
Abstract
Qualitative analysis is often a textual undertaking. However, it can be helpful to think about and represent study phenomena or narrative accounts in nontextual ways. In this article, we share our unique and artistic process in developing and employing pictorial narrative mapping as a qualitative analytic technique. We recast a nontextual, artistic–analytic technique by combining elements related to narrative mapping and narrative art. This technique involves aesthetic attunement to data and visual representation through pictorial design. We advanced this technique in the context of a narrative study about how arts-informed dissemination methods influence health-care practitioners’ delivery of care. We found that the Pictorial Narrative Mapping process prompted an aesthetic and imaginative experience in the analytic process of qualitative inquiry. As an analytic technique, Pictorial Narrative Mapping extends the inquiry process and enhances rigor through artistic means as well as iterative and critical dialogue. Additionally, pictorial narrative maps can provide a holistic account of the phenomenon under study and assist researchers to make meaning of nuances within complex narratives. As researchers consider employing Pictorial Narrative Mapping, we recommend that they draw upon this technique as a malleable script yielding to an organic process that emerges from both their own data and analytic discussions. We are further curious about its imaginative capacities in social and health science literature, its possibilities in other disciplinary contexts, and the prospects of what Maxine Greene refers to as becoming more wide awake—in our case, in future research analytic endeavors.
Keywords
Introduction
Qualitative analysis is usually a textual undertaking involving the identification and examination of key research ideas derived from study data. Using an iterative process (Butler-Kisber, 2010; Lapum et al., 2012), researchers typically employ a combination of inductive and deductive means to code data, synthesize and cluster codes into themes, and make interpretive links to the existing literature (Creswell, 2007; Streubert & Carpenter, 2011). While there are variations in analytic processes based on a study’s research purpose and the methodological approach, a final step of the analytic process involves decisions concerning data representation (Butler-Kisber, 2010). Researchers sometimes use visual techniques to represent data such as matrices, graphs, hierarchal tree diagrams, concept mapping, and cartographic mapping (Butler-Kisber, 2010; Creswell, 2007; Silverman, 2005). These visual mapping techniques can provide a conceptual understanding and a holistic overview of the study phenomenon as well as facilitate a different way to represent patterns in the data (Butler-Kisber, 2010). These visual maps can also provide another layer of analysis to facilitate researchers’ understanding of a particular phenomenon and assist in answering research questions more fully. However, like most qualitative analysis, these maps also tend to be textually dominated.
It can be helpful to think about research and represent findings in ways that are nontextual, such as images, to expand one’s way of knowing. It has been suggested that images can extend and richen our understanding of the social worlds of research participants (Meo, 2010). However, considering that researchers are the “instrument” in qualitative work (Richardson, 2000), an image, just like any other analytic description in research, is interpretive (Harper, 2000). Thus, interpretive discussions are vital not only to qualitative research (Denzin & Lincoln, 2000) but to how images are created, examined, and perceived.
The purpose of this article is to share our journey in refining and implementing a novel qualitative analytic technique that we have termed: Pictorial Narrative Mapping. This technique involves aesthetic attunement to data and visual representation of findings through systematically designed and constructed pictures. We employed this technique in the context of a narrative study exploring how an arts-informed dissemination method influences health-care practitioners’ delivery of care. We first provide an overview of narrative mapping and narrative art, both of which have influenced the development of the Pictorial Narrative Mapping process. Next, we provide a brief background to the study context in which this technique was further established. We then detail the components of the Pictorial Narrative Mapping process and share examples of the created maps as a way to examine the research findings and highlight a temporal and contextual understanding of the study phenomenon. Last, we provide an interpretive discussion about the methodological implications of Pictorial Narrative Mapping as a valuable qualitative analytic technique in research followed by the lessons that we have learned.
Background: Narrative Mapping and Narrative Art
The origins of narrative mapping cut across multiple disciplines. In the field of geography, maps have been used for centuries as a cartographic tool associated with global narratives (Caquard & Cartwright, 2014). Some cartography even includes pictorial maps with drawings as frequently seen in children’s atlases (Field, 2014). Within the anthropological and ethnographic fields, cartographic understandings of maps have been extended to consider sociocultural concerns from a spatial perspective (Roberts, 2012). Similarly, Pollner and Stein (1996) refer to narrative mapping within a sociological context in terms of how telling stories provides a psychosocial geographic mapping of personal experiences and how social worlds are produced through the sharing of these stories. Also, quite common in the field of education is the creation of narrative maps as visual displays of storylines (including plot, setting, events, and characters) that can facilitate students’ capacity to discuss reading material (Reutzel, 1985). In the digital media field, Mamber (2003) refers to narrative mapping as a way to visually and temporally represent the unfolding of events by incorporating text, images, and graphs.
Mapping has been increasingly employed in the research process to enhance the extraction, analysis, and representation of study data. In the health sciences, the visual mapping of stories has been used as a qualitative technique to aid data analysis (Beck, 2006) in which the temporal flow of study participants’ narratives is highlighted (Lapum, 2009; Lapum et al., 2010). In sports psychology and health disciplines, narrative maps of athletes during various life stages have been developed and explored as a way for other athletes to leverage their own personal experiences (Partington, Partington, Fishwick, & Allin, 2005; Phoenix & Sparkes, 2007; Sparkes, Perez-Samaniego, & Smith, 2012). Powell (2010) discusses how maps have evolved to be a methodological tool in representing data and identifying connections, benefiting fields such as psychology, sociology, and anthropology. Numerous scholars have discussed the value of maps in qualitative research (Wheeldon & Faubert, 2009) in terms of mind mapping to facilitate transcription and analysis of interviews (Tattersall, Powell, Stroud, & Pringle, 2011), illustrated story mapping to frame and enhance focus group discussions (Ureda et al., 2011), and concept mapping as a form of visual dialogue to deepen the analytic process and communicate findings (Butler-Kisber & Poldma, 2010; De George-Walker & Tyler, 2014). Many of these authors have noted how narrative mapping enables a holistic representation of a particular phenomenon or participant story (Lapum, 2009; Mamber, 2003). However, the narrative mapping techniques used by these authors are predominantly textual (e.g., Beck, 2006; Greenhalgh et al., 2005; Pollner & Stein, 1996; Reutzel, 1985).
