
Abstract
Brain health is profoundly influenced by lifestyle factors, offering promising avenues for the prevention and mitigation of various brain health issues, including age-related cognitive decline. This review examines evidence on how key lifestyle modifications, including diet, exercise, sleep, stress management, social engagement, exposure to toxic environmental factors, risky behaviors, and cognitive training, affect brain health. Historical background is provided, but original articles published within the past 6 years that discuss lifestyle medicine are the focus of this review. The main topics covered are how Mediterranean, Nordic, and vegetarian diets support cognitive resilience, how physical exercise (aerobic and anaerobic) enhances neuroplasticity, and explain sleep’s role in metabolic clearance. In contrast, persistent stress leads to hippocampal atrophy, and toxic environmental exposures and head injury increase dementia risk. Other lifestyle modifications, such as meditation and social support, can mitigate these impacts. Cognitive reserve, built through lifelong learning and social interaction, provides resilience against neurodegeneration. While these strategies on their own hold value, personalized multimodal interventions have proven to be the most effective approach for promoting overall brain health and attenuating age-related cognitive decline.
Keywords
“Physical exercise enhances neuroplasticity, hippocampal volume, and executive function while reducing dementia risk.”
Introduction
Humans, unlike other smaller mammals, have slower and protracted preadult growth. This is due to the high energetic cost of human brain development.
1
Higher cognitive functions depended on the expansion, increased density, and complexity of the neocortex during evolution. The ability to plan, make decisions, and process emotional and social contexts came at a hefty energetic cost. Despite being only 2% of our weight, our brain function requires 20% of the total energy expenditure, and of that 20%, neurons alone expend 70-80%.1,2 In kilowatt hours (kWH), this equates to 0.3 kWH/day for an average adult, which is more than 100x what the typical smartphone requires.3,4 At rest, the brain uses 320 calories to think, and comatose patients expend 2 to 3 times less energy than the average person.
2
The question becomes, could the expansion of our cerebral cortex be our eventual downfall? It is difficult for the brain to maintain healthy metabolic function with age due to decreased mitochondrial functions and increased oxidative stress, resulting in insufficient energy supply to the synapses of brain cells, which reduces synaptic communication and synaptic strength.
5
Cognitive decline then occurs due to atrophy. In addition to natural aging, toxic proteins can accumulate, as with many neurodegenerative diseases, which further blunts mitochondrial function and cuts off energy supply.
6
Although many of these discrete mechanisms leading to age-related cognitive decline or neurodegeneration are not fully understood, and treatments are scarce, there are preventative lifestyle measures that may delay onset. This review will focus on the pillars of lifestyle medicine and how they, along with additional lifestyle habits, affect brain health. The authors will discuss the most recent data concerning: (1) Diet, (2) Exercise, (3) Sleep, (4) Stress, (5) Social Support, (6) Environment and Risky Behaviors, and (7) Cognitive Training/Education (Figure 1). In addition, multimodal clinical trials for preventing dementia and future directions will be explored. The lifestyle habits for maintaining a healthy brain. Diet: Adopting brain-healthy dietary patterns (Mediterranean, Nordic, and Vegetarian) with ketogenic elements provides substantial cognitive benefits. Exercise: Combining aerobic and resistance/strength training significantly supports brain health and resilience. Sleep: Consistent, quality sleep (7-9 hours per night) is crucial for cognitive function and long-term brain health. Social Engagement: Building social connectedness through community activities, support groups, and addressing sensory impairments enhances brain health. Stress Management: Mindfulness, meditation, and good social support mitigate stress, with Cognitive-Behavioral Therapy offering added benefits. Cognitive Reserve: Lifelong learning, social interaction, and education build cognitive reserve, reducing age-related cognitive decline. Exogenous Factors: Reducing air pollution exposure, limiting smoking and alcohol, and preventing head injuries promote healthy brain aging.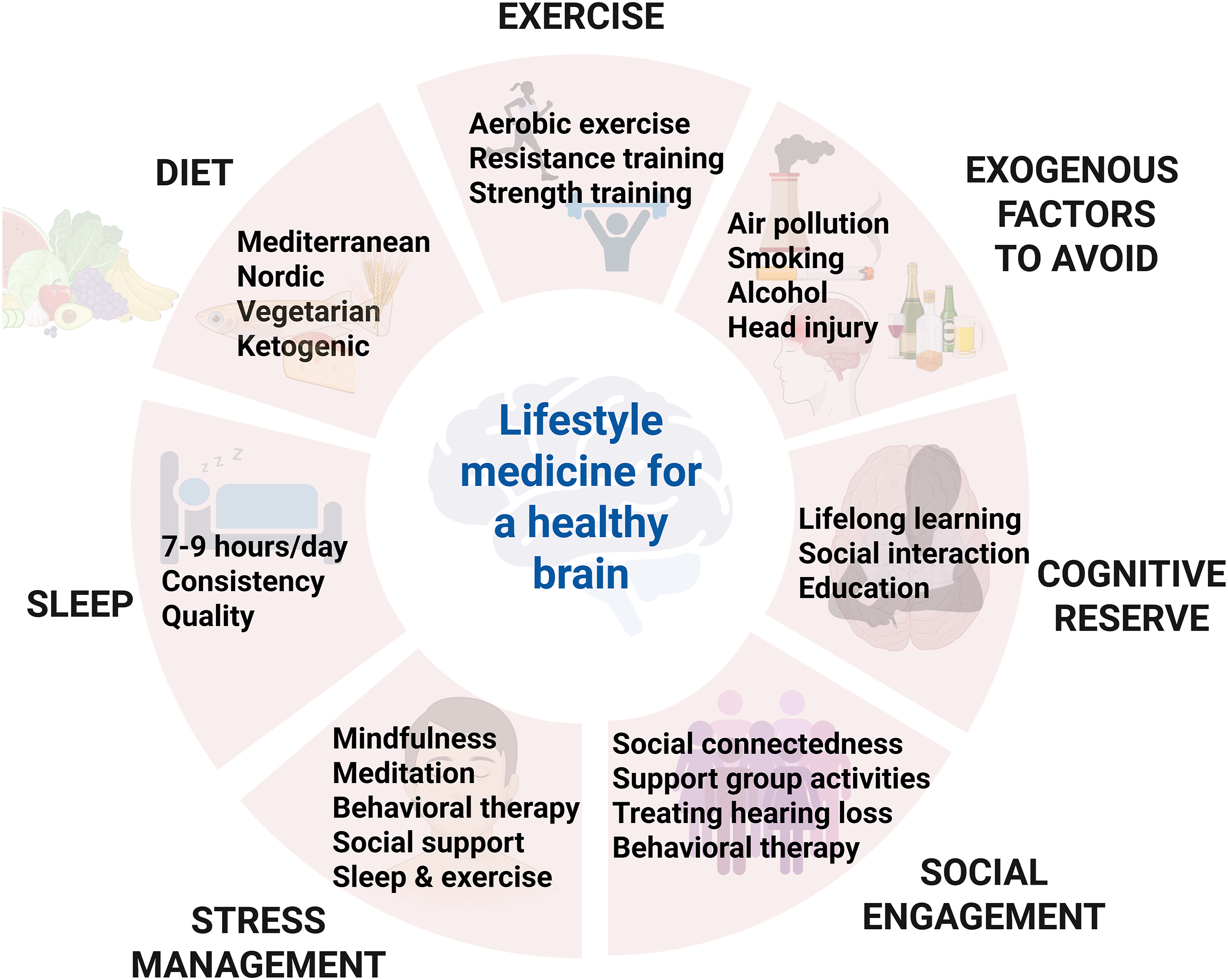
The Brain’s Energy Sources
Glucose, ketones, and lactate are the primary energy sources for the brain. Neurons mainly rely on glucose, but ketones and lactate can substitute during fasting or exercise, respectively.7-11 Because the brain has negligible intrinsic energy stores, it depends on a continuous substrate influx from the blood, regulated by the blood-brain barrier (BBB). 12 The BBB limits free transport and selectively allows essential nutrients through astrocyte “end feet” that contact pericytes and the basement membrane of the capillary. 13 GLUT1, GLUT2, GLUT3, GLUT4, and GLUT5 comprise a family of glucose transporter genes. Glucose intake is mediated by GLUT1 in endothelial cells of the BBB. While GLUT1 ensures delivery of glucose to glia, GLUT3 specifically mediates glucose into neurons.14-16 Monocarboxylic acid transporters (MCTs) transport lactate from astrocytes to neurons. 17 Lactate, produced from glycolysis and derived from pyruvate without energy cost, can replace glucose as a carbon source for metabolism. 18 Lactate provides 8% of the brain’s energy requirements, increasing to 60% during intense exercise.19,20 Lastly, energy from ketones, also transported through MCTs, is essential for the brain during development (30-70% of energy) and in adults when glucose is scarce.21,22 Ketones are a chemical produced after fat breaks down in the liver. Only astrocytes can generate ketone bodies from fatty acid beta-oxidation, but all cell types can uptake ketones for energy. 23 Ketogenic diets are used to treat epilepsy and may prevent AD.24-26 Therefore, diet and exercise are essential in the fight against the degenerating brain as the blood circulates these nutrients, which make their way through the BBB to influence neuronal signaling and health.
