
Abstract
Objective
This study aimed to explore the therapeutic effect of high-frequency repetitive transcranial magnetic stimulation (HF-rTMS) with two different inter-train intervals (ITIs) on upper limb motor function in the early period of stroke.
Methods
We recruited 48 post-stroke patients in the early period and randomly divided them into three cohorts: the sham group, the short ITI (8 s) group, and the long ITI (28 s) group. HF-rTMS was delivered at 20 Hz. The amplitude of motor evoked potentials at the affected cortical region, representing the abductor pollicis brevis muscle, reflected cortical excitability. At baseline, immediately after treatment, and 1 month after treatment, we evaluated the recovery of upper limb motor function using Brunnstrom recovery stages (BRSs) and the Fugl–Meyer Assessment for upper extremity (FMA-UE), and assessed functional independence using the Barthel Index (BI).
Results
HF-rTMS with two different ITIs significantly improved upper limb functional recovery relative to the sham group, but there was no significant difference in cortical excitability changes or BRS, FMA-UE, or BI scores between the different ITI groups.
Conclusions
At the early post-stroke stage, HF-rTMS with short ITIs generates a similar therapeutic effect to HF-rTMS with long ITIs, suggesting that treatment times can be decreased.
Keywords
Introduction
Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive approach that is used to enhance plastic changes by stimulating cortical neurons. 1 Low-frequency rTMS (LF-rTMS; ≤1 Hz) reduces cortical excitability and high-frequency rTMS (HF-rTMS; >5 Hz) enhances cortical excitability.2,3 An increasing number of studies have shown that rTMS can cause sustained neuroplasticity in the brain, including long-term potentiation or depression. As a result, rTMS has been widely applied to treat neuropsychiatric disorders.4–7 Recently, rTMS has also been used effectively to improve motor function after stroke. 8 Interhemispheric competition is reported to be altered in post-stroke patients, with an increase in cortical excitation of the unaffected cortex and a decrease in cortical excitation of the affected cortex. 9 Thus, either inhibitory LF-rTMS over the contralesional motor area or excitatory HF-rTMS over the ipsilesional motor area have been delivered to promote motor function recovery in acute, subacute, or chronic stages of stroke. 10
As well as patient-related factors (e.g., on/off medication, disease status), rTMS treatment effects also rely on subtle differences in rTMS parameters, such as the stimulation intensity and frequency, stimulation site, stimulation train duration, pulse number per session, and total duration of stimulation.7,11 HF-rTMS is reported to be effective at enhancing motor performance in post-stroke patients. 12 Notably, a recent report demonstrated that HF-rTMS (using 20 Hz stimulation) with different inter-train intervals (ITIs) had a minimal effect on cortical excitability, but that the different intervals differentially influenced short-interval intracortical inhibition in healthy individuals. These findings provide evidence that ITIs might be able to be reduced with no influence on the effects of rTMS. 13 However, these conclusions were based on one session of rTMS in healthy individuals, and it remains unclear whether HF-rTMS with different ITIs might have similar effects in the treatment of neurological and psychiatric disorders. In the present study, we evaluated the effects of 20 Hz HF-rTMS treatment with short ITIs (8 s) or long ITIs (28 s) on upper limb motor function in post-stroke patients.
Material and methods
Participants
Acute ischemic stroke patients with upper limb paralysis were consecutively recruited between November 2018 and June 2019 from the Department of Neurology at the Integrated Hospital of Traditional Chinese Medicine, Southern Medical University. The inclusion criteria were as follows: 1) first-ever ischemic stroke; 2) fit the diagnostic criteria of stroke verified by cranial magnetic resonance imaging (MRI); 3) aged 18 to 70 years; 4) stroke onset was less than 2 weeks earlier; 5) patients had at least 10° of voluntary flexion and extension of the fingers and wrist in the affected limb; and 6) patients were conscious and had stable vital signs. The exclusion criteria were as follows: 1) severe trauma in the brain, or any other central nervous system disorders; 2) complications such as fever and epilepsy; 3) lack of compliance because of aphasia or cognitive impairment; 4) failure to obtain a motor evoked potential (MEP); 5) contraindications for MRI or rTMS (metal or implanted devices in the brain/skull, or a history of epilepsy or severe head trauma, as specified in the guidelines by Rossi et al. 14 ); and 6) other conditions that made the principal investigator consider the patient inappropriate for participation. The study protocol was approved by the ethics committee of the Integrated Hospital of Traditional Chinese Medicine, Southern Medical University. All patients gave written informed consent before treatment.
