
Abstract
Keywords
“Dietary habits are associated with cancer risk and survival, whilst also affecting the risk of other chronic diseases, including those associated with cancer risk.”
Introduction
Dietary habits are associated with cancer risk and survival, whilst also affecting the risk of other chronic diseases, including those associated with cancer risk. Estimates vary, but the landmark report by Doll and Peto from 1981 and revisited in 2015 suggested that up to 35% of cancers could be attributable to diet although the risk varies based on cancer site.1,2 More conservative calculations from the United States suggest that 3.4% and 4.9% of cancer risk in women and men, respectively, are associated with dietary risk factors. 3 When you include alcohol consumption as a risk factor, this increases to almost 10%. Unhealthy dietary patterns are now also the leading risk factor for chronic illness and premature death worldwide. 4 Globally, diets have increasingly shifted towards being high in ultra-processed and animal-based foods while lacking in fiber-rich plant foods. 4 This type of diet promotes inflammation, insulin resistance, and adversely affects the gut microbiome, which may promote carcinogenesis. 5 Studies show that these unhealthy dietary patterns negatively impact rates of remission, survival, and quality of life after a cancer diagnosis whilst increasing the risk of cardiometabolic diseases and second cancers.6,7
This knowledge has been incorporated into national and international guidance from the World Cancer Research Fund (WCRF)/American Institute of Cancer Research (AICR) and American Cancer Society (ACS) on cancer prevention and survivorship with recommendations to increase intake of fruits, vegetables, whole grains, and beans, whilst avoiding processed meat and alcohol, and minimizing red meat and ultra-processed foods.8-10 Yet, awareness amongst people with cancer and their families remains low. 11 This may be, in part, because the support from dietitians during cancer care is limited and mainly directed towards preventing weight loss. 12 In addition, oncologists have little undergraduate or postgraduate nutrition training and are not equipped to address dietary questions.13-15 Patients with cancer are keen to receive dietary guidance from their oncologist, but rarely receive this, leading to patients obtaining their information from non-accredited sources.11,12,16-19
The aim of this study was to investigate: (1) Whether oncologists are aware of available dietary guidelines for cancer; (2) Whether oncologists routinely educate patients about dietary guidelines and support patients in making healthier dietary changes; (3) Oncologists’ attitudes and barriers toward the importance of dietary counselling for improving the health and well-being of their patients; and (4) Whether oncologists’ personal dietary choices influence their dietary recommendations for patients.
Methods
Survey and Study Design
A 25-question online survey was developed collaboratively between the research team, composed of a hematologist, a hematologist and medical oncologist, a radiation oncologist, a research dietitian, a sociologist, and a statistician, following a literature review to establish existing knowledge. The survey was divided into the following sections: General information about the respondent including demographics and clinical practice, respondents’ dietary behaviors, respondents’ current practice with regards to dietary counselling, attitudes and barriers towards dietary counselling, and knowledge of current dietary guidelines for cancer. The full survey can be found in the supplemental data file 1.
Participant Inclusion and Recruitment
The survey was administered to oncology providers through the American Society of Clinical Oncology (ASCO) Research Survey Pool (RSP), a service available to members who engage in survey research. The RSP provides a mechanism for surveying oncology professionals made available through ASCO’s Center for Research and Analytics (CENTRA). The survey “pool” consists of ASCO members worldwide who have opted-in to participate in optional research survey projects conducted by other members. The survey was administered using an online survey tool from Qualtrics. The survey was distributed to 1157 current members between July 9th and August 20th, 2024, selected at random by CENTRA. The following selections were made from the ASCO database of members; fellows and currently practicing oncologists (exclude students); Stage of career: currently practicing (exclude retired); Degrees: advanced practice providers and doctoral level physicians (exclude nurses); Location: domestic and international; Professional role: gynecologic oncologist/hematologist/medical oncologist/pediatric oncologist/radiation oncologist/surgical oncologist; Cancer type: all cancer types. In addition, the survey was distributed to members of the British Society of Haematology (BSH). An initial question was included to exclude those not currently seeing patients with cancer for at least 4 h per week from completing the survey. No incentive was offered to respondents.
Ethics and Data Protection
This study was reviewed by the Memorial Sloan Kettering Cancer Center Institutional Review Board and determined to be exempt from further review. The survey was fully anonymized.
Statistics
Descriptive analyses are presented for responses to survey questions. Fisher’s exact and Pearson’s Chi-squared tests were used to analyze associations between participants’ personal dietary patterns and their practice behaviors, attitudes and beliefs. Participants were divided into 3 groups: omnivorous, plant-based dietary patterns (pescatarian/vegetarian/vegan/plant-based/Mediterranean), and Western diet based on their self-reported diet pattern.
