
Abstract
Introduction
Studies on autism spectrum disorder in recent years have controversially indicated similarities with schizophrenia. Cognitive dysfunction is present in both disorders, and while there is a rich array of interventions for cognitive dysfunction in schizophrenia, there are few such treatments for autism spectrum disorder. In this study, we have investigated a potentially useful approach in autism spectrum disorder by comparing autism spectrum disorder with schizophrenia in regard to the characteristics of cognitive dysfunction and therapeutic response to cognitive remediation therapy.
Method
We studied seven patients with autism spectrum disorder and eight patients with schizophrenia, using a frontal/executive programme as the intervention. The characteristics of cognitive dysfunction in autism spectrum disorder before frontal/executive programme and the therapeutic response to frontal/executive programme in autism spectrum disorder patients were compared with those in schizophrenia patients, based on evaluation of cognitive function and social function. The changes in cognitive and social function after treatment in each patient group were compared using the Mann–Whitney’s U test.
Results
The severity of cognitive dysfunction did not differ significantly between autism spectrum disorder and schizophrenia. Frontal/executive programme was effective in autism spectrum disorder, with subjects showing about the same therapeutic response as in schizophrenia.
Conclusion
Frontal/executive programme appears to be useful for patients with autism spectrum disorder. Furthermore, the similarities in cognitive dysfunction and therapeutic response between autism spectrum disorder and schizophrenia are highly relevant to the recent debate concerning the similarity between these two disease concepts.
Keywords
Introduction
Psychiatric occupational therapy in Japan is now recommended not only for schizophrenia patients but also for the growing numbers of individuals with developmental disorders such as autism spectrum disorder (ASD) (Yotsumoto, 2015). Consequently, psychiatric occupational therapy must now be provided for patients with a wider variety of disorders than in the past (Japanese Association of Occupational Therapists, 2010). Psychiatric occupational therapy now not only provides interventions for daily living support and social skills but also includes more therapy aimed at reducing cognitive dysfunction and improving social outcomes.
Cognitive function in schizophrenia has been studied since the 1960s, and in recent years, cognitive dysfunction has come to be seen as a core symptom of this disorder (Green, 1996). Since the beginning of the 21st century, cognitive remediation therapy (CRT) has garnered attention as a new intervention for cognitive dysfunction and it has been the subject of much research in recent years. CRT has been defined as “a behavioral training-based intervention that aims to improve cognitive processes (attention, memory, executive function, social cognition, or metacognition) with the goal of durability and generalization” (Matsui, 2012), thereby achieving direct improvement in cognitive function and generalization to social function.
While cognitive dysfunction in schizophrenia has been the subject of considerable research, attention is also beginning to turn to cognitive function in ASD. Several brain regions such as the amygdala, caudate nucleus, and prefrontal cortex show abnormalities in ASD (Cheung et al., 2010; Pinkham, Hopfinger, Pelphrey, Piven, & Penn, 2008). Environmental factors also exert an influence over time, so that by adulthood, each ASD patient will have acquired his or her own particular neural foundations and behavioral patterns. The developmental process results in individual differences in abilities and also gives rise to neurocognitive deficits in such areas as executive function, memory, and visuospatial cognition. Among them, a number of executive dysfunctions have been reported in ASD (Pennington & Ozonoff, 1996). In addition, obstacles to theory of mind and joint attention have also been reported (Dahlgren & Trillingsgaard, 1996; Sigman, Mundy, Sherman, & Ungerer, 1986). Attempts have been made to treat these dysfunctions with CRT, but in only a small number of patients, and further study is needed regarding the treatment of cognitive dysfunction in ASD.
Although there are a variety of forms of CRT, almost none aim to stimulate brain function in a graded and comprehensive manner. The frontal/executive programme (FEP) is a form of CRT designed specifically to treat frontal lobe dysfunction in schizophrenia. It aims to stimulate cognitive function from a low to high level. Its effectiveness has been demonstrated in schizophrenia (Omiya et al., 2016), and it has also been shown to be effective in ASD (Miyajima et al., 2016). Accordingly, the cognitive dysfunction of ASD is an essential therapeutic target; it is expected that FEP would produce the same therapeutic effect for both ASD and schizophrenia. Therefore, the goal of this study was to compare individuals with ASD and schizophrenia with regard to the characteristics of cognitive and social dysfunction and therapeutic responses to FEP.