MEP measurements
Prior to the HF-rTMS treatment, MEPs were obtained using a magnetic stimulator (CCY-IV, Yiruide Co. Ltd, Wuhan, China) equipped with an electromyography apparatus. Patients were requested to remain relaxed throughout the experiments. To determine the hotspot of the cortical representative area of the abductor pollicis brevis (APB) muscle, the coil was optimally placed on the APB cortical representative area in the affected cerebral hemisphere where it induced the largest evoked potential, based on the International 10/20 system. 3 We then delivered magnetic stimulation over the hotspot. The resting motor threshold (rMT) was identified as the smallest intensity needed to generate a MEP of >50 μV peak-to-peak amplitude in 5 out of 10 consecutive stimuli, by applying single-pulse magnetic stimulation on the stimulation site.
rTMS protocol
The magnetic stimulation was delivered by a CCY-IV magnetic stimulator with a 7 cm “8”-type coil. The study participants were randomly assigned to three HF-rTMS groups using a randomization distribution table, generated by a computer. The three groups were the sham group, the short ITI group, and the long ITI group. All participants received 10 rTMS sessions over 2 weeks (one session per day from Monday to Friday). The basic HF-rTMS parameters were as follows: 20 Hz, 2-s stimulation, 1200 pulses, 110% intensity of rMT at the stimulation site. For short ITI rTMS, the parameters were: 2-s stimulation, 8-s interval, and 5 minutes per session. For long ITI rTMS, the parameters were: 2-s stimulation, 28-s interval, and 15 minutes per session. For the sham group, the magnetic coil was applied to the hotspot of the APB cortical representative area in the affected side of the brain, but no magnetic stimulation was delivered.
Conventional treatments
After each rTMS session, all participants received 30 minutes of conventional physical therapy and 30 minutes of occupational therapy from a specialized therapist during this study. Specifically, the conventional physical therapy consisted of active and passive motor exercises of the affected limbs. The occupational therapy consisted of functional tasks, such as holding a cup, taking a small object or ball, using chopsticks or a hairbrush, or other similar activities related to daily life. Additionally, conventional drug treatment was used and included antiplatelet and anticoagulation treatments, and the reduction of blood lipids, blood pressure, or blood glucose.
Clinical outcome evaluation
The impairment and recovery of upper limb motor function was evaluated using the Brunnstrom Recovery Stages (BRSs)15,16 and the Fugl–Meyer Assessment for upper extremity (FMA-UE). 17 The independence levels of patients were assessed using the Barthel Index (BI). 18 These clinical outcome assessments were performed by a neurologist with experience in these scales who was blinded to the study assignment at baseline, after rTMS, and at follow-up.
Statistical analysis
Statistical analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). The Student’s t-test and Mann–Whitney U test were used to compare normally and non-normally distributed data, respectively. Categorical data analysis was performed using the chi-squared test, while numerical data analysis was conducted using the repeated measures ANOVA. For within-group comparisons across the three time points, a repeated measures ANOVA with Bonferroni correction was performed. The three time points (baseline, after rTMS, and follow-up) were used as the within-group factors. The three groups were used as the between-group factors. A P-value less than 0.05 was considered a significant difference.
Results
Of the 64 initially recruited stroke patients in this study, 48 patients were eventually eligible (Figure 1). There were no significant differences among the three groups in basic clinical information, such as age; sex; onset, duration, and location of stroke; and baseline BRS, FMA-UE, and BI scores (Table 1). Four patients (one from the sham group, two from the short ITI group, and one from the long ITI group) were discharged before the end of rTMS because of medical insurance complications, leading to rTMS termination. In addition, four patients were lost during follow-up: two patients in the sham group and one patient in each of the short and long ITI rTMS groups. No adverse events, such as seizure, headache, or aggravated motor function of the upper limb, were reported throughout this study.

Flow diagram of the study.
Demographic and clinical characteristics of participants.
