
Abstract
Objective
Upper limb paralysis, which is a sequela of stroke, limits patients’ activities of daily living and lowers quality of life. The objective of this study was to examine the effects of peripheral nerve stimulation on hemiparetic upper limb functional recovery in chronic stroke patients undergoing low-frequency repetitive transcranial magnetic stimulation and occupational therapy.
Methods
The subjects were chronic stroke patients who participated in a two-week inpatient programme including repetitive transcranial magnetic stimulation and occupational therapy. There were two groups of patients: the peripheral nerve stimulation group (11 patients who underwent peripheral nerve stimulation) and the control group (11 patients who previously participated in the same inpatient programme but without peripheral nerve stimulation, selected via propensity score matching). The peripheral nerve stimulation group had 1 h of peripheral nerve stimulation on the median and ulnar nerves during occupational therapy. The outcome measures were the Wolf Motor Function Test, Fugl-Meyer Assessment, and Motor Activity Log.
Results
Wolf Motor Function Test, Fugl-Meyer Assessment, and Motor Activity Log showed significant improvement after the intervention in the peripheral nerve stimulation group. Particularly, the Fugl-Meyer Assessment hand score significantly improved in the peripheral nerve stimulation group compared to that in the control group (median change: 2 versus 0; p = 0.021, r = 0.49).
Conclusion
The combined use of peripheral nerve stimulation with occupational therapy after repetitive transcranial magnetic stimulation may result in a better functional recovery of in hemiparetic upper limb. Peripheral nerve stimulation with stimulation above the sensory threshold and below the motor threshold is easy to combine with occupational therapy upper limb function training and is therefore clinically useful.
Keywords
Introduction
Upper limb paralysis, which is a sequela of stroke, could limit patients’ activities of daily living (ADL) (Saito, Koyama, & Domen, 2018; Smania et al., 2009) and lower the quality of life (QOL) (Samsa & Matchar, 2004). Thus, occupational therapy (OT) is an essential intervention for promoting the functional recovery of hemiparetic upper limbs due to stroke. The recovery of severe upper limb paralysis plateaus in 80% of stroke patients by 6 weeks after onset and by 11 weeks in 95% of patients. In mild paralysis, recovery plateaus in 80% of patients by three weeks and by six weeks in 95% of patients (Nakayama, Jorgensen, Raaschou, & Olsen, 1994). Hence, improvement in upper limb paralysis ≥6 months after a stroke has conventionally been seen as difficult. Nevertheless, repetitive transcranial magnetic stimulation (rTMS) (Hsu, Cheng, Liao, Lee, & Lin, 2012) has recently been reported to promote recovery from post-stroke upper limb paralysis, even at the chronic stage. In chronic-stage stroke, excess contralesional motor area excitation suppresses the ipsilesional motor area through the corpus callosum, which in turn reduces interhemispheric inhibition and worsens motor functions on the paralysed side (Grefkes et al., 2008). rTMS is assumed to improve the interhemispheric inhibition. Low-frequency rTMS of approximately 1 Hz on the contralesional motor area could suppress excitation of this area and encourage activity in the ipsilesional motor area (Takeuchi & Izumi, 2012). Several studies have shown that OT training after low-frequency rTMS for two weeks improves upper limb paralysis in chronic stroke patients (Abo et al., 2014; Kakuda et al., 2016, 2012).
Electrical stimulation therapy, such as peripheral nerve stimulation (PNS), has also been shown to promote upper limb functional recovery in chronic stroke patients. To stimulate for long periods without fatigue or pain during PNS, low-intensity electrical stimulus at the sensory or motor threshold is used on peripheral nerves. Recovery of hand movement has been clinically reported in stroke patients after 2 h of PNS (Celnik, Hummel, Harris-Love, Wolk, & Cohen, 2007; Wu, Seo, & Cohen, 2006). Moreover, using PNS for 2 h before upper limb functional training was found to improve object manipulation skills (Carrico et al., 2016a; Carrico et al., 2016b; Conforto, Cohen, dos Santos, Scaff, & Marie, 2007; Conforto et al., 2010). Effects of upper limb function recovery were also observed when PNS was performed simultaneously with upper limb functional training (Ikuno et al., 2012).
