (Sullivan-Bolyai et al., 2014). Parents can become more engaged in a focus group by starting the discussion with a story about their child or talking about their experience with their child.
Data Collection and Analysis
As there was no special literature on analyzing focus groups of children, youths, or parents, this section was written on the basis of general literature about analyzing focus groups.
Data Analysis
The analysis of focus group interviews must fulfil four critical qualities: systematic, verifiable, sequential, and continuous. A systematic analysis is defined as an analysis in which a predetermined and sequential process is followed. To provide an audit trail, the analysis plan must be documented in a reproducible manner that is understandable to all members of the research team. For a continuous analysis, the first focus group is treated followed by subsequent focus groups until no new ideas, categories, and themes emerge (Krueger & Casey, 2009).
The most commonly used analytic techniques are grounded theory analysis (R. Barbour, 2018; Strauss & Corbin, 1998), thematic analysis (Shaha et al., 2011), and content analysis (Mayring, 2003). Grounded theory analysis is characterized by three stages (Strauss & Corbin, 1998). In the first stage, also referred to as open coding, the data are compiled into small units. A descriptor, or code, is attached to each of these analytic units. During the second stage, also termed axial coding, these descriptors/codes are grouped into categories. Finally, in the third stage, also referred to as selective coding, the core category is identified and the association with all other themes is developed. Constant comparison is used to identify similarities and differences (Strauss & Corbin, 1998). Thematic analysis actually refers to the first two steps of the grounded theory analysis. The transcripts are coded and themes are identified (Coyne & Carter, 2018; Shaha et al., 2011). A special form of thematic analysis is template analysis. The principle of the template analysis is that the researcher produces a coding template with the identified themes of their data. This template is then applied to further data. The codes will be modified and added to when analyzing the next transcripts (Brooks, McCluskey, Turley, & King, 2015). Content analysis, as described by Mayring (2003), creates smaller blocks of data. A code is attributed to these data blocks, but instead of creating a theme from the codes as in constant comparison analysis, these codes are categorized into similar groupings and then counted (Mayring, 2003; Onwuegbuzie, Dickinson, Leech, & Zoran, 2009).
Another possibility, especially in analyzing focus groups with children, youths, or parents is the ethnographic analysis. Ethnographic analysis focuses on the particularities of the situation under study and in the participants rather than the analyst’s perspectives. The data are presented as accounts of social phenomena or social practices. The data are used as a window to the lives of the research participants (Wilkinson, 2016).
Analyzing transcribed data can be performed manually or using analytical software such as ATLAS.ti (8.0), NVivo (12), NUD*IST (6.0), and MAXQDA (18.0.0). In manual analysis, the transcripts are printed, and the pieces of paper are then cut into relevant sections or the important sections are highlighted manually or by computer. To identify the transcript corresponding to each piece of paper, each transcript is printed on sheets of different colors, and the lines of the transcripts are numbered (Krueger & Casey, 2009). In classical content analysis, the quotes are then arranged into categories. These categories may need to be divided into subcategories or combined into a larger category (Krueger & Casey, 2009). Throughout the analysis, the main research question or study purpose guides the researcher’s focus (Krueger & Casey, 2009).
Videotaping the focus group interview can support the analysis process (R. Barbour, 2018). When using audiotapes, the field notes of the nonverbal behavior taken by a second researcher should be analyzed in context of the discussion (Kidd & Parshall, 2000). Drahota and Dewey (2008) advocate using a sociogram to conceptualize group dynamics, compare focus groups, and reflect on moderator techniques. In a sociogram, which is a pictorial reflection of the flow of a discussion, arrows are used to depict the number of times a topic moves from one group member to another (Drahota & Dewey, 2008).