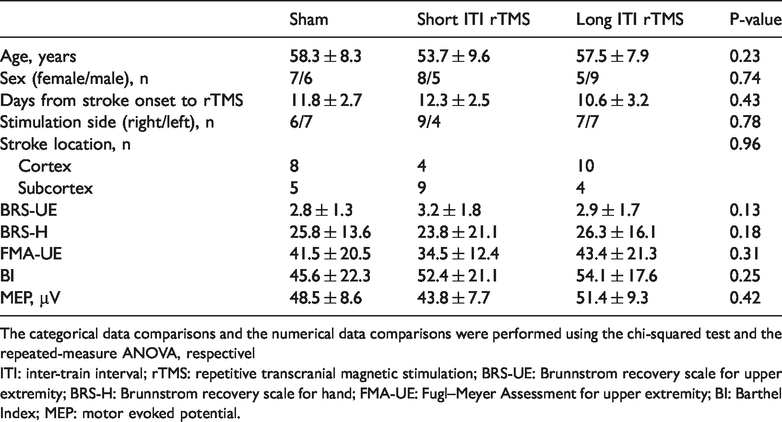
The categorical data comparisons and the numerical data comparisons were performed using the chi-squared test and the repeated-measure ANOVA, respectivelITI: inter-train interval; rTMS: repetitive transcranial magnetic stimulation; BRS-UE: Brunnstrom recovery scale for upper extremity; BRS-H: Brunnstrom recovery scale for hand; FMA-UE: Fugl–Meyer Assessment for upper extremity; BI: Barthel Index; MEP: motor evoked potential.
In the post-stroke patients, the percentage of cortical excitation was markedly increased in the affected side of the brain in all three groups immediately after the rTMS or sham intervention (F = 5.57, P = 0.003; Figure 2). The increase was maintained for at least 1 month. Compared with the sham group, the two rTMS groups had higher increases in the percentage change of cortical excitation (immediately after intervention: P = 0.028 for the long ITI group, P = 0.032 for the short ITI group; at the 1-month follow-up: P = 0.017 for the long ITI group, P = 0.036 for the short ITI group). However, there was no difference in the change of excitability between the short and long ITI rTMS groups (P = 0.16).
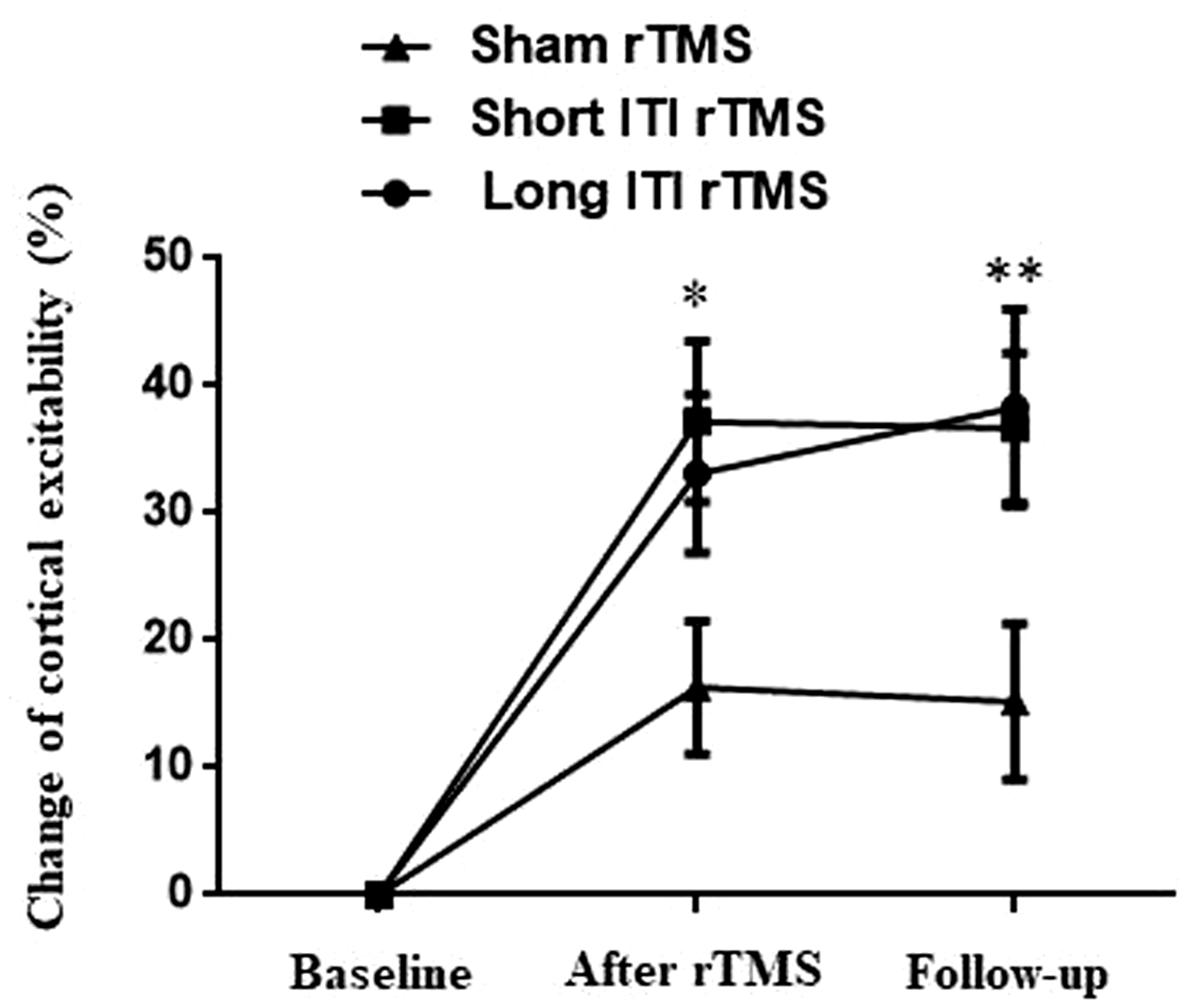
Effect of short and long ITI HF-rTMS on the percentage change of cortical excitability in the affected hemisphere of post-stroke patients, as reflected by mylohyoid MEP amplitude. *P < 0.05 and **P < 0.001 indicate a significant difference compared with the sham group. There were no significant differences between the short ITI group and the long ITI group. The percentage change of cortical excitability was calculated using the following formula: (MEP amplitude after stimulation course or at the end of follow-up – MEP amplitude before stimulation)/MEP amplitude before stimulation × 100%.
