
Abstract
Background
The most common cognitive dysfunctions in patients with schizophrenia are information processing, memory, and learning. Based on the hypothesis of rehabilitation and brain stimulation in memory and learning, adding a form of neuromodulation to conventional rehabilitation might increase the effectiveness of treatments.
Aims
To explore the effects of psychosocial occupational therapy combined with anodal Transcranial Direct Current Stimulation (tDCS) on cognitive performance in patients with Schizophrenia.
Methods
Twenty-four patients diagnosed with schizophrenia were randomized into the experimental and control groups. We used The Cambridge Neuropsychological Test Automated Battery (CANTAB) and the Loewenstein Occupational Therapy Cognitive Assessment battery (LOTCA) to assess spatial recognition, attention, visual memory, learning abilities, and high-level cognitive functions like problem-solving. All participants received customized psychosocial occupational therapy activities. Furthermore, the experimental group received 12 sessions of active anodal tDCS for 20 minutes with 2 mA intensity on the left dorsolateral prefrontal cortex (DLPFC) while the patients in the sham group received sham tDCS.
Results
Combining tDCS to conventional psychosocial occupational therapy resulted in a significant increase in spatial memory, visual learning, and attention.
Conclusions
Anodal tDCS on the left DLPFC improved visual memory, attention, and learning abilities. Contrary to our expectations, we could not find any changes in complex and more demanding cognitive functions.
Keywords
Introduction
Schizophrenia is one of the top 15 debilitating disorders (Vos et al., 2017) and patients with schizophrenia show significant deficits in different cognitive domains (Lesh & Niendam, 2011). Attention, reasoning, problem-solving, learning, verbal memory, visual memory, social cognition, and processing speed are among the commonly impaired cognitive functions in patients with Schizophrenia (Nuechterlein et al., 2004).
Cognitive impairment is one of the most critical effective factors in the occurrence of long-term social and professional performance problems (Carbon & Correll, 2014). Cognitive impairments are the first signs of the disease and can affect a person’s quality of life, functional skills, and activities of daily living (ADLs) (Green, 1996; Strassnig et al., 2014). Considering the importance of cognitive skills, one of the primary goals of therapists in psychosocial rehabilitation is improving cognitive functions.
The effectiveness of Occupational therapy (OT) interventions for cognitive impairments in patients with schizophrenia has not been studied sufficiently and studies in this regard have presented controversial conclusions. Hadas et al. compared the impacts of Instrumental Enrichment with OT interventions. Despite improvements in the OT group after a year, these authors could not find a significant difference between groups in terms of cognitive measures (Hadas-Lidor et al., 2001). Wykes et al. observed significant enhancements in cognitive skills after 3 months in both groups, of intensive OT, as the control group, and neurocognitive remediation, as the experimental group. The improvements were most significant in the cognitive flexibility tests and visual span (Wykes et al., 1999). Shimada et al. also studied the effectiveness of Individualized OT in patients with schizophrenia. Following 3 months, results showed significant enhancement in attention and working memory (Shimada et al., 2018).
Cognitive Rehabilitation Therapy (CRT) is a practical treatment approach for OTs (Abreu & Toglia, 1987). Investigations indicated that CRT could decrease frontal lobe dysfunctions and promote related cognitive functions in patients with schizophrenia. Psychiatric rehabilitation treatments, such as cognitive tasks, can lead to neurogenesis and the amelioration of various brain functions (Cheung et al., 2016).
This long treatment duration could lead to the frustration of clients, financial problems, and ending the therapy before attaining any changes. Understanding the causes of cognitive dysfunction in schizophrenia and targeting them could help therapists reduce treatment duration.
While the exact underlying mechanism of cognitive impairment in schizophrenia is still uncertain, the lack of efficient connections between cortical neural networks is considered as a model to prove functional disorders (Friston, 1998). There are two types of connectivity, one of which is structural plasticity that causes changes in the brain structure. The other type of connectivity is synaptic plasticity, which involves the alterations in synaptic activities. The latter is responsible for learning and memory (Friston, 2002). Furthermore, there are at least five major cognitive networks in the brain: (1) Language network in Wernicke’s and Broca’s areas, (2) Explicit memory network in the inferior parietal cortex, (3) Face-object recognition network in mid temporal and temporopolar cortices, (4) Spatial attention network in the posterior parietal cortex, and (5) executive function—working memory network in inferior parietal and prefrontal cortices (Mesulam, 1990). Researchers believe that abnormal neuroplasticity between brain areas play a vital role in the cognitive impairments occurring in schizophrenia (Stephan et al., 2006).
