
Abstract
Depression is a global health concern, with various treatments available. In this study, participants (n = 430) were self-selected or medically referred to a residential lifestyle program at the Black Hills Health & Education Center (BHHEC), with a mean stay of 19 days. Individualized treatment plans included structured physical activity sessions, counseling sessions, and the provision of a vegan diet. Beck Depression Inventory-II, self-reported total exercise minutes, resistance exercise minutes, and sleep, along with the number of holistic treatments and counseling sessions, were evaluated. Paired samples t-tests indicated a significant decrease in depression scores over time (MT1 = 20.14, MT2 = 6.17, P < .001). Results from the multiple linear regression that evaluated total exercise minutes, resistance exercise, number of treatments and counseling sessions, and average reported hours of nightly sleep on depression scores at time 2 indicated that average reported hours of nightly sleep were the only significant predictor of depression scores at time 2 (P < .05). While depression scores significantly improved from baseline to post-assessment for all participants, it is possible that an unmeasured variable, or the synergistic intervention effect of the wellness program, accounted for changes in depressive symptoms over time. Future studies should incorporate sleep quality and assessing time spent in nature to explore these relationships further.
“The average number of hours of sleep per night was the only significant predictor of depression scores after treatment.”
Introduction
Mental health is essential to overall health and a basic human right. 1 Galderisi et al 2 describe mental health as a state of balance that allows individuals to effectively use their skills in line with societal values. It involves essential cognitive and social skills, emotional awareness and regulation, empathy, resilience to life’s challenges, social role fulfillment, and a harmonious mind-body relationship. 2 Depression, a mood disorder affecting mental wellness, contributes significantly to the global disease burden, affecting over 300 million people worldwide with the World Health Organization (WHO) ranking it as the largest contributor to global disability. 3 In the United States, mental health disorders are increasingly prevalent, with an estimated 22.8% of adults (57.8 million in 2021) experiencing a diagnosable mental disorder, 4 and approximately 8.3% suffering from at least one major depressive episode each year. 5
Various protective and risk factors have been identified, including biological, psychological, and social determinants, as contributing to the development of depression. 6 Current treatments for depression, such as pharmacotherapy and psychotherapy, have variable effectiveness.7,8 High rates of nonadherence with medication9,10 and the need for more effective treatment methods, especially for those with mild to moderate symptoms, have led researchers to explore alternative approaches, including nutrition,11,12 physical activity, 13 and lifestyle interventions. 14 Given the limitations and challenges associated with traditional depression treatments, there is an increasing interest in exploring comprehensive lifestyle interventions. The biopsychosocial model of depression suggests that a combination of treatments, including diet, exercise, and psychological support, may be more effective in managing depression. 15 These interventions, encompassing diet, physical activity, and holistic health practices, offer an integrated approach to managing mental health disorders, including depression.
Dietary habits have been shown to have an impact on mental health.16-18 Physical activity has been shown to reduce the incidence of depression 19 and may lower the risk of mortality in patients with depression. 15 Further, a recent meta-analysis found that physical activity and exercise have been used as treatment for major depressive symptoms and were found to have a large and significant effect on improving depression. 20 Circadian dysregulation is a common link between sleep and depression, and sleep/circadian-based strategies can be effective at relieving depressive symptoms. 21 Individually tailored motivational counseling is effective in assisting individuals in making behavioral changes that reduce sedentary behaviors and depressive symptoms. 22 Given the prevalence and impact of depression, there is an increasing interest in utilizing real-world evidence to identify and evaluate effective treatment strategies beyond conventional approaches.
Purpose
We examined the effectiveness of a brief, minimally invasive comprehensive lifestyle intervention on depressive symptoms in a diverse group of participants. The intervention included dietary modifications, exercise routines, counseling, and holistic health practices, aiming to address the multifaceted nature of depression. As such, we wanted to understand the predictive utility of self-reported total minutes of exercise, minutes of anaerobic exercise training, total hours of sleep per night, and the number of holistic treatments and mental health counseling sessions on changes in depression-related symptoms.
Materials and Methods
Participants
Sutliffe et al 23 (2015) first reported the materials and methods. Participants either chose to participate via self-selection or were medically referred to take part in this brief comprehensive residential lifestyle program at the Black Hills Health & Education Center (BHHEC) near Rapid City, SD, between May 2005 and June 2012. All participants were personally responsible for the expenses associated with participation in the program, with some portions of treatment covered by medical insurance.
A total of 430 adults aged 18-90 years (Mage = 57.5 ± 15.7 years) were included in the study. Each participant signed a BHHEC informed consent form agreeing to allow personal de-identified health history, biometric data, and treatment protocols to be used for research purposes. The BHHEC Institutional Review Board approved this study.
