
Abstract
Background/Objectives
Visual demonstration by occupational therapists is very common in psychiatric treatment, however, some patients with schizophrenia could not imitate the actions despite the absence of any physical impairments. Therefore, the purpose of this study was to identify how cognitive functions such as attention and cognitive processes in the imitation process is necessary and how these processes were related to the ability to convert this into action (imitation) in patients with schizophrenia.
Method
The participants were patients with schizophrenia with mean age 59.2 (± 11.3) years, 23 were men and 10 were women. The participants were tested for imitation ability and cognitive function, working memory, and motor imagery.
Results
Three subjects achieved full scores in the visual imitation test. However, the median of the total score was 10.0, with many subjects failing to imitate multiple tasks. Imitation learning is associated with duration of illness(t = −4.09, p = .000), mental health(t = −2.30, p = .029), and cognitive function such as the ability to retain visual information(t = −2.97, p = .006), and that these factors are interrelated.
Conclusion
To effectively promote imitation learning in patients with schizophrenia, occupational therapists need to establish teaching methods that make it easier for learners to retain visual information from the early stages of their illness.
Introduction
Imitation, as defined in this study, is the copying of movements by matching one’s own movements with those of another person (Sevlever & Gillis, 2010). Imitation has a central role in human development and the learning of motor, communicative, and social skills. The young child’s ability to imitate the actions of others is an important mechanism for social learning; that is, for acquiring new knowledge. In the process of development, we learn cultural conventions of physical behavior, such as casual gestures and body movement, by imitating others. The acquisition of language, which is necessary for problem solving, also develops on the basis of imitation. Thus, we are able to construct a sophisticated social life through imitation, and imitation is thought to play a particularly important role in our interactions with others and groups.
In occupational therapy for psychiatric patients, particularly in training for social life skills, exercise, and handicrafts, we often use a method in which an occupational therapist performs a movement as an example and the patient imitates the movement in order to learn it. The purpose of imitation learning is to efficiently learn a desired behavior by imitating the occupational therapist. When some patients with schizophrenia attempt to imitate such movements, they can only do so poorly or not at all, despite the absence of any impairment of physical function.
Imitation in patients with schizophrenia has been studied. Matthews et al. (2013) showed that patients with schizophrenia were more likely to be unable to imitate finger, mouth, and facial expressions displayed on a screen than healthy control participants. Schwartz et al. (2006) conducted a study in which patients with schizophrenia were asked to imitate facial expressions displayed on a screen, and demonstrated that these patients were less accurate in imitating them than healthy controls. Walther et al. (2013) revealed that imitation deficits in schizophrenic patients were associated with catatonic symptoms. Park et al. (2008) analyzed the relationship between imitation ability and psychiatric symptoms, and showed that patients with impaired imitation ability had conspicuous negative symptoms. This suggests that negative symptoms, such as flat affect and social withdrawal, may have an impact on the willingness and motivation to imitate. In sum, previous studies, as described above, have shown that imitation ability in patients with schizophrenia is often impaired and associated with psychiatric symptoms.
Impairment of cognitive function, as well as psychiatric symptoms, is a fundamental feature of schizophrenia (Barch, 2005; Gold, 2004; Kahn & Keefe, 2013; Keefe et al., 2005; Sharma & Antonova, 2003). Cognition is necessary for humans to manage in their everyday (personal, social, and occupational) lives. Cognitive functions include the ability to work on things in a selective and focused way; to concentrate for a long time; to learn new information and skills; to make plans; to determine and implement strategies for action; to understand language and use language proficiently for communication and self-expression; and to retain information and manipulate it to solve complex problems. These abilities are impaired to some degree in patients with schizophrenia (Sharma & Antonova, 2003). Keefe and Harvey (2012) performed linear regression analysis to determine a predictive composite cognitive score, based on educational background and learning experience, as an indicator of premorbid intellectual function. A total of 98.1% of schizophrenic patients fell below expectations. The cognitive functions of working memory, executive function, and episodic memory in patients with schizophrenia have been the focus of several recent studies (e.g., Barch, 2005).
