
Abstract
Our findings indicate clustering of lifestyle behaviors among emerging adults in the US and we successfully identified unique lifestyle patterns for males and females.
Introduction
Emerging adulthood is an important, and often positive, developmental period for individuals in their late teens to mid-twenties. 1 However, emerging adults in the United States (US) experience the highest prevalence of depression compared to all other adults, about 1 in 5, which equates to over 6 million individuals.2,3 High rates of depression increase the risk of suicide, which is the second leading cause of death for this age group. 4 Emerging adults experience various unique factors that may increase their risk of depression. For instance, emerging adults experience a great deal of stress and pressure related to situations like living alone for the first time, starting work or higher education, and developing relationships.5-7 These unique pressures, in addition to increased use of social media, can contribute to depression.5-10 The consequences of depression among this age group are widespread, with negative impacts on work and school performance, relationships, and health. 11 Depression negatively impacts overall health and the development of other mental illnesses, as well as comorbid diseases, such as obesity, diabetes, and cardiovascular disease.12-14 These negative consequences can continue beyond emerging adulthood and are associated with increased mental and physical morbidity and mortality throughout adulthood.15-17 Therefore, depression in emerging adults is a serious public health burden that warrants additional study.
Despite increased access to psychotherapies and pharmacotherapies in recent years, depression rates among emerging adults have continued to rise.18-20 As modest increase in treatment cannot keep up with the prevalence of depression among emerging adults, research should explore risk factors that, once targeted, have the potential to reduce symptoms of depression. 3 Although numerous factors influence the mental health of emerging adults including financial, academic, and social pressures, focusing on modifiable lifestyle behaviors allows for more targeted and proactive depression management. Modifiable lifestyle behaviors are promising intervention targets for mental illness, especially for emerging adults. Emerging adulthood involves a dynamic shift in physical and social environments, which influences key lifestyle behaviors. 8 While emerging adulthood presents many challenges, this life stage also presents a unique opportunity for intervention as one’s lifestyle is just beginning to be developed. As a result, lifestyle psychiatry is incorporating a holistic approach to prevent and treat depression by adjunctively targeting modifiable lifestyle behaviors. 21 Physical activity, diet and nutrition, restorative sleep, social connection, mindfulness and meditation, and mind-body activities have been emphasized as the domains of lifestyle psychiatry due to their role in the pathophysiology of mental illness and effectiveness in improving symptoms of mental illness.21-23 A lifestyle encompasses various behaviors, including those targeted in lifestyle psychiatry, but other related behaviors, like sedentariness and substance use (e.g., smoking and drinking), should also be considered.21,24 Among these behaviors, a poor quality diet, poor sleep duration and sleep quality, physical inactivity and sedentariness, tobacco/nicotine use, and alcohol consumption have been independently associated with depression in emerging adults.25-37
Overall diet quality of US emerging adults is poor and often marked by pro-inflammatory dietary behaviors, including increased intake of fast foods, foods high in salt and sugar, as well as reduced intake of fruits and vegetables and breakfast.27,38,39 Pro-inflammatory dietary patterns are associated with depression,40,41 particularly in emerging adults, suggesting that the inflammatory potential of the diet may be targeted to prevent depression. 42 The relationship between physical activity and depression is well-established in the general adult population,24,43,44 with both public health organizations and practitioners recommending adequate physical activity to improve mood and prevent depression.45,46 However, many Americans are not meeting the recommendations for physical activity, 47 with evidence suggesting physical inactivity is highest among emerging adults.48-50 Beyond just physical inactivity, sedentary behavior, typically defined as sitting or other activities that expend ≤1.5 metabolic equivalents of energy, has also been associated with depression.51,52 Unfortunately, research reports an increase in sedentary behavior among emerging adults, likely related to school, work, as well as the high rates of social media usage and other sitting activities, like video games.53,54 Regarding sleep, emerging adults often neglect sleep for competing priorities related to work, school, and social activities. Both poor sleep duration and quality have been reported in emerging adults and are associated with depression.28,29,55 In addition, lifestyles of emerging adults are often characterized by high rates of substance use, including tobacco/nicotine products and alcohol. 56 Substance use is often indicated as a risk factor for depression and is associated with poor mental health outcomes in emerging adults.32-35 Overall, the unhealthy lifestyle behaviors prevalent among emerging adults may increase their risk of depression. Therefore, research should explore how modifying lifestyle behaviors can reduce risk of depression in emerging adults.
The connections between these unhealthy lifestyle behaviors and depression are well-established.27,29,30,37,51 However, independent associations may not show the full picture as lifestyle behaviors co-occur and are often synergistic with one another. 57 Research exploring the combined effects of lifestyle behaviors (i.e., lifestyle patterns) suggests that the effect of multiple lifestyle behaviors together may be more impactful than targeting an individual behavior alone.58,59 For instance, the synergistic effect of multiple behaviors was reported to elevate physiological burden in middle-aged adults. 58 Additionally, specific to depression, a combined healthy lifestyle (3 or more behaviors) was associated with reduced risk of depression in the general adult population. 59 Observational studies have found similar results in emerging adults outside the US, with unhealthy lifestyle patterns associated with increased risk of depression.60-63 To date, most of this research has been conducted in populations other than emerging adults in the US.57-63 Thus, whether this relationship holds true for emerging adults remains unclear. Given the high prevalence of unhealthy lifestyle behaviors among US emerging adults,27-29,38,39,48-50,53,54,56 and their relationship with depression,32-35,42,44-46,51,52,64 research should explore the combined impact of an unhealthy lifestyle on depression in emerging adults to identify prevention and treatment targets.
Few studies have explored the relationship between combined lifestyle behaviors and depression in emerging adults in the US,65-67 despite high rates of mental illness and unhealthy lifestyle behaviors in this population.5,7,33,36,42-44,51 Moreover, no studies to date have included the inflammatory potential of the diet in their assessment of combined lifestyle behaviors in emerging adults. As diet can directly influence inflammation in the body and this inflammatory response plays a role in the pathophysiology of depression, the inflammatory potential of the diet is an important aspect of lifestyle to investigate. 68 Furthermore, sleep quality, substance use (e.g., smoking and drinking), and sedentary behavior are important lifestyle behaviors for emerging adults that are less studied in this context and may also influence inflammation in the body.69-72 An investigation into the lifestyle patterns of emerging adults in the US should consider both well-established and more emerging lifestyle behaviors associated with depression including, a pro-inflammatory diet, poor sleep duration and quality, physical inactivity and sedentary behavior, tobacco/nicotine use, and alcohol consumption.
The lifestyle patterns of US emerging adults and the relationship between lifestyle patterns and depression have yet to be established. In order to develop more effective and targeted interventions for emerging adults in the US, the lifestyle patterns of this population must be understood, including how they are associated with depression. The present study aims to address this gap by utilizing nationally representative data from the US National Health and Nutrition Examination Survey (NHANES) to identify the lifestyle patterns of male and female emerging adults in the US and explore the relationship between lifestyle patterns and depression in this population.