Intervention Description
All participants were expected to follow the general weekly schedule that was distributed to all guests and posted on the main bulletin board, based upon their own needs and situations, which included the following: two group vegan meals per day served buffet-style and eaten ad libitum in a group dining facility, morning group-based inspirational presentations, daily group lectures, exercise activities, group cooking classes, group recreational/social activities, and ample time allowed for rest and relaxation. In addition, each participant was provided with an individualized treatment plan based on responses to questionnaires, surveys, and physician examinations. The individualized plans included holistic treatments such as massage and hydrotherapy, personal strength training sessions, and individual sessions with wellness personnel, including a master’s degree-trained mental health counselor. The BHHEC program was conducted in 3-week cohort sessions, beginning on Monday and ending on Thursday, lasting an average of 19 days. The primary aim of the intervention was to optimize overall health and wellness and reduce chronic disease risk factors. The intervention did not follow a specific mental health/depression protocol but rather a generalized wellness program with specificity and application determined by diagnosis or physician-prescribed treatment plan.
Daily Routine
The standard daily routine during each session started with a wake-up call at 5:30 a.m. followed by an inspirational thought for the day and a medical check with a physician and/or nurse. An energizing walk followed a stretching session, and then participants consumed breakfast. Daily lectures and personalized holistic treatments of massage, fomentations, and/or hydrotherapy filled out the mid-morning schedule. As the second meal of the day approached, participants prepped for the cooking class/teaching kitchen session for the day, which included helping to prepare the mid-day meal with the supervision of the teaching kitchen instructor. Participants then partook in the meal they had prepared. After some light walking and relaxation, personal training sessions were conducted at the strength training center. After some more free time and a lecture, the participants took time to relax and then retired for the day in the early evening. Although the program is designed to be more of a wellness retreat, it maintained a foundation of an in-depth holistic lifestyle medicine program seeking to optimize natural healing. A major guiding principle of this intervention was to have the entire daily participant schedule synchronized in the natural circadian light-dark rhythms that are important for human homeostasis and correcting the possibility of circadian dysregulation often associated with clinical conditions, such as mood disorders. 21 Participants were encouraged to establish a routine bedtime each day while transitioning to less exposure to bright lights and electronic devices near bedtime, to maximize sleep quality.
Medical Examinations
Participant medical examinations, including general health history, assessment of typical sleep, dietary, and exercise habits, height, weight, waist, and hip measures, were performed by staff physicians on the first Monday morning after arrival. Administration of the Beck Depression Inventory (BDI-II) baseline measures were performed before or upon arrival. Exit examinations, the assessment of minutes exercised, number of hours slept, holistic treatments received, counseling sessions attended, and repeated measures of the BDI-II were completed just before the completion of each 18-day cohort session.
Beck Depression Inventory-II
The most current version of the BDI-II was designed for individuals 13 years of age and over with a fifth to sixth-grade, or higher, reading level. The BDI-II utilizes a different Likert-type response scale for each item representing not present (0), more than usual (1), much more than usual (2), and all of the time (3). Each of the four response options increases in severity ranging from not present (0) to more severe (3) and the possible total score for the entire inventory ranges between zero and 63. The total score cutoffs used the following diagnostic terms to classify individuals: minimal depression (scores of 0-13), mild depression (scores of 14-19), moderate depression (scores of 20-28), and severe depression (scores of 29-63). Higher scores from the BDI-II represent more severe symptomatology for depression. 24
The BDI-II was selected because of its ability to assist in the identification and assessment of depressive symptoms in clinical settings as well as among healthy individuals. 25 The BDI-II was first published in 1996, with a revised version of the BDI published in 1961. 26 The BDI-II has a high-reliability coefficient alpha (α = 0.80), and construct validity has been established. The BDI-II can differentiate depressed from non-depressed patients. 27 In addition, according to Rejeski et al (2006), 24 the BDI-II is one of the most widely used and well-validated self-report measures of depressive symptoms, providing a current measurement of depression-related symptoms limited to the past two weeks. This is not sufficient for, nor intended to be, a diagnostic tool but is rather a minimally invasive means for screening individuals to determine the severity of depression and to identify specific areas of concern.
Dietary Component
All participants were provided access to the same vegan food offered ad libitum and provided buffet-style twice daily (8:00 am & 2:00 pm daily). A third meal was not encouraged or promoted, but participants were provided a limited amount of fruit, bread, and spreads if desired. Although individual dietary intake records for participants during the intervention are unavailable, macronutrient and micronutrient needs were met or nearly met through daily dietary intake. 23 The vegan diet used in this intervention comprised fresh fruits, fresh vegetables, intact whole grains, and various legumes, nuts, and seeds; the standard intervention dietary protocol did not provide any dietary supplements, animal products, or animal byproducts. A random sampling of participants’ diets revealed, on average, 56.8% of the participants’ daily calories came from low glycemic, micronutrient-rich carbohydrate sources with a resulting intake of 49.11 g of fiber per day. Dietary fat made up 29.6% of the daily calories, and protein provided 13.6% of the caloric intake. Additional micronutrient analysis indicated that the dietary intake provided 2.4 mcg of B12, 320 mg of magnesium, 1200 mg of calcium, and 8 mg of zinc, on average. 23
Some examples of the foods provided at the two meals include:
First Meal: Fresh whole fruits and breakfast cold bar, fruit compote, whole wheat crepes, waffles, banana ice cream, cooked old-fashioned oats, smoothies, granola, almond milk, muffins, scrambled tofu with garden vegetables, hash brown waffles, cooked millet, whole nuts and seeds, berry jam.