Transcranial Direct Current Stimulation (tDCS) is a form of neuromodulation that delivers low electric current to the head. This portable brain stimulation device applies a current of 0.5–2 mA. The tDCS works by applying a positive (anodal) or negative (cathodal) current via electrodes to the scalp (Nitsche & Paulus, 2000). The current generated by the tDCS is subthreshold and cannot trigger an action potential in a neuron; instead, it changes the activity patterns of active neurons by bringing them closer to their firing threshold (Bikson et al., 2004). The tDCS can make measurable changes in neuroplasticity (Braun et al., 2016); with a much easier usage in clinics than other non-invasive brain stimulation methods, including Transcranial Magnetic Stimulation (TMS). In addition, tDCS has received attention due to its lower costs. The use of tDCS is simple, and the consequent feeling that evokes in an individual is transient and gentle (Hesse et al., 2011). The stimulation of different skull areas by tDCS can change brain excitability (Hordacre et al., 2018). Brain excitability affects synaptic plasticity and changes the neuronal mechanisms underlying memory and learning, such as long-term potentiation (Nitsche & Paulus, 2000). These alterations can influence various behaviors.
Electrical stimulation of the brain can evoke tangible and measurable changes in the neuronal circuits and neuroplasticity in patients with schizophrenia (Hasan et al., 2013; Hoy et al., 2014). Brain stimulation by tDCS can produce positive changes in cognitive tasks (Hoy et al., 2015; Vercammen et al., 2011). Studies showed that the Dorsolateral Prefrontal Cortex (DLPFC) plays an essential role in memory performance and other cognitive tasks. Moreover, they demonstrated that both left and right DLPFC are involved in cognitive skills (D’Esposito et al., 1998; Mottaghy et al., 2000).
Considering the results of several previous studies, in this study, we selected the left DLPFC (F3 in the international EEG 10/20 system) to apply 2 mA anodal tDCS for 20 min because applying this tDCS protocol in patients with schizophrenia can improve memory and learning (Gomes et al., 2018; Hoy et al., 2014; Smith et al., 2015; Vercammen et al., 2011). The investigation by Gomes et al. (2018) had the highest number of sessions among previous studies (10 sessions). In the present study, the treatment protocol included 12 intervention sessions and 4 additional sessions for pre-/post-assessments.
The functional outcomes of OT depend on activity-dependent plasticity in the neural system. As a result, brain stimulation (by tDCS) facilitates this plasticity, and we hypothesized that psychosocial OT interventions with tDCS could make significant and faster changes than OT interventions alone.
In this study, we assessed whether anodal tDCS, as a complementary treatment, in combination with OT can make any changes in visual memory and other cognitive functions within 2 weeks of intervention. In other words, we evaluated the possible functional changes following tDCS combined with OT.
Methods
Trial Design
The present study was a randomized, double-blind clinical trial with a 1:1 allocation ratio and pretest-posttest design approved by the ethical committee of the University of Social Welfare and Rehabilitation Sciences (ethical code IR.USWR.REC.1396.404). It was registered in the Iranian Registry of Clinical Trials (IRCT) with the following code IRCT20180317039116N1.
Participants
According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), 35 patients diagnosed with schizophrenia by a psychiatrist in a psychiatric hospital were enrolled in the current study. All participants signed informed written consent forms. Considering the inclusion and exclusion criteria, seven patients declined to participate and four individuals did not meet the inclusion criteria. Finally, 24 patients participated in the research and were analyzed at post-test. The inclusion criteria were being diagnosed with schizophrenia, being 25–55 years old, have a history of at least 1 year of hospitalization, and have a mini-mental state examination (MMSE) score higher than 18 (Crum et al., 1993) to check the cognitive ability of the participants for following commands and participating in therapeutic sessions.
We needed the complete attention and cooperation of participants. Therefore, patients were excluded in case of persecutory delusions. Other exclusion criteria entailed changes in drug regimen over the past month or during the intervention have a history of electroconvulsive therapy and have skin problems, such as skin scratches on the F3 area that cause disturbances in the electrical stimulation of the affected area. In addition, participants who took medications affecting the function of tDCS (Attachment number 1) and patients with chronic neurological diseases, namely, epilepsy, Parkinson’s diseases, Alzheimer’s disease, radiculopathy, and musculoskeletal disorder in the upper limb were excluded.