Thus, the combined use of PNS and upper limb function recovery training has been shown to be effective in improving upper limb functional recovery in stroke patients. Furthermore, several studies have evaluated the effects of combining of a periphery-to-cortex stimulation technique, such as PNS, with a cortex-to-periphery stimulation technique, such as rTMS. For example, rTMS with PNS has been shown to prolong the duration of brain excitability in healthy persons (McKay, Ridding, Thompson, & Miles, 2002; Stefan, Kunesch, Benecke, Cohen, & Classen, 2002), and, similarly, transcranial direct current stimulation (tDCS) combined with PNS has been shown to prolong the duration of brain excitability in stroke patients (Uy & Ridding, 2003). In addition, tDCS and upper limb function training with PNS has been shown to improve hand functional recovery in stroke patients (Celnik et al., 2009; Sattler et al., 2015; van der Lee et al.; 2001). Therefore, the combination of both peripheral and cortical stimulation and upper limb function training may improve upper limb functional recovery; however, studies using rTMS are lacking.
As PNS is effective in stroke patients with upper limb paralysis and can be combined with upper limb functional training in OT, we hypothesised that performing PNS during OT after rTMS could increase the therapeutic effects. In addition, there have been no reports incorporating PNS with OT after rTMS; thus, verifying the effects of adding PNS could contribute to the development of OT methods for upper limb hemiparesis due to stroke, which could, in turn, improve the ADL and QOL of chronic stroke patients.
Therefore, the objective of this pilot study was to examine the effects of PNS on upper limb functions of the hemiparetic forearm in chronic stroke patients undergoing a two-week inpatient programme of rTMS and OT training.
Methods
Design
This was a controlled study comparing a control group, who underwent a two-week inpatient programme of rTMS and OT, with a PNS group, who underwent the same programme, with the addition of PNS. We conducted a retrospective survey of the medical records to obtain historical control data; the patients in the control group were selected via propensity score matching with patients’ consent. Finally, we compared the effects between the two groups. This study was registered in the University Hospital Medical Information Network Clinical Trial Registry (UMIN ID: 000030080).
Participants
Patients in the control group were chronic stroke patients with upper limb hemiparesis who underwent rTMS and OT from August 2013 to September 2017 (n = 104). Those in the PNS group were chronic stroke patients with upper limb hemiparesis who underwent rTMS and OT as well as PNS from October 2017 to November 2018 (n = 12). The inclusion criteria were as follows: (1) stroke patients with upper limb hemiparesis, (2) at least 20 years old when consent was obtained, (3) able to voluntarily extend at least three fingers including the thumb in the hemiparetic upper limb, (4) able to raise the hemiparetic upper limb to at least the chest level, and (5) more than six months since stroke onset. The exclusion criteria included the followings: (1) aphasia, agnosia, apraxia, or other severe higher brain dysfunctions that would hinder participation in the study; (2) loss of sensation; (3) inflammatory disease accompanied by rheumatoid arthritis or other forms of arthritis; (4) previously had a combination of rTMS and PNS; or (5) had previously participated in this study. Since this was a pilot study, the sample size was estimated using an empirical approach.
Data regarding the patients’ characteristics, including age, sex, stroke type (infarction, haemorrhage), number of years since stroke onset, hemiparetic side, dominant hand, botulinum treatment, and number of hospitalisations for rTMS, were obtained from the patients’ medical records.
Interventions
The baseline schedule of the two-week inpatient rTMS and OT training was the same in the control and PNS groups. The patients were first assessed and examined on the first week day by a physician. From Tuesday to Friday, they underwent 20 min of rTMS followed by 1 h of OT training in both the morning and afternoon. On Saturday and Sunday, they did not receive rTMS but had 1 h of OT training. From Monday to Friday of the succeeding week, they underwent 20 min of rTMS followed by 1 h of OT training in the morning and afternoon. On Saturday, they did not receive rTMS but had 1 h of OT training. On Sunday, they were discharged after an OT assessment. In addition, they received 1 h of walking training daily from Tuesday of week 1 to Saturday of week 2, conduct by a physical therapist.
rTMS settings
All patients underwent rTMS using the same settings. rTMS was applied using a 70 mm figure-8 coil and MagPro R30 stimulator (MagVenture Company, Farum, Denmark). In each session, 1200 rTMS pulses at 1 Hz were applied to the skull of the contralesional hemisphere, at the site that induced the maximum motor-evoked potential in the first dorsal interosseous (FDI) muscle of the upper limb and was not affected by surface electromyography. Stimulus intensity was defined as the lowest stimulus intensity that was set at 90% of the FDI muscle resting motor threshold and caused a response of at least 50 µV in the relaxed FDI muscle in at least 5 out of 10 consecutive trials (Kakuda et al., 2012).