Methods
Study Design & Sampling
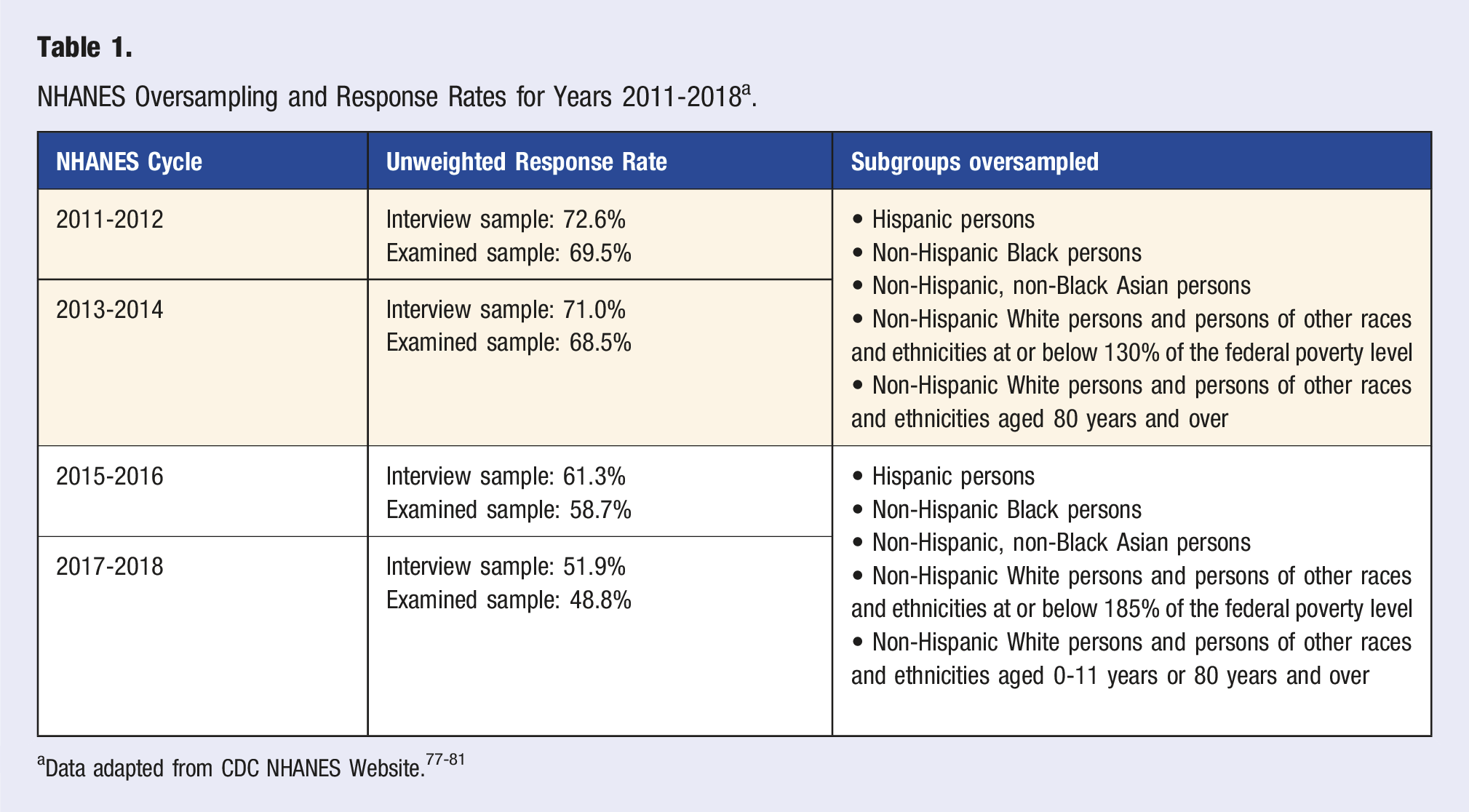
This secondary data analysis included participants from NHANES, a nationally representative survey that assesses the health outcomes of adults and children in the US conducted in 2-year cycles since 1999. 73 Emerging adults (between the ages of 18-25 years) with complete physical activity, sleep, depression, substance use, and dietary data were included in the analysis. NHANES is administered by the Centers for Disease Control and Prevention (CDC) and the National Center for Health Statistics (NCHS). 73 The sample for each NHANES cycle is obtained through a multi-stage design to ensure the sample is representative of the non-institutionalized civilian population in the US.74,75 The four-stage sampling design includes (1) primary sampling units (PSUs), which are typically US counties sampled from all 50 states, (2) census blocks within the PSUs, (3) households within census blocks, and (4) individuals in those households.74,75 Within this design, some subgroups, including individuals of specific races, ethnicities, income levels, and ages, are oversampled to ensure reliability of measures within subgroups.74,75 Oversampling can differ from cycle to cycle.74,75
NHANES Oversampling and Response Rates for Years 2011-2018 a .
Participants
Of the total participants from NHANES cycles 2011-2018, 3489 were between the ages of 18 and 25. Of the 3,489, 421 were excluded due to missing depression data, 8 were excluded due to missing physical activity data, 1 was excluded due to missing sleep data, 577 were excluded due to missing dietary data, and 463 were excluded due to missing alcohol or smoking data. A total of 2,019 participants met inclusion criteria and were included in the analysis. A complete flow diagram of study screening and selection can be seen in Figure 1. Flow diagram of participant screening and selection.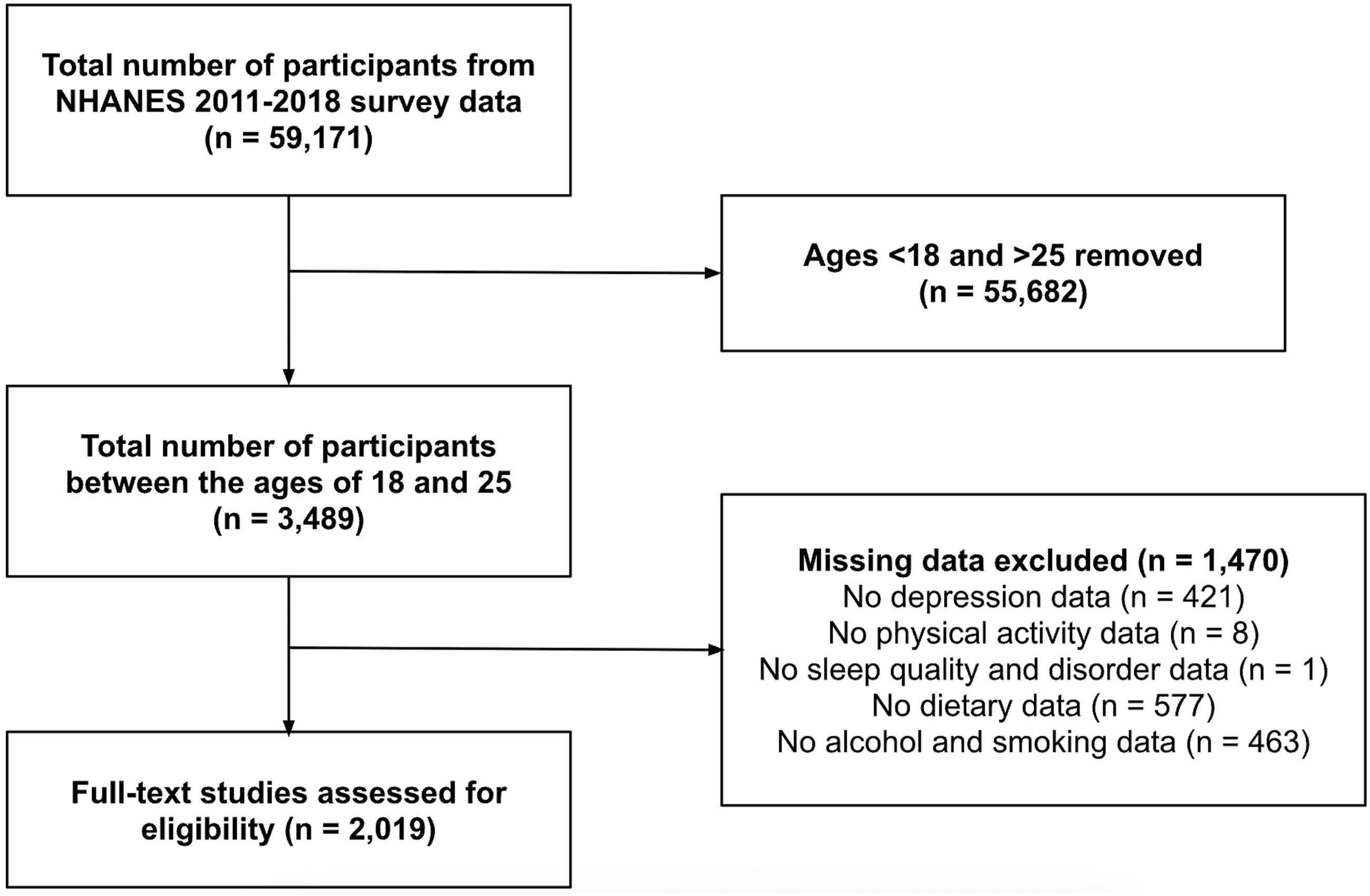
Measures
NHANES utilizes questionnaires and 24-hour dietary recalls to collect lifestyle behavior data. In this study, seven lifestyle variables were assessed: diet, sleep duration, sleep quality, physical activity, sedentary behavior, and substance use including alcohol consumption and smoking history. 82 Lifestyle behavior data were scored and dichotomized as either meeting recommendations for these behaviors or not. Individuals who met the recommendations for diet, sleep, physical activity, sedentary behavior, and substance use were considered “healthy,” while individuals who did not meet the guidelines were considered “unhealthy.” Scoring for each lifestyle behavior was based on previous literature and is described below. 35
Diet
The inflammatory potential of the diet was assessed using the Dietary Inflammatory Index (DII). 83 The DII uses up to 45 food parameters, which consist of whole foods, nutrients, and spices, to calculate an overall dietary inflammatory score. 83 This study utilized 28 dietary parameters available from NHANES 24-hour recall data to calculate the DII. As two days of dietary recall data were available, day 1 and day 2 totals were averaged. The DII instrument scores can range from −8.87 to 7.98, with higher (positive) scores indicating a pro-inflammatory diet. 83 Positive scores (≥0) were defined as “pro-inflammatory diet” and negative scores (<0) were defined as “anti-inflammatory diet.” 83
Sleep Duration & Quality
Sleep duration was assessed using responses to the question “How much sleep do you get (hours)?”. As recommended by the National Sleep Foundation, healthy sleep duration for 18-25 year olds is 7-9 hours. 84 Poor sleep was defined as individuals sleeping <7 hours or >9 hours and adequate sleep was defined as individuals sleeping 7-9 hours. 84 Sleep quality was measured using responses to the question “Have you ever told a doctor you had trouble sleeping?”. “Trouble sleeping” was defined as individuals who answered “yes,” while “no trouble sleeping” was defined as individuals who answered “no.”