Clinical assessments of BRS for upper extremity (BRS-UE), BRS for hand (BRS-H), FMA-UE, and BI at the three time points (prior to rTMS, immediately after intervention, and at the 1-month follow-up) are illustrated in Figures 3 and 4. There were significant interactions between time point and intervention for BRS-UE (F = 2.72, P = 0.036), BRS-H (F = 3.17, P = 0.037), FMA-UE (F = 4.48, P = 0.012), and BI (F = 2.19, P = 0.013) scores. For the within-group analysis, there were marked improvements in all clinical outcome assessments in all three groups after 10 treatment sessions compared with the baseline scores (all P<0.001 in the two rTMS groups; all P<0.01 in the sham group). These improvements were maintained at the 1-month follow-up. Relative to the sham group, the patients who received rTMS had a larger change in all assessments immediately after stimulation (all P<0.05; Figures 3, 4), and this was maintained at the 1-month follow-up. There were no significant differences in BRS-UE, BRS-H, FMA-UE, or BI scores between the short and long ITI rTMS groups either immediately after rTMS treatment or at the 1-month follow-up (Figures 3, 4).

Effect of short and long ITI HF-rTMS on motor function (BRS-UE and BRS-H scores) of the affected upper limb of post-stroke patients. The BRS-UE scores (a) and BRS-H scores (b) at baseline, after treatment, and at the 1-month follow-up in the sham, short ITI, and long ITI groups. There was a significant improvement in the two rTMS groups. *P<0.05 and **P<0.01 indicate a significant difference compared with the sham group. There were no significant differences between the short ITI group and the long ITI group.

Effect of short and long ITI HF-rTMS on motor function (FMA-UE and BI scores) of the affected upper limb of post-stroke patients. FMA-UE (a) and BI (b) scores at baseline, after treatment, and at the 1-month follow-up in the sham, short ITI, and long ITI groups. There was a significant improvement in the two rTMS groups. *P<0.05 and **P<0.01 indicate a significant difference compared with the sham group. There were no significant differences between the short and long ITI groups.