To imitate movements made by others, a person must observe the movements carefully, visualize them, and reproduce them in their own movements. It is thought that the brain’s ability to retain visual object as an image is involved in imagining movements. Therefore, learning by imitation may be, in addition to psychiatric symptoms, deeply related to one’s cognitive ability to observe another person’s movements in detail; to convert the other person’s movements into a visual image or concept and retain them; and finally to convert the retained representation into movement (Barch, 2005). However, it is not fully understood which area of cognitive function decline is related to the reduction seen in patients with schizophrenia. If this decline in imitation ability in schizophrenia is examined from the viewpoint of cognitive function, it should be possible to provide effective imitation learning while taking cognitive aspects into account. The hypothesis of the present study was that individuals with imitation disorder would have impaired cognitive functions such as working memory, control of motor imagery, and retention of visuospatial information.
This study was to investigate the performance of imitation skills and its relationship with other cognitive functions such as working memory, control of motor imagery, and retention of visuospatial information, in patients with schizophrenia.
Methods
Research Design
A cross-sectional and quantitative study design was used.
Participants
The participants were included among those diagnosed with schizophrenia based on the DSM-5 criteria (DSM-5; Diagnostic and Statistical Manual of mental disorders - Fifth edition.2013), who were patients of psychiatric hospitals and daycare centers in Aomori Prefecture, Japan. The selection criteria were persons: (1) with a diagnosis of mental illness, (2) 18–75 years of age, and (3) agreeing to participate in this study. Exclusion criteria were: (1) the medical condition was unstable, or the person was judged by the doctor or facility manager to be incapable of cooperating; (2) the person was unable to move their limbs as instructed, due to motor dysfunction; (3) persons aged under 18 or over 75; (4) persons who did not agree to participate in the study. After explaining the aims of the study to all the participants, and stating that they could refuse consent without suffering any disadvantage, we enrolled those who had given consent to participate in the study, for a total of 33 participants.
Assessments
Imitation ability
Imitation ability was assessed based on the items in the Standard Performance Test for Apraxia (SPTA; Japan Society for Higher Brain Dysfunction, Higher Brain Performance Test, 2003). The SPTA was developed with the aim of enabling differential diagnosis and analysis of higher motor function impairment. It can detect not only apraxia, but also motor paralysis, motor ataxia, and involuntary movements in patients with brain injury, as well as a variety of conduct disorders and impairment of skilled motor functions that cannot be fully explained by general psychiatric impairment. To examine the imitation ability in patients with schizophrenia, we used the following seven items: “Chin hand of Ruria,” “I, III, IV ring,” and “I, V ring,” from the high-level item of upper limb (one hand) finger imitation; “Figure eight,” “Butterfly,” and the “Paper/rock interaction test” from the high-level item of movement of the arms (both hands) without an object; “Ruria and stretch fist,” from the high-level item of continuous movement of the arm (one hand); plus one item, the “Reverse fox,” used as a screening test for dementia. Two points were given for perfect matching, one point for partial matching, and no points for mismatching. The total points (0–16) were counted, with higher scores indicating better imitation ability.
Cognitive function
Cognitive function was assessed using the Japanese version of the Brief Assessment of Cognition in Schizophrenia (BACS-J; Keefe et al., 2004), which can easily evaluate cognitive function in patients with schizophrenia. The six evaluated items were verbal memory, working memory, motor speed, attention and speed of information processing, verbal fluency, and executive function. Verbal memory testing can evaluate verbal memory; working memory can evaluate information processing of images; motor speed can evaluate visual attention and motor coordination; attention and speed of information processing can evaluate conversion and distribution of visual attention; verbal fluency can evaluate reasoning; and executive function can evaluate visual information processing, reasoning, and judgment. The severity of each assessment item can be determined using a Z-score.
Working memory
Lack of working memory is a form of neurocognitive impairment often observed in patients with schizophrenia (Aleman et al., 1999). The working memory section of the BACS-J test assesses the ability to retain verbal information; thus, we performed the Mental Rotation Test (MRT; Yamada & Uehara, 2008) to assess working memory, particularly the function of retaining visuospatial information. The MRT can test visuospatial cognitive function in patients with schizophrenia; patients rotate the visual information visualized in the brain as if rotating a real object. In the present study, the participants were asked to view photos, displayed one by one on an 11.6-inch screen, of a right or left hand or foot at different orientations and angles, and then answer ‘right’ or ‘left’ as fast as possible. The time taken to answer each task was measured, and the number of errors and time required for 10 tasks were totaled.