Physical Activity & Sedentary Behavior
Physical activity and sedentary behavior were assessed using the NHANES Physical Activity Questionnaire, which is based on the Global Physical Activity Questionnaire. Physical activity and sedentary behavior are distinct behaviors that influence the amount of energy being expended throughout the day. 85 Physical activity includes body movements that expend energy above your resting metabolic rate, including activities of daily living (i.e., work-related physical activity) and programed physical activity (i.e., walking, biking, running). 85 In contrast, sedentary behavior includes waking behaviors with very low energy expenditure (i.e., sitting, reclining, lying down). 85
Total moderate and vigorous activity from work, leisure, and recreation were scored to determine metabolic equivalents (METs). An individual met the Physical Activity Guidelines for Americans if their total METs was ≥ 600. 45 METs of 600 includes at least 150 minutes to 300 minutes a week of moderate-intensity or 75 minutes to 150 minutes a week of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous-intensity aerobic activity. 45 Individuals who did not meet these recommendations (METs <600) were scored as “physically inactive,” while individuals who did meet these recommendations (METs ≥600) were scored as “physically active.” 45
The World Health Organization’s Guidelines on Physical Activity and Sedentary Behavior identify sedentary behavior of greater than 7.5 hours as a risky or unhealthy behavior. 46 Individuals who reported >7.5 hours were defined as “sedentary” and individuals who reported <7.5 hours were defined as “non-sedentary.” 46
Substance Use
Individuals reported the number of alcoholic drinks they typically consumed on days they drank alcohol within the past year. Alcohol consumption was scored based on the Dietary Guidelines for Americans. 86 Individuals were defined as “drinkers” if females reported consuming >1 drink per day and males reported consuming >2 drinks/day. 86 All others were defined as “nondrinkers.” Smoking history was assessed through one item, which inquires if an individual smoked at least 100 cigarettes in their life, a cut point suggested by the World Health Organization. 87 Individuals who answered “yes” were defined as “smokers” and individuals who answered “no” were defined as “nonsmokers.”
Depression
Symptoms of depression were assessed using the Patient Health Questionnaire (PHQ-9). The PHQ-9 contains 9 items that assess symptoms of depression with 4 possible responses based on symptom frequency. 88 This assessment tool identifies an overall depression symptom score by totaling responses, with each score describing a severity category: minimal (score of 0-4), mild (score of 5-9), moderate (score of 10-14), moderately severe (score of 15-19), and severe depression (score of 20-27). 88 As is consistent with previous literature, moderate, moderately severe, and severe were defined as “with depression symptoms” and minimal and mild as “without depression symptoms.” 67
Sociodemographic Variables
Sociodemographic data collected included age, race/ethnicity, education level, family income, employment status, sex, marital status, and body mass index (BMI). Age, race/ethnicity, education level, family income, and employment status were included due to potential confounding effects.89-91 Other sociodemographic variables, such as sex, marital status, and BMI, described the study sample. Race/ethnicity comprised four categories: Non-Hispanic White, Non-Hispanic Black, Hispanic, and Other Race (including multi-racial). Education level consisted of four categories: less than high school, high school graduate/GED or equivalent, some college or AA degree, and college graduate or above. Family income was reported using the ratio of family income to poverty guidelines. Poverty income ratio (PIR) is calculated by dividing total household income by the federal poverty level for their household size. 92 Individuals with a PIR of ≥1 were defined as higher income and individuals with a PIR of <1 were defined as lower income. 92 Employment status was summarized using a question that inquired about the “type of work done last week.” Employed was defined as “working at a job or business” or “with a job or business but not at work,” and unemployed was defined as “looking for work” or “not working at a job or business.” Marital status was dichotomized into “married” and “unmarried.” BMI was defined using existing cut points: BMI of 18.5-24.9 kg/m2 was considered healthy, BMI of <18.5 kg/m2 underweight, BMI of >24.9 kg/m2 or <29.9 kg/m2 overweight, and BMI ≥30 kg/m2 obese. 93
Statistical Analysis
Descriptive data were summarized using weighted means and standard errors or counts and weighted percentages. Sample weights in NHANES are needed to account for survey non-response, survey design (including oversampling), and post-stratification adjustments to ensure the sample is representative of the non-institutionalized civilian population in the US. 73 For all analyses, we used a combined 8-year sample weight (for years 2011-2018) using the formula wtdr2d/4, indicating that we used dietary 2-day sample weight (wtdr2d) and 4 cycles of NHANES for a total of 8 years. 94 Complete information about data collection can be found on the CDC’s website. 94
A latent class analysis (LCA) was conducted to identify lifestyle patterns for emerging adult males and females using seven lifestyle behaviors. To determine the optimal number of latent classes, we fit multiple models from 2 to 8 classes, taking sample weights and cluster features into account, and analyzing the fit statistics, including Akaike’s information criterion (AIC), Bayesian information criterion (BIC), adjusted Bayesian information criterion (aBIC), and entropy. Bootstrap likelihood ratio tests (BLRT) were also used to determine the optimal number of classes. Higher entropy and lower AIC, BIC, and aBIC indicated a better fit, while a significant BLRT P-value indicated that the subsequent class model was a better fit than the previous class model. The best fit was determined using these fit statistics as well as the interpretability and clinical significance of the resulting classes.
Once the optimal model was determined, we analyzed differences between classes using chi-squared tests for categorical variables and analysis of variance (ANOVA) for continuous variables. Multiple logistic regression was used to analyze how lifestyle patterns were associated with odds of depression by sex when controlling for age, race, education level, family income, and employment status. All analyses were conducted using SAS version 9.4 and P-values <0.05 were considered statistically significant.
Results
Sample Characteristics
Demographic Characteristics
Demographic & Lifestyle Characteristics Stratified by Sex.
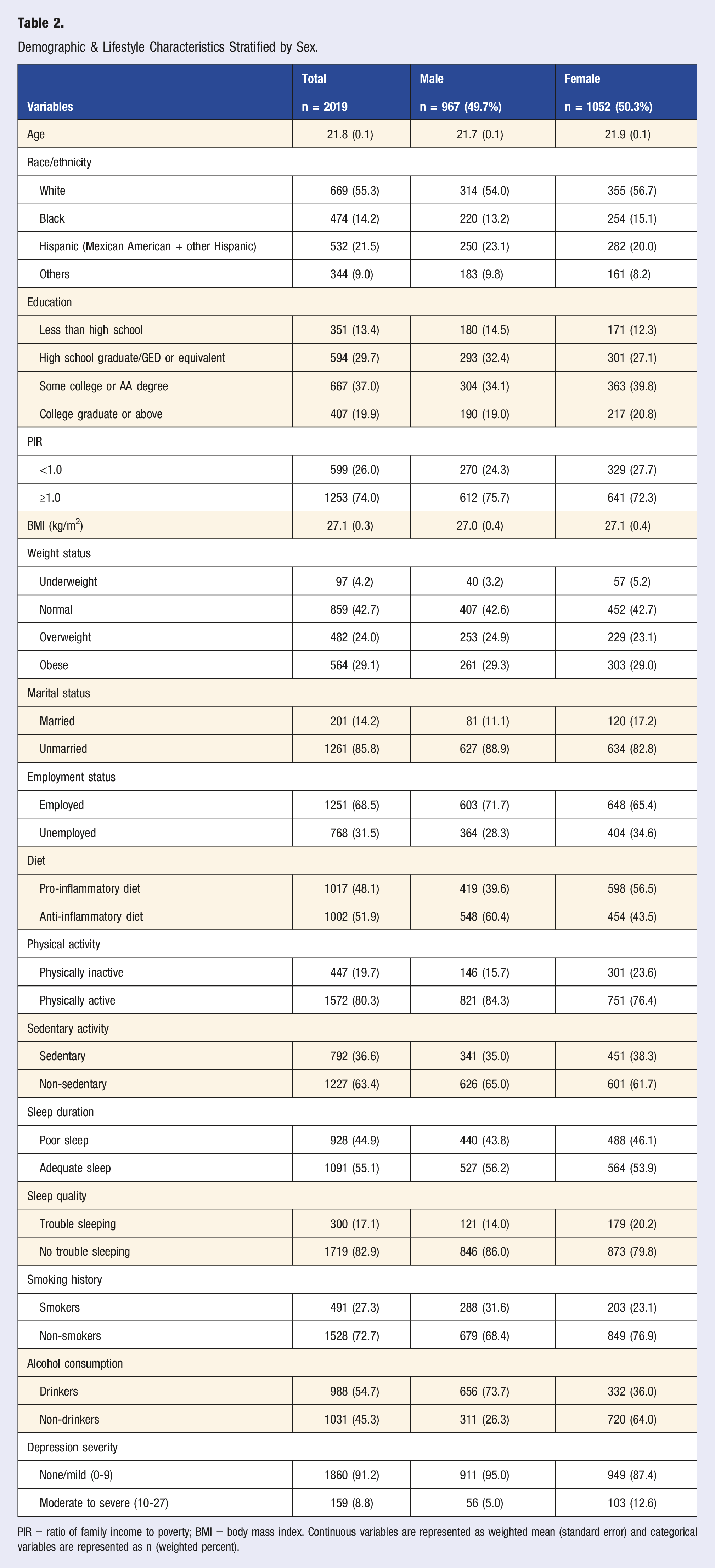
PIR = ratio of family income to poverty; BMI = body mass index. Continuous variables are represented as weighted mean (standard error) and categorical variables are represented as n (weighted percent).