Results
Respondents Characteristics.
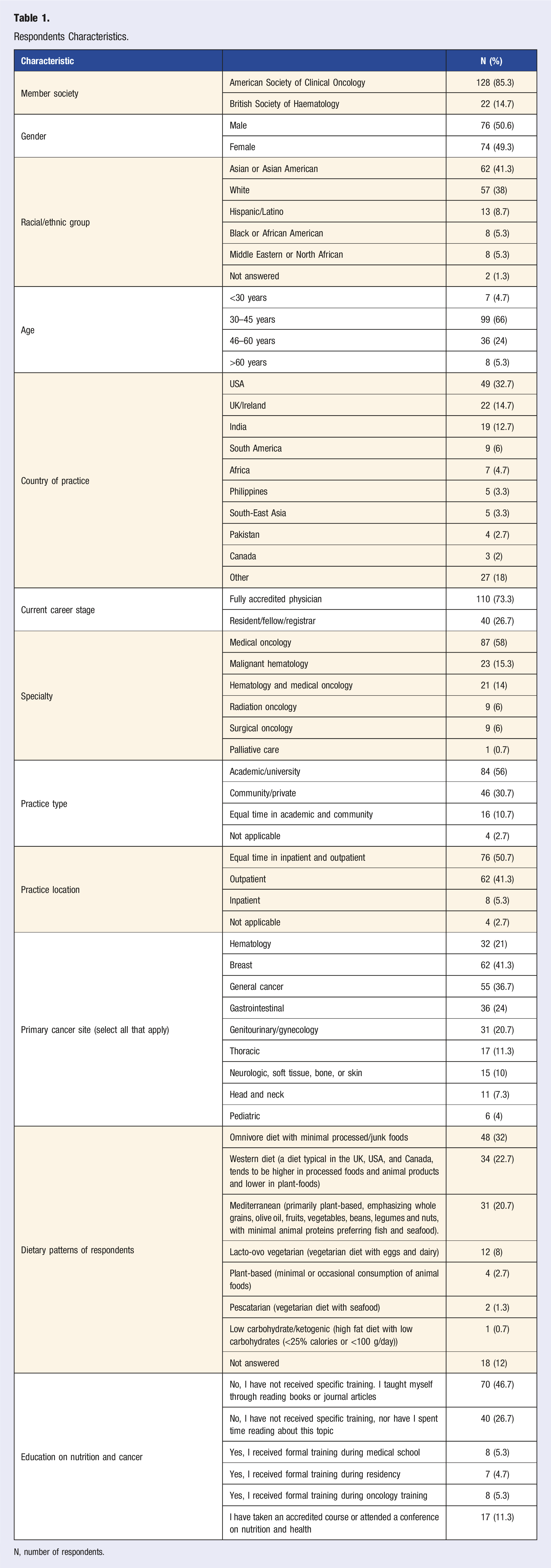
N, number of respondents.
Respondents’ Practice Patterns
Just under a quarter of respondents referred all their patients with cancer to a dietitian/nutritionist while 1.3% referred none of their patients. Respondents also mentioned referring patients for reasons such as patient request (46%), cancer symptoms or treatment side effects that affect nutritional status (58%), and chronic comorbidities such as obesity, diabetes mellitus, cardiovascular disease (20%). When asked about the frequency of discussing diet and nutrition with patients, responses included very often (24%), often (34.7%), sometimes (23.3%), rarely (6%), and not applicable (12%).
Respondents were asked if they provided available cancer-specific dietary guidelines to their patients. While 47.4% provided guidelines, 17.3% were not aware of any guidelines and 35.3% discussed nutrition but did not provide any guidelines. The guidelines most often used included National Comprehensive Cancer Network (NCCN), ASCO, WCRF/AICR, and ACS (see supplemental file 2, Table 1).