Healthy Brain Dietary Patterns
Comparison of Nutritional Components in the Mediterranean, Nordic, and Vegetarian Diets. The Mediterranean, Nordic, and Vegetarian Diets Support Brain Health. All Three Diets Emphasize Vegetables, Fruits, Whole Grains, Low-Fat Dairy and Eggs.
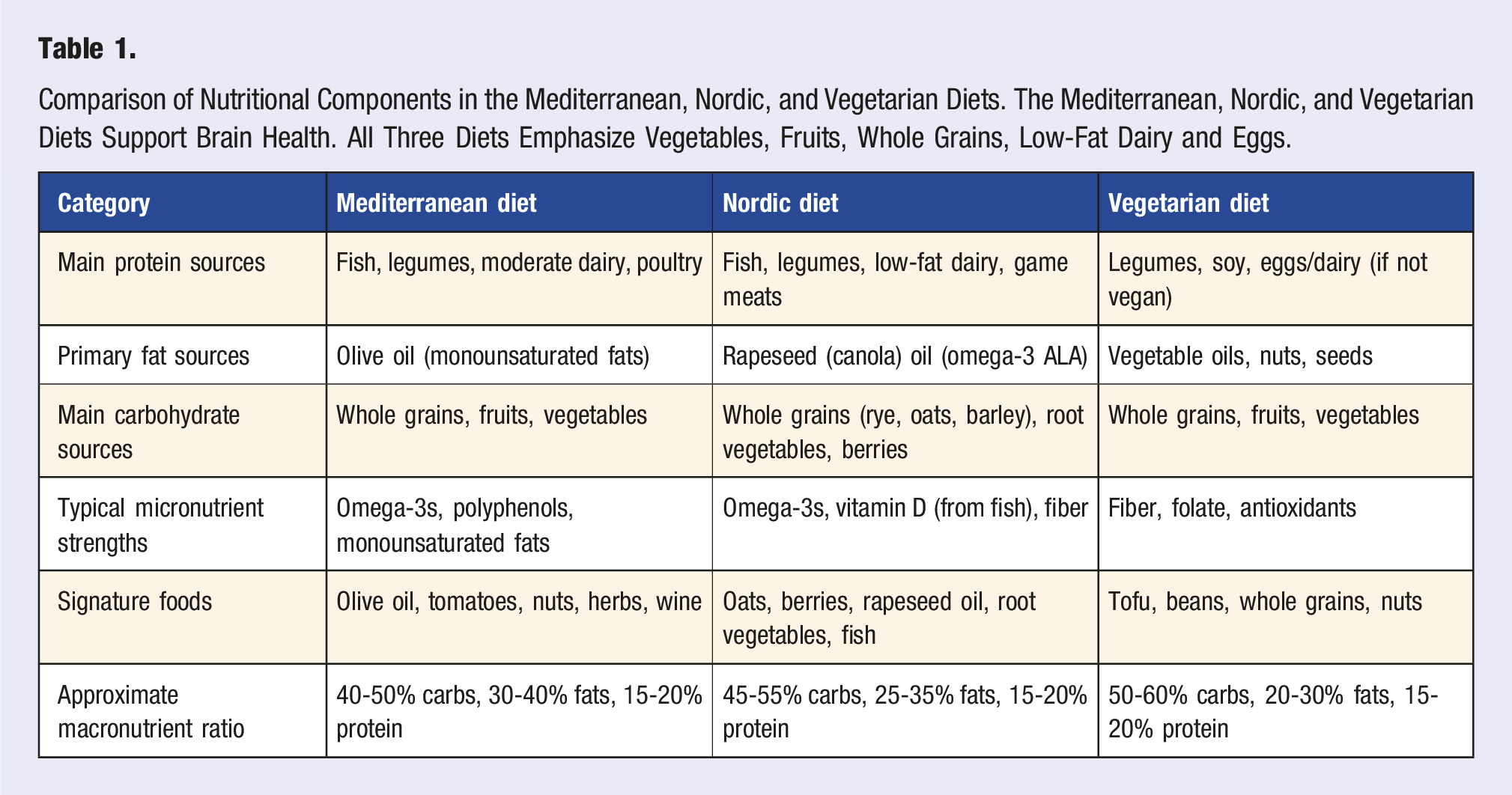
The Mediterranean diet is the most well-studied dietary pattern that is beneficial for maintaining cognition. 27 Inspired by cuisine eaten in the countries by the Mediterranean Sea, it contains whole grains, vegetables, legumes, extra virgin olive oil, nuts and seeds, fruits, fish and poultry, low-fat dairy products (such as cheese and yogurt), and wine (Table 1). 30 The Mediterranean diet limits the consumption of sweets, fried foods, red and processed meat, refined oils, and butter. 30 Two systematic reviews and meta-analyses showed reduced rates of cognitive decline associated with higher adherence to the Mediterranean diet.36,37 This finding has been corroborated in the PREDIMED (Prevención con Dieta Mediterránea) trial with a 4.1-6.5 year follow-up period.38,39 More recently, a meta-analysis of 20 studies that involved more than 44,000 individuals showed that the Mediterranean diet is associated with reduced white matter hyperintensity, which is damage to the myelin surrounding nerve cells, the white matter of the central nervous system. 40 Taken together, the evidence is clear that a Mediterranean diet is excellent for maintaining cognition.
Additional Mediterranean-style diets have been designed to reduce hypertension and preserve cognition. The DASH diet is similar to the recommendations of the Mediterranean diet and was intended to prevent and treat hypertension.34,41-43 The main difference between the diets is that the DASH diet limits refined sugar, processed foods, full-fat dairy products, saturated fats, trans fats, and sodium. 29 Interestingly, individuals who adhered to the DASH diet had better cognition in observational studies, but there was no association with cognition in prospective studies. 27 The MIND diet is also a modified Mediterranean diet similar to DASH that additionally emphasizes green leafy vegetables and berries and limits sweets, processed foods, red meat, fried foods, and cheese.29,33 In contrast to the Mediterranean diet, the MIND diet does not emphasize the high consumption of fruits and fish. Although the diet was designed to preserve cognition, results from studies have been mixed. 27 A randomized controlled trial (NCT02817074) of 604 older adults at risk for dementia found improved cognition after 3 years for both the calorie-restricted MIND diet and the calorie-restricted controls. 44
The Nordic Prudent diet, or the Baltic Sea diet, focuses on foods consumed in Nordic countries, which include vegetables, fruits and berries, fish, rapeseed oil, and whole-grain products (Table 1). 45 In contrast, meat and alcohol are limited. 45 High adherence to the Nordic diet by participants who were 60 or older was associated with less cognitive decline over a 6-year follow-up period compared to individuals with lower adherence in an observational study. 46 A recent systematic review of the Mediterranean and Nordic diets that included 88 studies provided support that both diets are neuroprotective and reduce the risk of cognitive decline. 47
Vegetarian diets also appear to be beneficial for maintaining cognition (Table 1). In a Taiwan study, individuals over 50 who consumed a vegetarian diet were less likely to develop mild cognitive impairment (MCI) during the 9-year follow-up period compared to non-vegetarians. 48 Similarly, African Americans who ate more plant-based foods maintained cognition better than those who ate more ultra-processed foods, although the same was not true of white participants. 49 The protective effect of a plant-based diet was also observed in a study from the Netherlands that included participants who were apolipoprotein E4 carriers, the greatest risk factor for Alzheimer’s disease (AD). 50
Additionally, there is increasing evidence that a ketogenic diet low in carbohydrates and high in healthy fats, such as nuts, olive oil, avocados, and fatty fish, is beneficial for brain health.29,51 When carbohydrates are restricted, the body produces ketones that are used as energy for the brain. The results from several clinical trials that used medium chain triglycerides (MCTs) as a supplement rather than a change in diet to test memory-impaired older individuals for enhanced cognition suggested that ketosis induced by supplementation improves cognition.26,52-56 In one dietary clinical trial, participants with mild to moderate dementia put on a ketogenic diet supplemented with MCT for 3 months had improved cognition. 57 Another clinical trial observed an increase in memory function in older adults with mild memory loss who were placed on a ketogenic diet with 5-10% of the calories from carbohydrates compared to diets with 50% of the calories from carbohydrates after 6 weeks. 58 The importance of early intervention, specifically in prediabetic patients with MCI, for successful therapeutic outcomes was observed in a clinical trial in which a high-fat modified Mediterranean ketogenic diet improved prediabetic patients with MCI after 6 weeks. 59 More recently, a case study on a patient with Down syndrome and AD found a marked improvement in cognitive function after 6 weeks on a ketogenic diet. 60 In general, these clinical trials suggest that more evidence-based research is needed before determining whether a ketogenic diet can help maintain cognition throughout life.