Lifestyle Behaviors & Depression
For the total sample, the dietary inflammatory potential was evenly distributed, with 51.9% of the sample consuming an anti-inflammatory diet and 48.1% consuming a pro-inflammatory diet. A majority of the sample was physically active (80.3%) and non-sedentary (63.4%). A little more than half of the sample (55.1%) reported adequate sleep with only 17.1% reporting trouble sleeping. Over a quarter of the sample (27.3%) were smokers and more than half of the sample were drinkers (54.7%). Regarding depression, the average depression score was 3.3 ± 0.1 indicating minimal depression symptoms. When depression symptom severity was categorized, almost 9% of the sample had moderate to severe depression symptoms (8.8%). Complete lifestyle and depression information can be seen in Table 2.
Latent Class Analysis
Indicators of Fit for Models With Different Numbers of Latent Classes.
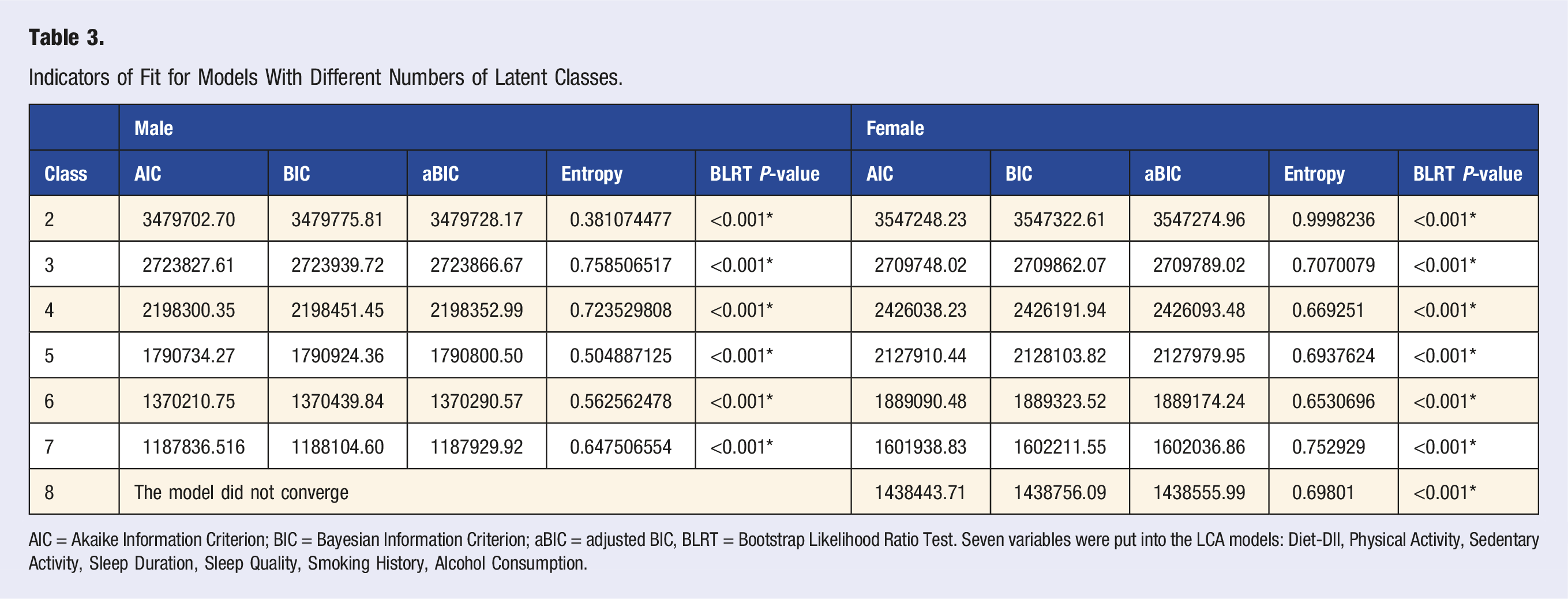
AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion; aBIC = adjusted BIC, BLRT = Bootstrap Likelihood Ratio Test. Seven variables were put into the LCA models: Diet-DII, Physical Activity, Sedentary Activity, Sleep Duration, Sleep Quality, Smoking History, Alcohol Consumption.
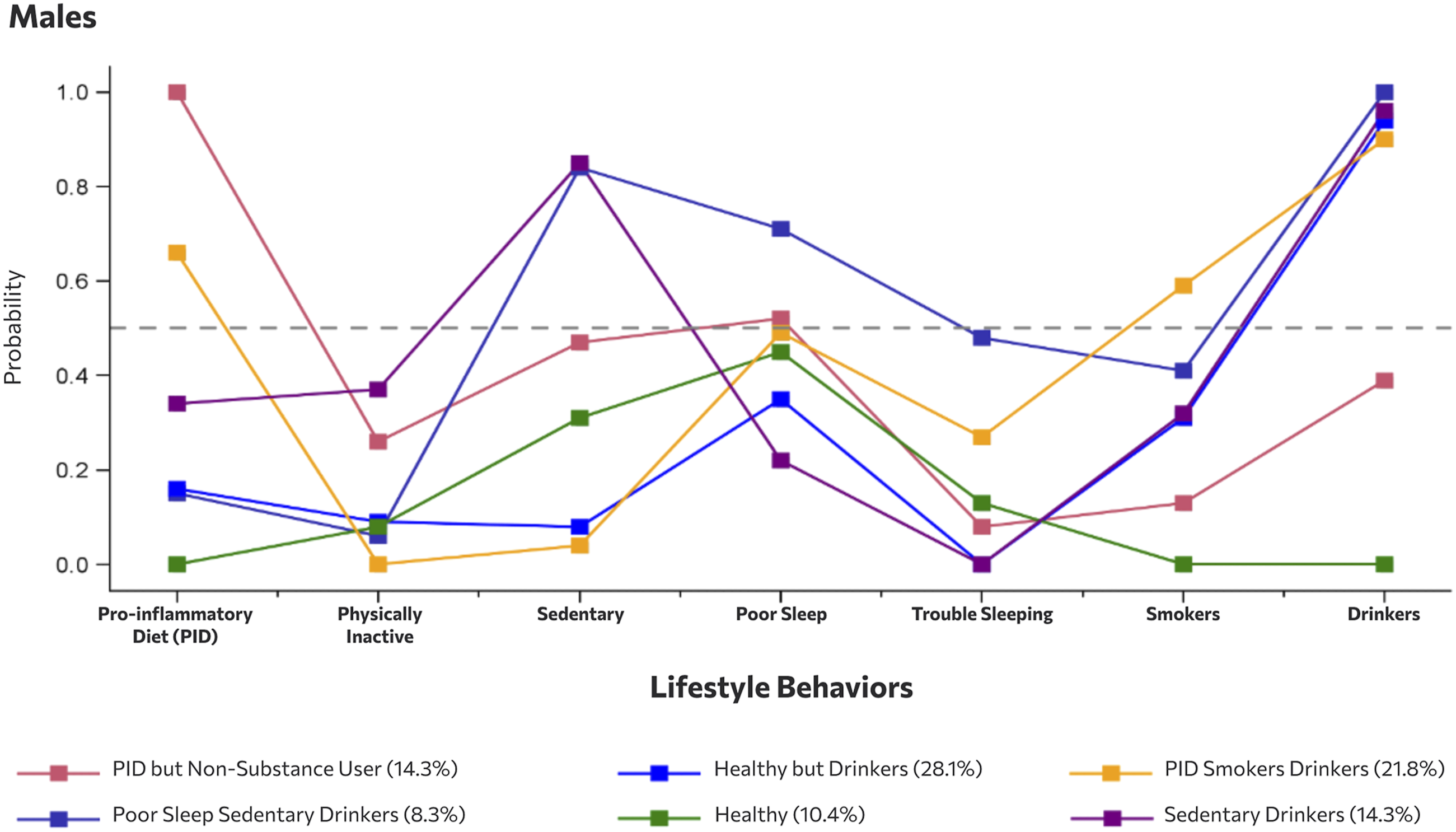
Conditional probability of lifestyle behaviors across latent class groups among male emerging adults.