Second Meal: Fresh garden greens and a complete fresh vegetable salad bar, nut and seed in-house salad dressings, vegetable burritos, vegetable lasagna, tamale pie, wild rice casserole, stir fry, quinoa loaf, stuffed dates, tofu pudding, date sesame bars, and no-bake carob balls.
Participants did not have access to alcohol, coffee, snacks, or food outside the center. They also did not have visitors or any sort of commissary from which to purchase additional foods.
Exercise Component
Based on the physician’s assessment and determination, participants were provided with guidance and instruction related to their medical clearance for performing exercise. Following medical clearance and based on the individual’s ability, participants were encouraged to join the group stretching and exercise sessions. Morning stretching sessions were led by a staff member and consisted of 15-20 minutes of light stretching. Daily outdoor and/or gym sessions using cardiorespiratory equipment sessions were scheduled twice daily. Participants could also walk/hike or use the cardiorespiratory equipment in their free time if so desired. Personal trainer-led strength training sessions were scheduled once a day for 2-3 days a week for 15-30 minutes per session. The primary equipment utilized was Cybex Eagle Selectorized Strength Equipment with plyometric, body weight, and free weight supplementation based on individual needs.
Statistical Analysis
All statistical analyses were conducted in IBM SPSS Statistics, version 29 (Armonk, New York). Means, standard deviations, and correlations were calculated for continuous variables, and percentages were determined for categorical variables. Variables were inspected for outliers and normality. Paired samples t-tests were used to analyze the effect of the intervention on the difference between BDI-II scores at baseline and time 2. Additional analyses explored the effect of the intervention on the differences in waist, hip, weight, Body Mass Index (BMI), and number of hours of sleep at baseline and time 2. Multiple linear regression models were used to determine if total exercise minutes, minutes of resistance exercise, number of holistic treatment sessions, number of counseling sessions, and average reported hours of nightly sleep affected BDI-II scores at time 2, using baseline BDI-II scores, diet at baseline (i.e., vegan, lacto-ovo vegetarian, no red meat, flexitarian, omnivore), age in years, education in years, number of medications reported at baseline, and weight at baseline as covariates. Additional multiple linear regression was used to determine if total exercise minutes, minutes of resistance exercise, number of holistic treatments, number of counseling sessions, and average reported hours of nightly sleep affected BDI-II scores at time 2 among those individuals who scored 20 or higher on the baseline BDI-II score. Baseline BDI-II, diet at baseline, age in years, education in years, number of medications reported at baseline, and weight at baseline were included as covariates.
Results
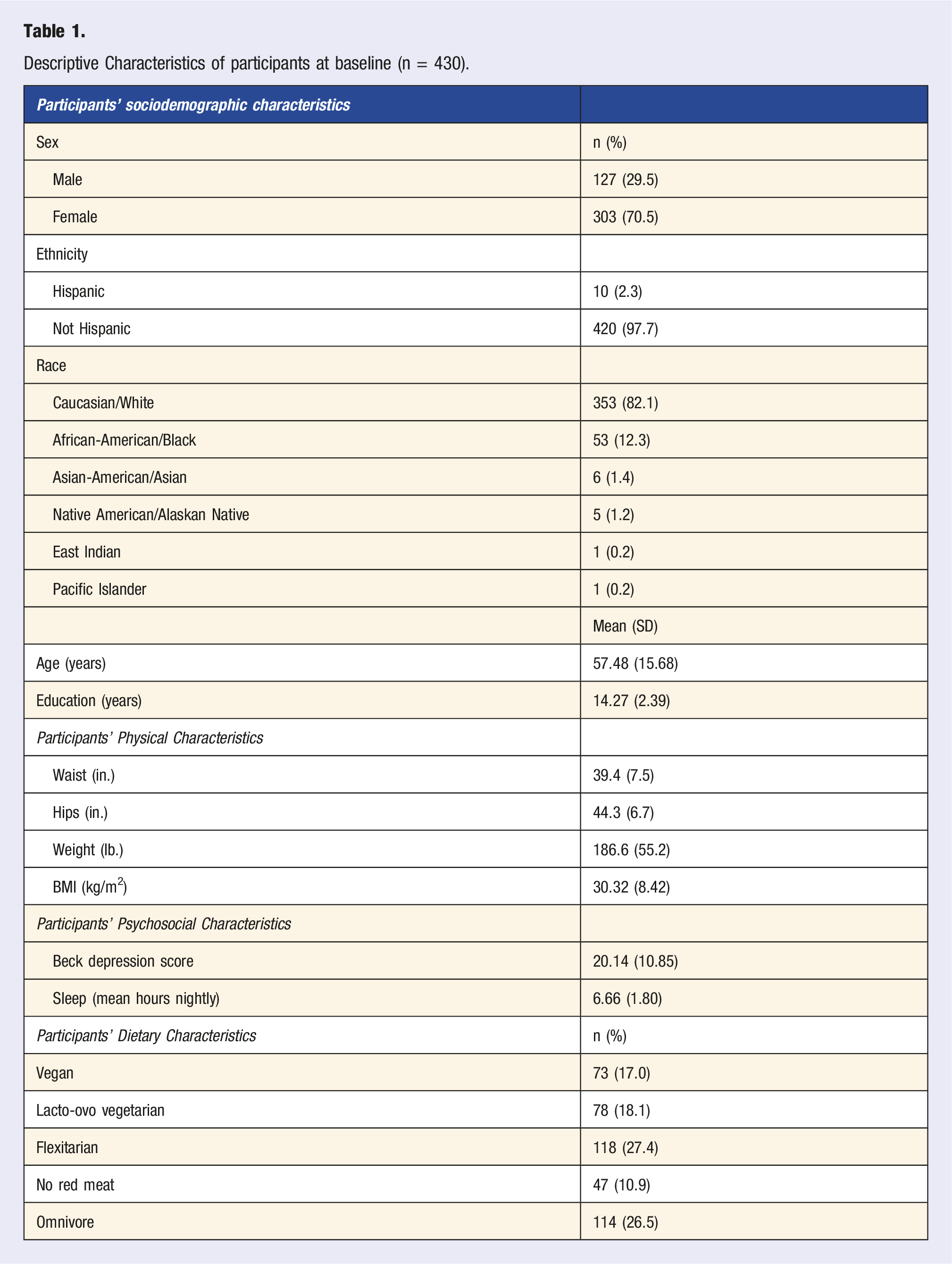
Descriptive Characteristics of participants at baseline (n = 430).