Methods
Subjects
The subjects were outpatients of the psychiatric department at Asahiyama Hospital who were determined by a psychiatrist to meet the DSM-5 criteria for ASD or schizophrenia. The inclusion criteria were age no older than 60 years and at least nine years of formal education; the exclusion criteria were dementia, drug dependence, alcohol dependence, and organic brain disease. This was a single-blind study with an FEP intervention group randomly assigned from patients with ASD and schizophrenia who were registered in the study. FEP was conducted in seven subjects diagnosed with ASD (three males, four females; mean age 36.1 ± 8.1 years) and eight subjects diagnosed with schizophrenia (three males, five females; mean age 43.3 ± 14.5 years). All participants gave written informed consent. Ethics approval was granted by the Ethics Committee of the Faculty of Health Sciences, Hokkaido University, and the Ethics Committee of Asahiyama Hospital.
Details of the intervention
The FEP used for this study was developed by Delahunty and Morice (1993) and published in Japan in a translation by Matsui, Shibata, and Shosaku (2015). The FEP consists of three modules: cognitive flexibility, working memory, and planning. It is designed so that the tasks become progressively more difficult as the sessions proceed. Each module is made up of tasks focusing on eye movement and perception, organization of information, fine motor movements, and others. The therapist encourages the subject to verbalize problem-solving methods and gives instruction on the use of effective strategies. In this way, the FEP system encourages subjects to execute tasks as correctly as possible. The FEP consists of 44 sessions in total, and each session includes training mainly using paper and pencil but also includes the use of building blocks (tokens) and fine hand movements. The subjects had two one-on-one sessions a week with the therapist, each lasting 1 h.
All therapists were occupational therapists and clinical psychologists who participated in joint study meetings. At the meetings, each trainer presented details of his or her sessions; FEP role-playing and video filming were used to increase shared understanding and perception toward FEP and reduce intertherapist differences in intervention methods.
Assessment
Cognitive functioning
The Brief Assessment of Cognition in Schizophrenia-Japanese version (BACS-J), Wisconsin card sorting test (WCST), and continuous performance test (CPT) were used to assess cognitive functioning. The BACS-J was devised by Keefe et al. (2004) and the Japanese version was developed by Kaneda et al. (2007) and validated by Kaneda et al. (2013) afterwards. It is used to assess cognitive functioning in the subjects based on scores in six cognitive function domains: verbal memory, working memory, motor speed, attention, executive functions, and verbal fluency, and a composite score. The assessment score was determined by calculating z-scores derived by comparison with the mean of normal individuals.
The WCST (Heaton, Chelune, Talley, Kay, & Curtiss, 1993) is a task that involves sorting cards according to certain rules that change over time, reflecting functioning in the prefrontal cortex. The WCST 128-card computerized version consists of four stimulus cards and 128 responses cards that depict figures of varying form, number of objects, and colors. The subject is instructed to sort each responses card under one of the stimulus cards and is told whether the sort was right or wrong. The subject must discover the correct matching rule using this feedback. When he or she succeeds in a category classification, the category achievement number increases (maximum value is 10). A wrong answer that cannot change the rule and repeat classification is called a perseverative error of the Milner type (PEM), and the erroneous reaction that classifies the card into the same category as the last mistake is called a perseverative error of the Nelson type (PEN). Individuals with schizophrenia and ASD have a marked tendency to perseverate and tend to complete fewer categories than unimpaired adults (Lysaker & Bell, 1994; Russo et al., 2007; Saoud et al., 2000; Van Eylen et al., 2011). In this study, the number of categories achieved, PEN, and PEM were used for the data analysis.
The CPT measures the ability to sustain attention by concentrating on letters randomly displayed on a computer screen and giving responses according to certain rules. Assessment is based on response time and number of errors (Rosvold, Mirsky, Sarason, Bransome, & Beck, 1956). In the data analysis of this study, the reaction time (ms) and the scores of errors were compared before and after treatment.