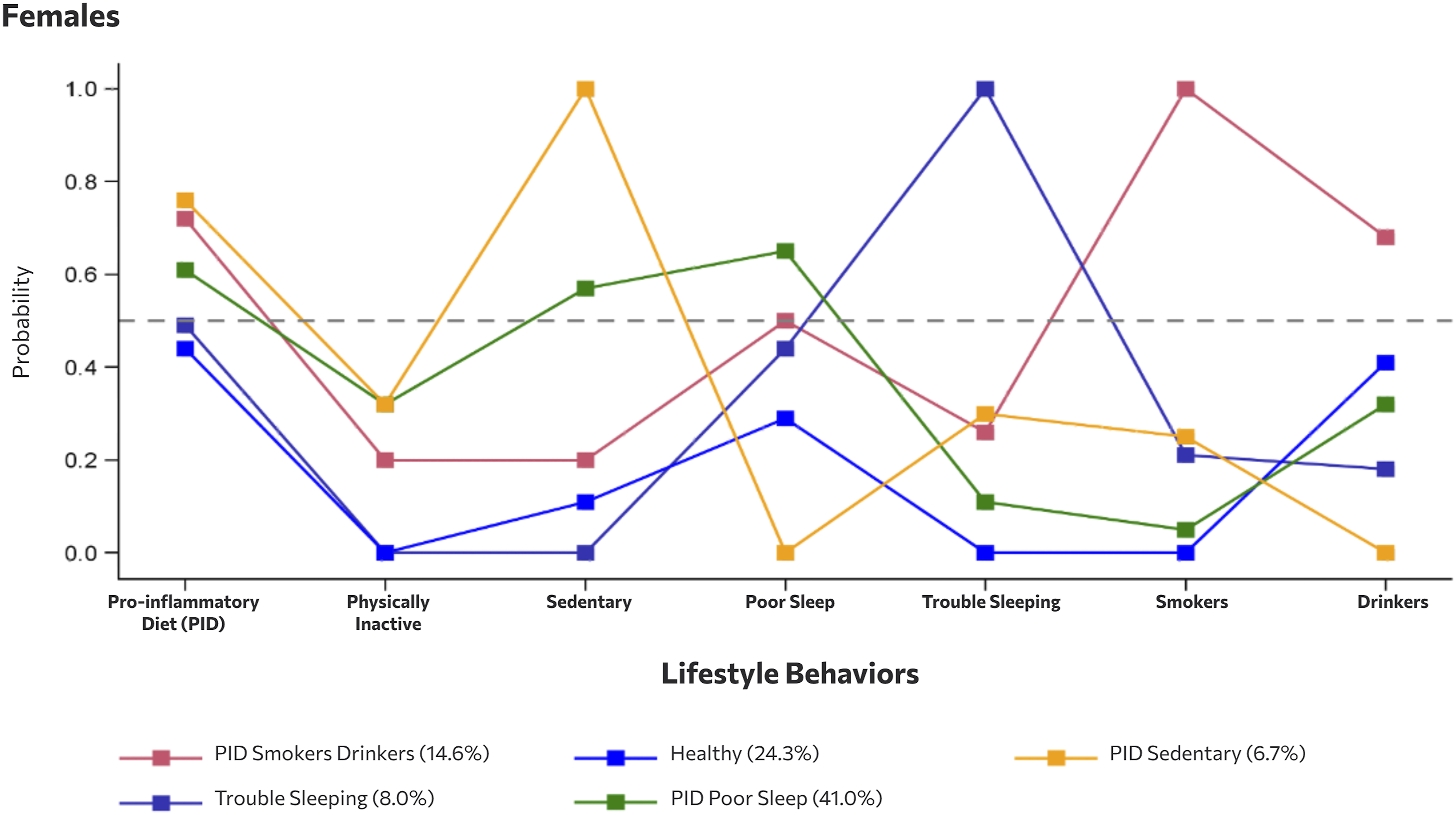
Conditional probability of lifestyle behaviors across latent class groups among female emerging adults.
Lifestyle Behaviors & Demographic Characteristics Across Latent Classes Among Males
For males, Class 1 was labeled as Pro-inflammatory Diet (PID) but Non-Substance User. This group had high probabilities of following a pro-inflammatory diet (100%). PID but Non-Substance User also had moderate probabilities of physical inactivity (33.8%), sedentariness (51.6%), and poor sleep (58.8%), but had lower probabilities of using substances like alcohol (24.1% drinkers) and tobacco/nicotine (6.6% smokers). PID but Non-Substance User were slightly younger than the other classes (mean age 20.8 ± 0.2 years), had a higher proportion of Black (23.1%) and Hispanic (26.1%) individuals, and had the highest obesity among the male classes (39.9%).
Class 2 among males was labeled Poor Sleep Sedentary Drinkers. These individuals had high probabilities of engaging in unhealthy behaviors including sedentary behavior (99.7%), poor sleep (85.9%), trouble sleeping (48.5%), smoking (40.7%) and drinking (100%). However, these individuals had high probabilities of engaging in physical activity (98.1%) and following an anti-inflammatory diet (89.0%). Poor Sleep Sedentary Drinkers were mostly White (63.1%) and had the highest percentage of individuals who graduated college (36.9%), had a PIR greater than or equal to 1.0 (85.8%), and were employed (85.1%).
Males grouped into Class 3 were labeled Healthy but Drinkers. These males had high probabilities of engaging in healthy behaviors, including an anti-inflammatory diet (99.5%), physical activity (90.7%), non-sedentary behavior (100%), adequate sleep (63.0%), no trouble sleeping (100%), and not smoking (62.1%) but were also drinkers (98.1%). Healthy but Drinkers were mostly White (54.7%) and Hispanic (29.0%) and completed high school/GED (36.9%) and some college (40.0%).
Class 4 was considered the Healthy group among males. Males grouped into the Healthy group had high probabilities of engaging in healthy behaviors, including an anti-inflammatory diet (100%), physical activity (94.6%), non-sedentary (72.4%), adequate sleep (56.1%), no trouble sleeping (87.4%), non-smokers (100%), and non-drinkers (100%). Healthy males were mostly White (47.2%), less educated (41.7% high school/GED), employed (70.9%) and had a high percentage (80.4%) of those with a PIR ≥1.0. The Healthy group also had the highest percentage of males who were married (16.3%).
The fifth class for males was labeled PID Smokers Drinkers. Individuals in this group had high probabilities of engaging in physical activity (100%) and non-sedentariness (100%) but also had high probabilities of engaging in unhealthy behaviors, such as pro-inflammatory diet (88.8%), poor sleep (48.0%), trouble sleeping (26.8%), smoking (51.9%), and drinking (91.8%). These males were mostly White (53.2%), had a higher percentage of individuals with a PIR <1.0 (28.1%), and had a high proportion of obesity (32.5%).
Demographic & Lifestyle Characteristics Stratified by Class Among Male Emerging Adults.