Alongside narrative mapping is a more aesthetic approach to telling a story called narrative art. This approach involves the telling of a story through the media of art (Lucas Museum of Narrative Art, n.d.) which can involve the design and construction of a piece of work using techniques such as sculpture, drawing, painting, installation art, and other arts-based media (Atkins, 2013). The umbrella term of narrative art first appeared in the 1960s, although the concept existed before this time period (Atkins, 2013). In addition to telling a story, narrative art can foster imagination and curiosity as well as spark discussions. Others have spoken about the methodological significance of imagination as a tool that can expand and generate understandings of the social world (Hayes, Sameshima, & Watson, 2015). Although our review of the literature did not identify the use of narrative art as an analytic technique or method of dissemination in research, its possibilities are boundless in terms of how its aesthetic form could provide a more holistic and layered understanding of human and social phenomena.
In developing Pictorial Narrative Mapping as a qualitative analytic technique, we combined elements of narrative art with narrative mapping. This form of narrative mapping, as expanded upon later in this article, brings a more artistic element to the analysis and visualization of qualitative data resulting in pictorial representations. It is a technique that emerged not only from textually dominated mapping methods but also from the highly visual arts-informed research methods of photo elicitation, collage, and portraiture. These more artistic methods moved us to think about the contribution of visuals and pictures to the qualitative inquiry and analytic processes. Photo elicitation, with its roots in visual anthropology, adds photographs into the research interview enabling a deeper and more elaborate participant narrative (Padgett, Smith, Derejko, Henwood, & Tiderington, 2013). This method enriches typical methods of collecting and analyzing data, promoting a richer understanding of participants’ lives (Kolb & Lorenz, 2013; Mandleco & Clark, 2013). Collage making, which has become increasingly popular in arts-based research, has been shown to enhance researchers’ understanding and representation of participants’ stories (Gerstenblatt, 2013) as well as facilitate analytic processes (Butler-Kisber, 2008; Butler-Kisber & Poldma, 2010). Additionally, Butler-Kisber and Poldma (2010) found that collage as a form of qualitative inquiry is an accessible format that can enable a deeper and nuanced understanding of research phenomena. Portraiture is a research methodology that draws upon the metaphor of a portrait to encourage researchers to inquire and capture the richness and complexity of human experience (Lawrence-Lightfoot & Davis, 1997). Thus, the merging of narrative mapping with visual art affords the potential for enhancing and deepening the qualitative analytic process.
In the journey to developing Pictorial Narrative Mapping as a qualitative analytic technique, the first author and her colleagues shifted from textual to more of a pictorial narrative mapping process during a study exploring hospital discharge (Liu et al., 2012, 2013); however, the design process of the maps was not fully detailed in these publications, and they were created by research team members who did not have expertise in drawing skills. In the above noted study, each participant’s story was mapped using visual methods that combined narrative art and narrative mapping. Participants’ metaphors and descriptions became the design impetus for these maps. The process of visualizing these descriptions and creating pictorial maps allowed the research team to discuss the nuances of meaning embedded within the metaphor beyond what textual descriptions could depict. For example, one participant discussed how he felt like a caged bird while in hospital and that discharge was like being freed, yet his story was fraught with fear and feelings of vulnerability because he no longer had the careful monitoring provided by health-care providers. This description led us to draw an image of a bird exiting its cage and perched on a tree branch (see Figure 1).
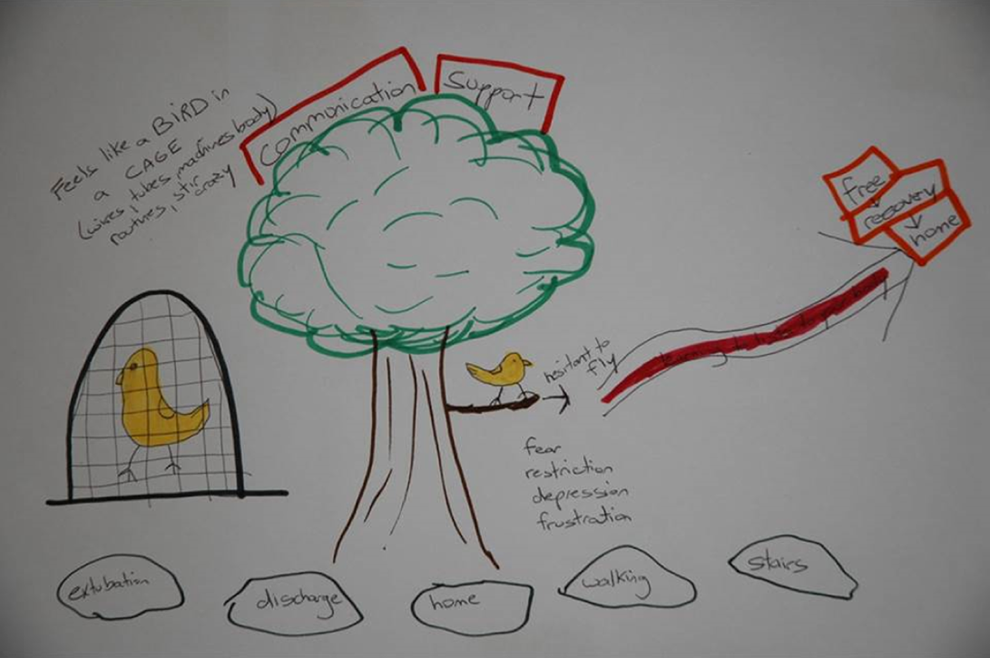
Caged bird.
While the bird was physically safe in the cage, its freedom was restricted. However, as the bird ventured out to the tip of the branch, it did not take flight. Conceptualizing this image allowed us to imagine not only the patient’s joy of recovery within the hospital as he gained freedom through the removal of machines and tubes but also the fearfulness of navigating his own recovery outside the hospital. Entering into the process of visualizing participants’ narratives permitted another layer of analysis. As we moved forth, we began to systematize the mapping process and incorporated it into the current study.
Study Background
We discuss Pictorial Narrative Mapping as a qualitative analytic technique in the context of the final phase of a multiphase study. The first phase was a narrative study about patients’ experiences of heart surgery in which findings were disseminated in the traditional format of prose through journal articles (Lapum et al., 2010, 2011). Following this, the first author translated patients’ stories into poetry and designed photographic images to metaphorically represent the embodied experience of surgery (Lapum et al., 2012; Lapum et al., 2013, 2015). The poetry and images were imprinted on hanging textiles within a 1,700 square foot and 9 ½ foot tall-art installation (Lapum et al., 2012). See Figure 2 for an overview of the art installation.

“The 7,024th Patient” art installation.