Social functioning
Social functioning was assessed using the Schizophrenia Cognition Rating Scale-Japanese version (SCoRS-J) and the Life Assessment Scale for the Mentally Ill (LASMI) (Iwasaki et al., 1994). SCoRS-J is an assessment scale recommended by the United States MATRICS (Measurement and Treatment Research to Improve Cognition in Schizophrenia) Neurocognition Committee as a suitable scale for functional prognosis with validity. It was devised by Keefe, Poe, Walker, Kang, and Harvey (2006) and the Japanese version was created by Kaneda et al. (2010). This scale assesses cognitive deficits related to day-to-day functioning and consists of 20 questions in the eight domains of memory, learning, attention, working memory, problem-solving, processing/motor speed, social cognition, and language. The responses to the 20 questions are graded 1–4, with a higher score reflecting more severe impairment. Based on these questions, global ratings from 1 (mild) to 10 (severe) are determined. This study used the global ratings in the data analysis. The questions are answered by the patient, an evaluator, and the patient’s caregiver, and the overall assessment is based on the mean score of all three respondents and the global score.
The LASMI is designed to evaluate the everyday and social life of individuals with schizophrenia; its reliability and validity have been established by Iwasaki et al. (1994). It consists of daily life, interpersonal relations, work skills, endurance and stability, and self-recognition from a total of 40 items in 5 subscales (Iwasaki et al., 1994). Each question is evaluated in five grades of 0–4, with the higher score reflecting more severe impairment. In the data analysis of this study, the average score of the five subscales was calculated, and the score was compared before and after the treatment.
The cognitive functioning scales were evaluated by the psychologist’s research assistant and the social functioning scales were evaluated by the medical staff and the occupational therapists who know the subjects well.
Data analysis
We compared the results of the assessments of both groups (ASD versus Schizophrenia), with respect to clinical characteristics, using Chi-square tests and the Mann–Whitney U test. To measure the therapeutic responses of both groups, the difference value before and after FEP treatment was evaluated. SPSSver20.0 (IBM) was used for the statistical analysis and the significance level was set at 0.05.
Results
Clinical characteristics
Clinical characteristics are shown in Table 1. There were no significant intergroup differences in age, years of education, sex, or IQ (p > .2). However, the amount of antipsychotic medication was significantly higher in the schizophrenia group (p < .01).
Baseline characteristics of participants.
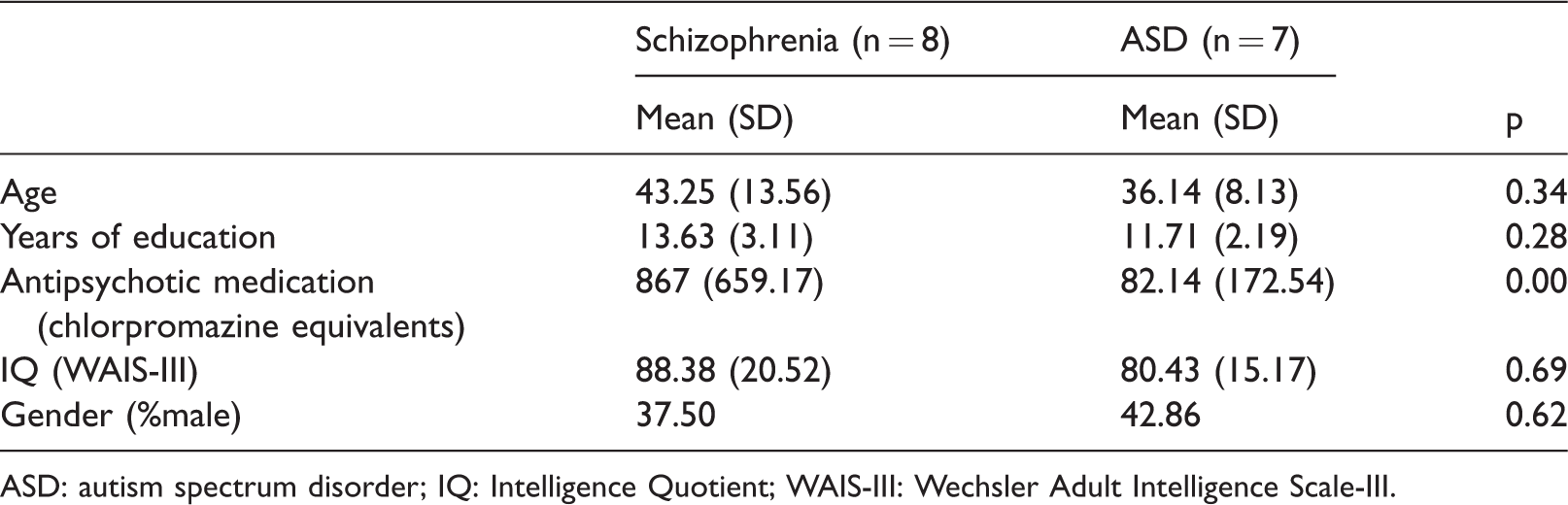
ASD: autism spectrum disorder; IQ: Intelligence Quotient; WAIS-III: Wechsler Adult Intelligence Scale-III.