Discussion
In the present study, we demonstrated that two different HF-rTMS protocols (HF-rTMS with 8 s ITI and HF-rTMS with 28 s ITI) promoted the recovery of motor function in the affected upper limb of hemiplegic patients in the early stroke stage. These two protocols had a similar therapeutic effect, but were markedly different in the amount of time taken to complete 10 rTMS sessions: 50 minutes for the short ITI protocol versus 150 minutes for the long ITI protocol. No noteworthy adverse effects were observed in either of these groups.
rTMS is a promising noninvasive approach for improving motor function rehabilitation in post-stroke patients. 1 There is evidence that HF-rTMS is useful in enhancing motor performance in patients in the chronic, 19 subacute, 20 and acute stages 21 of stroke. Different rTMS parameters (e.g., stimulus frequency and intensity, and the total number of pulses) lead to different therapeutic effects by differentially influencing cortical excitation and inhibition. 11 High-frequency stimulation (>1 Hz) is often used to increase cortical excitation in the affected side of the brain following stroke, based on the stroke-induced imbalance of excitation and inhibition between the two hemispheres. 10 HF-rTMS parameters involve stimulation frequency and intensity, ITI, duration, and total amount of stimulation. Higher frequencies of magnetic stimulation, and especially a frequency of 20 Hz, have been demonstrated to elicit more profound excitation effects with less interindividual variations. 22 Additionally, it has been reported that using more pulses may cause more inhibitory cortical alterations. 23 Thus, the therapeutic effect of rTMS may rely on the “dose” of rTMS. 24
The ITI is an important parameter of HF-rTMS, and is necessary to introduce excitatory effects. However, very short ITIs are thought to be unsafe, and potentially lead to seizures. One previous study suggested that 20 Hz HF-rTMS with 5 s ITIs is safe in healthy volunteers. 25 Another study reported that intermittent theta-burst stimulation (iTBS) with 8 s ITIs may promote the introduction of excitatory effects and decrease the enhancement of inhibitory effects compared with continuous TBS. 26 Accordingly, we used 20 Hz HF-rTMS with 8 s ITIs in the present study, and did not observe any adverse effects, such as seizures or headaches. However, the optimal ITI to elicit an excitatory effect remains to be investigated. It has been proposed that more robust effects might be induced by rTMS with a shorter ITI and a longer total stimulation duration. However, a recent study in healthy individuals demonstrated that 20 Hz HF-rTMS at different pulse intervals (4, 8, 16, and 32 s) had little effect on cortical excitability, but had differing effects on intracortical inhibition at the shorter intervals. 13 Consistent with this previous study, our results from patients in the early period after stroke suggested that 20 Hz HF-rTMS with 8 s ITIs had comparable therapeutic effects to 20 Hz HF-rTMS with 28 s ITIs. These findings suggest that shortening ITIs may not affect rTMS efficacy, which may lead to a decreased time and cost of clinical rTMS treatment. In addition, to shorten the whole course of treatment, augmenting session numbers or pulse numbers may also be beneficial. There is evidence to suggest that HF-rTMS twice daily is tolerable for patients with depression, and appears to be comparable to once daily HF-rTMS in the treatment of depression, while decreasing the number of required hospital visits.27,28 However, it is unclear if such conclusions may also apply to stroke patients, and further research is required.
Our study had some shortcomings. First, this was a small-scale, single-center clinical trial; thus, our findings need to be confirmed by large-scale, multicenter studies. Second, a previous report suggested that rTMS has a better effect on motor recovery in patients with subcortical stroke compared with cortical stroke. 29 We were unable to observe a difference in therapeutic effect between the two stroke-type subgroups because we had very small sample sizes (as few as four patients per subgroup). In future studies, the same type of stroke patients (either cortical or subcortical) should therefore be recruited. Third, in the current study, HF-rTMS over the motor cortex was used to improve the recovery of upper limb motor function. However, it remains unknown if our findings are applicable to other cortical regions, or to improve related neurological disorders such as depression. Finally, any other changes in HF rTMS parameters, such as a higher frequency, more pulses per session, or a longer treatment time, may lead to different results or an altered safety profile; more research is therefore needed.
Footnotes
Declaration of conflicting interest
The author(s) declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Natural Science Foundation of China (no. 81671284 and no. 81471338 to X. Zhou).