PNS and OT methods
ESPURGE (Ito Physiotherapy & Rehabilitation, Co., Ltd, Japan) was used as the PNS device. For PNS, one electrode was attached to the palmar surface, approximately two-fifths distal between the palmar wrist and elbow joint of the forearm, covering the median and ulnar nerves, and another electrode was attached 1 cm proximal to the first. The device was set to provide continuous stimulation for 1 h, at a frequency of 10 Hz and pulse width of 1 ms, at a level above the sensory threshold but below the motor threshold, without causing discomfort. All patients in the PNS group underwent PNS with the same settings. PNS was performed for 1 h during the morning OT session on weekdays when rTMS was also performed, and for 1 h during the OT session on Saturdays and Sundays when rTMS was not performed. OT training included joint range of motion training and neuromuscular facilitation. The training exercises performed with PNS comprised manipulation training (using cans, beanbags, blocks, and other objects) and practicing everyday movements using the hemiparetic upper limb (e.g. manipulating chopsticks and shaving). OT training were delivered by four occupational therapists who used uniform intervention approaches.
Outcome measures
The following measures for the upper limb function were used: Wolf Motor Function Test (WMFT) (Wolf et al., 2001), including the task execution time; Fugl-Meyer Assessment (FMA; upper limb items) (Fugl-Meyer, Jaasko, Leyman, Olsson, & Steglind, 1975); and Motor Activity Log (MAL) (van der Lee, Beckerman, Knol, de Vet, & Bouter, 2004), including the amount of use (AOU) and quality of movement (QOM).
The WMFT is a test specific to post-stroke upper limb hemiparesis and is composed of 15 items: six single joint movements and nine object manipulations. The test is scored by measuring the execution time for each item (in seconds) and evaluating the quality of motor function using a 6-point functional ability scale (maximum score, 75). Because of the differences in the total time to complete the 15 items, the task execution time was expressed as a natural logarithm, which is similar to that in the EXCITE trial (Wolf et al., 2006). As an assessment tool for post-stroke upper limb motor skills, WMFT has also been widely used to evaluate the effects of therapies, including the combination of rTMS and OT training (Kakuda et al., 2016) and constraint-induced movement therapy (Wolf et al., 2006). Thus, we selected this test because it could be used to evaluate important motor skills that involve the hemiparetic upper limb. The WMFT scores was set as the primary outcome in this study.
The FMA is a stroke-specific test based on the stages of post-stroke motor paralysis recovery described by Brunnstrom (1966). Thirty-three items related to upper limb movements are scored on a 3-point scale (maximum score, 66; minimum score, 0). The sub-scales are as follows: A) shoulder–elbow–forearm (0–36 points); B) wrist (0–15); C) hand (0–21), and D) coordination/speed (0–9).
The MAL is a 14-item test that assesses how much and how well the patient uses the hemiparetic upper limb in daily life. The maximum score is 5; the minimum score is 0. The MAL is widely used as an objective assessment for the quality and quantity of upper limb use.
The same outcome measures were used for both the control and PNS groups. For the control group, results before and after the intervention were obtained from the medical records. The PNS group was evaluated before and after the intervention.
Statistical analysis
The characteristics of the patients in the control group were matched to those of the patients in the PNS group using propensity scores. The characteristics used to calculate the propensity scores were based on previous studies (Fritz et al., 2006; Fritz, Light, Patterson, Behrman, & Davis, 2005; Takebayashi et al., 2013) and the investigators’ clinical experience. These characteristics comprised pre-intervention WMFT, FMA, MAL-AOU, MAL-QOM, age, sex, time since stroke onset, stroke type, hemiparetic side, botulinum treatment, and number of hospitalisations for rTMS.
The basic pre-intervention attributes of the PNS and control groups were compared using the Mann–Whitney U test or Fisher’s exact test. The PNS and control groups’ WMFT, FMA, MAL-AOU, and MAL-QOM were compared before and after the intervention using the Exact Wilcoxon signed-rank test. Execution time in the WMFT and changes in the FMA, MAL-AOU, and MAL-QOM between the groups were compared using the Exact Mann–Whitney U test; the effect size (r) was calculated from the Z-statistic. We performed non-parametric tests because of the small sample size and ordinal data.