Motor imagery
We also performed the Controllability of Motor Imagery Test (CMI-T; Naito, 1994) to examine the participants’ ability to reproduce movements visualized in the working memory as real movements. Figure 1 shows three examples of instructions and their respective final limb positions. In the CMI-T, participants imagine movements equivalent to the instructions, such as “Raise your right arm forward to 90°,” or “Move your left foot forward 50 cm”. After all the instructions are heard, the participants attempt reproduce the posture imagined in their mind, using their own body. We used instructions recorded (in advance) at five-second intervals. The participants were asked to stand still with their eyes closed, and then adopt the final limb position after they had heard all the instructions. The level of difficulty was partially modified to suit patients with schizophrenia. A total of 15 tasks were assigned, with two, three, four, five, or six instructions, three tasks for each. One point was given for successful reproduction and no points for failure, after which the total points (0–15) were summed, with higher scores indicating better motor image function. Examples of instructions and correct final limb positions in the CMI-T.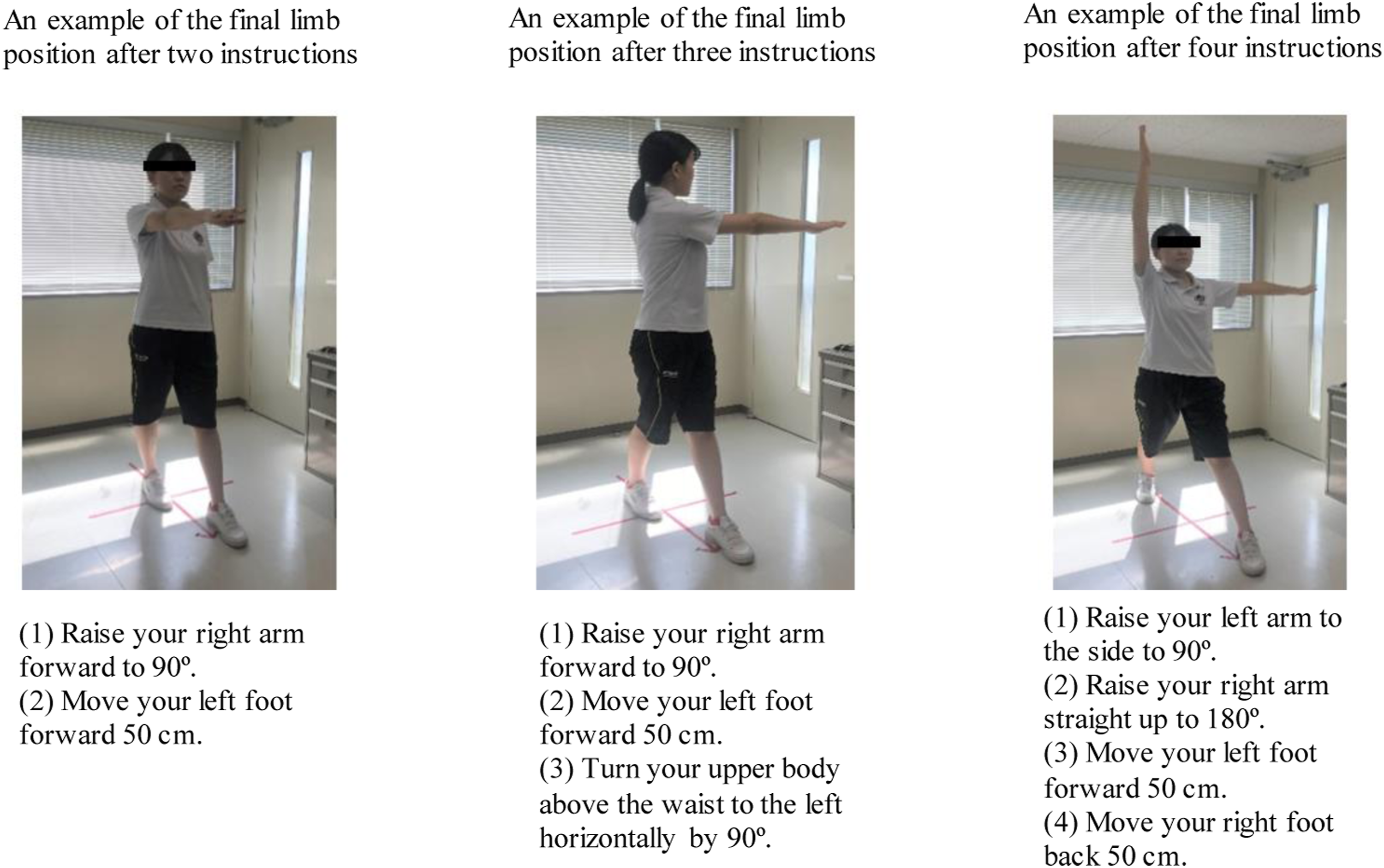
Procedures
The study was conducted from September 9 to 27, 2019. All participants were clinically stable and recruited from Fuse Hospital in Aomori, Japan. The purpose and procedure of the study was explained to the participants. Each assessment lasted approximately 20–30 minutes, and was undertaken either in the morning or the afternoon, to minimize the chance of fatigue and the effect of one assessment on another. All assessments were performed in a quiet dedicated space. The occupational therapist and participant sat face-to-face, in such a way that participants could not see the record form. When the participants found it difficult to decide upon an answer, they were encouraged to make their best guess.