Statistical analyst randomized participants into two groups with a 1:1 ratio using Random.org (Haahr, 2010). The leading researcher was blind to the randomization process. The experimental group (N = 12) received conventional OT and tDCS, while the individuals in the control group (N = 12) received conventional OT and sham tDCS (Fig. 1). Experimental design and study timeline.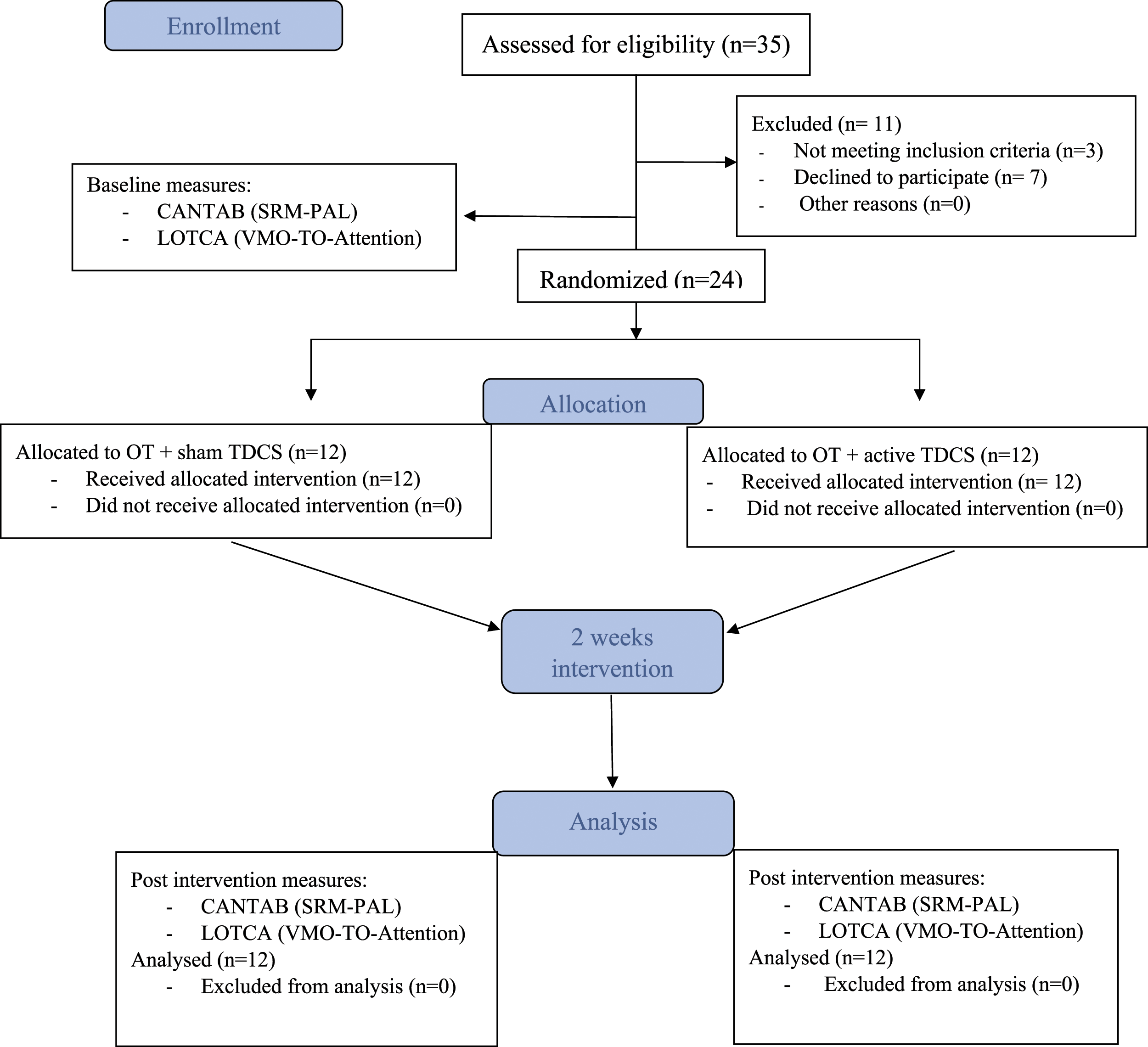
Anode (Active) and Cathode electrodes were positioned according to the 10/20 EEG system. We used a two-channel tDCS device in this research (Neurostim 2, Medina Teb, Iran). The center of the anode electrode was placed over F3, and the cathode electrode was placed on the right Supraorbital area. Brain stimulation was applied for 12 sessions of 20 min with an intensity of 2 mA. Both electrodes were 25 cm2, wrapped in cotton material, and soaked in saline (Vercammen et al., 2011). Sham tDCS had the exact electrode positioning and size, but the current stopped after 30 seconds to blind participants. Although they could feel the initial itching sensation, the stimulation could not induce any effects (Ambrus et al., 2012).
Assessment Tools
The outcome measurement tools were: MMSE, Cambridge Neuropsychological Test Automated Battery (CANTAB), and Loewenstein OT Cognitive Assessment battery (LOTCA) cognitive tests.
To evaluate the cognitive skills pre- and post-intervention, we used spatial recognition memory (SRM) and paired-associate learning (PAL) subtests of the CANTAB, as well as visuomotor organization (VMO), thinking operations (TO), and the Attention domains of the LOTCA battery.