Future Directions for Improving Dietary Patterns
The Nutrition for Dementia Prevention Working Group has proposed recommendations for incorporating genetics, nutrition assessment tools, biomarkers that link dietary patterns with surrogate outcomes for cognitive decline, and novel clinical trial designs to guide future trials that may be beneficial for assessing dietary patterns. 28 The key to improving clinical trials may be to focus on dietary patterns that increase synergistic beneficial nutrients and decrease detrimental nutrients rather than focusing on single nutrients or supplements. Since dietary patterns are complex, the use of network analysis could help identify healthy and unhealthy patterns by comparing individuals with and without dementia, as in the Bordeaux study. 61 In this analysis, individuals with dementia had network central hubs representing foods they routinely consume that included cured meats. 61 In contrast, healthy controls without dementia had fewer connected networks, indicating a greater consumption of a variety of foods, and central hubs focused on healthy foods. 61 In addition, trials would benefit from longitudinal studies that included large cohorts of individuals over a lifespan, similar to the PREDIMED study, and include personalized approaches and public health interventions.28,38 In addition, more research is needed on culturally diverse dietary patterns since those presented above do not represent many underrepresented minorities because of limited knowledge in this area. 59 Additional studies are needed to determine whether nutritional supplements such as magnesium, vitamin D, B vitamins, and creatine help prevent cognitive decline. 62
Exercise for Dementia Prevention
Numerous studies have shown that physical activity enhances cognition and decreases the likelihood of developing AD and other types of dementia. Which types of exercise impact the brain and work best to boost memory, thinking skills, and executive function will be examined (Figure 2). The importance of physical activity was observed in the 1970s when researchers first reported a link between the neurotransmitter dopamine, a chemical messenger that plays an important role in the brain’s reward system, and reaction time. The increased dopamine levels during exercise are believed to contribute to better cognitive function. Although this link was established over 50 years ago, the evidence is still unclear regarding which exercise is most beneficial for healthy aging. For example, last year researchers found that (1) dopamine is released after acute cardiovascular physical exercise, (2) endogenous dopamine is an important neuromodulator for reaction time improvement and (3) reaction time is only altered when exercise is associated with signals from higher brain centers.
63
These data suggest that humans can rapidly alter their behavior using neuromodulatory systems, which have significant implications for promoting cognitive health. Exercise improves brain health. (A) Aerobic exercises such as running, biking, and walking can improve cortical connectivity, memory processing, and processing speed and increase gray matter volume and telomere length, which all contribute to better cognitive outcomes. (B) Anaerobic exercise such as weight lifting can reduce morbidity, improve cognitive abilities, and increase white matter and molecules essential for synaptic growth.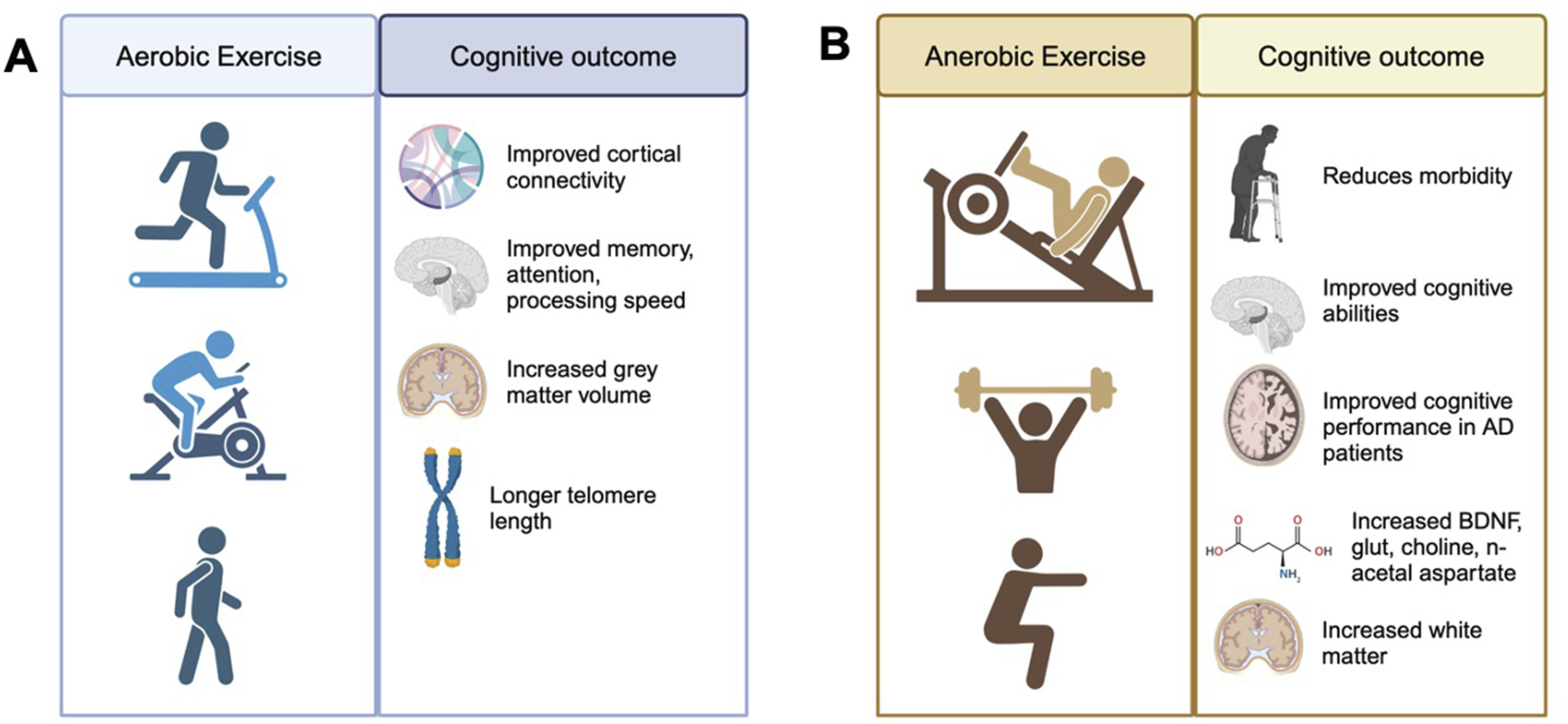
Long-term regular exercise can act as a prophylactic against aging, dementia, and neurodegeneration. More specifically, sustained aerobic physical exercise for 20 to 30 minutes that is sufficient to increase the heart rate and need for oxygen translates to cardiovascular fitness. This can be objectively assessed with measurement of oxygen consumption per unit time (VO2 max). 64 Aging is associated with a decline in VO2 max at a rate of 10% per decade after the age of 25 and up to 15% between the ages of 50-75.65,66 This can be due to a sedentary lifestyle, decreased maximal heart rate and stroke volume, reduction in blood volume, stiffening of the heart muscle fibers, and thickening of arterial walls.67-69 Age-related muscle loss also plays a role in VO2 max decline; however, individuals with an active lifestyle demonstrated a slower rate of decline than sedentary individuals.70-72 Therefore, training can influence muscle mass and VO2 max. In a study comparing older and younger rowers using upper and lower body activities (rowing and cycling), older subjects exhibited similar VO2 max scores to the younger cohort in cycling when controlling for muscle mass. 73
Cognition scores also improve after aerobic exercise (Figure 2A). For example, a 6-month randomized control trial among seniors translated into significantly improved cortical connectivity and activation compared to controls. 74 A meta-analysis of patients with dementia or MCI undergoing sustained exercise regimes showed improved memory, attention, processing speed, and executive function. 75 Brain volume, specifically gray matter, which decreases with age, is increased after 1 year of aerobic exercise compared with a control group of simple stretching and toning. 76 This was correlated with improved spatial memory. These data suggest that aerobic exercise is effective in reducing hippocampal volume loss and improving memory function. Even on the genetic level, exercise is beneficial. Telomere length, an index of cellular aging, was longer (predictive of longer life) in individuals who jogged or ran for 75 minutes per week. 77
Although a majority of the literature has focused on aerobic exercise and brain health, resistance and strength training are just as important, as seen by the correlation of muscle mass and cognition (Figure 2B). The available evidence on strength training is limited, but functional and structural brain changes are evident, and it is frequently recommended to counteract the age-related deterioration of physical functioning.78-82 Resistance training reduces morbidity and may also prevent cognitive decline and increase wellness.83,84 For example, greater strength in the quadriceps, hand grip, higher leg power, and whole body muscle strength are linked to better Mini-Mental State Exam scores as a measure of cognitive abilities.85-88 Concerning neurodegeneration, after 6 months of progressive resistance training, global cognitive performance improved in older adults according to the Global AD Assessment Scale. 89 Cognitive improvements in response to resistance training are based on changes in brain-derived neurotrophic factor (BDNF), frontal lobe structure, and decreased white matter (brain tissue composed of myelinated nerve fibers) atrophy and lesions.59,90,91 The most recent trial revealed that strength gains after 12 weeks of resistance training correlated with markers of brain health. 92 Using proton nuclear magnetic resonance imaging, N-acetyl aspartate, choline, glutamate-glutamine, and creatine were measured in the hippocampus and prefrontal cortices. These neurochemicals were sustained in the experimental aging group, but were decreased in the control sedentary group. In patients with MCI, 6 months of progressive resistance training improved cognition and expanded gray matter, and reversed the progression of white matter hyperintensities (a biomarker of cerebrovascular disease). Interestingly, the computerized cognitive training, but not resistance training, attenuated the decline in memory performance mediated by enhanced functional connectivity between the hippocampus and frontal cortex. 93 These findings suggest that exercise and cognitive training could enhance cognitive reserve.