Respondents’ Dietary Guidance
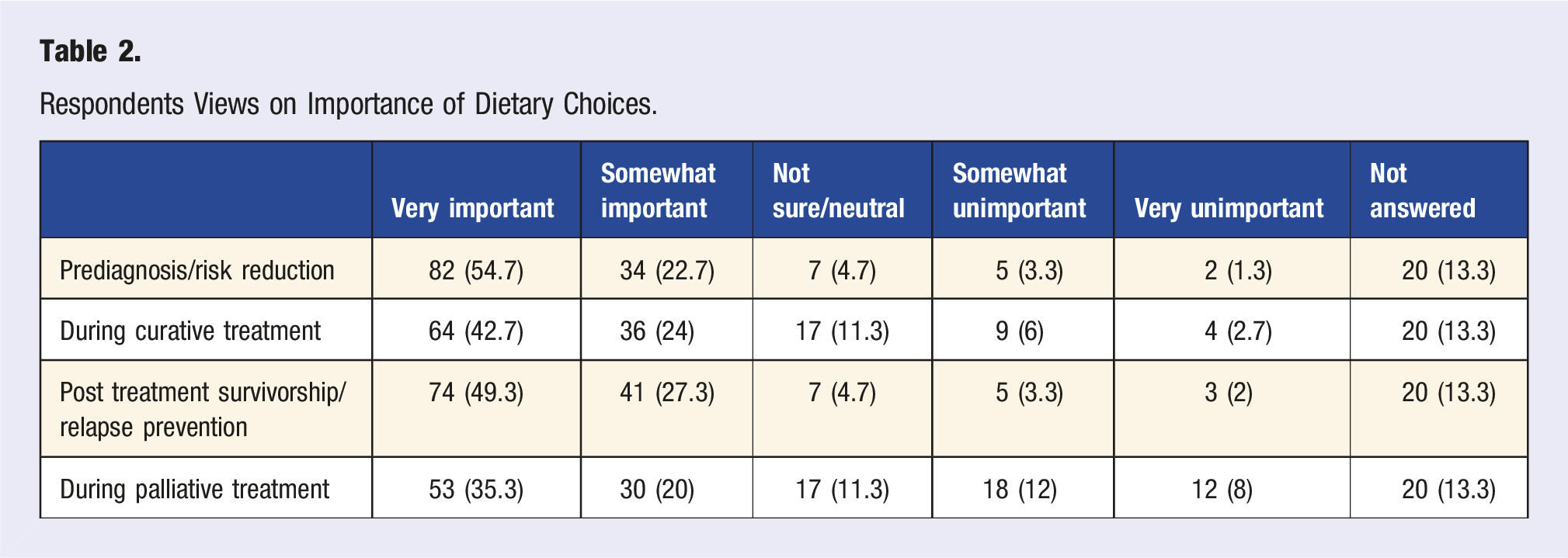
Respondents Views on Importance of Dietary Choices.
Respondents’ Dietary Recommendations for Patients With Cancer. a
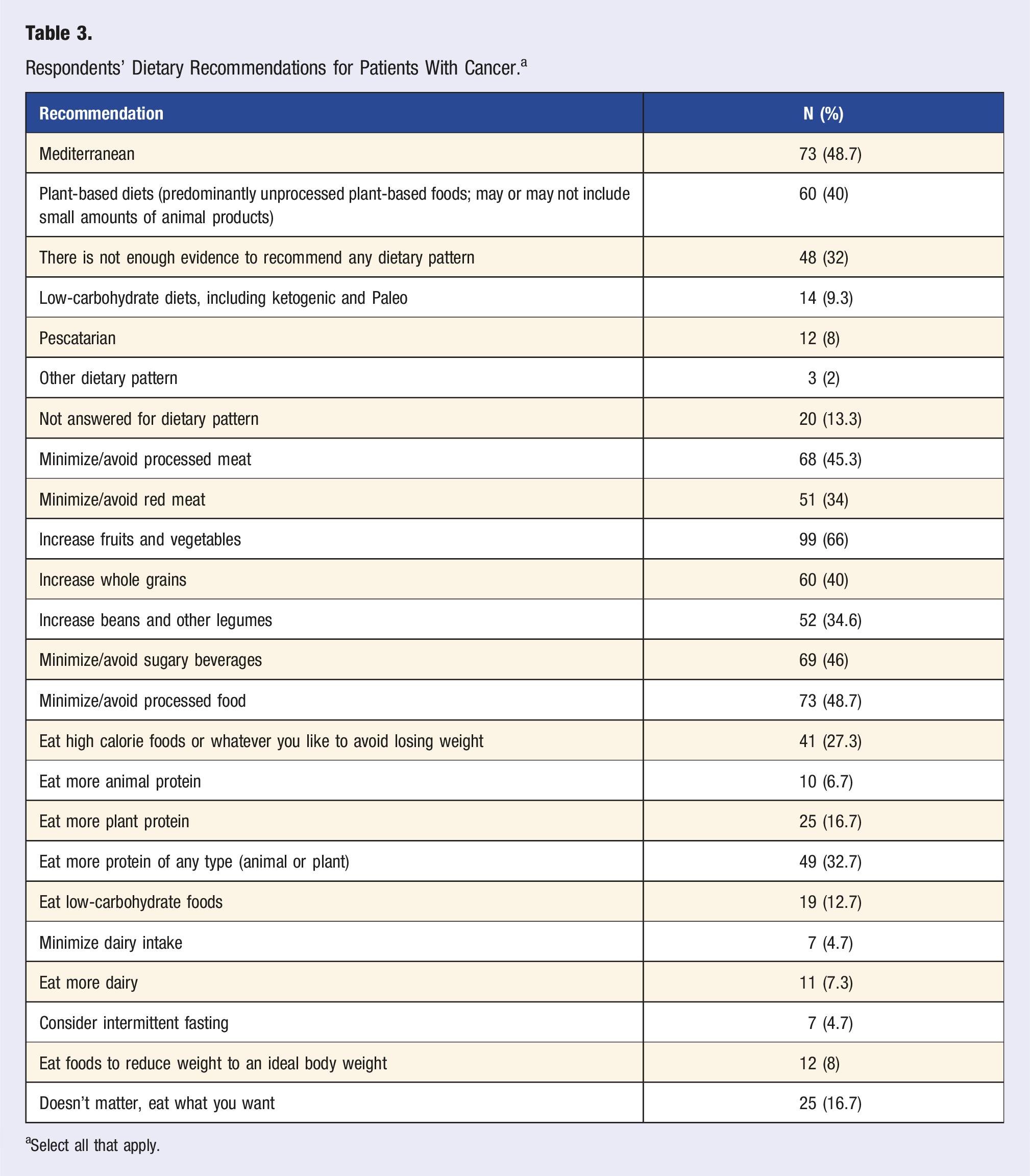
aSelect all that apply.