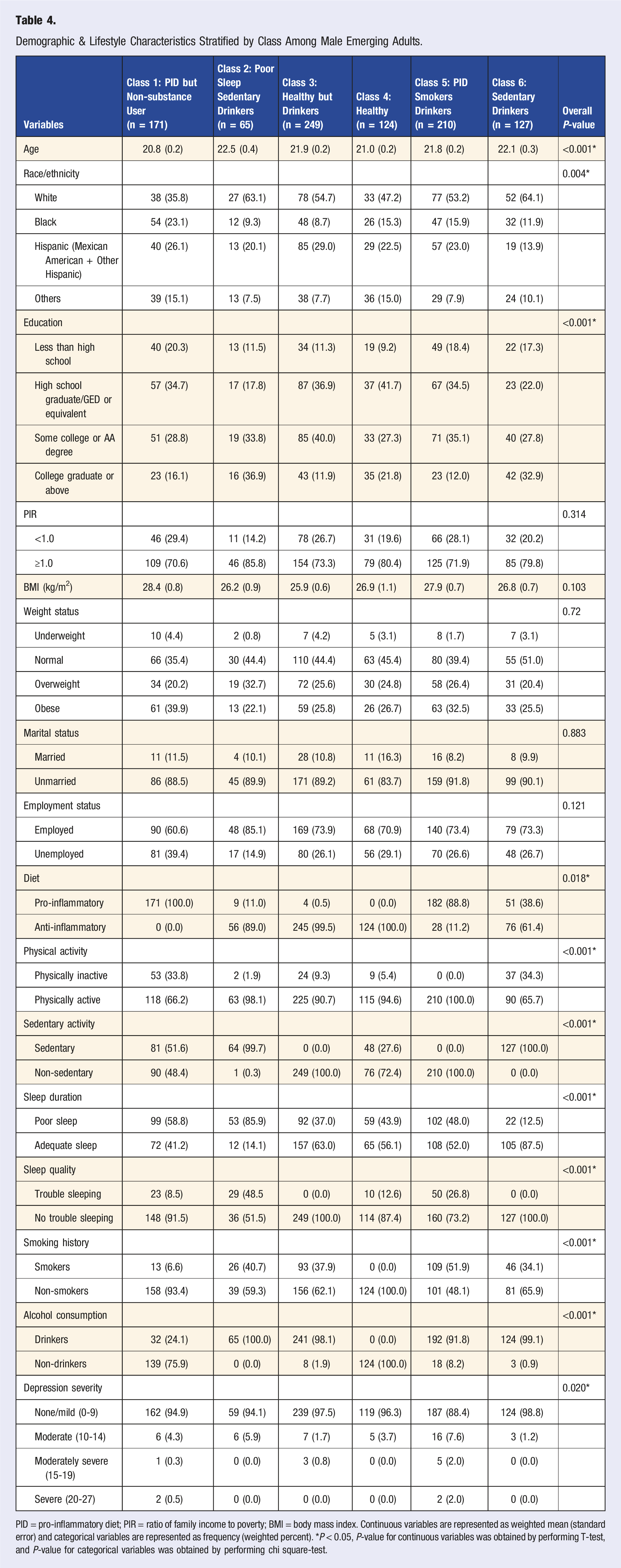
PID = pro-inflammatory diet; PIR = ratio of family income to poverty; BMI = body mass index. Continuous variables are represented as weighted mean (standard error) and categorical variables are represented as frequency (weighted percent). *P < 0.05, P-value for continuous variables was obtained by performing T-test, and P-value for categorical variables was obtained by performing chi square-test.
Lifestyle Behaviors & Demographic Characteristics Across Latent Classes Among Females
For females, Class 1 was labeled PID Smokers Drinkers. Individuals in this group had high probabilities of engaging in unhealthy behaviors, such as pro-inflammatory diet (73.1%), poor sleep (53.9%), trouble sleeping (21.3%), smoking (100%), and drinking (73.1%) but also had high probabilities of engaging in healthy behaviors, such as physical activity (81.5%) and non-sedentariness (80.7%). These females were mostly White (64.3%) and had the lowest percentage of Black individuals (8.9%). The PID Smokers Drinkers female group were also less educated (19.9% less than HS), and had a low PIR (33.6% PIR <1.0), high proportion of overweight (29.1%) and obesity (33.4%), and the highest proportion of unemployment (36.5%).
Females in Class 2 were labeled Trouble Sleeping. These females had the highest probability of trouble sleeping (100%) but also had high probabilities of engaging in healthy behaviors, including high physical activity (100%), non-sedentariness (100%), adequate sleep (50.7%), non-smoking (75.0%), non-drinking (84.0%). Females in this group also had a higher probability of following a pro-inflammatory diet (53.5%). The Trouble Sleeping group was mostly White (72.2%) females, who were educated (51.8% some college), with a high proportion of individuals with a PIR ≥1.0 (77.5%), and the lowest proportion of individuals with obesity among the female classes (23.2%).
Females grouped into Class 3 were considered the Healthy group. These individuals had the highest probability of engaging in healthy behaviors among females with the exception of drinking. The Healthy group had the highest probability of following an anti-inflammatory diet (64.7%), engaging in physical activity (100%), non-sedentariness (100%), adequate sleep (76.0%), no trouble sleeping (100%), non-smoking (100%), but some drinking (39.7%). This group was mostly White (54.2%) but had a high proportion of Hispanic females (23.2%) compared to the other classes. The Healthy female group were also highly educated (42.9% some college; 23.5% college graduate or above) and had a low proportion of individuals with obesity (27.9%).
Class 4 consisted of females who were labeled as PID Poor Sleep. These females had high probabilities of engaging in unhealthy behaviors including a pro-inflammatory diet (66.8%), inactivity (33.4%), sedentariness (71%), drinking (30.2%), and had the highest probability of poor sleep (63.5%) among the female classes. Interestingly, these individuals had low probabilities of reporting trouble sleeping (5.9%) and smoking (0.3%). The PID Poor Sleep group had the highest proportion of Black (19.8%) and Hispanic (23.2%) females among the female classes, were highly educated (26% completed college or above), had low obesity (27.6%), a high proportion of unmarried females (85.9%), and moderate proportion of employment (66.2%).
Demographic & Lifestyle Characteristics Stratified by Class Among Female Emerging Adults.
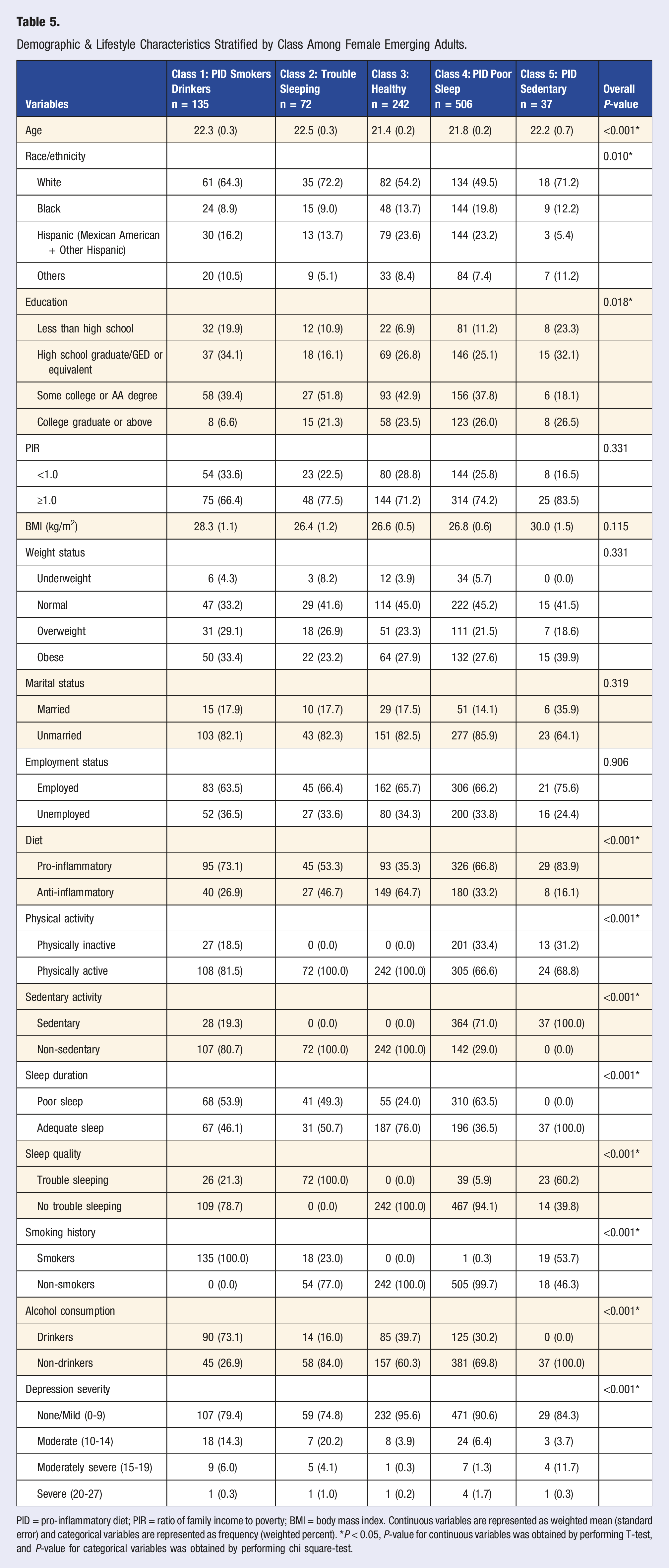
PID = pro-inflammatory diet; PIR = ratio of family income to poverty; BMI = body mass index. Continuous variables are represented as weighted mean (standard error) and categorical variables are represented as frequency (weighted percent). *P < 0.05, P-value for continuous variables was obtained by performing T-test, and P-value for categorical variables was obtained by performing chi square-test.
Associations of Lifestyle Groups With Depression
The Association Between Class and Depression Among Emerging Adults.