Descriptive Characteristics of participants at Time 2 With Paired Differences Between baseline and Time 2.
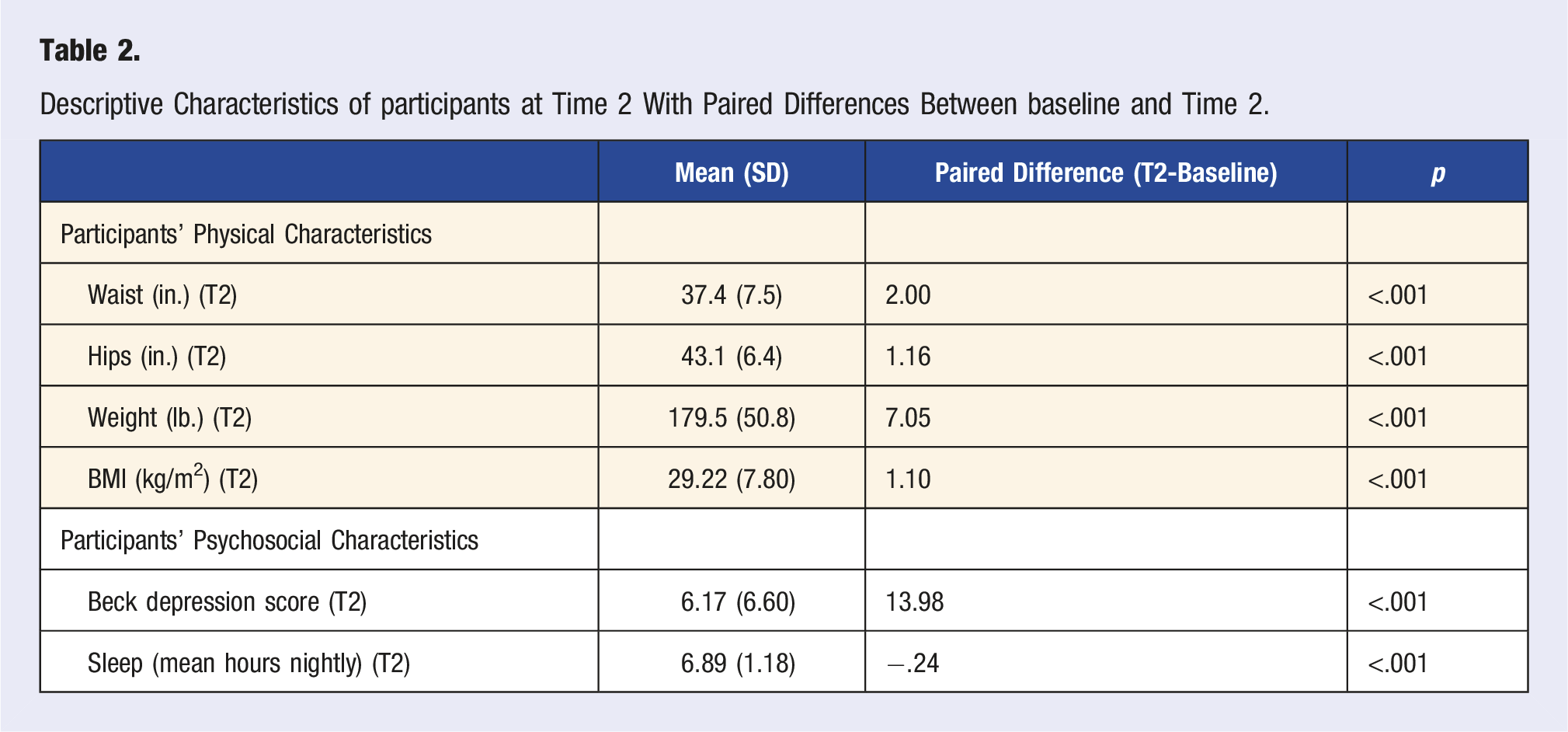
Paired samples t-tests were used to evaluate the difference in mean BDI-II score between time 1 and time 2. Data indicated a significant decrease in depression scores over time, with a mean decline of 13.98 points over time (MT1 = 20.14, MT2 = 6.17, P < .001) (Tables 1 and 2). When evaluating depression scores among those who scored 20 or higher at baseline, there was a significant decrease in depression scores over time, with a mean decline of 21 points (MT1 = 29.38, MT2 = 8.44, P < .001) (data not shown).