Group interactions and processes and the way how opinions might have changed during and through the discussion should be assessed, discussed, and analyzed (Drahota & Dewey, 2008; Kidd & Parshall, 2000; Kitzinger, 1994; Massey, 2011; Rothwell, 2010; Twinn, 2000). Focus groups should be analyzed as planned discussions in a specific and controlled context and not as a naturally occurring discussion (Smithson, 2008). The Emotional Group Culture Categorization System developed by Rothwell, Siharath, Badger, Negley, and Piatt (2008) is a useful framework for analyzing these interactions and processes.
Like in every research, methodological rigor has to be assured. To achieve trustworthiness in qualitative content analysis, Lincoln and Guba describe different techniques. Trustworthiness involves credibility, transferability, dependability, and confirmability (Graneheim & Lundman, 2004; Lincoln & Guba, 1985). Internal consistency of the coding can be increased if the person who conducts the analysis participates in all the focus groups and communicates regularly with the other members of the research group while the analysis progresses. To assess content validity, a second analysis could be conducted and comparison with other literature that show similar findings increase the confidence in the validity of findings and constructs (Kidd & Parshall, 2000). Another possibility is to present the analyzed findings to the original groups to ensure that their views were captured correctly (Kagaari et al., 2017; Parker et al., 2012; Ronen, Rosenbaum, Law, & Streiner, 2001).
Children, youths, and parents can be involved in the analysis. Especially with children and youths, it’s important that their views are captured from their sight of the world. They can be asked to code and group the generated data into categories or themes that they chose by themselves (Gillett-Swan, 2018). Children’s perspectives or views should be seen as a standpoint from which analysis proceeds (Coyne & Carter, 2018). Foster-Fishman, Law, Lichty, and Aoun (2010) developed a data analysis method called the ReACT to effectively engage youths in the data analysis process. The method uses a sequence of games to engage the youths in the three phases of data analysis (data reduction, data organization, and conclusion/verification).
Another important issue in analyzing qualitative data is the self-reflection on the part of the researchers. They should actively reflect upon and articulate their position and views or perspectives, so that the interpretation and results of the data can be better understood (Sutton & Austin, 2015).
Transcription
Focus groups are usually recorded with audio- or videotapes and are subsequently transcribed (Krueger, 2006). Unlike adults, children often appear to be unconcerned about being audio- or videotaped (Chan et al., 2011; Kennedy et al., 2001). There is also the possibility to capture the group discussion by memory, taking field notes, or writing flip charts (Krueger & Casey, 2009; Moffat et al., 2009). Taking notes can complement the audiotapes with observations and behaviors that are not captured by the tapes. When discussing sensitive topics or if participants feel uneasy with when an audiotape is running, the use of field notes instead of audiotaping should be considered. In focus groups with children though, taking comprehensive notes might be very difficult as they move from one aspect to another in a very high speed (Kennedy et al., 2001).
Interviews can be completely transcribed, an abridged transcription can be produced (Burns & Grove, 2005; Krueger, 2006; Krueger & Casey, 2009) or the audio recording can be analyzed directly (Greenwood, Kendrick, Davies, & Gill, 2017). Complete transcripts depend on the length of the interview and can require several hours to create. Transcribing an interview takes about 4 times as long as the recorded interview and generates approximately 30–50 pages of text for a focus group interview of one and a half hours (D. L. Morgan, 1993). In an abridged transcript, only the relevant and useful portions of the discussion are transcribed, consisting of approximately 10–30 pages (Krueger & Casey, 2009; Sutton & Austin, 2015).
A note-based analysis primarily relies on the field notes taken by the moderators and assistants. A memory-based analysis relies on the moderators’ and assistants’ memories of the focus group. The last analysis method should only be performed by researchers experienced in this technique because it requires considerable skill and expertise (Krueger & Casey, 2009).