The MMSE test provides an initial cognitive assessment. Scoring above 18 for male patients indicates men’s ability to follow commands and complete the tests (Folstein et al., 1975).
The CANTAB test is a battery of computer-based neuropsychological tests that were developed at Cambridge University. It assesses the components of cognition, especially those associated with the frontal and temporal regions. This collection consists of 22 neuropsychological tests in the cognitive field. The subject responds to the tests by touching the computer screen. All tests are non-verbal and culturally neutral. In this study, we used two sub-tests that include visual memory assessment (SRM and PAL). Besides, perceptual-motor evaluation (MOT) is an eligibility test to evaluate the participant’s ability to follow commands and do the tests (Cambridge Cognition, 2006).
The SRM test is for the evaluation of spatial recognition and visual memory. This test is sensitive to frontal lobe dysfunction. It has two phases; in the presentation phase, a white square is shown on the screen in different places. The individual must remember these places in the next phase. In the recognition phase, the square reappears in the same places as in the presentation phase, in reverse order. On each appearance, it is paired with a distractor square in a place that was not in the presentation phase. The participant should ignore the distractor and touch the square in the place that has appeared before. These steps are called a block. Each block is repeated three more times with five new locations. In this study, the number of correct responses was selected as the change criterion. The higher the number of participant’s answers in the test, the higher the scores. A higher score indicates better performance in the test (Cambridge Cognition, 2006).
In the PAL, boxes are displayed on the screen. These boxes are opened one at a time, in a randomized order. Some of them show a pattern. The patterns shown in boxes are then displayed in the middle of the screen, one at a time, and the participant must touch the box where the pattern was located. Each stage may have up to six trials in total. When the participant gets all the locations correct, they proceed to the next stage with more boxes. PAL assesses visual memory and learning. In this study, the mean trials to correct responses were selected as a change criterion. This criterion was obtained by dividing the total number of attempts into completed steps. Lower scores for this criterion show a person’s better performance in the test (Cambridge Cognition, 2006).
The LOTCA test has 20 items categorized into four subscales of Orientation (two items), perception (six items), VMO and TO. The VMO evaluates perceptual-motor integration with spatial components. This subscale includes seven items of copying geometric forms, pegboard construction, reproduction of two- and three-dimensional models, plain and colored block designs, reproduction of a puzzle, and drawing a clock. The TO subscale assesses sequencing and categorization and entails five items, namely, pictorial classification, pictorial sequencing, object classification (structured and unstructured), and geometrical sequencing (Rojo-Mota et al., 2017). The Persian version of LOTCA has suitable Construct validity in Iranian society (Karbalaei-Nouri et al., 2009).
Procedure
The outcome assessor and participants were blinded to group allocation. The researcher who applied tDCS and performed visual memory tasks was not blinded. Pre-test assessments were conducted on two consecutive days. Afterwards, the experimental group received actual electrical stimulation two sessions per day for six nonconsecutive days (a total of 12 sessions). There was a 3-hour interval between two consecutive sessions. All participants performed visual memory tasks during the first stimulation and received OT interventions after the second stimulation.
At the beginning of each session, all participants in both groups spent 20 min on three visual memory tasks while receiving brain stimulation (or sham stimulation). Each task was repeated five times. The first task was to remember the order of the cards and then find the cards whose places had changed. The second task was to memorize the cards and then recall the deleted cards. The third task was to remember the cards and then name them all entirely. Trials were sorted from simple to challenging.
Following the second stimulation, participants received regular psychosocial OT activities, including board games, card games, making Origami, and one session of group therapy to improve attention and memory. In group therapy sessions, the patients were randomly allocated into two groups of four patients. There were 50 cards on the table from different categories, such as fruits, foods, and animals that had to be memorized within 10 min. Next, both groups were given 5 min to recall as many cards as possible and write them down. The second activity in the group therapy sessions was pantomime.
The post-test assessments were carried out in two consecutive days right after the completion of the intervention.
Statistical Analysis
Regarding the Shapiro–Wilk test results, TO and SRM scores were normally distributed while VMO and PAL scores did not have a normal distribution.
The training effect on TO and SRM test performance was evaluated using a 2 × 2 mixed-design analysis of variance (ANOVA) with group and time as between- and within-subject factors, respectively. In addition, the Kruskal–Wallis test was performed for nonparametric variables, followed by the Mann–Whitney U test. All tests were two-tailed and p < 0.05 was considered significant. We also used the Wilcoxon Rank Sum test and paired t-test to examine changes in the final assessments of cognitive skills, compared to baseline.
Attention was an ordinal variable in this research. Therefore, Chi-square and Kappa tests were utilized for the analysis of this factor.
Results
Patient demographics and clinical data.