Paired samples t-tests also evaluated the difference in waist circumference, hips circumference, weight, BMI, and number of hours of reported sleep between time 1 and time 2. Data indicated significant differences in all variables (all p’s < .001) (Table 2). When evaluating these variables among those who scored 20 or higher on the BDI-II at baseline, there were significant differences in all variables (all p’s < .001) (data not shown).
Bivariate Correlations Among depression, Physical Activity, Counseling Sessions, Holistic Treatments, and Covariates.
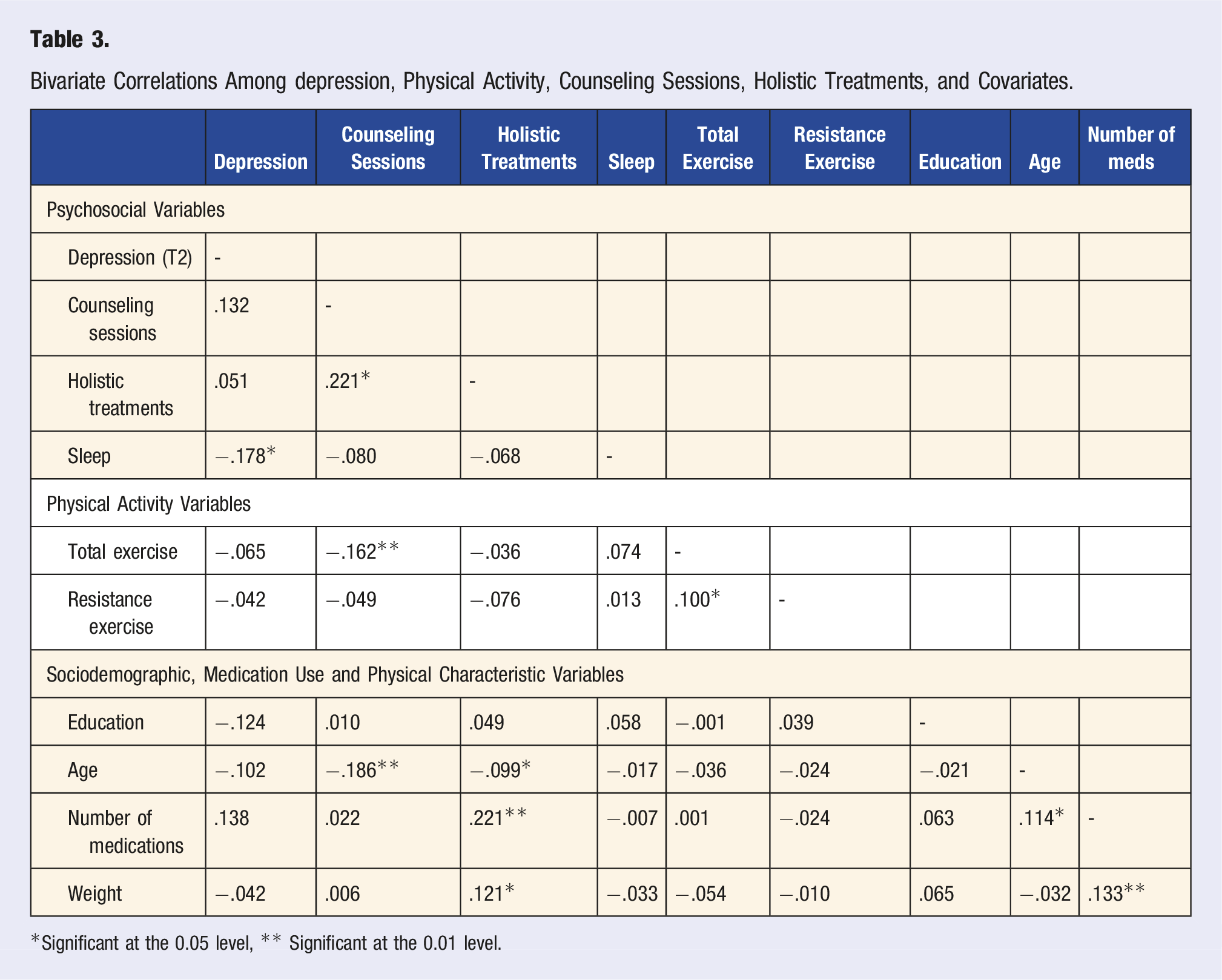
*Significant at the 0.05 level, ** Significant at the 0.01 level.