Discussion and Conclusion
Drawing on existing literature, important factors for planning, conducting, and analyzing focus groups with children, youths, and parents are presented. Focus groups are effective and suitable for collecting data on the perceptions, attitudes, and beliefs of children, youths, and parents. Focus groups can be administered with children and adolescents (Heary & Hennessy, 2002; Hoppe et al., 1995; Horner, 2000; Kennedy et al., 2001; M. Morgan et al., 2002; Peterson-Sweeney, 2005; Ronen et al., 2001) and with parents of hospitalized children (Teare & Smith, 2004). Focus groups with children can capture their perspectives, original ideas, and insights, which are often neglected in more traditional child research. Such interviews provide an innovative approach to understanding the children’s experiences from a developmental perspective. Commonalities and conflicts that arise in the family context can also be explored in focus groups. Focus groups with children and parents, individually or together, can be used to explore the shared experiences and conflicts that arise within families and can provide insight into how families manage these issues (R. S. Barbour, 1999).
Conducting focus groups with parents often don’t differ from conducting focus groups with other adults. If they are parents of sick children, the planning requires special attention like when conducting focus groups with vulnerable populations such as cancer patients, children, and adolescents. They might need support in finding someone to look after their children while they are away. This can be more challenging if the child is sick. The participants need information about locally available resources should they require help after the study. Similarly, a support system for participants may be needed if sensitive topics are discussed (Briller, Schim, Meert, & Thurston, 2007).
Successful focus groups with children require consideration of their developmental abilities and needs. Engaging the children’s interests and tailoring the interview to their level of comprehension are necessary prerequisites to maximize participation (C. D. Clark, 2011; Heary & Hennessy, 2002). Focus groups largely mitigate the data-gathering limitation caused by low literacy/reading levels, which can be problematic in quantitative methods using self-report questionnaires (Kennedy et al., 2001).
Focus groups provide researchers with large amount of data on a specific topic in a relatively short period of time. Researchers can observe interactive discussions in which common experiences and diverse opinions are shared. Group interactions can stimulate debate and encourage participants to explore and clarify their views (Clarke, 1999).
Even though we didn’t find literature making any specific statements to the way how the characteristics of the focus group members influence the interpretation of the data, we think this is an important issue. As in other qualitative methods, the contexts and constraints of the participant’s lives should be considered when analyzing qualitative data (Hunleth, 2011; Smithson, 2000). In reverse conclusion, we think the researcher should take in to consideration, for example in which development age the children or youths in the focus groups were, if the teenagers were girls or boys or if the parents were parents of healthy or sick children and youths.
The disadvantages of focus groups include the potential effects of social desirability, such as participant or peer conformity and unwillingness to disagree with another participant (Daley, 2013). In those cases, important but relatively extreme opinions are not captured and the data may be biased. There is some evidence proposing that some participants of focus groups have tried to please the moderator by giving the answers that they think the moderator wants to hear. The social pressure in adolescent focus groups can bias the results (Daley, 2013). As alternative approach to focus groups, Norris, Aroian, Warren, and Wirth (2012) developed adaptation of interactive performance for their research with sensitive topics and adolescents.
Logistically, focus groups can be difficult to assemble. Focus groups may discourage certain people from participating, including those who are not very articulate or confident or those with communication problems or special needs. Focus groups may also discourage some individuals from sharing sensitive or personal information because anonymity cannot be ensured (Gibbs, 1997; Parahoo, 2007). As in all qualitative analyses, deviant case analysis is important. In other words, attention must be paid to minority opinions or responses that do not fit within the researcher’s overall theory (Kitzinger, 1995).
However, several obstacles to the performance of focus groups still exist. It can be difficult to obtain a sufficient number of participants when planning focus groups with small populations. The challenges in including parents of sick children in focus group interviews are another topic requiring further research to better understand the needs of these parents and what incentives could be provided to them for their participation in a focus group. The search for literature of the last 10 years showed that there was only little current literature about how to conduct focus groups with children, youths, and parents. That means that more research about conducting focus groups with children, adolescents, and parents is needed. Future research is also needed to understand how children, adolescents, and parents experience their participation in a focus group, for example, what was important to them, what they enjoyed, and what they would change if they could (Hunleth, 2011).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Finnish National Post-Graduate School in Nursing Science, Academy of Finland, and a grant from the Nursing Science Foundation, Basel, Switzerland, to the first author.