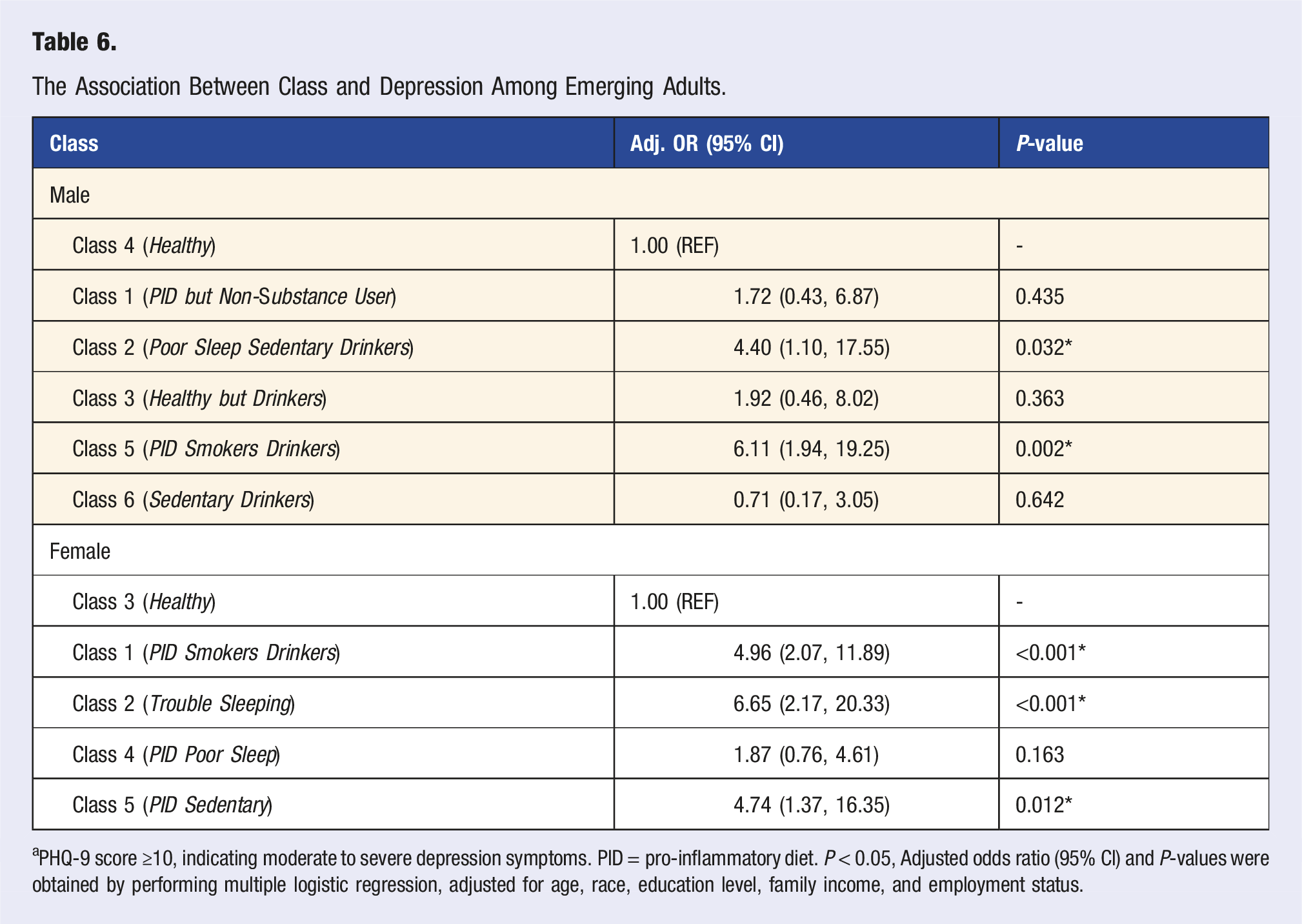
aPHQ-9 score ≥10, indicating moderate to severe depression symptoms. PID = pro-inflammatory diet. P < 0.05, Adjusted odds ratio (95% CI) and P-values were obtained by performing multiple logistic regression, adjusted for age, race, education level, family income, and employment status.
For females, when compared to the Healthy reference group, those in the PID Smokers Drinkers, Trouble Sleeping, and PID Sedentary groups had significantly increased odds of having more severe depression symptoms. Females in the PID Smokers Drinkers group had almost 5 times the odds of having more severe depression symptoms (aOR [95% CI]: 4.96 [2.07, 11.89], P < 0.001), while females in the Trouble Sleeping group had more than 6 times the odds of having more severe depression symptoms (aOR [95% CI]: 6.65 [2.17, 20.33], P < 0.001) compared to the Healthy reference group. The PID Sedentary group had over 4 times the odds of having more severe depression symptoms (aOR [95% CI]: 4.74 [1.37, 16.35], P = 0.012), compared to the Healthy reference group.
Discussion
To our knowledge, this is the first study to explore the relationship between lifestyle patterns of emerging adults in the US, including the inflammatory potential of the diet, sleep quality as well as physical activity and sedentary time, sleep duration, smoking history, and alcohol consumption. We identified multiple high-risk behaviors in our sample of emerging adults, including 48.1% following a pro-inflammatory diet, 36.6% with >7.5 hours of sedentary time, 44.9% with <7 or >9 hours of sleep per day, and 54.7% drinking past the recommended limit for alcohol intake. Our findings indicate clustering of lifestyle behaviors among emerging adults in the US and we successfully identified unique lifestyle patterns for males and females. These patterns included, PID but Non-Substance User, Poor Sleep Sedentary Drinkers, Healthy but Drinkers, Healthy, PID Smokers Drinkers, and Sedentary Drinkers for males, and PID Smokers Drinkers, Trouble Sleeping, Healthy, PID Poor Sleep, and PID Sedentary for females. Compared to their corresponding Healthy reference group, males in the Poor Sleep Sedentary Drinkers and PID Smokers Drinkers groups and females in the PID Smokers Drinkers, Trouble Sleeping, and PID Sedentary groups had increased odds of more severe depression symptoms. These results emphasize the need to promote a healthy lifestyle and comprehensively target these behaviors for the prevention and treatment of depression in emerging adults.
Given the high prevalence of depression in US emerging adults, effective, low-risk strategies should be identified. Our study not only supported the idea that lifestyle behaviors cluster together in US emerging adults, but also highlighted possible intervention targets in the form of comprehensive lifestyle behaviors. We observed clustering of lifestyle behaviors and identified six lifestyle patterns for males and five lifestyle patterns for females. Clustering of lifestyle behaviors has been seen in adolescents, older adults, and now emerging adult populations.62,63,97-99 While research typically studies lifestyle behaviors in isolation, an individual’s lifestyle is made up of multiple behaviors that co-occur and often have a synergistic relationship with one another. 57 Unhealthy lifestyle behaviors tend to cluster together and are associated with poor mental health outcomes, including increased risk of depression.35,60,67,99,100 Studies that utilize clustering techniques, like LCA, help us better understand how specific lifestyle behaviors that cluster or co-occur can create a combined effect on depression risk that is greater than the effect of the individual behaviors. Typically the group with the highest rates of unhealthy behaviors67,99,100 or highest number of unhealthy behaviors35,60 is associated with increased odds of mental health problems. Our study adds to this body of research that emphasizes the need for future studies to explore how these behaviors co-occur and how they relate to risk of mental illness.
Clustering of behaviors may vary for populations of different ages and geographic origins and depending on which lifestyle variables are being studied. Previous studies in emerging adults have typically identified three to five lifestyle patterns, while our study identified five lifestyle patterns for males and six lifestyle patterns for females.25,62,63,65-67,99 Our study was the first study to explore this clustering phenomenon in US emerging adults, stratified by sex using seven lifestyle variables, and as a result, we were able to present unique sex differences in lifestyle patterns and how they relate to risk of depression. Our study identified only one overlapping lifestyle pattern for males and females, PID Smokers Drinkers. Previous studies that have stratified lifestyle patterns by sex found three to five overlapping patterns for males and females.63,65 Grant et al. conducted a LCA in US emerging adults using three lifestyle variables: fruit and vegetable intake, physical activity, and alcohol consumption and identified five common classes for both sexes. 65 The inclusion of an overall measure of diet quality beyond fruit and vegetable intake plus the addition of sedentary time, sleep quality, and smoking history, may have resulted in more distinct patterns between sexes in our study. Sex and gender related differences in lifestyle behaviors have previously been reported in emerging adults.101-103 Distinct approaches to diet, sleep, exercise, drinking, and smoking have been observed, with research suggesting that sex and gender related biological and psychosocial factors may influence lifestyle behaviors.101-103 Future research should further explore these differences to develop more informed and targeted lifestyle interventions.