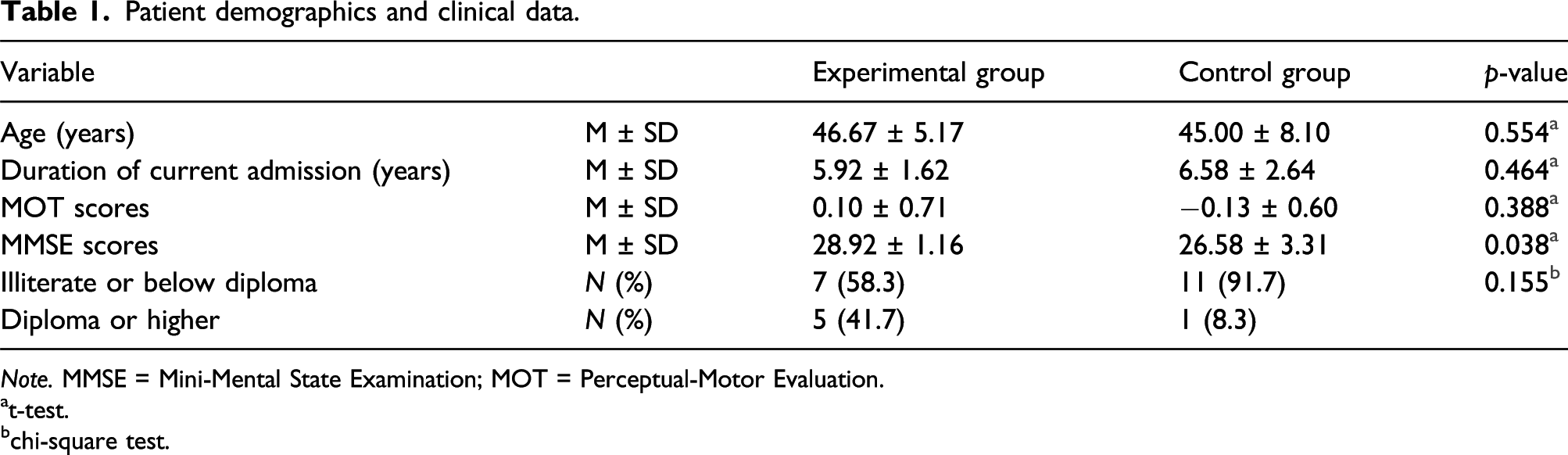
Note. MMSE = Mini-Mental State Examination; MOT = Perceptual-Motor Evaluation.
at-test.
bchi-square test.
Results of mixed-design ANOVA for SRM and TO.
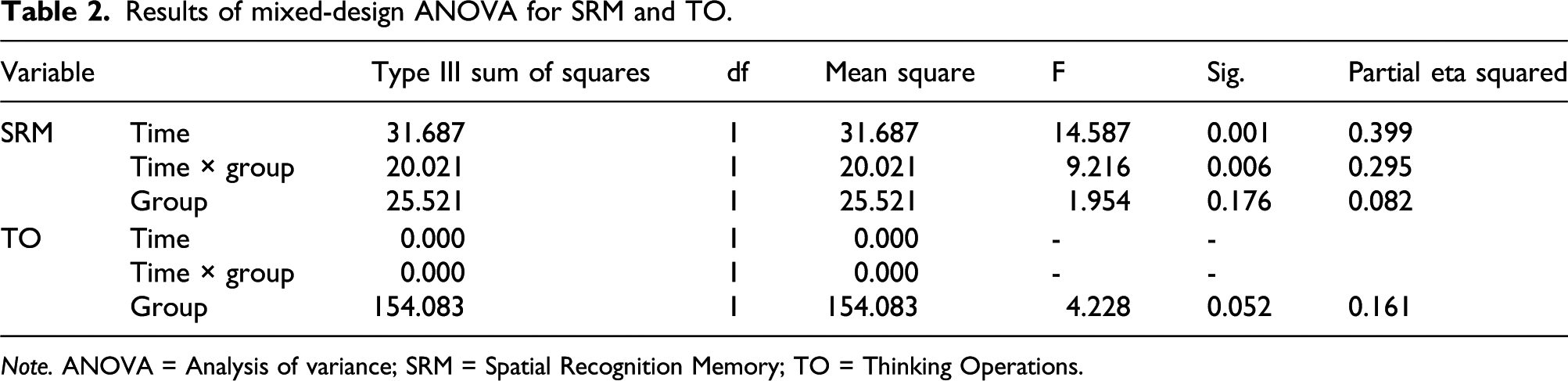
Note. ANOVA = Analysis of variance; SRM = Spatial Recognition Memory; TO = Thinking Operations.
Changes in cognitive measures between experimental and control groups.