Statical analysis
The correlation between the total score on the imitation test and each item, including the score on sub-items of the BACS-J, the total score on the CMI-T, and the number of errors and time required in the MRT, was analyzed using a Spearman’s rank correlation coefficient matrix. Stepwise multiple regression analysis was also performed, with the total score on the imitation test as the dependent variable and the items that had shown a significant correlation in the univariate analysis as the independent variables. Statistical processing was performed using EZR software. The level of significance was set at 5%.
Ethical Consideration
The study was conducted after obtaining approval from the ethical committee of Hirosaki University Graduate School of Health Sciences (Reference number 2019-03).
Results
Demographic Characteristics of Participants. n = 33.
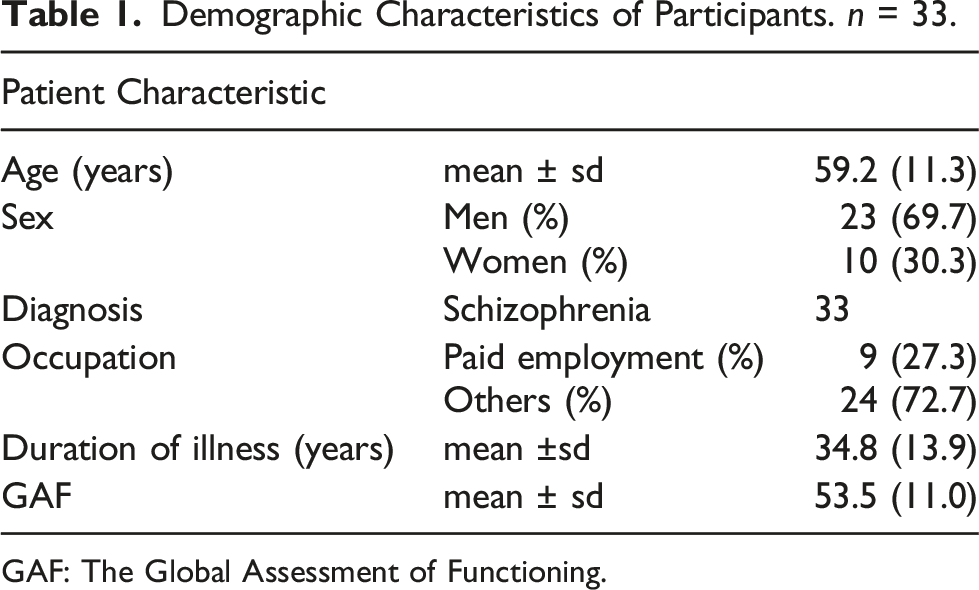
GAF: The Global Assessment of Functioning.
Results of Imitation Test and Each Evaluation Index.