Our findings presented multiple lifestyle patterns associated with an increased risk of depression. Looking at these patterns overall, high-risk lifestyles were typically characterized by high rates of substance use, following a pro-inflammatory diet, and/or poor sleep duration or quality. These behaviors may contribute to depression through various mechanisms, such as inflammation.71,104 Both excessive alcohol intake and smoking have been shown to increase inflammatory biomarkers, including C-reactive protein and interleukin-6.71,104 Use of these substances can also lead to highs and subsequent lows or “crashes” in mood, which may contribute to worsening depression symptoms overall. Excessive alcohol intake may also lead to social consequences, like poor job or academic performance, strained relationships, and isolation that can lead to depressed mood. 105 Regarding diet, dietary intake can contribute to inflammation through the gut-microbiome and the production of inflammatory cytokines. 106 A pro-inflammatory diet is also often devoid of nutrients and high in “empty calories,” which may not provide adequate nutrition required for proper mood stabilization. 107 Similarly, when individuals experience poor sleep quality, they are more likely to experience issues with neurological functioning and emotional regulation, which can lead to depressed mood.108,109
Consistent with previous studies in emerging adults, this study found that lifestyle patterns with high rates of substance use were associated with increased risk of mental illness.61-63,65,66 However, most of these studies identified patterns with high rates of substance use and inadequate PA or high sedentary behavior.61-63 Interestingly, our study found that among the high-risk patterns, physically activity, specifically meeting the Physical Activity Guidelines for Americans, was not enough to protect individuals from risk of depression when other unhealthy lifestyle behaviors were present. For instance, Poor Sleep Sedentary Drinkers, had high rates of alcohol use and sedentary behavior and also high rates of PA. Similarly, Peterson et al and Dong et al discussed how emerging adults can simultaneously be physically active and sedentary.54,63 The impact of sedentary behavior separate from physical activity has been previously emphasized, with the Physical Activity Guidelines for Americans including recommendations specific to sedentary behavior starting with the 2nd edition in 2018. 45 Overall, a strong link is present between substance use and depression symptoms in the literature but more research is needed to explore how substance use co-occurs with other unhealthy lifestyle behaviors in emerging adulthood.
We identified a unique class among females, Trouble Sleeping, characterized by high probability of reporting poor sleep quality to a doctor. While behaviors like diet and physical activity are commonly studied included in lifestyle pattern research, sleep quality has more recent evidence highlighting its role as a risky health behavior within a lifestyle.109,110 In relation to mental illness, few studies have included sleep in their analysis of lifestyle patterns and depression in emerging adults60,62,67,99,111 with only two studies including sleep quality60,111 and one including both sleep quantity and sleep quality. 111 Using hierarchical regression analysis, Wickham et al. identified both sleep quality and sleep quantity as the strongest predictors of depression symptoms in their sample of emerging adults, which aligns with our findings. 111 However, Wickham et al. did not stratify by sex and we only found this relationship to be true among females. 111 Interestingly, both sleep disturbances and depression have been reported as more common among emerging adult females, suggesting a need to screen and target sleep disturbances among females. 55 Given the relationship between sleep and depression as well as its potential as a high-risk modifiable lifestyle behavior, future studies should consider both sleep quality and sleep quantity when assessing overall lifestyle.
External factors would also have an impact on both lifestyle behaviors and depression in emerging adults. This population faces various social, financial, and academic pressures in the form of increased use of social media, rising student loan burdens, and high achievement culture.9,10,112,113 These external factors may contribute to depression and may also lead to high-risk behaviors. We identified high-risk lifestyle patterns that include high rates of substance use, sedentary behavior, inflammatory dietary intake, and troubled/poor sleep. Pressure to succeed at both school and work as well as financial burden of student loans may lead to increased stress that causes emerging adults to turn to substances or junk foods as a coping mechanism. These pressures may also result in sleep disturbances. Furthermore, the proliferation of social media in addition to working or studying for long hours can lead to increased sedentary behaviors even if these individuals are meeting physical activity requirements. Use of social media, student loan burden, and high achievement culture have continued to increase in recent years, as have global factors, including the COVID-19 pandemic, cultural and political polarization, and increased awareness of global threats.113-115 In addition to modifiable lifestyle behaviors, future studies should aim to consider these external factors as possible confounding variables when exploring the relationship between lifestyle behaviors and mental illness in emerging adults.
This study was the first to explore the relationship between lifestyle patterns and depression in emerging adults assessing diet using the DII. Previous studies have used other dietary patterns, like the Healthy Eating Index (HEI) 67 or Dietary Approaches to Stop Hypertension (DASH) 61 dietary pattern, or specific components of diet, like fruit and vegetable intake or breakfast intake.62,63,99 These high-risk eating patterns or behaviors were not typically associated with depression in previous research.61-63,67,99 In contrast, we identified two high-risk classes among females (PID Smokers Drinkers, PID Sedentary) and one high-risk class among males (PID Smokers Drinkers) characterized in part by high probabilities of pro-inflammatory dietary patterns. The inflammatory potential of the diet was high in our sample of emerging adults, with almost half (48.1%) following a pro-inflammatory dietary pattern. High rates of dietary inflammation are likely related to increased intake of fast foods and processed foods in this population, which are higher in added sugars, saturated fats, and sodium. 116 Assessing dietary inflammation in emerging adults provides unique insights into the role that diet plays as part of an overall lifestyle. Future research should continue to assess dietary inflammation given its strong association with depression.40,41,68,117
Limitations
While this study provides unique insights into the relationship between lifestyle patterns and depression in emerging adults in the US, we must consider the study limitations. First, while NHANES is a rich, nationally representative dataset, it is also cross-sectional in nature and therefore we cannot determine the causality of this relationship. Nor can we ignore the bidirectional relationship between lifestyle and depression as we cannot rule out the possibility that depression leads to unhealthy lifestyle behaviors. Specifically, the clusters of lifestyle behaviors highlighted in this study (combinations of poor sleep quality, pro-inflammatory dietary pattern, and substance use) may all be coping mechanisms for depressed moods. Poor sleep quality may be a side effect of depression, as it is listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM) as one criteria for major depressive disorder. 118 Individuals who are depressed may crave junk foods or comfort foods that are high in saturated fats, added sugars, or other inflammatory components as a way to self-soothe. 119 In addition, substances like alcohol and tobacco or nicotine products are often used as coping mechanisms by individuals experiencing depression.34,105,120 Second, the lifestyle behavior data collected in NHANES are self-reported and thus we cannot rule out the possibility of self-report bias. Third, while LCA is considered a robust and statistically sound technique for analyzing patterns among a population, it is not without limitations. One such limitation is the potential loss of information in recoding continuous variables into binomial or categorical variables. 95 Finally, while this study included the largest number of lifestyle variables among studies exploring lifestyle patterns among emerging adults (seven variables), other important lifestyle behaviors and external factors were not included as they were not measured in NHANES. Lifestyle psychiatry highlights social connection, mindfulness and meditation, and mind-body activities, which were not included in the present study. In addition, external factors influence the mental wellbeing of emerging adults, including not only financial, social, and academic pressures but also a changing geopolitical landscape. Future studies should aim to consider these additional lifestyle behaviors and external factors in their analysis.
Implications and Future Directions
The present study highlighted multiple lifestyle patterns among emerging adults in the US associated with increased risk for depression. These lifestyle patterns, Poor Sleep Sedentary Drinkers and PID Smokers Drinkers for males and PID Smokers Drinkers, Trouble Sleeping, and PID Sedentary for females, not only provide insight into how unhealthy lifestyle behaviors cluster together but also provide direction for future lifestyle interventions. Our findings indicate that lifestyle interventions in emerging adults in the US should target sleep quality and quantity, inflammatory potential of the diet, substance use (e.g., smoking and drinking), and sedentary behavior for the prevention or adjunctive treatment of depression. Furthermore, our findings suggest that interventions may need to be tailored for males and females, as lifestyle behaviors cluster differently between the sexes.
Conclusions
Emerging adulthood presents a unique opportunity for intervention as lifestyle is often just beginning to be developed during this period and these lifestyle behaviors may persist throughout adulthood. Using a nationally representative sample of US emerging adults, we successfully identified clusters of lifestyle behaviors and distinct lifestyle patterns associated with increased risk of depression. These findings support the hypothesis that clusters of unhealthy lifestyle behaviors (overall unhealthy lifestyle) increase risk of depression, thus, adopting a healthy lifestyle may be an effective prevention or treatment strategy to reduce risk of depression.
Footnotes
Ethical Considerations
This secondary data analysis included publicly available de-identified data from the National Health and Nutrition Examination Survey (NHANES). All NHANES survey protocols are reviewed and approved by the National Center for Health Statistics Ethics Review Board (ERB) to ensure the protection of all participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.