A p value <0.05 was considered statistically significant. All statistical analyses were performed using EZR Ver.1.37 (Saitama, Japan) (Kanda, 2013).
This study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 2013) and ethical guidelines for medical and health research involving human subjects (Ministry of Health, Labor, and Welfare, Japan, 2015). This study was approved by the institutional ethics committee (approval number 3877) and the appropriate ethics review board (approval number 30013001). The institution’s website homepage posted information about the study and provided the patients an opportunity to withdraw from participation. The study procedures were explained to the patients in the PNS group and or their family members at hospital admission. All patients in the PNS group in this study provided written informed consent.
Results
Figure 1 shows a flow diagram of the study. Of the 12 patients in the PNS group, one patient dropped out because of a family health issue, thus, only 11 patients in the PNS group completed the therapy and were analysed in this study. Of the 104 patients in the control group, 11 patients were selected using propensity score matching.
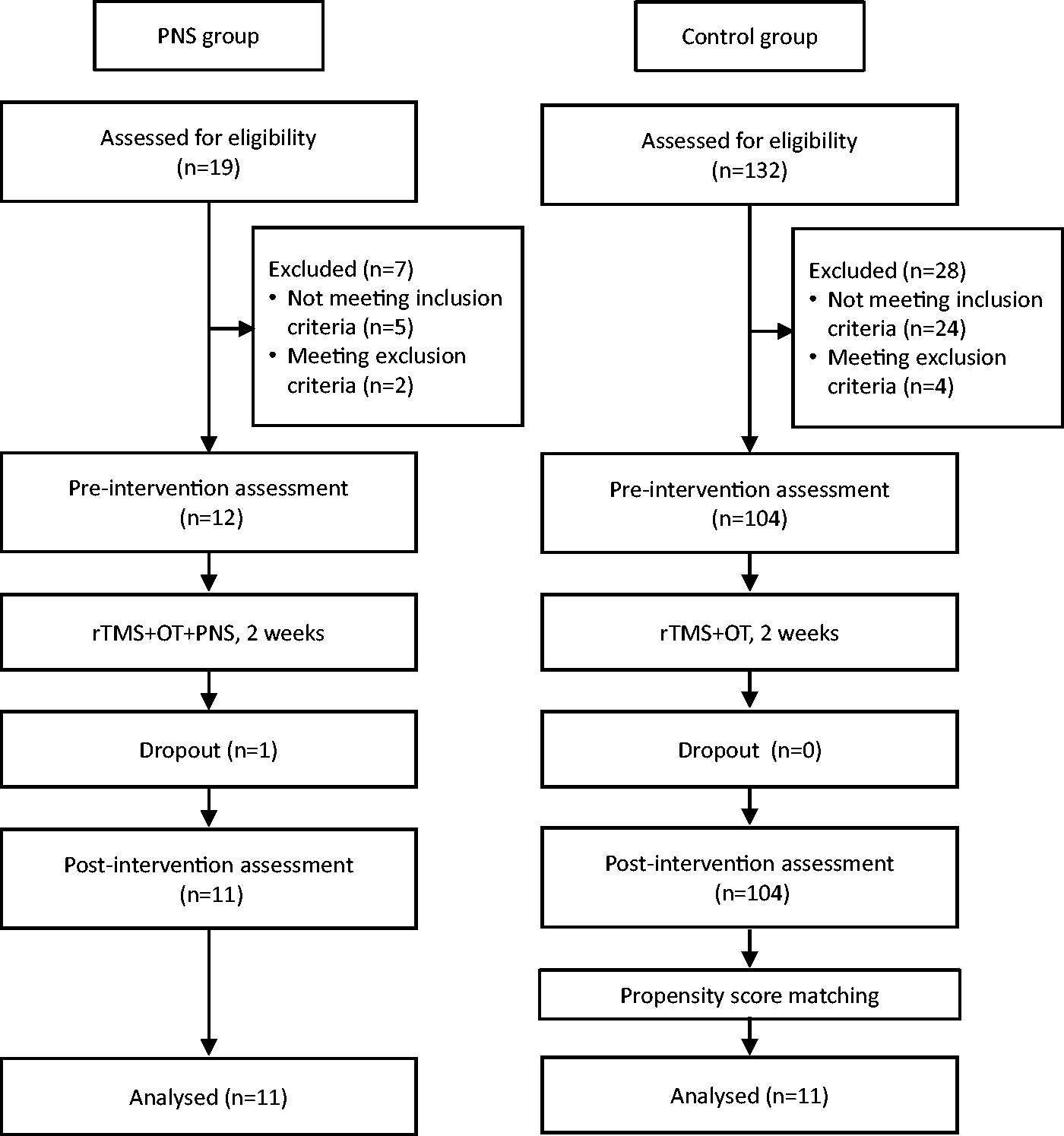
Flow diagram of the study.