Table 3 shows specific dietary recommendations provided to patients by respondents. The most common recommendations given were to increase consumption of fruits and vegetables (66%), whole grains (40%), beans and legumes (34.6%), and protein (32.7%) and to avoid/minimize processed food (48.7%), sugar-sweetened beverages (46%), and processed meat (45.3%).
Regarding alcohol consumption, 43% respondents advised avoiding alcohol consumption, whereas 27% advised drinking in moderation (≤1 drink per day for women or ≤2 drinks per day for men) as acceptable, 11% didn’t provide advice, 7% provided individualized advice, and 12% did not respond to this question.
Respondents’ Education, Attitudes, Barriers, and Knowledge
Respondents Perceived Barriers When Discussing Nutrition With Patients. a
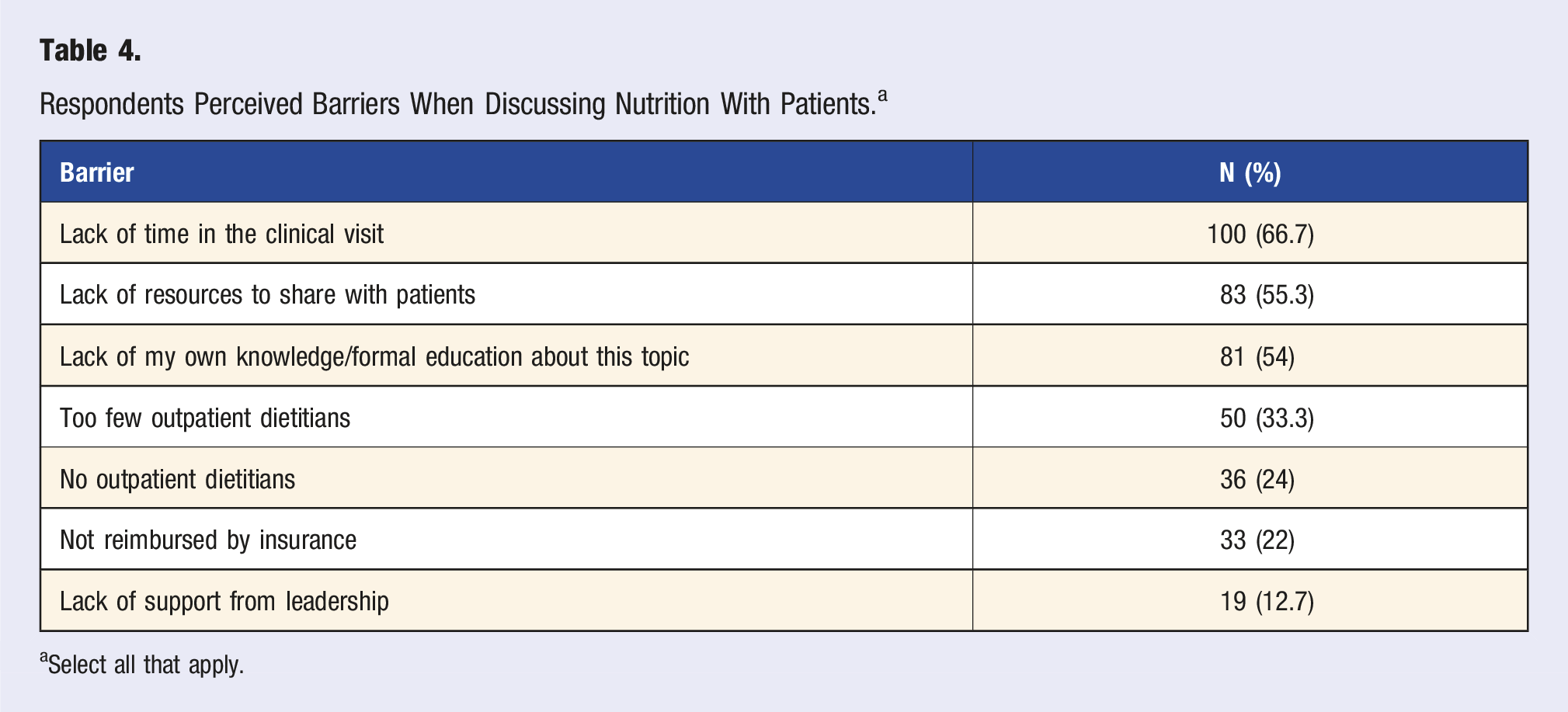
aSelect all that apply.