We then conducted a narrative study about individuals’ reactions to the installation, finding that arts-informed dissemination was a powerful approach that created an emotive and embodied space for individuals to imagine the experience of another (Lapum et al., 2014). As a result of the series of studies noted above, we conducted a third phase in which we focused on the knowledge translation capacity of arts-informed dissemination. We received ethics approval for this project from the first author’s institution and the hospital where the dissemination event occurred.
In this current study, we explored how arts-informed dissemination influences cardiovascular practitioners’ delivery of patient care. This study received ethics approval from the first author’s institution and the hospital where the art installation was displayed. Written informed consent was provided by all participants. Individual interviews were conducted with each participant at the time of viewing the installation and again 6 months later, so that we could explore the knowledge translation capacity of the arts. An interdisciplinary group of 19 practitioners was recruited including physicians, physiotherapists, pharmacists, ethicists, speech language pathologists, advanced practice nurses, and registered nurses; the latter was the largest disciplinary subgroup in our sample, a reflection of the workforce population. Study attrition included three individuals who did not complete the second interviews (for reasons unknown). During the analytic phase of this study, we employed Pictorial Narrative Mapping as part of Lieblich, Tuval-Mashiach, and Zilber’s (1998) narrative methodological approach that focuses on both the form and content of a story. In earlier phases of this study, we used textual-based narrative maps (Lapum, 2009), concept mapping, and diagrammatic and metaphorical sketches documenting key narrative ideas (Lapum et al., 2012). However, in this current study, it was our goal to design and construct a picture for each participant’s interview in order to better understand their experience and provide a holistic overview of their narrative.
Pictorial Narrative Mapping Process
An interdisciplinary team was composed for this project including artists, nurses, physicians, social scientists, and both graduate and undergraduate students. Two artists, who were skilled at using a selection of media to draw and paint, were part of the core analytic team. We met weekly for about 35 sessions to perform a narrative analysis followed by the Pictorial Narrative Mapping technique. For each participant’s interview, we collaboratively designed a pictorial narrative map. Based on our design, the majority of the maps were constructed individually by the two artists. However, a few of the maps were constructed collaboratively by the team and some were constructed individually by the team’s nonartists.
An iterative and dialogical process was followed in which we moved back and forth between the identification of the narrative plotline, the raw data, and the visual component of the narrative maps. We worked collaboratively and critically to ensure that the maps were grounded in the data. As such, reflexive questioning was an integral component of the process in which analytic decisions were fully examined and documented. A dialogical process allowed for all voices to be considered, and consensus was reached about the composition and aesthetics of the narrative maps before their construction. We documented the analytic discussions in field notes detailing emerging narrative ideas, plotlines, visual schemes, and analytic decisions.
A guiding principle was to draw upon the narrative plotline to form the foundation of the visual map; this principle was part of the structured process determined prior to the commencement of analysis. In terms of the plotline, both story content and form were considered (Lieblich, Tuval-Mashiach, & Zilber, 1998). After a participant’s plotline was identified, we engaged in discussions guided by the questions: How could this plotline be visualized? What would it look like? What should be in the picture and what should not be in the picture? Each of these questions was followed by the most important question, which was why assisting us to deliberate on the rationales behind our decisions. We followed an organic process in which the data directed our discussions and decisions. We also maintained an open process to permit literal and metaphorical visual representations. Additionally, we ensured our discussions were comprehensive and extensive in which we discussed many visualizations for each participant interview, so that we did not limit ourselves. Hence, we constantly reevaluated throughout the process and withheld final decisions until all discussions were complete, and everyone had an opportunity to speak.
We maintained aesthetic attunement throughout the discussion, but focused on the design composition after decisions were made concerning the overall picture to be displayed. At this point, we directed our analytic discussions to the picture’s tone, color, texture, and media. For example, what emotional tone did we want to convey in the image and why? What colors should we use and how does this relate to the emotional tone and the participant’s storyline? What arts media and textures will best convey the participant’s storyline? We did not limit ourselves to one particular media but used combinations of photography, acrylic paints, watercolors, pencil crayons, copic markers, gel pens as well as additional textures including cardboard, dirt, and hospital gloves. These discussions remained iterative and dialogical as we moved back and forth between the picture and the data, engaging in constant dialogue about our decisions and rationale. Aside from analytic field notes, the two artists on the team often kept their own mapping notes specific to composition details. At times, the two artists would create draft pictures during these analytic discussions, which acted to further our dialogue about the picture’s composition and aesthetics.
Pictorial Narrative Maps
In this section, we discuss a selection of the maps that were created to represent participants’ responses to the art installation (i.e., Map 1/Interview 1), and how this type of arts-informed dissemination method influenced their practice, that is, their patient care delivery in the cardiovascular context (Map 2/Interview 2). Although most maps are presented as sets, 3 of the 19 participants have only one map because they did not complete the second interview. Presented herein are photographs of the created maps. We specifically discuss methodological decisions concerning the design composition of these maps. Although we provide a textual explanation, the maps represent the study participants’ narratives at a particular moment in time and thus, a certain openness and dynamism need to be maintained because their stories continue outside of this research. Additionally, this openness provides space for readers to determine the relevance and applicability of these maps and the technique to their own contextualized spaces. Because textures are often difficult to fully apprehend with photographs, the design explanations also facilitate a better visualization of the maps.
Participant 6 (P06)
P06, who had worked for many years as an intensive care nurse, participated in Interview 1 only. We designed Map 1 (see Figure 3) based on his comparison of the installation to “Alice in Wonderland,” mimicking a larger than life feeling in which he was “in the patient’s world” and taking a “tour” of their journey through heart surgery. We used lightening with yellow glows and water along the path to capture how the art installation was “enlightening,” “striking,” and prompting him to reflect on his practice.

Alice in wonderland.
Although his narrative had an optimistic tone about how the installation would “change [his] practice,” he was unable to specify how at the time of Interview 1. For this reason, we purposefully sketched a path that ended at a door slightly ajar and emitting light to capture his anticipation of practice changes.
The creation and design of PO6’s map facilitated our understanding of the immersive nature of installation art as a dissemination method. Additionally, his narrative reflects the need for researchers to theorize about how to further facilitate the knowledge translation process so that viewers can more easily articulate the potential practice changes—instead of the door being slightly ajar at the end of the path, it would be wide open.