Comparison of cognitive function and social function before and after treatment
Differences in cognitive function in both groups before and after treatment are shown in Table 2. There were no significant intergroup differences in the BACS-J (p > .5), WCST (p > .2), or CPT tests (p > .09) of the cognitive function assessments. Changes in the BACS-J composite scores are shown in detail (Figure 1). The results in both groups showed a similar upward trend after treatment compared to before treatment. Differences in social function in both groups before and after treatment are shown in Table 3. There were no significant differences between groups on the SCoRS-J (p > .05) and LASMI (p > .07) of the social function assessments.
Characteristics of cognitive function in participants with both disorders before and after frontal/executive programme.
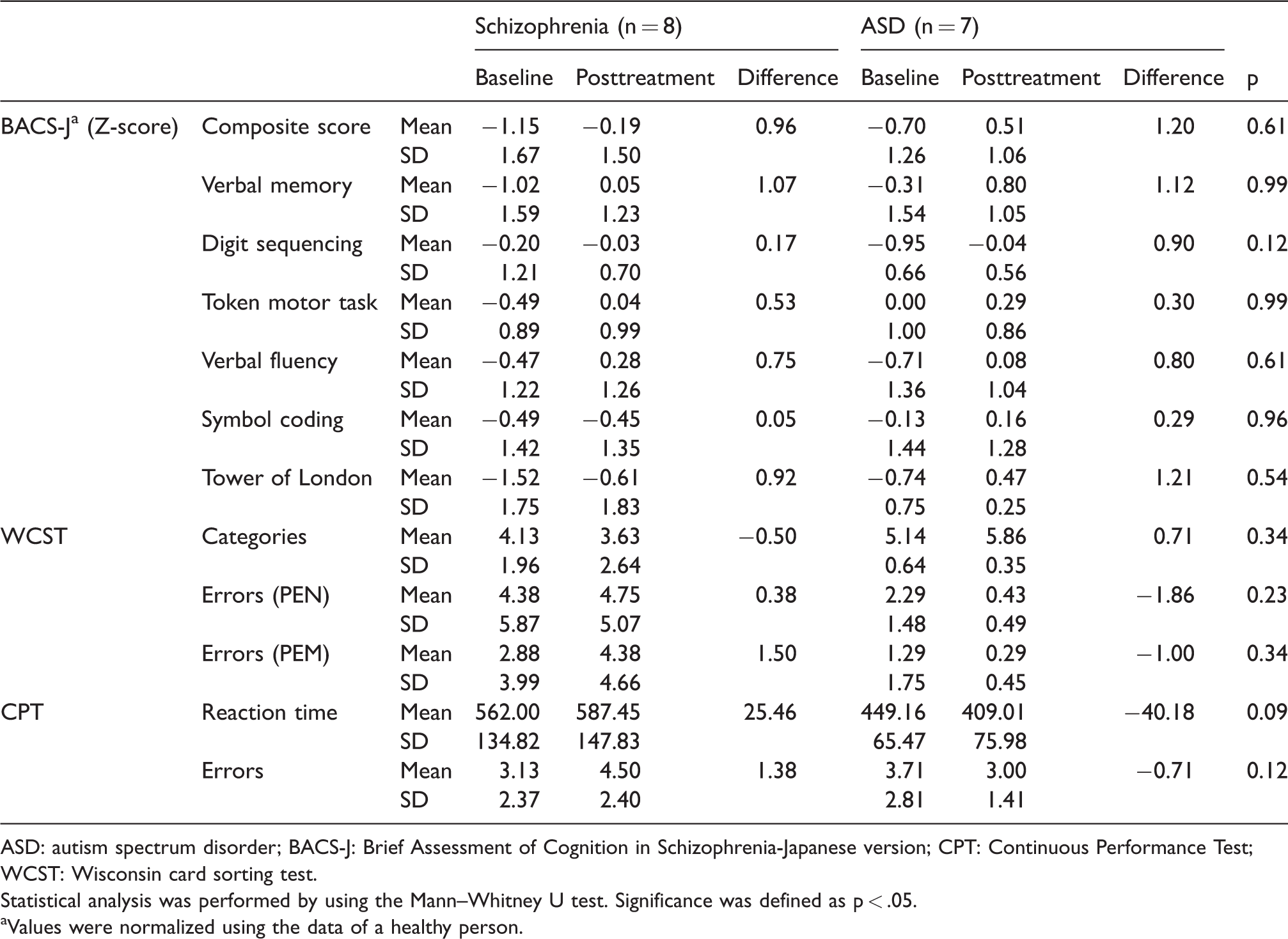
ASD: autism spectrum disorder; BACS-J: Brief Assessment of Cognition in Schizophrenia-Japanese version; CPT: Continuous Performance Test; WCST: Wisconsin card sorting test.
Statistical analysis was performed by using the Mann–Whitney U test. Significance was defined as p < .05.
aValues were normalized using the data of a healthy person.
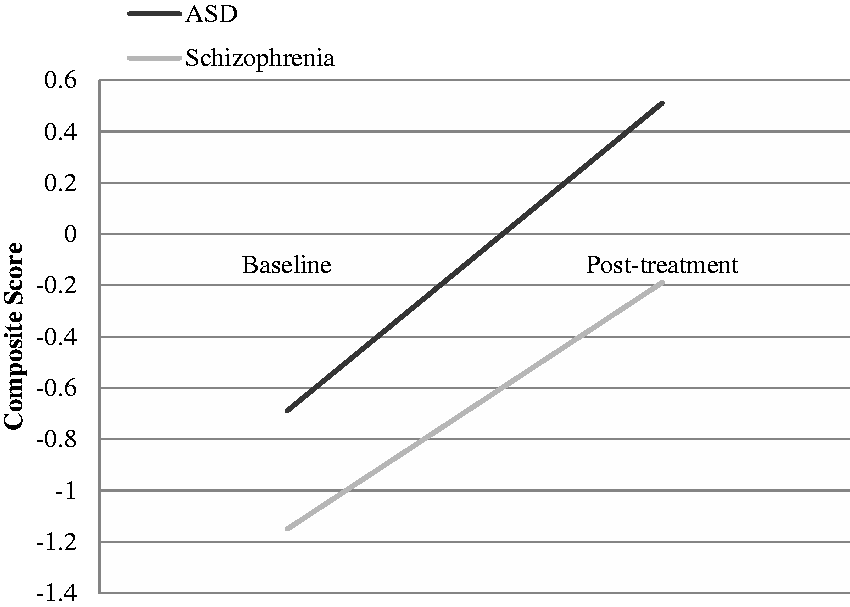
Changes in BACS-J composite scores after treatment. ASD: autism spectrum disorder.
Characteristics of social function in both disorders before and after frontal/executive programme.