Respondents Beliefs as to Whether There is Sufficient Evidence to Provide Nutrition Recommendations to Patients.
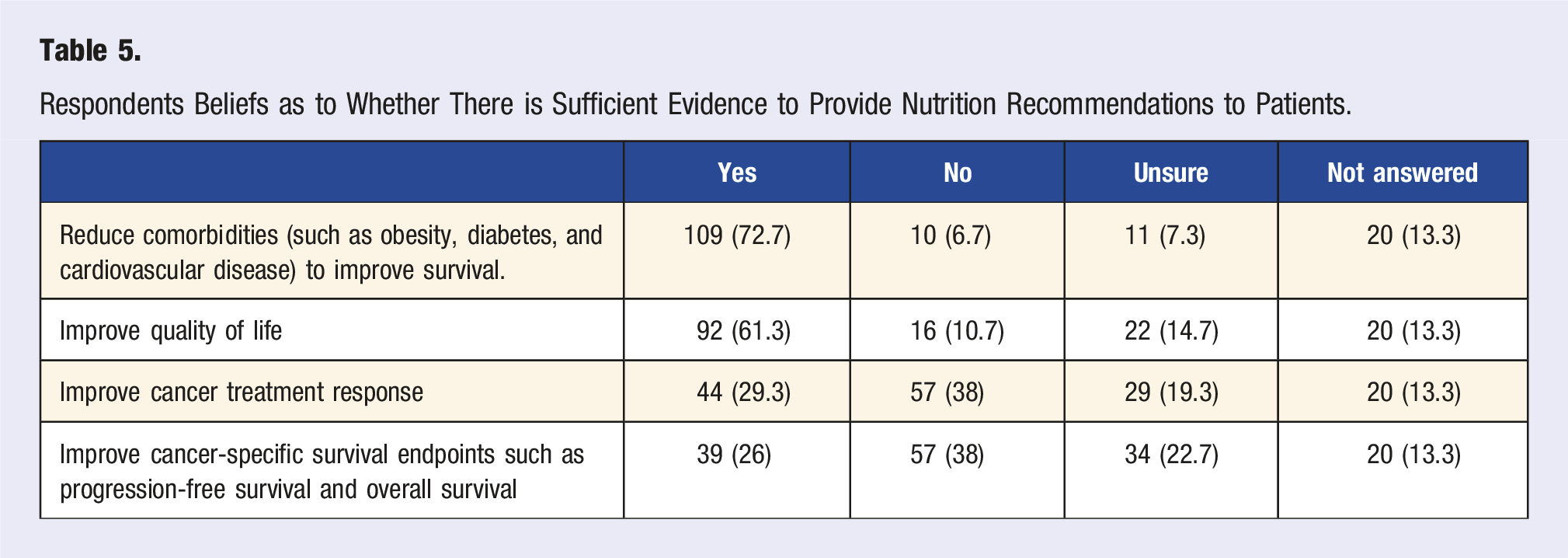
Respondents were asked about the type of evidence they would require in order to recommend a specific dietary pattern to their patients. The majority would like to see data from interventional clinical trials in cancer populations while a smaller proportion felt that epidemiologic, retrospective, preclinical data as well as data in non-cancer comorbidities would be acceptable to share. For interventional clinical trials, 66.7% would like to have evidence from a large, randomized phase 3 interventional dietary trial with a clinical cancer outcome as a primary endpoint; 64.7% evidence from a large, randomized phase 3 interventional dietary trial with a non-cancer clinical outcome (such as quality of life) as a primary endpoint; 44% evidence from a randomized phase 1 or 2 dietary interventional trial showing potential benefit and 25.3% evidence from a non-randomized phase 1 or 2 dietary interventional trial showing potential benefit. For non-trial evidence, 50% of participants would be satisfied with evidence from large population-based epidemiologic studies and preclinical data, 31.3% with evidence from retrospective studies with correlative data, and 34.7% with evidence from research confirming benefits of dietary changes for comorbidities (diabetes, cardiovascular disease, obesity).