Participant 14 (P14)
P14’s Map 1 (see Figure 4) was designed to capture her narrative plotline focused on how the installation prompted reflection on the “mechanical” and “task-oriented” elements of her practice and how these acted in ways to overlook the “human part” of the patient’s experience. The clock represents both how the installation “struck” her and the way that “timeframes” structure her practice and engulf much of her efforts. We designed the picture so that the clock concealed part of a person’s face to symbolize the secondary nature of patients’ emotional needs in her practice. We purposefully designed the clock to have an antiquated feeling, not to suggest her practice was unimportant or obsolete, but rather to capture how routines of practice are firmly grounded in tradition.

Task-oriented practice.
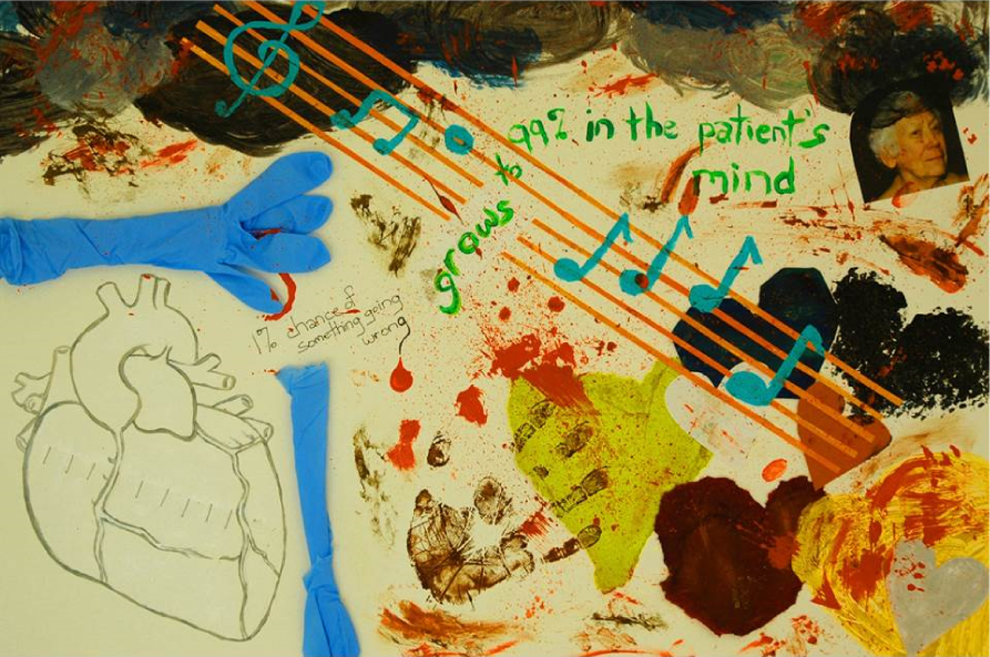
In P14’s Map 2 (see Figure 5), we used music as a metaphor to represent how the installation reinforced the importance of being “in tune” with patients and how it made her “more aware” of their emotions. Although a cognitive change is apparent in P14’s thinking, it appears that this did not necessarily translate into behavioral modification of her practice. We thus designed Figure 5, so that a musical staff is attached only to the nurse’s head representing the cognitive change she experienced and how she remains focused on psychomotor skills such as intravenous maintenance.

In tune with the patient.
We reflected upon how these maps drew our attention to the institutional structures that govern practice and, as a result, impact practitioners’ capacity to modify their practice. Specifically, the size of the clock and its design features in Figure 4 highlight the significance of technocratic efficiencies in health care.
Participant 1 (P01)
The idea of a museum became the guiding design feature of P01’s map for Interview 1 (see Figure 6) because she referred to walking through the installation as reminiscent of a “museum” in terms of the lighting and the feeling of silence that she experienced. She described the installation as “contemplative,” which prompted her to engage in reflection about the ease of getting “lost in the tasks” associated with cardiovascular practice. Her narrative pointed to ways in which the patient experiences reflected in the installation resonated for her and confirmed the importance of patient-centered care in her practice, highlighted by her direct gaze captured in Figure 6. Despite describing being engaged and inquisitive, her response to the installation was purely cognitive and neither emotional nor visceral responses manifest in her narrative. We thus made a decision in Map 1 to have her touching the painting, reflecting how the installation allowed her to get close to the patient’s experience but not necessarily become part of it.

The museum.
In contrast to Interview 1, in P01’s second interview, her descriptions of the installation focused on its “experiential” nature and how it allowed her to “experience individuals’ perceptions of that journey.” We thus designed Map 2 (see Figure 7), so that P01’s hand is clasped to the patient’s hand in which the patient is leading P01 through the journey during the 6-month period since the first interview, it appeared that P01 had further reflected on the installation and employed her lens as an advanced practice nurse to appraise the installation as a form of research and determine its applicability to her practice Additionally, what became most apparent in the second interview is the way that the installation acted as an educational tool about patient-centered care and empathy. We thus designed the background of the picture to resemble a chalkboard and used water to represent the way the installation drew her into the patient’s journey as well as the momentum of moving forward in terms of her reflective practice and patient-centered care approaches.
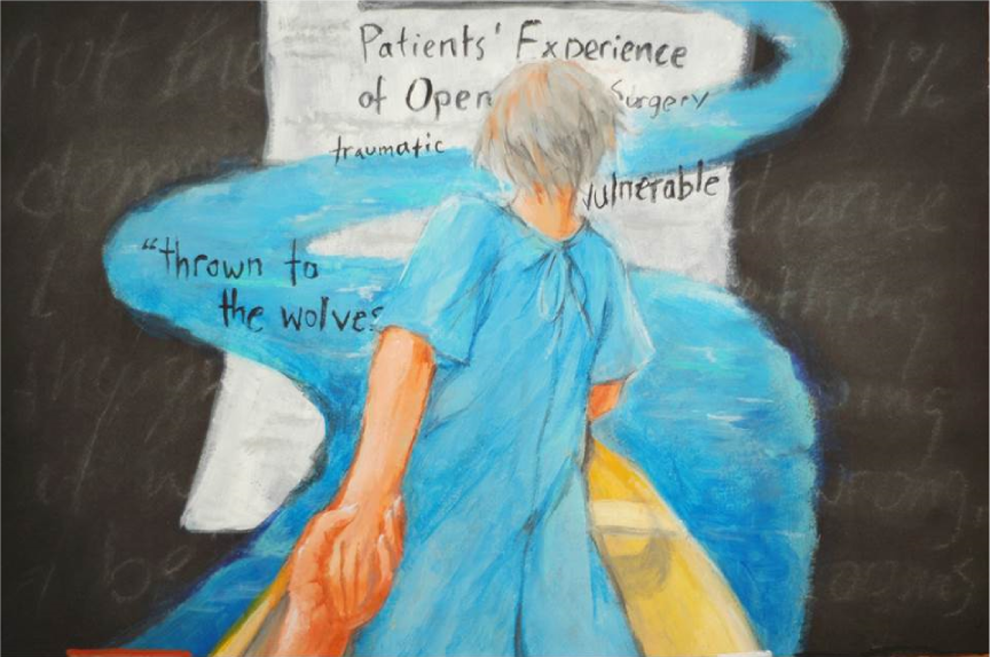
The journey.