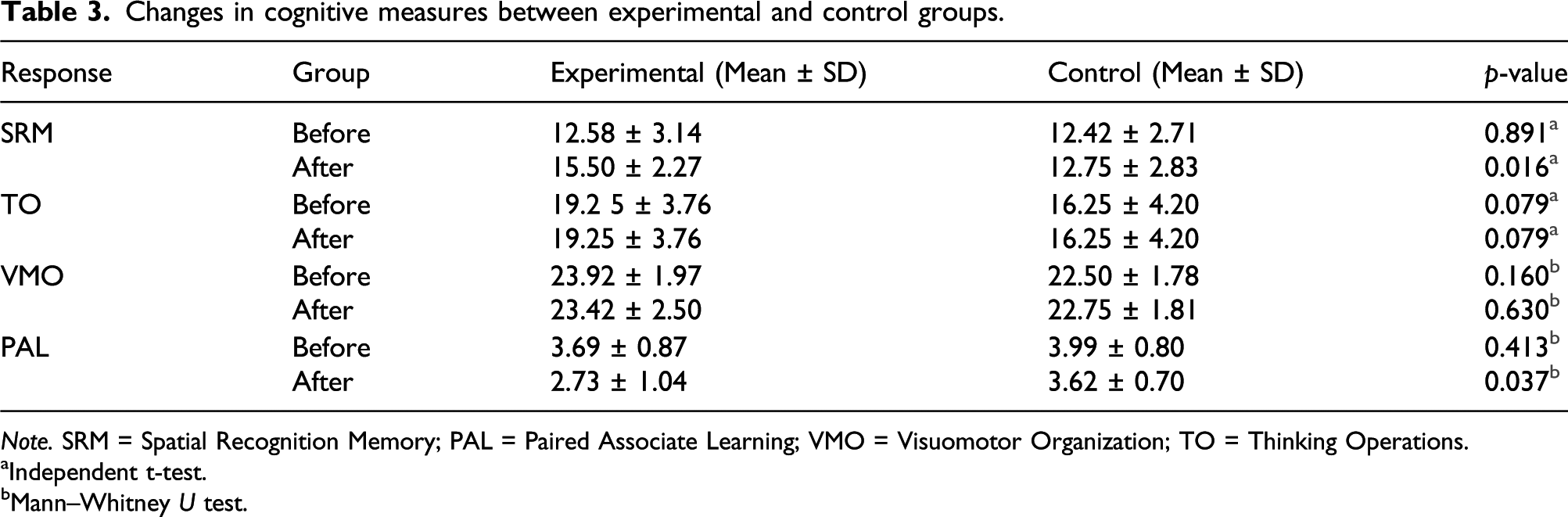
Note. SRM = Spatial Recognition Memory; PAL = Paired Associate Learning; VMO = Visuomotor Organization; TO = Thinking Operations.
aIndependent t-test.
bMann–Whitney U test.
The Kruskal–Wallis test showed a statistically significant difference in PAL score between groups (χ2(2) = 6.366, p = 0.012). The mean number of trials to reach the correct answer and the total mean score decreased in both groups, especially in the experimental group, which means all patients had better performance in PAL post-intervention. Further analysis revealed that the difference between the means of pre- and post-intervention in the experimental group was significant (3.21 ± 0.95, p = 0.011), whereas the control group showed no significant alterations (3.80 ± 0.75, p = 0.056). The baseline difference between the two groups was not significant (p = 0.413), while after the post-intervention difference was significant (p = 0.037) (Table 3).
Regarding the VMO scores, the mean scores of both groups diminished post-intervention. The Kruskal–Wallis test did not demonstrate a significant difference between the mean scores of the two groups. The difference between groups was not significant pre- and post-intervention (p = 0.160 and p = 0.630) (Table 3). Moreover, post-treatment changes in the intervention group were not significant (p = 0.285).
The TO mean scores did not change over time in either group and we did not find a time × group interaction effect in the ANOVA. Furthermore, no significant main effect was observed for the group variable (F (1, 22) = 4.228, p = 0.052, ηp2 = 0.161) (Table 2). The post-hoc analysis could not find a significant difference between nor within groups pre- and post-intervention (Table 3).
Attention distribution before and after intervention between groups.