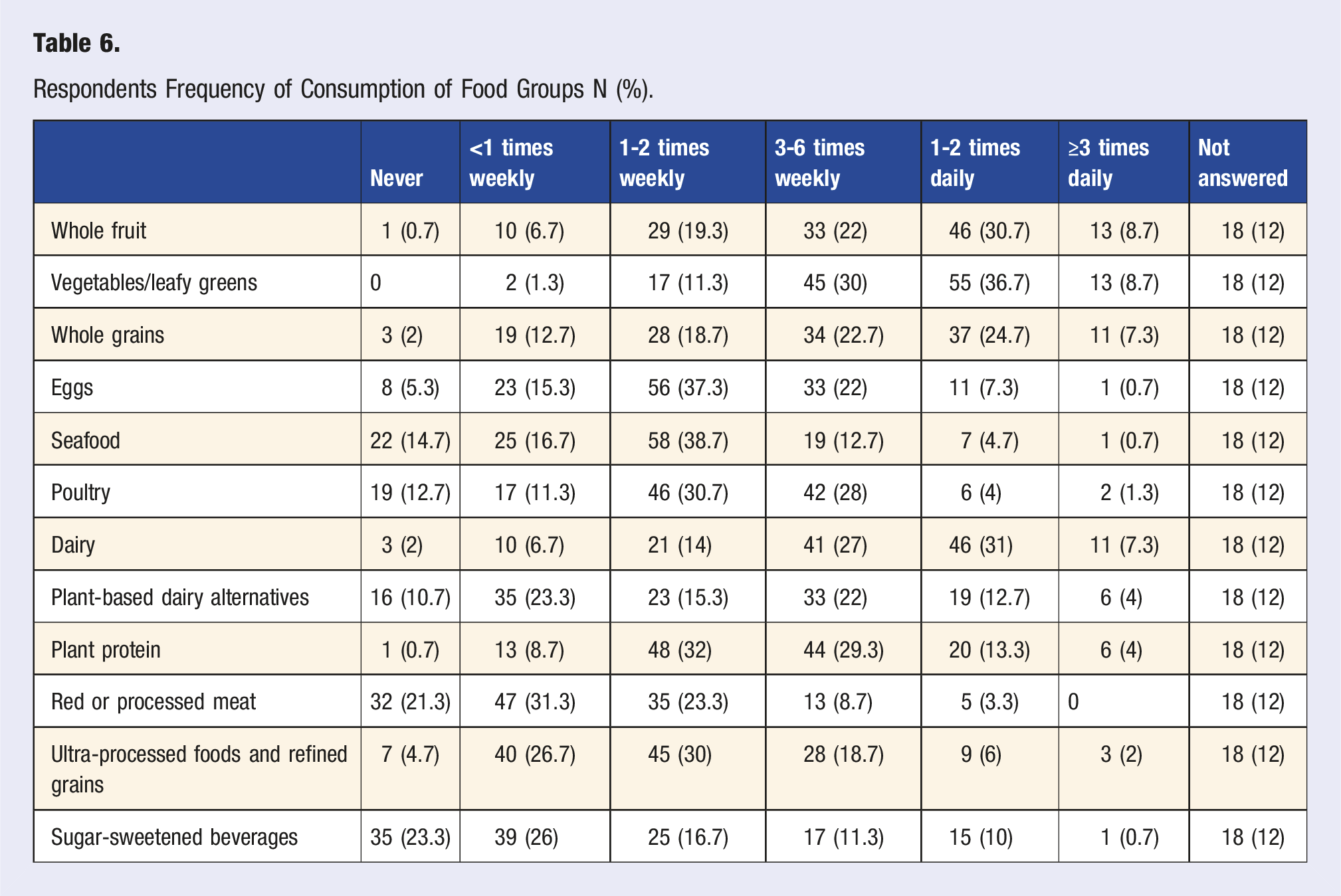
Respondents’ Personal Self-Reported Dietary Behaviors
Respondents Frequency of Consumption of Food Groups N (%).