We were struck by the contrast between the two images representing a shift from a static image positioned in a museum (Figure 6) to the motion characterized in Figure 7, reflecting a metaphorical classroom. This shift in images highlights the temporal and contextual processes associated with knowledge translation and specifically how participants’ uptake of research occurs over time in the context of their own practice.
Participant 2 (P02)
P02’s reference to how the lighting “made” her body “cast shadows” as she moved through the installation prompted us to metaphorically represent her as a dancer in Map 1 (see Figure 8). She purposefully came to the installation to “expose” herself to the patient’s experience (disseminated through the arts), which is reflected in the way that her body remains partly uncovered. We also used a spotlight in which she reaches out to the patient to capture what she described as a “cocooned feeling” wherein she became part of the patient’s world and more intimately understood their experiences, beginning to empathetically shift in her role as a nurse.
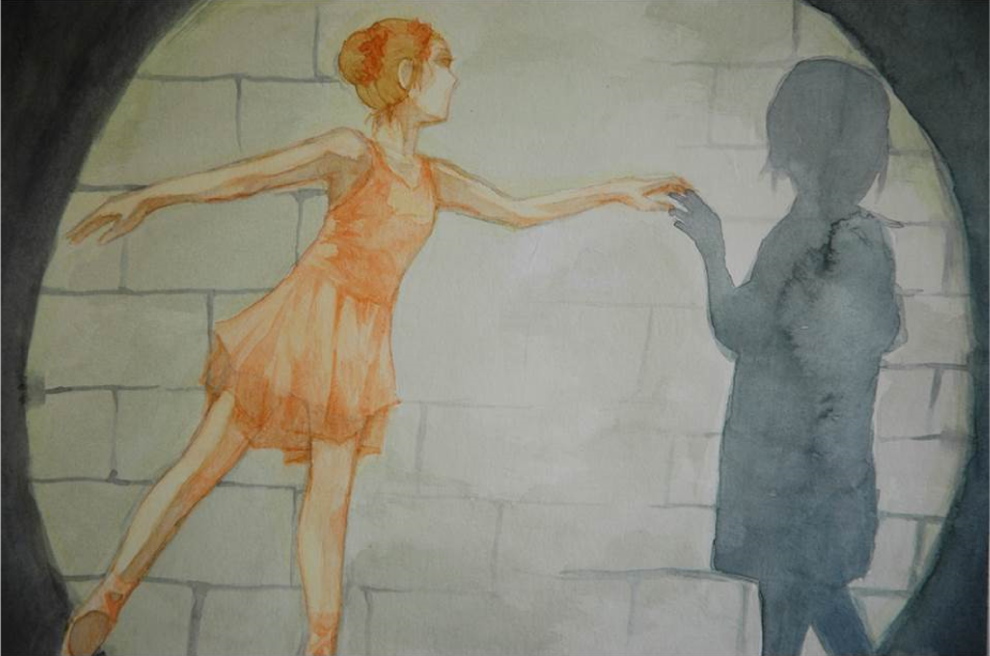
The dancer.

The empathetic shift.
In P02’s Map 2, we used an abstract design with vibrant, bleeding watercolors to represent her visceral and emotional responses and a shift toward a “different mental model” that is more patient centered and focused on understanding patients’ experiences from their perspective as opposed to the provider’s perspective. The spatial closeness between the participant (i.e., the practitioner) and the patient is enhanced in Map 2 compared to Map 1 to reflect how she continues to work at understanding the patient’s subjective experience.
For us, we found that these images highlight the way that installation art invites active participation from the viewer. Potentially, this beginning movement and momentum acts in ways to shift practice particularly when routinized practices associated with health care are often deeply engrained.
Participant 9 (P09)
The visual of an electromagnetic spectrum in P09’s Map 1 (see Figure 10) is representative of his narrative in terms of how the installation “make[s] absent what is present and make[s] present what is absent.” This led to a discussion on how disciplinary perspectives can be restrictive in what one “see[s].” He explicated that practitioners have a low “bandwidth” for empathy and that the installation may “pedagogically … expand our bandwidth around empathy.” For him, the installation made him reflect on “a narrative that [he] wouldn’t normally have encountered” because he is “trained in a certain way of looking” based on his disciplinary background as an ethicist. The images, outside of the visible spectrum (representative of the patient’s experience taken from the exhibit), are what he is working to see.

Bandwith for empathy.
We designed P09’s Map 2 (see Figure 11), so that he was physically placed in the picture because he spoke about a more active and personal reflection of his own practice. He mentioned that the installation was like a “doorway” that he entered, “open[ing his] thinking” and making him “think a little bit deeper” about patients’ experiences. We placed him in a large open meadow with several paths to capture the way that he was not only sensitized to hearing patients’ voices but also to demonstrate how he recognized that each patient encounter in his practice is “unique” and that they all have distinct needs.