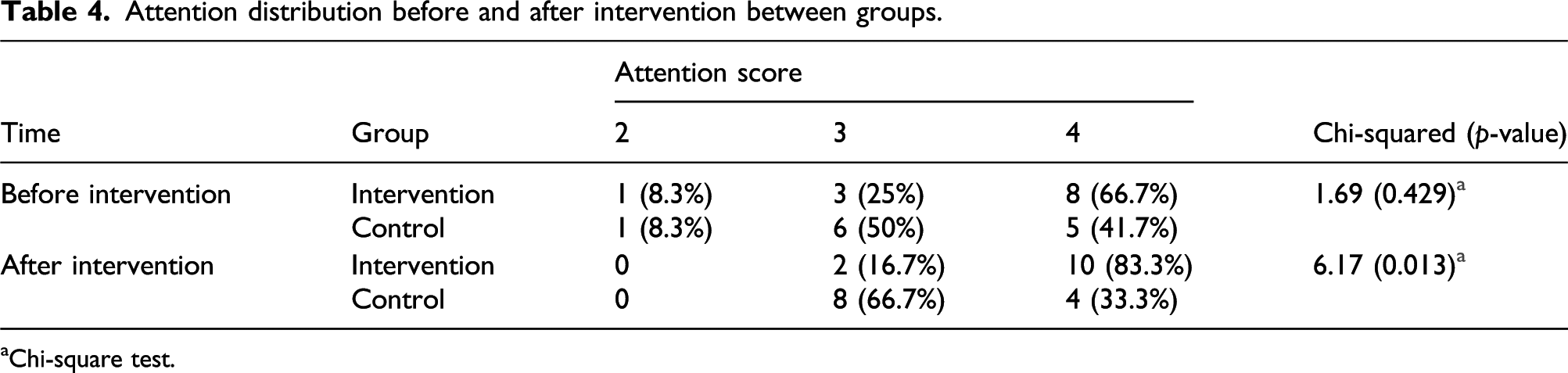
aChi-square test.
Discussion
This study examined the effectiveness of OT combined with anodal tDCS on cognitive skills in patients with schizophrenia.
These patients have abnormal neuroplasticity, which can induce cognitive impairments. In OT, patients learn cognitive skills through dynamic performances and activity leads to activity-dependent neuroplasticity. In addition, brain stimulation can facilitate this plasticity through diverse mechanisms, such as long-term depression or long-term potentiation. Therefore, combining brain stimulation with dynamic performances in OT can have more significant effects than OT/tDCS alone.
To the best of our knowledge, there has not been any optimal stimulation limits (e.g., intensity, the interval between sessions, the number of sessions, duration, and the electrode montage) for reducing the symptoms of schizophrenia. However, some earlier studies reported the positive impact of the non-invasive stimulation of the brain on cognitive functions. Hoy et al. reported that brain electrical stimulation could improve memory and learning abilities in patients with schizophrenia (Hoy et al., 2014).
The unique contribution of our study is the successful use of tDCS with conventional OT in a 2-week intervention. The present study is the first randomized controlled trial that showed tDCS can enhance psychosocial OT effectiveness and make significant changes in cognitive skills (i.e., SRM, PAL, and Attention) in patients with schizophrenia. To evaluate the generality of improvements, we used distinct assessment tools, namely, a precise CANTAB test and a more functional LOTCA test. All the selected components of CANTAB improved significantly. However, some LOTCA sub-tests, such as TO and VMO did not change after intervention. In other words, our study design reduced the required time to significantly enhance basic cognitive skills, while we probably need a more extended intervention period to find the improvements in functional and high-level cognitive abilities.
Patients with schizophrenia usually have impaired learning and visual memory (Nuechterlein et al., 2004). Therefore, in the current investigation, we utilized SRM and PAL tests to assess visual memory and visual learning. The results indicated that anodal tDCS could improve the function of visual memory, learning, and attention in these participants.
The changes in SRM and PAL scores were significant in the experimental group post-intervention. The results regarding memory and learning were similar to previous studies (Hoy et al., 2015; Ruf et al., 2017). Hoy et al. reported that applying anodal tDCS for three sessions of 20 min on left DLPFC with a current intensity of 2 mA may improve memory and learning. During stimulation, participants performed 130 working memory trials (N-back) which were also used as the outcome measure. Ruf et al. (2017) demonstrated that placing 1 mA anodal tDCS for three sessions on the right and left DLPFC of healthy patients can boost spatial memory and verbal memory, respectively. Moreover, these authors used verbal and spatial N-back tasks during sessions.
Another study (Vercammen et al., 2011) applied one anodal and one sham tDCS session in a cross-over design for 20 patients with schizophrenia. Anodal tDCS was applied on left DLPFC for 20 min at an intensity of 2 mA. During each condition, participants performed 150 associative learning trials from the weather prediction test, which was one of the outcome measures. The findings revealed improvements in associative learning in individuals who had better performance at baseline assessments. However, the induced changes were not statistically significant. In the present study, we found a significant difference in PAL scores in the test group. The mentioned difference might be attributed to the higher intensity of treatment in our study, compared to the previous one. Furthermore, we used distinct tasks and assessment tools to diminish the practice effect. Smith et al. used five sessions of anodal tDCS on LDLPFC in patients with schizoaffective and schizophrenia. Six out of 17 individuals in the intervention group and 8 of 16 individuals in the control group were diagnosed with schizoaffective. The findings of their study showed significant improvements in the working memory and attention/vigilance domains of The MATRICS Consensus Cognitive Battery (MCCB). However, no significant differences were observed in the visual memory domain (Smith et al., 2015). The inclusion of patients with schizoaffective and usage of distinct assessment tools might be the reason for different results compared with our findings. Jeon et al. (2018) applied 10 sessions of 2 mA anodal tDCS for 30 min on the left DLPFC area in 56 patients with schizophrenia (Cathode was placed on F4). Despite significant differences in the working memory subtest and the overall score of MCCB after the intervention, the visual learning score was not significant. In the present study, we used visual memory tasks during stimulation time and OT interventions that can improve brain plasticity (Ballesteros et al., 2018).