Future Studies on Physical Activity for Preventing Cognitive Decline
Ideally, it is best to be physically active throughout life, but it is always possible to benefit from a fitness regimen regardless of age or current fitness level. In previously sedentary healthy middle-aged adults, 2 years of exercise training improved VO2 max and decreased cardiac stiffness. 94 Current evidence reveals that only 12% of adults over 65 meet the physical activity recommendations (physical activity for 30 minutes at least 5 days a week). This could be due to a lack of motivation, and future interventions should address self-regulation barriers such as negative views on aging (that it is uncontrollable or irreversible), low self-efficacy beliefs, and deficient goal-planning skills.95,96 The AgingPLUS trial is attempting to implement programs to target these beliefs, and this trial is ongoing. Although there have been many more basic science studies on the exact mechanisms behind exercise interventions and brain health, there is a need for better randomized controlled human trials on different forms of exercise, especially as a prophylactic. Additionally, exercise regimes may benefit from personalized medicine approaches as women often experience greater muscle loss and inflammatory responses to aging than men. 97 Lastly, exercise can be for everyone and access to a gym is not needed. Exercise modalities for everyone include walking, basketball, shoveling, yard work, rowing machines, and biking.
The Need for Sleep
Sleep is fundamental for human health, occupying roughly one-third of one’s lifespan, yet its full range of functions remains only partially understood. Extensive research confirms that sleep is essential for maintaining brain health, cognitive function, and overall well-being. Sleep occurs in distinct phases—rapid eye movement (REM) and non-REM (NREM) sleep, each of which contributes uniquely to our mental and physical well-being. 98 REM sleep is primarily associated with emotional regulation, creativity, and the consolidation of procedural and emotional memories. Whereas the NREM sleep, especially the deep slow-wave sleep (SWS) stage, is essential for restorative processes, strengthening neural connections, and facilitating memory consolidation. 99 Without adequate sleep, nearly every aspect of waking life, from attention and problem-solving to mood and judgment, becomes more effortful and less fulfilling. Despite these critical functions, modern society often prioritizes productivity and entertainment over sufficient sleep, leading to widespread sleep deficiency. Alarmingly, approximately 62% of the global population fails to achieve the recommended minimum of 7 hours of sleep per night for adults. 100 The economic consequences of sleep-related issues are also profound, costing high-income countries an estimated 1-2% of their Gross Domestic Product. 101
While acute partial sleep deprivation does not necessarily produce significant cognitive impairments, Total Sleep Deprivation (TSD) for even 1 night can dramatically impair attention, mood, and memory, with deficits comparable to those observed under alcohol intoxication.102-104 Sleep is crucial for skill acquisition. Studies indicate that individuals who experience sleep deprivation on the night following learning show virtually no improvement in performance over the following days. Whereas, those who sleep immediately after training exhibit significant enhancements, observable as early as the next day and sustained throughout the following week. 105 Studies also suggest that acute TSD disrupts higher-order cognitive functions, including memory maintenance, complex problem-solving, attention, emotional judgment, and decision-making.106,107 In high-stakes environments such as emergency response and military operations, sleep loss critically impairs the brain’s ability to process feedback, increasing the likelihood of errors. 108 One night of TSD has also been shown to increase susceptibility to false memories, with sleep-deprived individuals more likely to incorporate misleading post-event information into their recollections during memory retrieval. 109 These cognitive impairments are closely linked to upregulated brain excitability and altered plasticity due to sleep deprivation, further diminishing cognitive performance. 110 Concerningly, even a single night of TSD has been associated with increased β-amyloid accumulation in the brain, a factor linked to neurodegenerative conditions such as AD, and chronic sleep loss exacerbates this accumulation.111,112
Chronic sleep disruption has wide-ranging detrimental effects on brain function and overall health. Long-term inadequate sleep is strongly associated with accelerated brain aging, cognitive decline, and an increased risk of neurodegenerative disorders such as dementia.113-118 Research indicates that as many as 15% of AD cases may be attributable to poor sleep. 119 Cognitive impairment is also linked to greater variability in sleep patterns, including those seen in shift workers, with disrupted sleep patterns emerging as a predictive factor for later-life cognitive decline.113,117,120,121 Prolonged sleep disruption alters brain reward networks by increasing sensitivity to rewards while dulling sensitivity to losses, ultimately impairing decision-making and risk assessment. 122 Furthermore, sleep deprivation has been shown to impair creative thinking and increase migraine frequency, although further research is required to fully elucidate this relationship.123,124 Importantly, research has shown that children who consistently sleep less than 9 hours per night exhibit reduced gray matter volume in brain regions responsible for attention, memory, and inhibitory control, highlighting the long-term impact of insufficient sleep on cognitive development. 125 Sleep plays a crucial role in waste clearance from the brain, with recent discoveries highlighting that sleep is a heightened state for the removal of neurotoxic byproducts, including β-amyloid.117,126,127 Beyond its cognitive effects, chronic sleep loss has profound metabolic and physiological consequences, disrupting hormonal regulation by lowering leptin levels while increasing ghrelin, which promotes hunger, overeating, and weight gain. 128 Collectively, these findings reinforce the necessity of maintaining consistent, high-quality sleep as a cornerstone of cognitive and physical health.