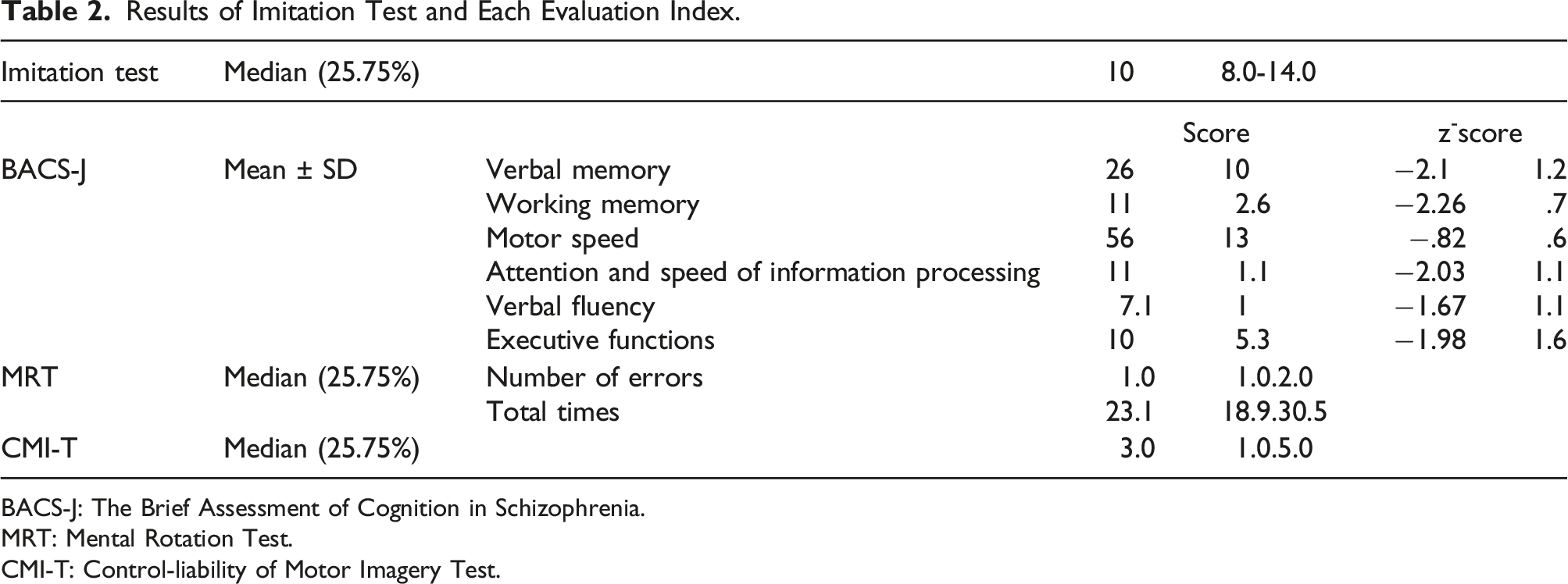
BACS-J: The Brief Assessment of Cognition in Schizophrenia.
MRT: Mental Rotation Test.
CMI-T: Control-liability of Motor Imagery Test.
Correlation between Imitations Skills, Other Cognitive Functions and Demographic Characteristics.
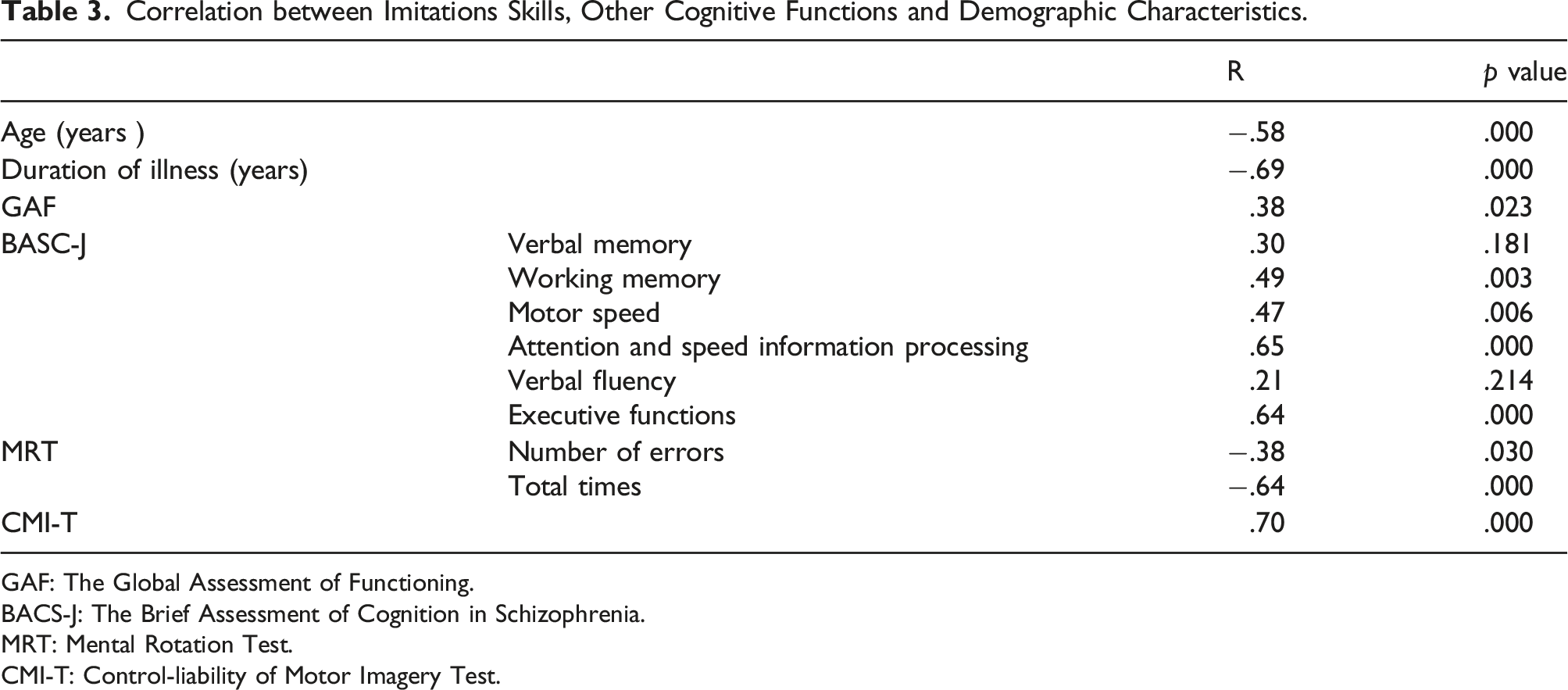
GAF: The Global Assessment of Functioning.
BACS-J: The Brief Assessment of Cognition in Schizophrenia.
MRT: Mental Rotation Test.
CMI-T: Control-liability of Motor Imagery Test.