Table 1 shows the results of the comparisons in patient characteristics and pre-intervention assessments between the PNS and control groups. None of the items differed significantly between the groups.
Comparisons in the characteristics and pre-intervention assessments between the PNS and control groups.

IQR: interquartile range; OT: occupational therapy; PNS: peripheral nerve stimulation; rTMS: repetitive transcranial magnetic stimulation.
aExact Mann–Whitney U test.
bFisher’s exact test.
In the comparisons between pre-intervention and post-intervention upper limb function in the PNS group, significant differences and large effect sizes were observed for the WMFT (p = 0.014, r = 0.51), FMA (p = 0.005, r = 0.61), MAL-AOU (p = 0.009, r = 0.57), and MAL-QOM (p = 0.014, r = 0.54). In the comparisons between pre- and post-intervention upper limb function in the control group, a significant difference and large effect size were observed only for the FMA (p=−0.009, r = 0.57). In the comparisons between the PNS and control groups in terms of the change in upper limb assessments (pre-intervention to post-intervention), a significant difference and large effect size were observed for the FMA hand score (p = 0.021, r = 0.49) (Table 2).
Comparisons in upper extremity function between pre- and post-intervention, within and between the PNS and control groups.
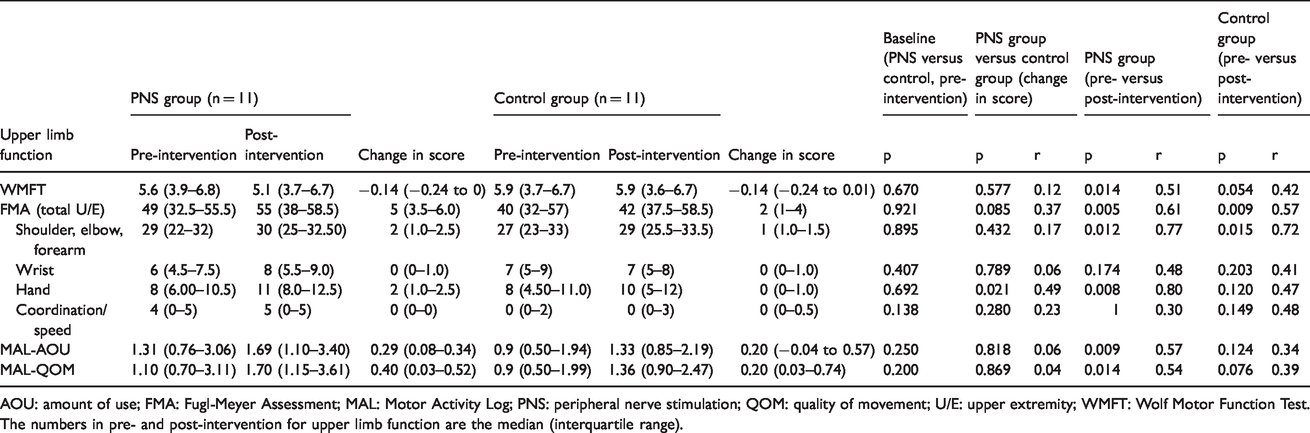
AOU: amount of use; FMA: Fugl-Meyer Assessment; MAL: Motor Activity Log; PNS: peripheral nerve stimulation; QOM: quality of movement; U/E: upper extremity; WMFT: Wolf Motor Function Test.
The numbers in pre- and post-intervention for upper limb function are the median (interquartile range).
Discussion
We incorporated 1 h of PNS with OT training in a two-week inpatient programme that included rTMS and OT training for chronic stroke patients to verify the effects of PNS on the functional recovery of the paralysed upper limb. Upper limb functions were evaluated using the WMFT, FMA, and MAL. The PNS group showed significant improvements in all upper limb functional evaluations (WMFT, FMA, and MAL) after the intervention. Particularly, the change in the FMA hand score was significantly higher in the PNS group than in the control group.