Studies have consistently demonstrated that stable sleep of at least 7 hours per night is sufficient to maintain cognitive health in healthy adults (Figure 1).129,130 Although controversial, it is worth noting that excessive sleep has been linked to negative cognitive outcomes, highlighting the importance of maintaining a balanced sleep duration.115,131,132 Mitigation strategies for short-term sleep deprivation are well-established, with research highlighting the benefits of maintaining a consistent sleep schedule, practicing relaxation techniques such as meditation, engaging in regular physical activity, limiting caffeine and alcohol intake before bedtime, and optimizing the sleep environment to enhance both immediate cognitive performance and long-term brain health. These interventions help restore the balance between REM and NREM sleep, ensuring that both restorative functions and memory consolidation processes occur effectively. For chronic sleep deprivation, several evidence-based strategies can mitigate its long-term effects. Cognitive-behavioral therapy for insomnia has been demonstrated to improve sleep continuity and duration by addressing maladaptive sleep behaviors. 133 Relaxation techniques such as mindfulness, deep breathing, and meditation reduce pre-sleep anxiety, thereby improving sleep onset and overall quality.134-137 Light therapy, which involves strategic exposure to bright light, can also help reset circadian rhythms in individuals with mistimed sleep schedules. 138 In cases where sleep debt accumulates, scheduled napping and sleep extension have been shown to partially restore cognitive performance.139,140 Furthermore, engaging in regular physical activity has been associated with improved sleep quality and cognitive resilience. 138 Interestingly, while some cross-sectional analyses suggest that physical activity can mitigate the negative effects of poor sleep on cognitive health, recent research indicates that inadequate sleep may diminish the cognitive benefits of physical activity.141,142 While some advocate for stimulants like modafinil or caffeine to counteract short-term cognitive deficits from sleep irregularities, they cannot fully replace natural sleep’s benefits, especially for memory consolidation, which, once lost, is irrecoverable.132,143,144 These findings collectively reinforce the importance of integrating good sleep hygiene, cognitive and behavioral interventions, and physical activity as fundamental strategies for preserving cognitive health and mitigating the detrimental effects of sleep deprivation.
In summary, sleep is not merely a passive state but a dynamic process essential for cognitive function and overall brain health. While short-term sleep deprivation can lead to immediate impairments comparable to intoxication and disrupt critical cognitive processes, chronic sleep disruption poses even more severe risks, including accelerated brain aging, metabolic disturbances, and structural brain changes. By understanding the distinct roles of REM and NREM sleep and adopting strategies to ensure adequate, high-quality sleep, cognitive performance can be protected and enhanced both in the short term and over the lifespan.
Future Studies to Elucidate the Role of Sleep
Despite extensive research on sleep and brain health, several gaps remain. Individual differences in sleep requirements and resilience to deprivation are not well understood, highlighting the need for studies on genetic and neurobiological factors. The bidirectional relationship between sleep and neurodegeneration, particularly in AD, remains unclear, requiring mechanistic research to determine whether sleep loss is a primary driver of neurodegeneration or an early symptom of cognitive decline. The link between excessive sleep and cognitive decline also remains uncertain—whether it directly contributes to poor brain health or is a compensatory response to underlying medical conditions. Additionally, while research suggests that poor sleep may blunt the cognitive benefits of exercise, the nature of this interaction is not well understood, necessitating further investigation into how sleep and physical activity influence brain function at a neural level. The role of sleep in gut microbiome regulation and its impact on cognition is an emerging field that requires deeper exploration. Furthermore, pharmacological interventions like modafinil fail to replicate the full cognitive benefits of natural sleep, underscoring the need for alternative therapies such as cognitive-behavioral and lifestyle-based approaches. Lastly, most research has focused on adults, leaving gaps in understanding how sleep needs evolve across the lifespan, particularly in children and older adults. Addressing these gaps will be essential for optimizing sleep interventions and promoting long-term cognitive health across all age groups.
Social Engagement and Loneliness Affect Brain Health
This section will examine the importance of social engagement as it relates to brain health. The 19th and 21st U.S. Surgeon General Vivek H. Murthy, M.D., M.B.A., brought the public’s attention to the current epidemic of loneliness and isolation. 145 He has declared, “We are called to build a movement to mend the social fabric of our nation.” The social restrictions enforced during the COVID-19 pandemic have expanded this epidemic worldwide. 146 In his 2023 report, Murthy warned that the “epidemic is poised to precipitate a wave of cognitive decline and dementia,” and this is now confirmed based on an abundance of evidence from social isolation and perceived loneliness studies.
A systematic review of 6 studies concluded that maintaining regular social engagement reduces the risk of AD. 147 Another systematic review found that low social engagement and loneliness increased the risk for AD. 148 Being single, by choice, widowhood, or divorce, and living alone is associated with an increased risk of dementia. 148 A systematic review of 8 studies with more than 15,000 participants concluded that people with more social contact were less likely to develop dementia compared to those with less frequent contact. 149 Another systematic review also reported a small decreased risk of dementia after a short follow-up period (less than 4 years), whereas studies with longer follow-up periods (8.8- and 12-year) found a higher risk of dementia.88,150,151
Perceived loneliness is also associated with increased dementia risk. 114 The largest meta-analysis using longitudinal data pooled from >608,000 individuals across 21 samples confirmed that perceived loneliness increased the risk of all dementias and cognitive impairment. 152 Facilitator-led interventions designed to increase social contact and participation in activities have yielded inconsistent results on general cognitive function. One Finnish randomized controlled trial with a 3-month intervention observed a small significant improvement in performance on the AD Assessment Scale-Cognitive Subscale, however, other studies from the USA and China did not show any benefit.153-155 Multimodal studies that will be described later did show some benefits.
Hearing loss is also associated with an increased risk of dementia.156,157 Although it is not known how hearing loss may lead to dementia, in some cases, it may be due to psychosocial factors, including loneliness, depression, and social isolation. 114 It may also be due to decreased cognitive reserve resulting from decreased environmental stimuli. 114 Alternatively, it may be due to shared cardiovascular pathology. 114 The use of hearing aids is protective against cognitive decline and dementia. 158 Depression is also a risk factor for dementia. 114 The mechanism linking these chronic diseases remains unknown but reduced self-care and social interactions may be involved. 114
Interventions for Reducing Loneliness and Social Isolation
In the past few years, there has been a surge of articles elucidating approaches to reduce loneliness in the elderly.159-164 Some methods that are currently being investigated for individuals include support groups that focus on shared interests, improving transportation and technology access to improve social connectedness, one-on-one befriending approaches, treating hearing loss to improve the quality of social interactions, healthcare providers linking patients with social services, and cognitive-behavioral therapy (Figure 1). 165 Population health strategies also need to be tested so that more individuals may benefit. This may include health-system funding programs that integrate several approaches, including communication technology engagement, befriending programs, and organizing community-based social hubs (Figure 1). 165
Stress and Stress Reduction
Stress, in both biology and psychology, refers to physical and emotional challenges that activate the body’s coping mechanisms. While low to moderate stress can foster resilience, enhance adaptability, and reduce the risk of mental health disorders such as depression and antisocial behaviors, chronic or excessive stress has profound negative effects on brain health. 166 The COVID-19 pandemic further highlighted stress-related mental health impairments, including declines in working and prospective memory, increased anxiety, and depression, with potential long-term societal consequences.167,168 Prolonged stress exposure alters brain structure and function, particularly in the hippocampus, prefrontal cortex, and amygdala, leading to impaired memory, decision-making, and emotional control.169,170 MRI studies show that hippocampal atrophy is common in posttraumatic stress disorder (PTSD) patients, with smaller hippocampi linked to greater declarative memory deficits and lower hippocampal activity.171-173 However, it remains unclear whether trauma causes hippocampal shrinkage or if a smaller hippocampus increases PTSD vulnerability.166,174 The Hypothalamic-Pituitary-Adrenal (HPA) axis, a central stress-response system, releases cortisol that binds to hippocampal receptors, affecting learning and memory. 166 Elevated cortisol levels, whether from environmental stressors or artificial administration, impair verbal and visual memory, reduce problem-solving abilities, and exacerbate cognitive deficits in both PTSD patients and healthy individuals.175-180 Excess cortisol has also been linked to cognitive decline and neurodegenerative diseases, such as AD, by accelerating beta-amyloid accumulation.181,182 However, the PTSD-dementia link remains inconclusive. Studies have found increased dementia risk in PTSD patients, especially with comorbid conditions like depression,183-186 yet a 5-year follow-up study showed no increase in AD pathology, 187 suggesting other contributing factors. With only 1 meta-analysis and high study variability, PTSD’s role as a modifiable dementia risk factor remains uncertain. 114 Similarly, psychological stress has been considered for dementia risk scores, but limited evidence and its strong correlation with depression, a known dementia risk factor, make assessment challenging.188,189 Ultimately, stress is an unavoidable part of life, but while acute stress can be adaptive, chronic stress disrupts critical brain functions, increasing vulnerability to psychiatric disorders, memory deficits, and neurodegeneration.