Result of Analysis of Factors Related to Imitations Tests.
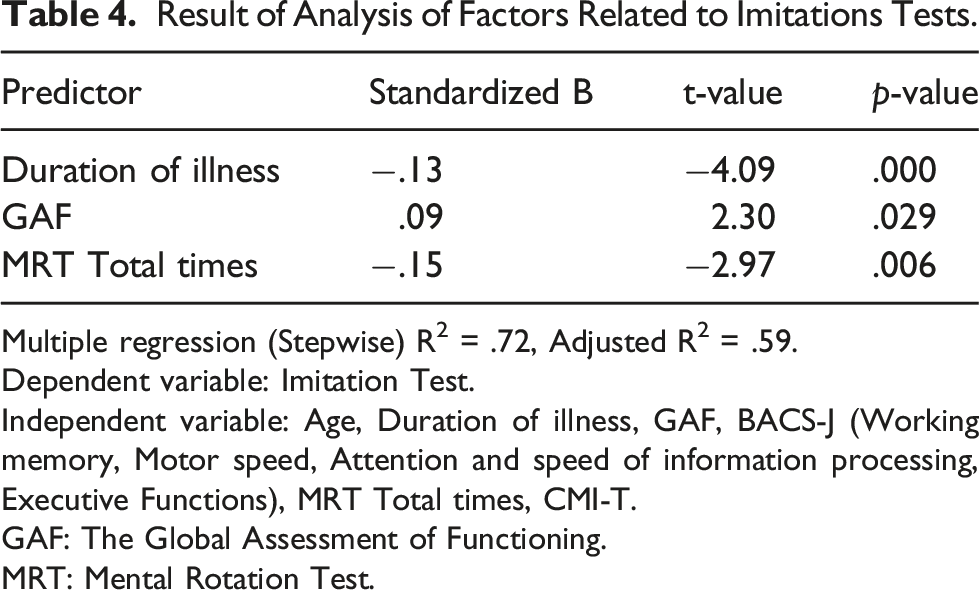
Multiple regression (Stepwise) R2 = .72, Adjusted R2 = .59.
Dependent variable: Imitation Test.
Independent variable: Age, Duration of illness, GAF, BACS-J (Working memory, Motor speed, Attention and speed of information processing, Executive Functions), MRT Total times, CMI-T.
GAF: The Global Assessment of Functioning.
MRT: Mental Rotation Test.