Respondents’ Personal Choices May Affect Dietary Guidance Provided to Patients
In a subgroup analysis, responses were compared based on respondents’ own dietary choices between omnivorous (n = 42), Western (n = 32), and predominantly plant-based dietary patterns (n = 49) (Supplemental file 2, Table 2). While the frequency of discussing nutrition with their patients was not different, those following a Western diet were significantly more likely to tell patients to “eat what they want” (P = .005) and less likely to recommend low-carbohydrate diets (P = .049) when compared to those following an omnivorous or plant-based dietary pattern. Participants following a plant-based dietary pattern (36.7%) were more likely to consider their role to discuss nutrition with patients compared to participants following an omnivorous (23.9%) or Western diet pattern (15.6%) (P = .024). While the number of respondents receiving training was low overall, those following an omnivorous (14.2%) or plant-based (4.1%) diet were more likely to select that they received formal lectures during oncology training compared to Western diet (0%) (P = .036). Consistently, those following a plant-based diet (12.2%) were more likely to have taken an accredited course or attended a conference on nutrition compared to western/omnivorous diet (0%) (P = .01). Participants following a plant-based dietary pattern were more likely to consider diet to be “very important” for reducing the risk of cancer (P = .002), during curative treatment (P = .002), for survivorship/relapse prevention (P = .024), and during palliative treatment (P = .008) compared to those following an omnivorous or Western diet.
Discussion
This survey highlights the current awareness amongst oncologists of the role of dietary patterns in cancer care as well as the persistent barriers that limit the integration of nutrition counselling into routine oncology practice. While the majority of respondents acknowledged the importance of dietary choices across the cancer continuum, from prevention to survivorship, there remains a significant gap between awareness and implementation. Only a subset of oncologists routinely provided cancer-specific dietary guidance, and many report inadequate training and resource constraints. This is at odds with patient expectations and their clinical needs given that prior studies have documented the importance placed on nutrition counselling by patients and the high prevalence of diet-related problems.11,12 Surprisingly, the percentage of respondents referring all their patients to a dietitian was higher than expected (23.3%), given that prior survey data have shown that staffing of nutrition and dietetic services in cancer centers is inadequate. 20
Consistent with existing literature, the majority of respondents had received little or no formal nutrition education during their medical training, despite evidence that patients increasingly seek nutritional advice from their oncology care teams.13,14,21 This lack of training, coupled with structural barriers such as time limitations and insufficient access to dietetic support, was reported as a major impediment to offering comprehensive nutrition counselling. These findings underscore the need for enhanced nutrition education in medical curricula and greater institutional support for continuing medical education support in nutritional oncology as well as system-level changes to allow integration of dietary guidance into oncology services. This is being addressed to some degree with countries such as the USA and UK having issued guidance on nutrition training and competencies for medical students.22,23 Medical schools and residency programs are beginning to incorporate various types of nutrition programs including “food as medicine” and “culinary medicine” and postgraduate fellowships in nutrition are emerging. 24 In addition, the American Board of Lifestyle Medicine offers a global certification program for physicians that includes nutrition education. 25 Importantly, these training programs should integrate physician dietary counselling and skills development to build self-efficacy for adherence to plant-based eating patterns.
In fact, this study identified a relationship between oncologists’ self-reported personal dietary behaviors and their clinical practice. Respondents adhering to a plant-based dietary pattern (pescatarian/vegetarian/vegan/Mediterranean) were more likely to counsel patients on diet and engage in self-directed learning on nutrition. Conversely, respondents following a Western dietary pattern were less likely to consider dietary choices important at the various stages of a patient’s cancer journey. Respondents following plant-based dietary patterns were more likely to consider dietary choices important for patients receiving curative treatment. This correlation suggests that personal health behaviors may influence clinicians’ perceptions of the relevance of dietary advice in oncology, aligning with previously observed trends in Lifestyle Medicine. 26 Given that fiber-rich dietary patterns are recommended in cancer-specific dietary guidelines, this may be a reflection of respondents’ own knowledge.8-10
While the majority of respondents expressed belief in the value of dietary interventions for improving quality of life and reducing comorbidities, fewer felt confident in the evidence linking diet to treatment response or cancer-specific outcomes. This is despite the presence of numerous observational studies and some recent clinical trials that suggest potential benefits of dietary interventions for cancer-specific outcomes.27-31
A significant proportion of respondents indicated that large randomized controlled trials with clinical endpoints would increase their confidence in recommending specific dietary patterns. These views are in keeping with the ASCO guideline on diet during cancer treatment, which states that the evidence supporting dietary interventions is currently limited. 32 This underscores the need for further research to build a robust evidence-base and translate findings into clinical practice guidelines. Randomized studies are ongoing and being reported with encouraging results 33 . The LEANer trial demonstrated higher rates of pathological complete remission in patients with breast cancer on chemotherapy who received a nutrition and exercise intervention. 30 The currently funded ENICTO U01 will address diet and relative dose intensity in 2 patient groups—those with breast cancer (≥65 years) and ovarian cancer. 34
Strengths of this study include that it addresses an important yet under-explored area in oncology practice, especially given the degree of patient interest. It uniquely correlates oncologists’ personal dietary patterns with their clinical behaviors and attitudes, offering novel insight into how lifestyle factors may influence professional practice. The international sample offers insights across various oncology subspecialties and practice settings and provides actions that can be taken within the profession to address gaps in knowledge and practice. However, the study has a number of limitations. The small sample size limits the generalizability of the results although the 13% response rate is in keeping, if not better than other survey’s administered through ASCO. 15 In addition, all of the participants were physicians, whereas nurse specialists, physician associates, and other allied health professionals play an important role in supporting patients through their cancer journey and are potentially more likely to be involved in assessing non-medical needs such as nutrition. 35 There is also the potential that self-selection bias may have led to an overrepresentation of individuals with a greater interest in diet and nutrition. For example, 32.7% reported consuming a plant-based dietary pattern, a proportion that is higher than expected from a physician community. 36 Additionally, responses were self-reported without the use of a validated dietary questionnaire and hence subject to recall and social desirability bias. Self-reported dietary patterns did not necessarily align with reported consumption of food group. For example, less than 10% of respondents consumed 3 or more portions of fruit, vegetables, and whole grains a day, yet 20% reported consuming a Mediterranean-style dietary pattern. Finally, while the study included participants from multiple countries, the majority were practicing in high-income settings, which may limit generalizability to low-resource contexts.