Effective stress mitigation strategies include mindfulness-based stress-reduction (MBSR), meditation, physical exercise, cognitive-behavioral therapy (CBT), social support, and healthy sleep habits (Figure 1). MBSR incorporates breathing techniques, body scan meditation, and gentle movements to enhance present-moment awareness. It reduces stress by promoting cognitive flexibility by consciously interrupting habitual stress responses, lowering stress hormones, and enhancing brain volume and activity in areas linked to emotional and cognitive resilience.190-194 Similarly, meditation is widely used to manage stress-related conditions, including anxiety, depression, chronic pain, hypertension, and heart disease. Various meditation forms, including guided visualization, deep breathing, mindfulness meditation, Qigong, Tai Chi, Yoga, integrate breathwork, movement, and cognitive focus, foster relaxation and resilience.190,195 Even brief, consistent MBSR and meditation practices are known to be impactful in managing stress.190,196-198 However, it is worth noting that while both approaches are effective for stress mitigation, they may not significantly restore cognition, as observed in older adults with subjective cognitive decline who practiced these techniques for 6 months. 199 Physical exercise, both aerobic activities and strength training, has been shown to help in stress mitigation and lower stress hormones.200-204 CBT helps by restructuring maladaptive thought patterns, reducing stress perception, and enhancing coping mechanisms205,206; while social support and strong interpersonal relationships serve as protective factors, buffering against stress-induced neuropsychological effects and lowering physiological stress responses. 207 Maintaining healthy sleep habits is also critical, as sleep deprivation exacerbates stress effects, while proper sleep hygiene helps regulate cortisol levels and improve cognitive resilience. 208 Integrating these strategies provides a well-rounded approach to stress management, promoting emotional balance, cognitive function, and long-term mental health. Ongoing research continues to refine and personalize these techniques for optimal effectiveness.
Future Studies for Stress Mitigation
Further studies are needed to explore the long-term impact of stress and PTSD on cognitive decline and their potential role as risk factors for dementia and other neurodegenerative conditions. Since stress is often intertwined with sleep disturbances, depression, anxiety, etc., understanding how these comorbidities interact is crucial for developing personalized stress mitigation strategies. Investigating the biological pathways through which chronic stress affects brain function, such as HPA and cortisol dysregulation, inflammation, and oxidative stress, can help identify effective interventions. While MBSR and meditation techniques offer stress relief, their effects vary, and some individuals, particularly those with pre-existing mental health conditions, including PTSD, may experience adverse effects. 194 Therefore, further studies must evaluate their risks and ensure they are appropriately tailored rather than universally prescribed. Advancing neuroscientific and psychological research will be key to refining stress management strategies that enhance cognitive resilience and long-term brain health.
Building Cognitive Reserve is Important for Brain Health
Cognitive reserve (CR) is built on education and mental and social activity throughout life (Figure 1). The Rush Memory and Aging Project reported that having a greater purpose in life is associated with a reduced risk of AD. 209 A study using Swedish twins showed one of the first links between education and dementia in 2001, and to this day, lack of education is a major risk factor for AD. 210 These findings suggest that improving education can boost CR to act as a defense against dementia and age-related cognitive decline (ARCD). Meta-analyses have revealed that low education level met the criteria as a risk factor for dementia, whereas high education was protective.211,212 However, the analysis of education has been met with controversy. Criticisms have included diagnostic bias, confounders such as age and gender, and whether or not educational attainment can be considered a uniform concept across diverse populations. In a review of databases from 1985-2010, 58% reported significant effects of lower education on risk for dementia, whereas 42% reported no relationship. 213 Additionally, a relationship between education and dementia risk was more consistent in developed regions. More recently, in individuals aged 75 and up using an operational definition of education (more than 10 years of education), researchers observed lower dementia risk in those with more years of education, showing that the number of years is important, not just the form of higher education. 214 When taking a life span approach, examining the variability of dementia using age-specific distribution of dementia events, the model age of onset is 85 in adults with a college degree. The model age for adults with less than a high school degree occurs before age 65. 215 These data were measured across race and gender groups and suggest that higher levels of education can delay the onset of dementia and compress dementia into later stages of life. Many studies have reviewed and concluded that education promotes cognitive functioning and lowers dementia risk in old age, but what is the mechanism? Educational attainment is associated with advantages in cognitive functioning during early adulthood that might be preserved into old age. Education may provide knowledge and cognitive skills that allow individuals to process tasks in a more efficient way which is less damaging. Brain changes associated with CR and education might be discrete, more on the synaptic level than macrostructural changes. Therefore, these changes may not be measurable using current MRI techniques. Based on this idea that education makes the largest impact in early life and is preserved in later life, the conclusions drawn here may indicate more brain reserve than compensation or CR (Figure 1). 216 In support of this hypothesis, higher education has been associated with a slower decline in individuals with lesser atrophy, but with a faster decline in those with greater atrophy. 217
Future Studies on CR and Education
Current evidence for education’s impact on dementia is consistent with a threshold model. That is, a person with more education will, on average, perform better in old age. This means that if both individuals are equally impacted by age-related insults or pathology, starting at the same age, then the person with more education will take a longer time to reach cognitive decline or lower cognitive functioning. Education is not strongly associated with reductions in cognitive decline in later adulthood. Although associations may arise under certain circumstances, these are unknown and could be a future area of work. Additionally, future research should examine mechanisms of cognitive development in childhood into early adulthood to better understand the mechanisms behind late-life protection. There is still a need to understand the individual differences in the rate of cognitive aging and factors that postpone or slow cognitive decline. CR most likely encompasses many aspects discussed in this review.
Environmental Factors and Risky Behaviors to Avoid for Brain Health
Exposure to some risky substances, including alcohol and tobacco, environmental factors, such as air pollution, and risky behaviors such as trauma and head injury, can increase the risk of dementia (Figure 1). This section will address what is currently known about these exogenous factors and suggest additional research needed for clarification.
The majority of the evidence from systematic reviews suggests that light to moderate alcohol consumption reduces the risk of AD. 32 Daily and heavy alcohol consumption, however, may increase one’s risk for cognitive decline.32,218 A systematic review concluded that there are major limitations in the design of many of the studies examining the dose-response of alcohol and long-term mental effects due to bias. 219 Based on the current data, the best recommendation would be to avoid daily and heavy alcohol consumption to reduce the risk of developing dementia.
In contrast to alcohol consumption, systematic reviews consistently conclude that smoking increases the risk of AD in current smokers. 32 There was no association with dementia for former smokers or never smokers, but this may be because these 2 categories of smoking were poorly defined in most studies. 32 Unfortunately, bias in some of the studies that were funded by the tobacco industry has led to the false claim that smoking reduces the risk of AD. 220 A rigorous analysis of 43 studies showed that case-control studies yielded lower average risk estimates than cohort studies. 221 In addition, there were lower risk estimates for studies supported by the tobacco industry. 221 Therefore, smoking avoidance throughout life or implementing a smoking cessation program would be beneficial for maintaining brain health.