Chi et al. observed that one session of 2 mA anodal and cathodal tDCS on anterior temporal lobes in bilateral design for 13 min can significantly increase the visual memory of healthy people. Although visual memory improved in latter study (Chi et al., 2010), we cannot relate these findings to patients with schizophrenia because there are some identified abnormalities in the brain of patients with schizophrenia (Qiao et al., 2019), furthermore, the stimulation areas were different from the current investigation. Contrary to our results, Gomes et al. did not find a significant difference in Visual learning and working memory following 10 sessions of 2 mA tDCS on left DLPFC in patients with schizophrenia (Gomes et al., 2018). Another study found the detrimental effects of cathodal and anodal tDCS (on visual cortex) on visual processing tasks (Jahshan et al., 2020). Neither investigation used psychosocial rehabilitation and cognitive trials during stimulation.
In accordance with changes in attention scores, Smith et al. revealed significant enhancement in the attention/vigilance domain of MCCB (Smith et al., 2015). Gladwin et al. (2012) reported that anodal tDCS on left DLPFC could promote working memory and selective attention in healthy people. In latter research, 14 students received 10 min of 1 mA active anodal tDCS and sham tDCS in counter-balanced order. Results showed that active tDCS could reduce reaction time for tasks that require attention. On the contrary, another study (Coffman et al., 2012) showed that only alerting attention was improved after 30 min of 2 mA anodal tDCS. These researchers utilized the attention network task test to assess three forms of attention, namely, alerting, orienting, and executive in 20 healthy participants. The electrode was positioned on the F10 area in this research. The results of the present study indicated improvements in executive attention. This inconsistency might be due to different stimulation parameters, outcome measures, and populations.
Many studies found significant improvement in the overall score of the MCCB test (Gomes et al., 2018; Jeon et al., 2018; Smith et al., 2015). Contrary to our expectations, and despite more therapy sessions and a more intensive treatment protocol, we could not find any changes in the VMO and TO scores. This might result from the difference in assessment tools. We cannot compare the results precisely because diverse studies used variable methods, parameters, and assessment tools.
Cognition is a neural network, and the connections between neurons in these networks play a central role in cognitive functions. Therapeutic techniques, such as CRT, improve cognitive functions by facilitating these connections (Galetto & Sacco, 2017), while tDCS facilitates learning by modifying the neural mechanisms, including long-term depression and/or potentiation (Samani et al., 2019). The anodal current shifts the resting membrane potential of pre- and post-synaptic neurons toward depolarization, elevating neuronal excitability and allowing for more cell firing. The cathodal current shifts membrane potentials in the opposite direction and decreases cell firing and, subsequently, neuronal excitability (Arul-Anandam et al., 2009; Nitsche et al., 2008).
The results of our study showed that tDCS, as an adjunct to conventional psychosocial OT, can improve visual memory, learning abilities, and attention in patients with schizophrenia. Many variables can affect cognitive functions, such as genetic, baseline cognitive abilities, and situational conditions. However, considering the importance of cognitive functions in everyday activities and occupations, therapists should look for better and faster ways to improve cognition. Many daily occupations need complicated cognitive functions, and it seems that even significant alterations in visual memory and learning abilities are not enough for improving functionality. However, tDCS can provide a neural substrate to facilitate rehabilitative techniques. We recommend larger sizes and more intervention sessions for both genders.
This study had few limitations. We could not complete a follow-up because more than 90% of patients were transferred to the non-educational sections of the hospital. Due to convenience and cultural practice, this study recruited male participants exclusively.
Conclusions
The findings of this study demonstrated that combining a form of brain stimulation, such as tDCS with conventional OT can significantly improve basic cognitive skills in patients with schizophrenia compared to OT interventions alone. The present study’s result has important implications for developing effective treatments. Moreover, it provides further evidence to support tDCS as an adjunct treatment for the enhancement of cognitive functions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
1. Drugs that affect tDCS function
Amphetamine
D-cycloserine
Citalopram
Sulpiride
Pergolide
Rivastigmine
Dextromethorpan
Lorazepam
Flunarizine