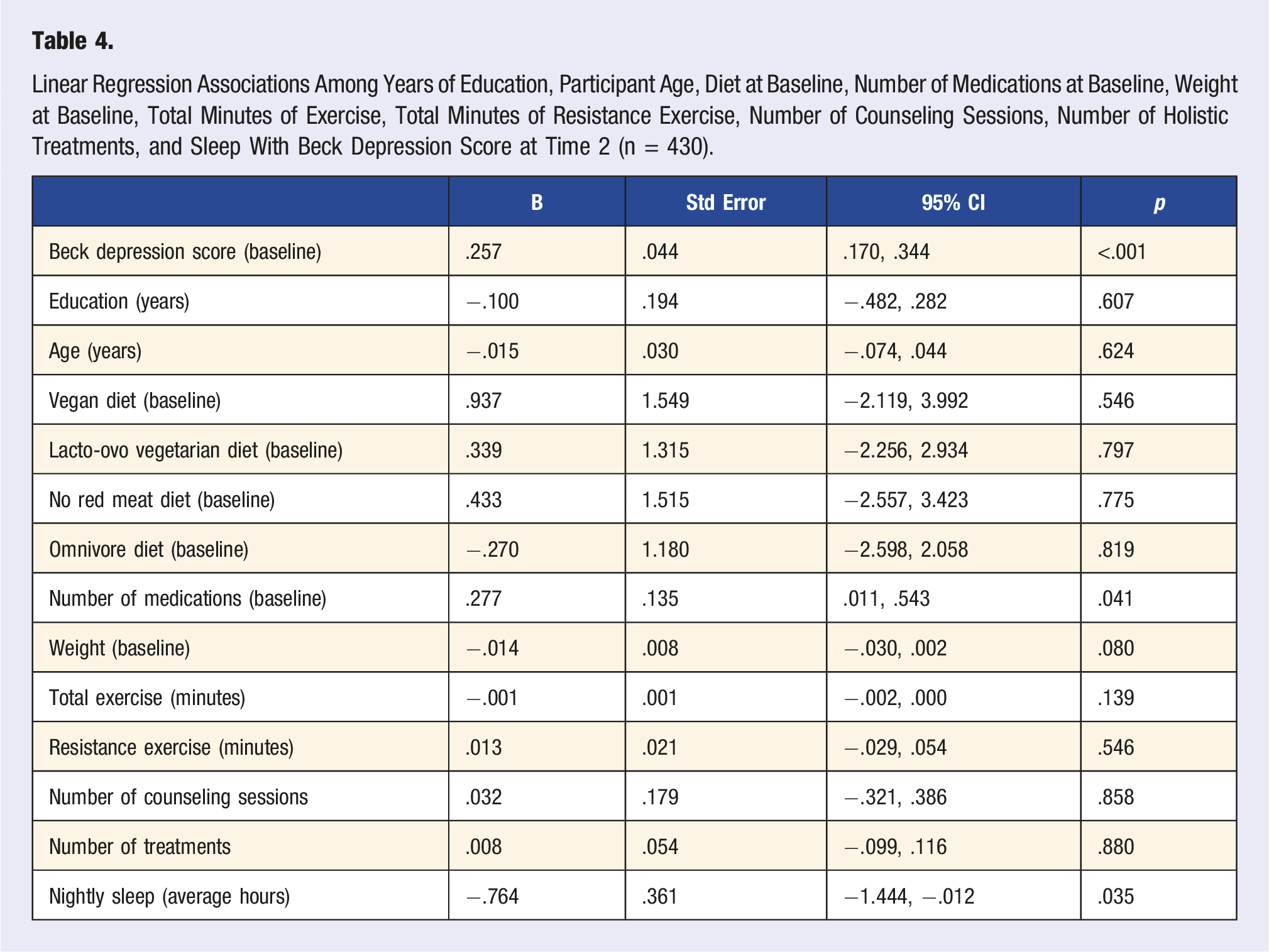
Linear Regression Associations Among Years of Education, Participant Age, Diet at Baseline, Number of Medications at Baseline, Weight at Baseline, Total Minutes of Exercise, Total Minutes of Resistance Exercise, Number of Counseling Sessions, Number of Holistic Treatments, and Sleep With Beck Depression Score at Time 2 (n = 430).
Discussion
We examined the effect of unique behavioral and lifestyle factors on changes in depression-related symptoms among adults enrolled in a residential lifestyle treatment program, emphasizing the importance of real-world evidence in understanding treatment efficacy. Depression scores were significantly improved from baseline to post-assessment, and individuals with moderate to severe depression scores at baseline experienced the most improvement in BDI-II scores. Findings indicated a negative association between average nightly hours of sleep during the participant’s stay and depression scores at the end of treatment. When examining individuals who had moderate to severe depression scores at baseline, sleep remained the only significant predictor of depression scores at post-assessment. Contrary to what was expected, total minutes of resistance exercise, total minutes of exercise, total number of holistic treatments, and total number of mental health counseling sessions were not significantly associated with depression scores at follow-up. While there were negative associations between counseling sessions with total exercise and age, results indicated only average reported hours of nightly sleep significantly predicted depression scores at post-assessment. This work contributes to a growing body of evidence that suggests lifestyle approaches (such as adequate sleep, social interaction, and mindfulness) can be utilized as a complementary strategy to reduce depression scores.28,29 It is critically important to understand why depression scores are higher in certain individuals to provide tailored interventions and treatments. 30 Specifically, our findings indicate wellness programs aimed at reducing depression among adults who have clinically significant and mild depression scores may want to promote sleep quantity.