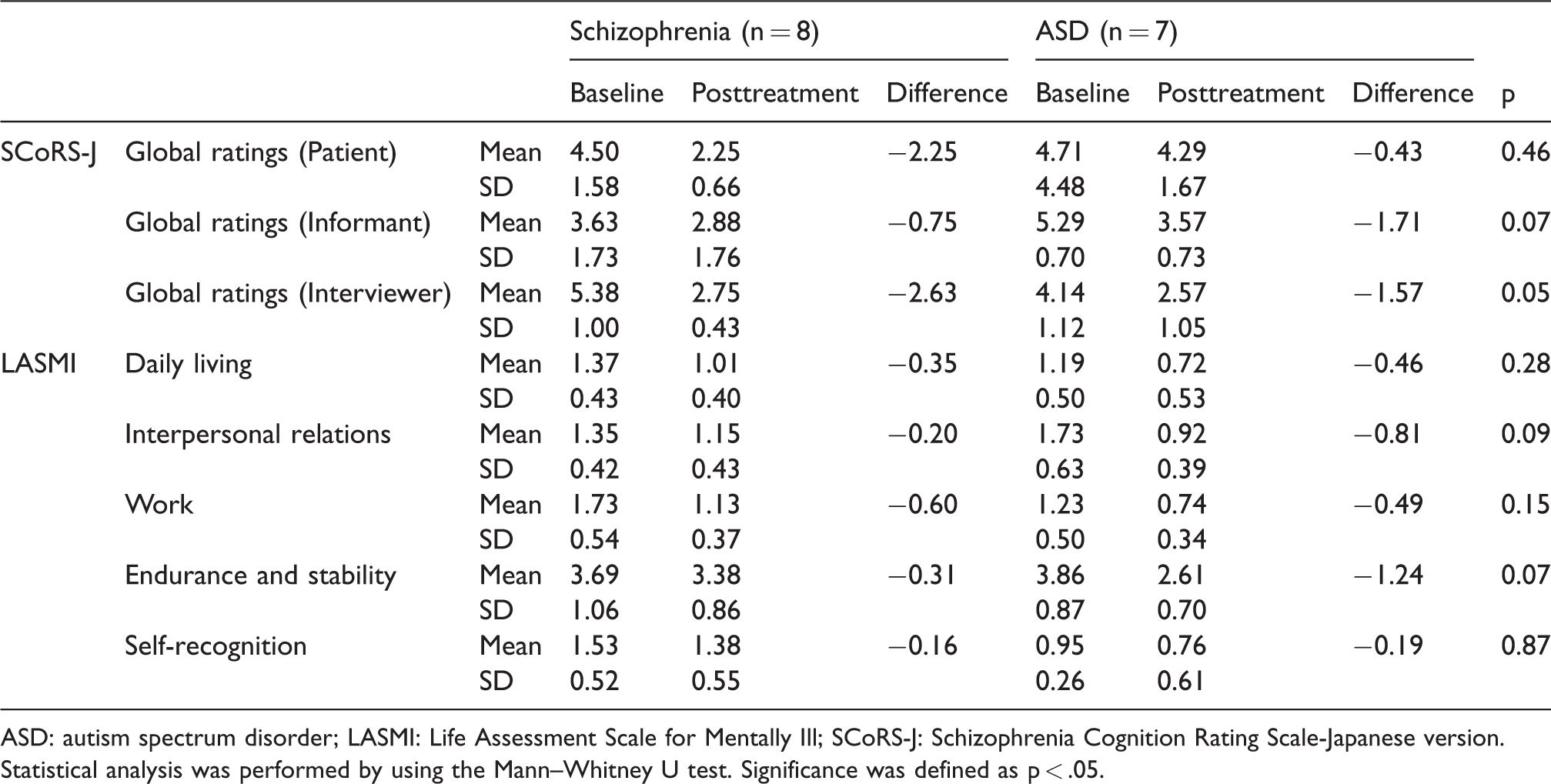
ASD: autism spectrum disorder; LASMI: Life Assessment Scale for Mentally Ill; SCoRS-J: Schizophrenia Cognition Rating Scale-Japanese version.
Statistical analysis was performed by using the Mann–Whitney U test. Significance was defined as p < .05.