Another clear risk factor for AD is head injury. A meta-analysis of 7 case-control studies found an association between head trauma that involved loss of consciousness and the risk of AD in males. 222 A systematic review of 15 case-control studies replicated the findings of the first meta-analysis using the same data but could not replicate the findings in more recent studies. 223 A 2010 report by Williams et al. concluded that traumatic brain injury appears to be associated with an increased risk of AD in males. 148 A scoping review of 45 studies revealed that about 50% of children and adults who have a single mild TBI have long-term cognitive impairment, including executive function, learning/memory, attention, processing speed, and language function. 224 Mild TBI is also associated with the onset or worsening of posttraumatic stress disorder, major depressive disorder, and suicidality. 225 Therefore, head protection equipment in sports and combat would improve brain health throughout life.
Attention to air pollution’s effects on the brain came from a 2002 study on dogs in Mexico City. 226 Since then, many epidemiological studies have linked air pollution to cognitive decline and dementia.227-235 However, no meta-analysis of these studies exists because of the diversity of air pollutants, study designs, and endpoints measured. 227 The recent Maastricht cross-sectional study of more than 4000 participants found that higher PM2.5 (particulate matter <2.5 micrometerμ) exposure is associated with more brain atrophy. 236 The overall conclusion based on the present evidence suggests that chronic exposure to air pollution is associated with cognitive decline, especially in visuospatial abilities and dementia. 227 Based on the evidence, using air filters to improve indoor air quality should be beneficial. In addition, implementing policies to reduce air pollution should have a huge impact on population health.
Future Studies on Exogenous Risk Factors Associated with Cognitive Decline
Although there have been many additional studies investigating potential environmental risk factors for dementia, including lead, solvents, electromagnetic fields, pesticides, aluminum, mercury, copper, and iron, the data to support their role in cognitive decline is inconclusive. 32 Therefore, further well-designed studies would be beneficial for determining if there are additional environmental factors and risky behaviors that may lead to cognitive decline.
Multimodal Trials Provide Evidence that a Healthy Lifestyle Helps Maintain Cognition
Multimodal Interventions to Improve Cognitive Decline. The ReCODE Study Involves all Possible Lifestyle Interventions and can Improve Cognition After 12 Months. The SMARRT Trial Modifying Exercise, Diet, Training, and Sleep Shows Modest Improvements in Cognition After 2 Years. The FINGER Trial Modifying Exercise, Diet, and Training Improves Executive Function After 2 Years. PRODEMOS is Unique in That It Uses Community Outreach and Telehealth to Modify Lifestyles. This Trial Modestly Reduced Dementia Risk Factors.
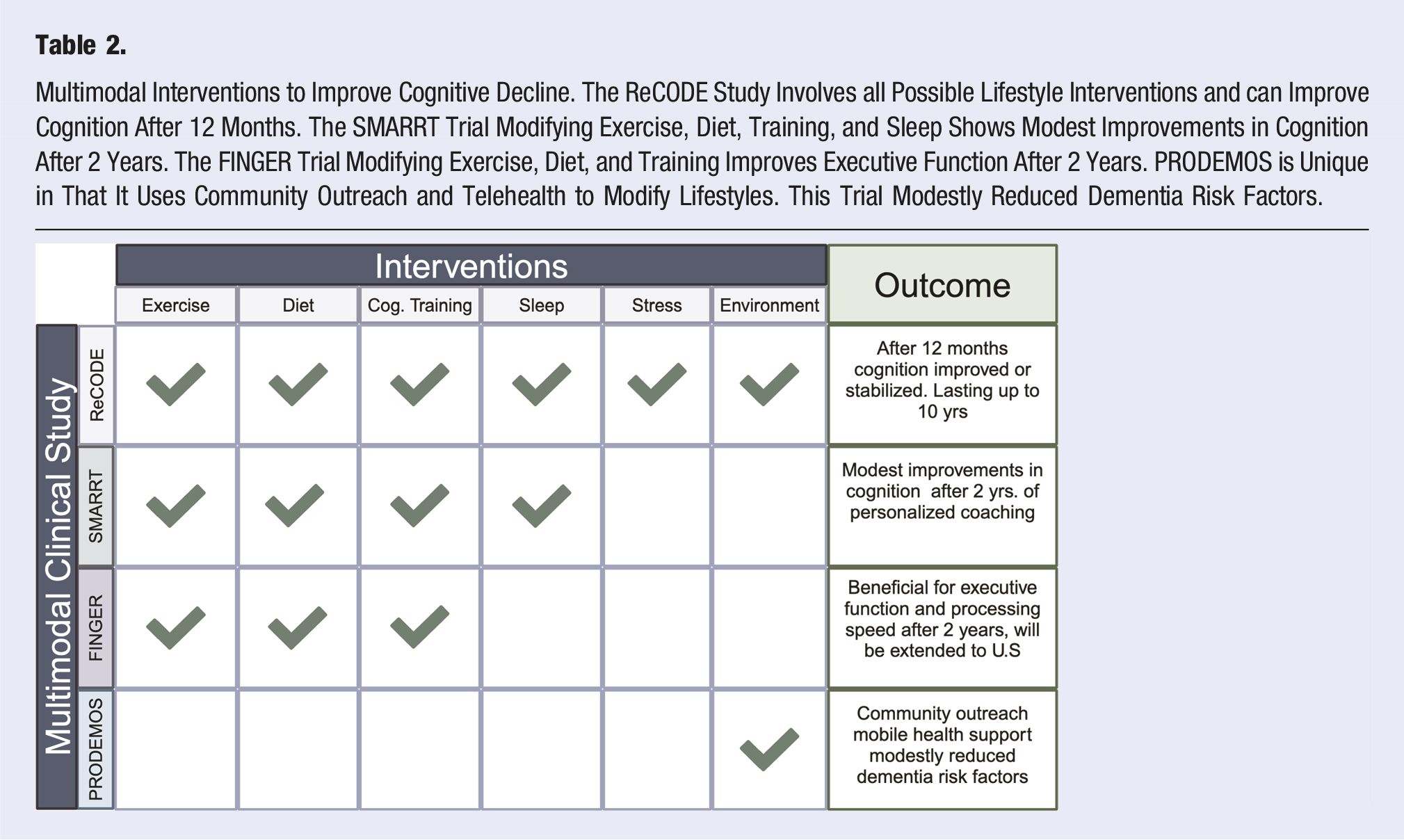
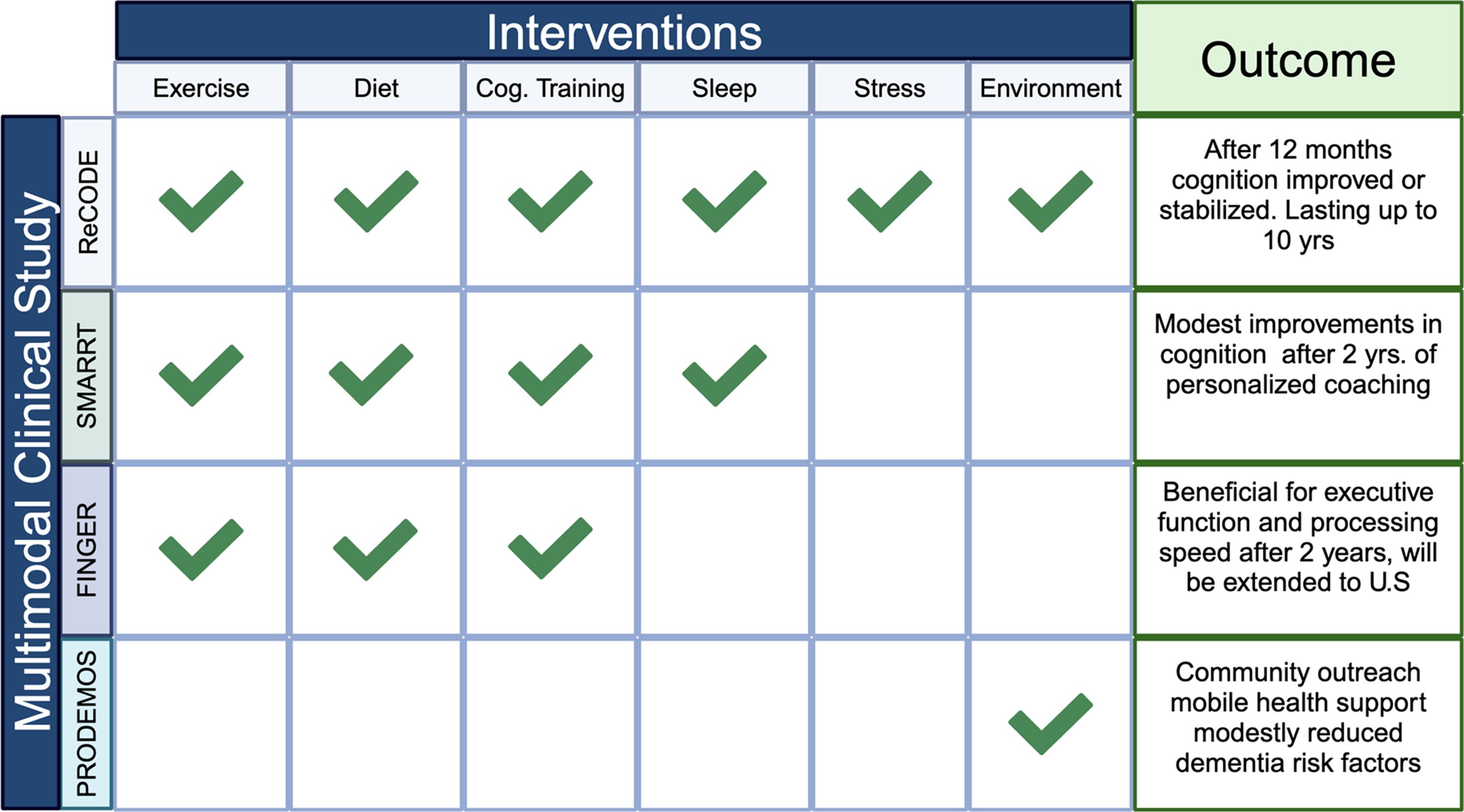
In the ReCODE (reversal of cognitive decline) program, 255 participants with subjective cognitive impairment, mild cognitive impairment, or early-stage AD received personalized recommendations to address their individual needs, which included information on nutrition, exercise, cognitive training, sleep, stress management, and detoxification. 237 The results showed that after 12 months, cognition stabilized or improved for all participants. 237 Some of the participants continue to show sustained cognitive improvement for more than 10 years. 238
In the Systematic Multi-domain Alzheimer’s Risk Reduction Trial (SMARRT, NCT03683394), 82 dementia-free older adults (70-89 years) were paired with a health coach and nurse to create personalized programs to reduce the participants’ risk of dementia.239,240 The participants set their own goals in this study, with most choosing physical activity (95.1%), hypertension (72%), cognitive activity (59.8%), and sleep (52.4%).239,240 The results after 2 years indicate that the participants who received personalized coaching had modest improvements in cognition compared to health education controls. 240
The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) trial was a 2-year multidomain intervention that included diet, exercise, cognitive training, and vascular risk monitoring over 2 years. 241 Results from the trial showed that diet, exercise, and cognitive stimulation were beneficial for executive function and processing speed compared to controls who received general health counseling. 241 The research from FINGER will be extended in the ongoing randomized controlled US POINTER study (NCT03688126). 35 Two thousand older American adults will participate in the trial for 2 years, with outcome assessments made at baseline and every 6 months.
The SMARRT, FINGER, and US POINTER trials provide personalized coaching, which successfully engaged the participants and led to successful outcomes for reducing the risk of cognitive decline. These programs are time-consuming and costly, and may not be useful for community-based programs. The multinational, randomized, controlled PRODEMOS (Prevention of dementia using mobile phone applications, ISRCTN15986016) trial takes a hybrid approach with community outreach using a coach-supported mobile health (mHealth) intervention. 242 Participants (1488 total) of low socioeconomic status in the UK or from the general population in China who are 55-75 years old with at least 2 dementia risk factors were the target populations. After a 12-18 month intervention, participants were evaluated for changes in cardiovascular risk factors, aging, and risk for dementia. The results from the study suggest that coach-supported mHealth intervention modestly reduced dementia risk factors. 242 A longer follow-up period is needed to assess whether this translates into a reduction in cognitive decline and dementia.