Against expectations, holistic treatments, mental health counseling appointments, and exercise (total minutes and total minutes of resistance exercise) were not significantly associated with depression score improvements. Participants at BHHEC could meet with a professional counselor in a one-on-one setting on an as-needed basis for the duration of their stay. Similar findings on mental health appointments and depression in private treatment facilities were reported by Patel and colleagues (2010), 31 who found that patients randomly assigned to receive counseling at a public facility, but not those receiving counseling at a private facility, saw improvements in depression. Although cognitive behavioral therapy (CBT) is often considered the gold-standard psychological treatment, 32 this specific therapeutic approach was not used by the mental health care team at BHHEC. Beyond the number of appointments, quality of care is also an important consideration for successfully treating individuals with depression 33 and was not collected in this study. Future research should incorporate both the number of counseling appointments as well as patient self-reports on the quality of treatment received to enhance understanding of the link between counseling and depression scores in adults enrolled in BHHEC.
Contrary to our results, numerous studies suggest that holistic treatments are effective in reducing depressive symptoms. A 2010 meta-analysis reported results from 17 randomized controlled trials that evaluated the use of massage therapy on depression scores and found a 0.76 reduction in depressive scores. 34 While massage was the most utilized form of treatment in the current study, the mean number of treatments for such techniques as Swedish massage and deep tissue massage was 3.9 ± 2.0 and 2.9 ± 1.6, respectively, indicating that within an average stay of 19 days, individuals only received a treatment once every 5 days. This may not have been a sufficient number of treatments to warrant an effect on depressive symptoms. Hydrotherapy in the form of Russian steam bath and hot tub use were the most reported water-based treatments with 56% of participants engaging in Russian steam baths (M = 2.1, SD = 1.5) and 47% using the hot tub (M = 1.8, SD = 1.4). Research examining the use of hydrotherapy techniques in depression treatment is promising, with a meta-analysis reporting that hydrotherapy significantly reduced depression scores (Standardized Mean Difference [SMD] = 0.53). 35 Similar to engagement in massage, participants may not have received sufficient treatments to elicit a significant change in depressive symptoms. Future research should explore increasing the number of treatments individuals receive during their stay at wellness centers.
Prior evidence indicates that exercise has a moderate to large effect on decreasing depression.20,36-38 In a meta-analysis using randomized controlled trials of exercise interventions in people with depression, individuals randomly assigned to exercise interventions showed a large and significant reduction in depression with larger effects demonstrated when people underwent moderate-intensity aerobic activity. 20 It is recommended that people trying to improve depression should engage in 3-5 sessions per week of aerobic exercise with combined mind-body exercises of moderate-intensity. 39 Resistance exercise has also been linked to lowered depression and improved cognitive decline.40,41 In healthy older adults, both aerobic and resistance exercise were associated with significantly reduced depression scores and depression significantly decreased in both medium-long-term treatments. 42 It is unclear why the present study findings are not aligned with findings on exercise and depression in previous research. It is plausible that the minutes of exercise and minutes of resistance exercise were poor proxies and do not account for exercise intensity. Future work should consider adding wearable passive sensors to collect data on participant heart rate, heart rate variability, circadian activity, and sleep patterns to better understand the link between exercise, sleep, and depression.
The average number of hours of sleep per night was the only significant predictor of depression scores after treatment. Sleep quantity has been repeatedly shown to improve mental health.43,44 In a study of young adults (ages 18-25), sleep quality was the strongest predictor of depressive symptoms, followed by sleep quantity and physical activity. 44 Other findings indicate that irregularities in total sleep time and wake time are linked to greater depression scores. 45 In terms of sleep quantity, individuals are at risk for depressive symptoms when they get fewer than four hours of sleep per night, and those at the highest risk for greater depressive symptoms only receive two hours per night. 46 Sleep contributes to overall health promotion and was recently included in the “Life’s Essential Eight” list, which focuses on metrics relevant to optimizing and preserving heart health. 47 According to the essential eight domains, individuals in the optimal range are getting 7-9 hours of sleep per night, while those in the lowest range are getting four or fewer hours of sleep per night. 47 In the present study, people reported an average of 6.89 hours of sleep per night, consistent with the range listed in Lloyd-Jones and colleagues’ 47 work.
Previous dietary analysis of the vegan diet consumed by participants in the current study indicated an average of 49 g of fiber originating from micronutrient-rich plant-based foods. 23 This dietary pattern (i.e., fiber-rich, plant-based, micronutrient-dense) is associated with reduced inflammation, a known contributor to depression.48,49 For example, a meta-analysis that included 17 studies with 157 409 participants revealed that individuals on pro-inflammatory diets were 45% more likely to suffer from depression and 66% more likely to suffer from anxiety disorders than those on anti-inflammatory diets. 50 These results are in agreement with several previous studies that support the consumption of nutrient-dense, plant-rich diets that are high in fiber for the reduction of depression or depression-related symptoms.17,18,51-53 An important extension of the dietary component portion of this work could be to examine the gut microbiome and how the gut-brain axis plays a role in mental health, specifically depression and anxiety disorders.