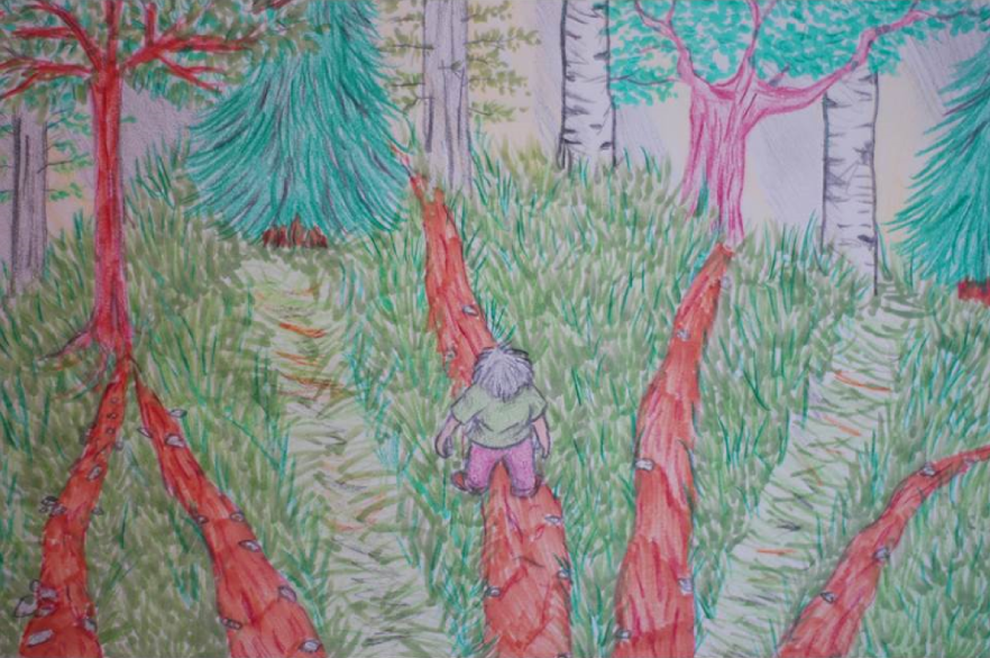
The meadow.
In reflecting on P09’s images, we began to consider the work involved on the practitioner’s part. It became apparent how practitioners needed to consciously examine their own disciplinary perspectives and practices and weigh these with the emerging evidence concerning patients’ perspectives.
Participant 12 (P12)
The design of P12’ Map 1 (see Figure 12) was guided both by the importance of reflection in her narrative and also the following statement: “I could see my own silhouette so it kind of puts you into their position like it almost makes you think like you’re the person that’s saying these words.” Thus, we used water to symbolically represent reflection and placed her in bare feet to capture the way that the installation stimulated a multitude of senses. Additionally, we designed the map with contrasting colors to represent the potential for transformation in her practice related to the “wake-up call” she experienced with darker tones representing patients’ experiences.

Reflection.
We designed map two (see Figure 13) to capture how the experience of walking through the installation prompted P12 to begin transforming her practice. She recognized that critical care settings can make people act like a “robot,” but the installation brought her back to “square one” of patient care viewing the patient as a person. To symbolize her practice changes, we designed the image in a way that the robotic armor is peeling off as she remembers the importance of holistic care and communicative interventions related to sensitivity and empathy. However, the robotic armor remains attached to cobwebs to metaphorically capture the routinized and engrained practices of critical care.

The robot.
Upon reflection, we noted the shift from the contemplative nature of Map 1 to more of a transformative and liberating feel of Map 2. These images highlight knowledge translation elements related to reflection on new evidence as well as the need for researchers to deliberately consider existing practices of care.
Participant 16 (P16)
We chose nature as a design element of P16’s first map (see Figure 14) to reflect her narrative plotline in terms of how she characterized her stance as someone who “has never wavered …despite … the external pressure” of the health-care system. Thus, in this pictorial design, we chose to metaphorically depict P16 as a strong and resilient tree in the foreground of the image advocating for patients. Additionally, we chose a tornado to symbolize the system because it is a powerful force that has its own schedule. P16 responded instantly to the installation by highlighting the system barriers that limit practitioners’ capacity to address patients’ concerns when “time” is a constant issue. As a physiotherapist, she said the installation confirmed that she was not just “a voice in the woods.” However, in the face of the tornado, she is surrounded by other practitioners who have become “down trodden” by the bureaucratic nature of a health-care system that can make one feel as if their “control has been taken away.” The trillium flowers under the strong tree represent the vulnerable patients P16 cares and advocates for.

Resilience.
A tree features in both maps representing the participant’s self-description as a source of strength and advocate for patients, although map two (see Figure 15) transitions to a softer image with the tree no longer in the foreground. We focused on designing Map 2 with a softer feel to the features (but still a tree that is symbolic of protection) because P16 indicated that the installation was “ethereal” and influenced her to be “more gentle” and let patients “lead the way.” The paths in the image demonstrate how she attempts to “merge the pathways” of the patient and the practitioner so that the important goals of recovery are achieved.

Protection.
Our reflections on Figures 14 and 15 led us to consider both the powerful nature of health-care systems in terms of governing practice but also the potential of individual practitioners to make practice modifications.
Participant 3 (P03)
P03’s narrative plotline focused on the tensions that he noted between the installation and his medical practice. He repeatedly referred to noticing how his patients have “shiny eyes” after surgery, representing a “return to life.” However, he was surprised at the depictions of so many negative emotional experiences associated with surgery and recovery within the installation. We used nature to metaphorically reflect life in P03’s Map 1 (see Figure 16) and placed a large, crisp, and bright image in the center to echo the importance of shiny eyes in his practice. Surrounding this center piece, we placed a diverse series of nature pictures to symbolize other layers of the patient’s experience that are entering his awareness. He stated that “you can feel the experience of the patient in the installation” and he clearly indicated the need to take the patient’s “point of view … into consideration.”

Shiny eyes.
In Interview 2, P03 described the installation as a “ray of light” that made him “aware … of what they [patients] are feeling.” In P03’s Map 2 (see Figure 17), we designed the image so light is emitting and P03’s hand is removing a mask symbolizing the strategies that he is using to discover the patient’s inner emotions. His comments reflect that he has to work at “getting below the level of anxiety” and the shiny eyes by building rapport, developing therapeutic relationships, and creative writing strategies to access patients’ feelings.

The mask.
Our reflections on Figures 16 and 17 prompted us to theorize about whether patients’ sharing of emotions is dependent on the practitioner’s discipline (i.e., medicine and nursing). Additionally, we began to consider how to further the knowledge translation process by having disciplines share their experiences and strategies to access patients’ inner emotions.
Participant 10 (P10)
P10’s narrative was fraught with dark emotions that were grounded in her nursing experiences. Initially, we had difficulty identifying her plotline because there were many layers to her story and her narrative was chaotic with “emotional tangents” about specific patients, family members, and the impacts on her. The design of Map 1 (see Figure 18) was guided by the paradox between the installation and her practice. She found the installation design “very sterile” and contrasted it to her practice as “completely unsterile. My practice has actual blood all over it. And Kleenexes and phlegm.” To reflect her narrative, we divided the picture into two sections: sterile and unsterile with the latter dominating. The unsterile side reflected her practice and descriptions of patient emotions that are “chaotic” and “dirty,” including fear and depression, creating “a big cloud” as people struggle to deal with them. She also described feeling “submerged … in the emotional dirt of the patient” and referred to use music to cope with this. We used layers of acrylic paint and other media, including cardboard cut-out hearts, hospital gloves, and actual dirt to vividly highlight both her storied content but also the chaotic narrative form.