In contrast to the trials described above, several multidomain interventions did not produce evidence of a benefit for cognition. In the Look AHEAD study (NCT00017953) of individuals with type 2 diabetes who were overweight or obese, no effect was noted in the prevalence of cognitive impairment after 10 years of decreased caloric intake and increased physical activity. 243
There were mixed results from the Netherland-based Prevention of Dementia by Intensive Vascular Care (preDIVA) trial (ISRCTN29711771), in which 70-78-year-old individuals with cardiovascular risk factors received 6 years of nurse-guided multidomain interventions compared to a control group who received standard care. 244 A post-hoc subgroup analysis showed that about 28% of the participants with untreated hypertension who adhered to the intervention had a reduced risk of dementia. 245 However, after 12 years, there were no cognitive benefits.244,245 These results may have been due to the high standard of care given to the controls, the age of the participants not being ideal, or the intervention not being of sufficient intensity. 244
In the French-based Multi-domain Alzheimer’s Prevention Trial (MAPT) trial, a broad range of ≥70-year-old participants without dementia who had spontaneous memory complaints were divided into 4 intervention groups. One group received a multidomain intervention including physical activity, cognitive training, nutrition consultations, plus an omega-3 polyunsaturated fatty acid supplement. The second group received the multidomain intervention plus a placebo. The third and fourth groups received an omega-3 supplement alone or a placebo. The results from the study showed no cognitive benefits after 3 months. 246 Several potential problems with this study included the short follow-up period and the age of the participants (mean 75·3 years) with memory problems but no dementia. Therefore, the participants may have a higher cognitive reserve and lower dementia risk. 246
Future Studies on Multimodal Approaches
Based on the success of some of the multimodal trials designed to maintain brain health, it is clear that providing the participants with lifestyle coaching is very helpful in encouraging continued engagement with the program. The trials suggest that diet, exercise, and cognitive reserve help reduce the risk of dementia. It is also clear that more studies are needed to better understand how to design personalized programs and community-based interventions.
A promising active trial is the PROtein enriched MEDiterranean Diet and EXercise (PROMED- EX, NCT05166564) randomized controlled 6-month trial. 247 Undernutrition often affects elderly individuals and increases their risk of developing dementia. The PROMED-EX trial is designed to determine if a protein-enriched Mediterranean diet and exercise can reduce the risk of undernutrition and cognitive decline. In this study, 105 participants ≥60 years old who are at risk for undernutrition and with subjective cognitive decline will be divided into 3 groups: protein-enriched Mediterranean Diet + exercise (PROMED-EX), protein-enriched Mediterranean Diet alone (PROMED), and controls that receive standard care. 247 The PROMED-EX and PROMED participants will receive counseling, a diet guide, and a recipe book. For the first 3 months of the trial, key foods selected by the participants will be delivered to their homes to encourage the adoption of the PROMED diet. In addition, the PROMED-EX participants will receive a personal exercise prescription plan that includes strength, aerobic, core stability, and balance exercises designed for their ability. 247 The controls will receive general healthy eating diet information at the start of the study, and personalized advice will be provided at the end of the study. To the best of our knowledge, this is the first study to test a protein-enriched Mediterranean Diet on the risk of cognitive decline. By combining counseling, nutritional guidance, and exercise, the results from the PROMED-EX trial are anxiously awaited.
Conclusion
Maintaining brain health is essential to extending lifespan and living without comorbidities. In this review 7 lifestyle habits that were scientifically proven to promote brain health are explored. A well-balanced diet, particularly the Mediterranean, Nordic, and vegetarian diets, has been shown to support cognitive resilience and brain health. Physical exercise enhances neuroplasticity, hippocampal volume, and executive function while reducing dementia risk. Sleep plays a crucial role in memory consolidation and rejuvenation, including metabolic clearance, with chronic deprivation contributing to neurodegeneration. Persistent stress can lead to hippocampal atrophy and memory deficits, along with causing anxiety and depression, underscoring the importance of stress-reduction strategies such as mindfulness, meditation, cognitive-behavioral therapy, and social support. Social engagement mitigates loneliness and cognitive decline, while environmental exposures such as air pollution and risky behaviors such as alcohol consumption, smoking, and traumatic brain injury increase dementia risk. Cognitive reserve, built through lifelong learning and social interaction, provides resilience against neurodegeneration. Importantly, recent data supports the use of multidomain approaches to prevent chronic disease.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.