Lastly, barriers to dietary guidance include lack of resources. In order to implement system-wide changes, institutions will need to acquire more staffing in dietetics and include registered dietitians with oncology practice certification. Additionally, institutions will need to address patient barriers to adoption of healthy diet patterns such as food insecurity, knowledge deficits, and self-efficacy to achieve dietary goals.
Conclusions
The results of this study emphasize the current state of awareness among oncologists of the importance of diet in cancer care, while also revealing critical gaps in training, confidence, and practice. There is a clear need for improved nutrition education throughout medical training, including support for enhancement of physician diet quality, as well as better integration of dietary guidance into routine oncology practice. Efforts to strengthen the evidence base through high-quality clinical trials, combined with system-level support and resource development, are essential to meet patient needs and realize the potential of dietary interventions in improving cancer outcomes.
Supplemental Material
Supplemental Material - Oncologists Knowledge and Attitudes Towards Providing Dietary Guidance to Patients With Cancer
Supplemental Material for Oncologists Knowledge and Attitudes Towards Providing Dietary Guidance to Patients With Cancer by Shireen Kassam, Zahra Kassam, David Nemirovsky, Andriy Derkach, Susan Chimonas, Cynthia Thomson, and Urvi A. Shah in American Journal of Lifestyle Medicine.
Supplemental Material
Supplemental Material - Oncologists Knowledge and Attitudes Towards Providing Dietary Guidance to Patients With Cancer
Supplemental Material for Oncologists Knowledge and Attitudes Towards Providing Dietary Guidance to Patients With Cancer by Shireen Kassam, Zahra Kassam, David Nemirovsky, Andriy Derkach, Susan Chimonas, Cynthia Thomson, and Urvi A. Shah in American Journal of Lifestyle Medicine.
Footnotes
Ethical Approval
This study was reviewed by the Memorial Sloan Kettering Cancer Center Institutional Review Board and determined to be exempt from further review. The survey was fully anonymized.
Author Contributions
Conceptualization: SK, ZK, and US; methodology: SK, ZK, SC, CT, and US; data collection: SK, ZK, and US; analysis: DN, AD, SK, ZK, and US; original draft: SK; review and edition: ZK, US, SC, CT, DN, and AD.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the NIH/NCI Cancer Center Support Grant (P30CA008748), the American Society of Hematology Scholar Award, the Paula and Rodger Riney Foundation, Blood Caneer United Academic Trials Grant and the Gabrielle’s Angel Foundation Grant (U.A. Shah), Radiation Oncology Physician Research Fund, Stronach Regional Cancer Centre (Z. Kassam), King’s College Hospital Research Fund (S. Kassam).
Declaration of Conflicting Interests
U.A. Shah reports grants from the Leukemia Lymphoma Society, NIH/NCI Cancer Center Support Grant (P30CA008748), American Society of Hematology, Gabrielle’s Angel Foundation, Paula and Rodger Riney Foundation, Willow Foundation, and HealthTree Foundation during the conduct of the study as well as grants from Bristol Myers Squibb and Janssen, personal fees from Sanofi, Janssen and i3 Health, and nonfinancial support from Sabinsa and M&M Labs outside the submitted work. No disclosures were reported by the other authors. S.K., Z.K., D.N., A.D., S.C., C.T. have no conflicts of interest to declare.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.