The paradox.
We designed P10’s Map 2 (see Figure 19) to capture her narrative plotline related to the health-care system’s flaws, particularly its tendency to ignore patients’ experiences: “I’ve just reflected on that whole gap … the whole chasm.” Drawing from the installation, she felt “the human touch” needed to be reintegrated into health care in order to better address patients’ emotions and grief. We symbolically represented the system’s chasm as a large fissure in the earth’s surface and reflection through water. In considering symbols of human touch and emotions, we chose to place transparent hands positioned in a stylized heart shape over the fissure, demonstrating the capacity to bridge the chasm; we were able to achieve this design best through a combination of painting (the fissure) and photography (the hands). Although Map 2 is less chaotic than Map 1, we maintained an acrylic texture to portray the fissure.
We contemplated on the obvious shift from a complex to a more simplified and clean design from Figures 18 to 19. For us, we considered how this might reflect how knowledge translation requires reflection and time before individuals gain a sense of clarity about specific practice modifications.

The chasm.
Discussion
The artistic underpinnings of Pictorial Narrative Mapping provide a space to cultivate imagination in the interpretive and analytic process of qualitative inquiry. Greene (2001) defines imagination as the capacity to see and appreciate another person’s social world, their experiences, and perspective. As such, imagination is a vital component of the researcher’s toolbox considering that one of the aims of social and health science research is to understand another person’s experience while providing rich and contextualized descriptions of phenomena. As opposed to terminating analysis prematurely or limiting it to a textual process, we furthered and corroborated our interpretations through Pictorial Narrative Mapping. We found that the process of designing and creating pictures to represent participants’ narratives further stimulated our imagination and curiosity about their experience of attempting to garner knowledge from the installation and apply it to their own practice. Our work echoes that of Sandelowski (1993) who finds that artistic endeavors associated with imagination are important components of rigorous research; these artistic endeavors provide portals to new understandings. Imagination, facilitated through artistic endeavors like Pictorial Narrative Mapping, can maintain and enhance researchers’ critical and creative engagement with the data.
To borrow Green’s (1995) term, the design process and representation of data through Pictorial Narrative Mapping awakened us through an aesthetic experience that expanded our way of knowing. Foster and Lorimer (2007) indicate that the aesthetic is a type of knowing “concerned with sensory perceptions” (p. 54). Our Pictorial Narrative Mapping process echoes their work suggesting that visual expression can charter the senses (Foster & Lorimer, 2007). As Dewey (1934) indicates, our senses are embodied experiences of how we encounter the world. For us, mapping narratives through pictorial media facilitated a deeper understanding of the other person’s world and provided another layer to explore participants’ experiences as they attempted to garner and apply knowledge from the installation. Elsewhere, we have discussed how the aesthetic lens of the arts can facilitate emotional knowing (Lapum et al., 2012) and thus expand the way that one connects with research data. Our work is reflective of others who have spoken to the importance of multimodal intelligences (Albrecht, 2007) in terms of aesthetic and emotional knowing through imagery. The visual imagery provided through Pictorial Narrative Mapping can stretch one’s cognitive understanding by applying a process to engage in analysis using one’s senses.
As an analytic technique, Pictorial Narrative Mapping acts in ways to extend the inquiry process and enhance rigor through an artistic means as well as iterative and critical dialogue. Our interpretations and design decisions were a continual process in which we often changed our perspective based on this dialogue. As with any research, dialogue can enhance credibility by facilitating some level of agreement on interpretations (Eisner, 1991). Even more importantly, the aesthetic experience of art and the provocation of imagination require a critical dialogue (Moon et al., 2013). The art-mediated dialogue extends the inquiry process because it prompts one to move back and forth between the data and the mapping process as well as probe further into participants’ narratives. As such, the use of nontextual forms of analysis (e.g., Pictorial Narrative Mapping) to enhance the textual analysis can act in ways to avert rash interpretive decisions by researchers. Reflexive and critical questioning were salient elements of this dialogical approach, allowing us to explicate our positionality by questioning each other’s interpretations and justifying analytic and design decisions. Thus, the process not only pushed us to explicate our assumptions and values and how they shaped our interpretations (Creswell, 2007) but also ensured a reflexive development of the maps. Similar to Weber (2008) and Foster and Lorimer (2007), we found the use of visual images facilitated reflexive dialogue in which team members’ assumptions were challenged. Drawing upon Greene’s (1995) work, we concur that imagination, facilitated through the arts, allows researchers to traverse beyond their worldview and provides an opening into another person’s world. However, we also recognize that imagination is influenced by the researcher’s experiences (Hayes et al., 2015), making open and reflexive dialogue vital to the process. We found ourselves constantly deliberating about pictorial composition and choices of imagery, color, texture, media, point of view, and emotional tone. Much of the rigor comes from the dialogical and critical questioning that is part of the Pictorial Narrative Mapping process. The extensive field note documentation of our discussions and decisions served as an audit trail and ensured that our interpretations and the pictorial narrative maps were grounded in the participant data.
Our development and use of Pictorial Narrative Mapping echoes other scholars who have found that the arts can provide a holistic account of the data while also maintaining attunement to the particular (Greene, 2001; Weber, 2008). For us, we recognized what Greene meant when she speaks about the way that the arts can awaken us to see nuances in complex narrative accounts while maintaining the capacity to move back and forth between the particular and the whole. Similar to Weber (2008), we found that the use of visual images in the research process extended the textual analysis. However, we do not propose that Pictorial Narrative Mapping be used as a form of method triangulation. Rather, it is more comparable to Richardson’s (2000) idea of a crystallization in thinking about validation. Like a crystal, pictorial narrative maps are dynamic and interpretive as well as reflective of one’s stance. For us, the maps provided a visual medium which permitted our gaze to easily go back and forth between the images. We were able to see narrative patterns and temporal changes while comparing and contrasting Maps 1 and 2 and all of the participants’ maps as a whole. Additionally, the maps provide a snapshot of the data in which both the essence and the context of a story are recognizable. Similar to Mamber (2003), we found that maps are an effective way to consolidate large amounts of data and still capture the main narrative components. For us, a critical step was to focus on the narrative plotline in relation to the research question to guide the design and not attempt to put everything in the image. As Weber (2008) indicates, visual images provide a “complete glimpse” (p. 46) of a person’s experience. Although seemingly antithetical, a complete glimpse is necessary in research in order to facilitate understanding. As Tesch (1990) indicates, it is important to not flood the audience with a plethora of detail to the extent that they are “left with hardly a perception of the phenomenon at all” (p. 304). Thus, a map or visual image provides a tool to succinctly understand complex forms of data (Mamber, 2003; Powell, 2010), providing an overall picture of the phenomenon under study.