Discussion
Cognitive dysfunction and social dysfunction responses to FEP
This is the first study to compare the therapeutic responses to FEP in ASD and schizophrenia. The level of cognitive dysfunction was found to be broadly similar in both disorders but slightly milder in ASD. This means that despite individual differences in ability among individuals with ASD, the characteristics of cognitive dysfunction in this group as a whole are not dissimilar to those in individuals with schizophrenia. FEP produced improvements in cognitive and social function in both groups, as has been found in previous research. The present study also found that in terms of therapeutic responses, individuals with ASD showed a similar level of improvement as those with schizophrenia.
FEP is a CRT programme that was originally designed specifically to treat frontal lobe dysfunction in chronic schizophrenia patients and is the only CRT that is a graded and comprehensive programme. The results of this study suggest that FEP is similarly effective as a therapy for frontal lobe dysfunction in ASD. The characteristic difficulties in strategic learning seen in both disorders are challenged in FEP by the requirement to accurately verbalize task content and task strategies. It is believed that this kind of training helps to promote the internalization of strategic learning and leads to improvements in memory, executive function, verbal fluency, and other cognitive processes (Wykes, Huddy, Cellard, McGurk, & Czobor, 2011). Omiya et al. (2016) and Miyajima et al. (2016) posit that improvements in social function arise not only from generalization of the improvement in cognitive function but also from the influence of the FEP therapeutic environment. It is speculated that improvements in social function are influenced by an increase in the subject’s sense of self-control as a result of the matching of language and thought, enhancement of intrinsic motivation as a result of active and independent training, and enhancement of a sense of self-efficacy and sense of achievement as a result of the close relationship with the therapist.
Another interesting finding is that individuals with ASD showed a similar level of cognitive dysfunction as those with schizophrenia and also a similar level of therapeutic responses to FEP. There is still some controversy regarding the similarity between ASD and schizophrenia. Historically, there have been periods when autism was regarded as childhood schizophrenia and periods when the two disorders were considered to be completely distinct (American Psychiatric Association, 2013). The disease concepts of both schizophrenia and autism have received much attention in recent years following the identification of similarities in cognitive function, brain imaging results, and genetic risks associated with disease onset (Cheung et al., 2010; Kasai et al., 2003; Pinkham et al., 2008; Yung et al., 2003). Chisholm, Lin, Abu-Akel, and Wood (2015) have investigated theoretical models for the association between the two disorders based on a review of prior research on co-occurrence. The models with good evidence supporting the reasons for co-occurrence were the increased vulnerability model, the associated liabilities model, the diametrical model, and the multiple overlapping etiologies model. The similarities in cognitive dysfunction and therapeutic responses seen in our subjects could perhaps be explained by the findings of these models (Chisholm et al., 2015).
As stated above, there are many commonalities between ASD and schizophrenia from the genetic level to cognitive dysfunction and clinical features. Consequently, against this background of similarities and a high possibility of co-occurrence, there has been an increase in ASD patients who would be eligible for psychiatric occupational therapy. The therapeutic effectiveness of and therapeutic responses to FEP demonstrated by our study also support the idea that provision of CRT as part of psychiatric occupational therapy for schizophrenia could be beneficially extended to ASD patients. The most essential strategy is the joint provision of CRT and occupational therapy at an early stage to improve cognitive and social functions, regardless of the disorder.
Limitations
In this study, the small sample size of both groups seems to be a likely confounding factor for the results of the therapeutic responses to FEP. Therefore, further research is needed to determine the effectiveness of FEP in a larger number of ASD patients and to investigate in more detail the characteristics of cognitive dysfunction and therapeutic responses in both disorders.
Conclusion
We investigated the characteristics of cognitive dysfunction in ASD and the therapeutic responses of ASD patients to FEP. Previous studies have found similarities between ASD and schizophrenia at the genetic level and in brain imaging. Both disorders also exhibit a similar level of cognitive dysfunction. The therapeutic responses to FEP were also similar in both disorders, and it was thought that this similarity could be explained by the resemblance between the two disease concepts. For this reason, CRT should be provided at an early stage in ASD, as it is in schizophrenia.
Footnotes
Acknowledgments
The authors thank all of the participants involved in study. We also thank the members of Asahiyama Hospital for their support with this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.