Discussion
Imitation is a series of motor learning movements which are adopted from a model and reproduced. (Piaget, 1981). In the process of imitation learning, the learner pays attention to the clues and characteristics of the teacher, retains them as representational forms, and reproduces them as physical movements. The normal functioning of these processes enables the person to form a mental image of how to perform the task, and successfully imitate it (Bandura, 1975). We conducted this study with the aim of revealing what kinds of cognitive functions are involved in this process of imitation. The results revealed that imitation is associated with similar cognitive functions.
Three participants achieved full scores in the visual imitation test. However, the median of the total score was 10.0, with many participants failing to imitate multiple tasks. The rates of correct answers were low, particularly for the Reverse Fox and Butterfly tests. To imitate these tasks, both hands needed to be used, with one hand placed on the other and reversing positions, and most of the patients appeared to have difficulty in imitating complex tasks using both hands.
The mean Z-score for each item in the BACS-J showed severe cognitive function impairment in verbal memory, working memory, attention and speed of information processing, verbal fluency, executive function, and total score; and mild cognitive function impairment in the case of motor speed. A study conducted by Keefe et al. (2006) involving patients with schizophrenia with a mean age of 35 showed mild impairment in working memory and executive function, and moderate impairment in verbal fluency. Terachi et al. (2017) examined patients with schizophrenia with a mean age of 65.7, and demonstrated that all the above items except motor speed and verbal fluency showed severe impairment. In a study conducted by Cholet et al. (2014), involving patients with schizophrenia with a mean age of 68.8, all the items except verbal fluency showed severe impairment. Cognitive function is moderately to severely impaired in patients with schizophrenia, and older patients have a greater likelihood of impairment (Keefe & Harvey, 2012). The participants in the present study were relatively old, with a mean age of 59.2, and, as in previous studies, overall cognitive function appeared to show comparatively severe impairment.
Correlation analysis between visual imitation and each evaluation index showed a mild to strong correlation between visual imitation and age; duration of illness; GAF score; working memory, motor speed, attention and speed of information processing, and executive function in the BACS-J; number of errors and total time required in the MRT; and the CMI-T score. Stepwise multiple regression analysis was performed with the total score on the visual imitation test as the dependent variable and these 10 items that showed a significant correlation in the univariate analysis as the independent variables. The results showed the duration of illness, GAF score, and total time required in the MRT to be predictor variables for the total score on the imitation test. Kucharska et al. (2005) revealed that emotion recognition and the ability to imitate facial expressions deteriorated with increased duration of schizophrenic illness. The volume of gray matter in patients with schizophrenia was also reported to decrease with increased duration of illness (Molina et al., 2004). The GAF scale is used to assess overall mental health, while taking psychology, society and occupational function into consideration. Deirdre et al. Robertson et al.(2013) revealed that GAF scores were associated with symptom severity and neuropsychological performance. Overall, the above studies suggest that extended illness and deterioration in mental health can affect the overall performance ability in patients with schizophrenia.
When taking the MRT, participants are required to recognize the status of an object (such as its position, shape, direction, size, and positional relationship) as a visual image through visual observation, and then retain and process the visual image while mentally inverting it (Yamada & Uehara, 2008). The results of the present study suggest that lower imitation ability in patients with schizophrenia is associated with impairment of cognitive function, particularly deterioration of the ability to retain visual information. Therefore, when teaching imitation, we should focus on impairment of the ability to retain visual information. For example, we should initially face in the same direction as the learner to make it easier for them to convert the visual image into a mental image. Subsequently, when the learner becomes able to fully retain a mental image of the teacher, face-to-face teaching can begin. Such step-by-step teaching is necessary until learners can achieve accurate imitation.
The above results suggest that imitation learning is associated with duration of illness, mental health, and cognitive function (such as the ability to retain visual information), and that these factors are interrelated. To effectively promote imitation learning in the context of schizophrenia, then, we must develop teaching methods that make it easier for learners to retain visual information from the early stages of their illness.
Several areas for future study are suggested. Given the relatively crude measure of cognitive functioning used in this study (BACS), further examination of the impact of Neuropsychological status on functional ability is needed. Longitudinal studies are needed to test the stability of the associations found in this study.
Conclusion
Finally, imitation is an important means by which we learn new social and nonsocial skills, impaired imitation ability may play a significant role in functional outcome of schizophrenia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.