To enhance long-term behavioral change to dietary patterns, participants were offered the opportunity to attend group cooking classes/teaching kitchen sessions and help prepare the food they would consume at the second meal. Only 14 participants indicated that they did not attend these kitchen sessions. We anticipate the high attendance rate will help the participants maintain their dietary patterns at home. 54
Finally, we believe it is possible that an unmeasured variable such as the synergistic intervention effect of the overall retreat experience can be the underlying reason for the significant changes in depressive symptoms over time. It has been shown that even a one-week retreat experience can substantially improve multiple dimensions of health and well-being. 55
Strengths and Limitations
There are several noteworthy strengths of the present study. First, the data were collected in a real-world setting, using data provided by participants enrolled in treatment at BHHEC. Unlike randomized trials in controlled settings, this study benefitted from using participants either referred by a medical provider or self-enrolled in the intervention. Length of stay varied and individuals received different treatments based on diagnosis, physician protocol, and/or personal preference. A major strength of this study is the enhanced ecological validity of study findings since data were collected in a real-world setting. As such, this work closely resembles clinical practice and has greater implications for similar treatment programs and wellness centers.
Another strength includes the large sample size and the extensive data collection process. This study was well-powered to examine the effects of different behaviors and treatments on change in depression scores. Participants were provided a high-fiber diet rich in micronutrient-dense, plant-based foods, known for their anti-inflammatory properties. Additionally, this sample included adults who ranged in age from 18-90 years old and represented a wide range of clinical characteristics. Finally, BHHEC offered participants a comprehensive residential lifestyle program that implemented a variety of holistic treatments, strength training, exercise, mental health counseling, and vegan nutritional components. Rather than focusing on only physical or mental wellness, this program encompassed a variety of treatments to holistically improve patient wellness. This incorporation of both physical and mental well-being into BHHEC is an effective way to destigmatize mental health treatment. 56
Present study findings should also be considered in light of study limitations. First, it is well-documented that time spent in nature and natural settings can improve depression.57,58 Additionally, time spent in nature has been shown to improve sleep quantity. 59 BHHEC is in a rural region of the Black Hills of South Dakota, with ample nature recreation opportunities and trails nearby. Participants were encouraged to spend time in nature, but no data were collected to represent total time spent in nature. Consequently, our model could not account for time spent in natural settings. Similarly, sleep quality was not assessed in the present study, which has been linked to reduced depression. 60 Future work should incorporate sleep quality and quantity measures to understand the unique contributions of both to changes in depression.
Some generalizability issues were present in our study sample; most participants were non-Hispanic White (82%) and female (70%). It is unclear if people from different racial, ethnic, gender, and socioeconomic status categories would benefit from aspects of treatment differently and if those differences would lead to clinically significant improvements in depression. Another limitation of this study includes data collection methods, namely issues related to social desirability and recall bias. As with any general survey tool used for large-scale screening, the BDI-II could be limiting. For instance, whenever individuals are completing self-report inventories, the setting in which the questionnaire is administered has the potential to influence the responses. Another limitation is when individuals with an accompanying physical illness are administered the questionnaire, the overall BDI-II score may artificially inflate due to the individual’s current extenuating circumstances. 61
In general, people tend to overreport physical activity and underreport foods consumed.62,63 Some of these discrepancies in reporting may result from social desirability bias or that participants responded in a way that they believe is favorable and free of judgment. 64 While the impact of social desirability bias on data quality is recognized in social sciences research, 65 it is improbable that participants in the current study deliberately reported moderate to severe depression to portray themselves more favorably.
A limitation related to stress is that we did not have specific data on participant stress levels at baseline, so we were not able to include this as a potential confounder. For future investigations, we recommend measuring pre- and post-stress levels for all participants through surveys or examining cortisol levels.
In future investigations, it may be wise to utilize a control group. Additionally, implementing a more rigorous study design (e.g., randomized controlled trial) to better assess individual intervention components should be considered.
Conclusions
In sum, exercise (the number of total minutes of resistance exercises and all exercises), the total number of holistic treatments and counseling sessions, and participants’ diet at baseline were not significantly related to depression scores in participants enrolled in a residential lifestyle treatment program. Total hours of sleep per night were the only significant predictor of depression scores among participants. Similar to that found in the overall sample, sleep was the only significant predictor of those with elevated depression scores at baseline. Depression scores significantly improved from baseline to post-assessment for all participants, with the strongest improvements in depression scores observed in individuals with moderate to severe depression scores at baseline. It is possible that unknown variables not accounted for in the data may have also influenced the overall improvement in depression scores, such as sleep quality and time spent in nature. Future work should consider incorporating real-time data collection methods such as ecological momentary assessment (EMA) to reduce recall bias and better understand micro-temporal changes in behaviors collected in real-time, and how that may influence changes in depression-related symptoms over time.
Footnotes
Acknowledgments
We are grateful for the study design and data collection protocol established by the late Ray L. Foster, MD, and for the data entry by Richard A. Nelson.
Author Contributions
JS was involved with the intervention design and implementation, consulted on the data collection, and was involved with the manuscript development, writing/editing. NL conducted all statistical analyses and contributed to manuscript development, writing, and editing. NP was involved with manuscript development and writing/editing. SH was involved with manuscript development and writing/editing.
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki, and approved by the Institutional Review Board of the Black Hills Health & Education Center.
Data Availability statement
All data related to this study is available by contacting the corresponding author.