Although some artists find textual descriptions of art to be an interference (Strati, 2000), there is always the concern that images may be misinterpreted (Weber, 2008). Considering the importance of the raw processes and conditions, leading to the artistic product (Dewey, 1934), it was important for us to share our design strategy and a selection of the maps to demonstrate process as well as the links between our discussions and our decisions. Additionally, it was important to provide some level of detail in order to explicate the Pictorial Narrative Mapping process, since it is a new qualitative analytic technique in this particular form. Of course, we fully recognize the interpretive nature of qualitative research (Creswell, 2007) and embrace the idea that the symbolism associated with visual images may provide an opening for further interpretive dialogue and the formulation of new meanings (Lorenz, 2011). Thus, these maps may not be reproducible with a different team. Rather, a different team may bring another layer of discussion to pictorially representing narratives and further extend the inquiry process. In fact, Harper (2000) contends that the potential and power of images “lies in its ability to unlock the subjectivity of those who see the image differently from the researcher” (Harper, 2000, p. 729). Drawing upon Dewey’s (1934) work, art is an active experience that invites further inquiry. Most importantly, we look at the maps as a partial but unfinished pictorial overview of participants’ experiences. Experience continues (Dewey, 1934) for all of us including ourselves as the designers and creators of the maps but also for the research participants and the viewers/readers. And still, the pictorial narrative maps represent a real moment in time that can be sensed, looked at, listened to, touched, and felt.
Lessons Learned
In terms of employing Pictorial Narrative Mapping, we would call upon others to be vigilant in terms of not rigidly following our process. What is most important is to draw upon this technique like a malleable script yielding to an organic process that emerges both from your own data and analytic discussions. As Sandelowski (1993) warns, rigor is at risk of rigor mortis if we merely apply qualitative techniques and neglect “artfulness, versatility, and sensitivity to meaning and context” (p. 1). The aesthetic process associated with the arts acts as a methodological agent facilitating an emergent and responsive approach that is affected by iterative and dialogical discussions immersed in the data (Lapum et al., 2012). Although the mapping process was established to a certain extent prior to the commencement of our analysis, embedded in our procedural outline and application were principles of versatility and dialogue.
Invariably, a query that we grappled with was whether artists are essential participants in Pictorial Narrative Mapping. Our answer to this is tenuous and multifaceted. We believe that a more definite answer requires other research teams to engage in this process, and we also wonder if it may depend on the team and their capacity for artistic thinking. For us, we found that the interdisciplinary collaboration of artists and nonartists ensured that we remain multilingual, immersed in the visual art form as well as the research data (Eisner, 2008; Liu et al., 2013) More important than the pictorial narrative map as an outcome is what is behind the map, that is, the aesthetic and design process that advances the analytic thinking and inquiry process. Some nonartists have learned and thus possess artistic thinking even though they do not have the capacity to draw or produce a piece of artwork. Thus, they can deliberate about design elements such as image composition, perspective, color, tone, texture, and so on. However, artists often possess technical knowledge that nonartists do not, such as the different art mediums (water colors, copic markers, photoshop) that are available and how they can contribute to the visual arts. Not surprizingly, we found that the artist’s renderings of maps versus those completed by nonartists in our project were more aesthetically appealing; fortunately our maps were collaboratively designed and the majority was created by artist team members. Since the visual representation of data through maps can evoke a multisensory, embodied experience (Powell, 2010), we are curious about whether artist’s versus nonartist’s renderings will influence how audiences/readers engage with and are affected in the dissemination phase of this project. Will the enriched discussions that accompany visual expression (Foster & Lorimer, 2007) be limited with nonartist renderings? Nevertheless, engaging in the process of Pictorial Narrative Mapping is not always about the picture in the end but the designing and dialoguing about the creation of a visual image.
As others have found, there are ethical and methodological challenges to consider when using visual images (Hannes & Parylo, 2014). For example, a concern associated with the use of visual images in research is the risk of revealing a participant’s identity (Hannes & Parylo, 2014). We were able to mitigate this challenge in our project by having the research team and artists create the pictures as opposed to participants taking photographs. At this stage, Pictorial Narrative Mapping has been specifically developed as an analytic technique that extended researchers’ interpretive discussions. However, the use of these maps in the data collection phase of research is unexplored. It would be worthwhile to seek out participants’ perspective of the composed map and engage them in the interpretive discussions in a more coparticipant manner as done in the context of photovoice methods with Hannes and Parylo’s work. Extending Pictorial Narrative Mapping in this manner would be similar to the philosophical assumptions that underpin photovoice where participants are actively involved not only in the creation of the image but also in the analytic and interpretive processes (Fortin, Jackson, Maher, & Moravac, 2015). Additionally, these maps could be used as an elicitation device the way that Mughal (2014) as well as others use photographs to probe and prompt further dialogue with participants.
Conclusion
In this article, we have shared our experience in developing and implementing Pictorial Narrative Mapping as a qualitative analytic technique. Echoing the work of other researchers, we recognize and have rendered the way that maps are a medium for telling a story (Field, 2014; Powell, 2010; Sparkes et al., 2012). We have recast a nontextual and artistic form of analysis by combining elements related to narrative mapping and narrative art. Researchers and artists have been experimenting with how visual data can facilitate one’s understanding of the social world (Kolb & Lorenz, 2013). We agree with Greene (1995) that the aesthetic experience associated with art can reawaken us to look at things beyond our own lens. As we advance Pictorial Narrative Mapping as a qualitative analytic technique, we are further curious about its imaginative capacities in social and health science literature, its possibilities in other disciplinary contexts and the prospects of what Greene refers to as becoming more wide-awake—in our case, in future research analytic endeavors.
Footnotes
Acknowledgments
Thank-you to those participants who shared their stories.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We appreciate the grant funding provided by the Associated Medical Services; and the Faculty of Community Services, Ryerson University.