In this study, the WMFT score was set as the primary outcome to evaluate the effect of adding PNS to rTMS with OT training on upper limb functional improvement. The WMFT scoring assesses the time it takes to manipulate objects and the quality of these movements. As adding the PNS resulted in greater recovery in hand function, we assumed that the restoration of basic hand movements would be reflected in object manipulation item using the WFMT; thus, we expected the WMFT score to improve more in the PNS group than in the control group. However, adding the PNS did not have a significant effect on the WMFT score, as no differences between the groups were noted. As object manipulation not only involves hand functions, but is also related to the functional level of the proximal part of the arm (such as the shoulder, elbow, and forearm), improvement in hand function alone may not be sufficient to reflect an improvement in object manipulation. Another study that used the WMFT as an outcome for the effects of adding PNS to a programme (Carrico et al., 2016a, 2016b) provided 2 h of PNS and 4 h of upper limb functional training per day, which is twice the amount in this study.
On the other hand, incorporating PNS into OT training showed an effect on the FMA hand score, which was a secondary outcome in this study. PNS involves stimulating sensory nerves at the sensory threshold level to encourage motor area activation and stimulating a peripheral nerve to activate the corresponding primary sensory area. This is hypothesized to affect the GABA inhibitory system, increase the excitability of the motor cortex, and promote long-term potentiation of the motor area (Kaelin-Lang et al., 2002; Liu & Au-Yeung, 2017; Sawaki, Wu, Kaelin-Lang, & Cohen, 2006; Wu, van Gelderen, Hanakawa, Yaseen, & Cohen, 2005). Therefore, the reason for the effectiveness of PNS in restoring hand function might be that the stimulation of the median and ulnar nerves on the distal forearm encouraged the activation of the portion of the motor area controlling the hand. In addition, performing movements that involved the hand, such as exercise or practicing object manipulation, might have promoted neuroplastic changes in the areas of the cerebrum related to the hand, which in turn promoted motor function recovery.
Nevertheless, incorporating PNS into OT training further improves hand function recovery, and increase the scores of the WMFT and MAL in patients with good voluntary movements of the proximal upper limbs. Thus, in future, an assessment for the effects of adding PNS to rTMS and OT training in stroke patients would be valuable.
In this study, the patients who underwent PNS did not complain of pain or request the therapy to stop because of discomfort, and that PNS could be performed during regular OT training sessions. Furthermore, PNS involves electrical stimulation below the motor threshold (causing little pain or discomfort), it could be administered during OT training, while patients are using their upper limbs for object manipulation. Hybrid assistive neuromuscular dynamic stimulation (Shindo et al., 2011) is another form of therapy that uses electrical stimulation to trigger myoelectric potentials in target muscles. However, as this requires patients to sense the myoelectric potential, it is of limited use in patients with moderate paralysis who have difficulty in sensing the myoelectric potential. In contrast, the PNS used in our study could be performed in patients with moderate upper limb hemiparesis, thus, could be applied to a wider range of stroke patients.
Limitations
One of the limitations in this study was that the comparison group comprised of patients who had previously undergone rehabilitation treatment, and the history effect of the participants in the comparison group might confound their performance. In addition, we have not performed a follow-up evaluation for the long-term effects of interventions in this study. Finally, the study involved a small sample size, which might have influenced the results.
The intervention duration in this pilot study might be too short to induce an effect on the WMFT. In addition, the MAL, which was a secondary outcome, showed similar results to those of the WMFT. We had previously assumed that the improvement of hand movements would be reflected in activities of daily living; however, there was only significant improvement in the MAL between pre- and post-interventions in the PNS group but not in the comparison group. Thus, examining the intervention duration and methods in future studies is necessary.
Conclusion
This pilot study examined the effects of a two-week inpatient programme of rTMS and OT training, with and without PNS, for chronic stroke patients. The results indicated that combining PNS during OT training resulted in the greater recovery of hemiparetic hand functions. PNS involves stimulation below the motor threshold, which is easy to combine with upper limb functional training in OT, such as task-orientated training, and is clinically useful. Further investigations regarding the duration of PNS and how the recovery of hand movements with PNS could be linked up with the upper limb functional training for the improvement of object manipulation skills and increasing the use of hemiparetic upper limbs in everyday life are necessary.
Footnotes
Acknowledgments
We are grateful to the staff and patients of Kakeyu Hospital for their support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japanese Association of Occupational Therapists (Grant-in-aid research programme, Research II, 2018-02).