
Abstract
Body image and body appreciation (BA) are often considered a young adult issue, but the importance of body image as a factor contributing to wellness persists across the lifespan. The study’s purpose was to examine 1 the association between participation in a 3-month health-and-wellness coaching (HWC) program on BA and 2 whether baseline measures of physical and mental health were related to changes in BA. 100 women completed a 3-month HWC program where BA and mental and physical health measures were collected pre and post intervention. A stepwise linear regression was conducted using measures of physical and mental health with BA as the outcome. A higher level of baseline depression was linked to more improvement in BA post-intervention (β = 0.033, P < 0.05), while higher baseline muscular endurance was linked to less improvement in BA at post-intervention (β = −0.022, P < 0.01). Results suggest that a 3-month HWC program has potential for improving BA, with stronger results possible among women with higher levels of depression at the start of the intervention, however without a control group, causation cannot be established.
“Higher levels of baseline depression scores were linked to greater improvements in BA important in supporting the potential benefits of health wellness coaching.”
Background
Health and Wellness Coaching (HWC) is a patient-focused approach to preventing and mitigating chronic disease-related risk factors.1,2 Research has provided empirical support for some psychological and physical benefits associated with HWC for individuals with chronic lifestyle risk factors (e.g., sedentary, overweight/obese, physical inactivity) such as reduced cholesterol, increased physical activity, and decreased depression symptoms.2-4 A potential unexplored factor involved in understanding the relationship of HWC and mental health is body image, which is defined as an “individual’s cognitive or affective evaluation of their body or appearance with a positive or negative valence.” 5 Despite the potential benefits of HWC on various health outcomes, there has been limited examination of the factors involved in the relationship. Within a sport context, research has shown that coaches’ communication and behavior can be significantly related to athletes’ body image, either positively or negatively. 6 Considering the widespread prevalence of body image concerns, it’s crucial for research to explore whether HWC can play a role in promoting and supporting positive body image.7,8
Body appreciation (BA) is a significant public health concern due to its demonstrated associations with stress levels, self-rated health, and depressive symptoms. 9 These relationships are particularly prevalent among women.10,11 More specifically, women who are appreciative towards their body might be more prone to engage in behaviors that are health promotive, making body image important to overall health. 12 Individuals with low body image, and thus lower BA, have been found to have higher propensity for eating disorders, depression, and overall, report lower quality of life.13,14 While the benefits of HWC and healthy body image are promising, the relationship between HWC, health outcomes, and body image is not well understood, particularly among high-risk groups.
Body Image Among Adults
Many studies on eating disorders tend to examine an individual’s body image more from a negative perspective rather than a positive one.15-18 However, an increasing amount of literature draws attention to BA, the positive aspect of body image. BA has been described as holding favorable opinions of one’s body that is perceived as accepting and respecting the body. 19 BA is an important part of body image research because, with its strong mental and physical health correlates, it is a viable intervention target. 9 While recognition of the important role of BA is growing, the available research is not robust, especially in populations with chronic health conditions.
People who have greater BA tend to show positive connections with various aspects like body esteem, favorable body evaluation, and indices of psychological well-being (e.g., self-esteem, self-compassion, life satisfaction, proactive coping, and positive affect).9,19 High levels of BA in individuals are inversely related to body dissatisfaction, social physique anxiety, body shame, body surveillance, and body checking behaviors.19,20 Indeed, current evidence suggests there is an overall positive relationship between health promoting behaviors and BA.12,21,22 Individuals with higher BA are more likely to participate in preventative medical care and seek medical attention. 12 Additionally, BA is positively associated with self-perceived physical health and intuitive eating behaviors.22,23 There is some evidence linking physical health directly to BA, but only in young healthy populations. 22
A previous meta-analysis has discussed the relationship between HWC and obesity, heart disease, and overall wellness. 2 Similarly, systemic reviews have highlighted the positive benefits of HWC on obesity-related measures in participants, such as decreased weight, decreased waist circumference, and decreased caloric intake.2,24 Research found that HWC interventions targeting heart disease increased medication adherence, decreased hospitalizations, and increased positive mental health.25-27 Additionally, HWC has had positive associations on overall health. 2 Notably, none of these studies focused on measured muscular strength or endurance but rather focused on physical activity time.
Addressing Body Image Using HWC
Importantly, HWC has been identified as a patient-centered, collaborative approach utilizing behavioral strategies (e.g., motivational interviewing, positive psychology, and self-determination) that goes beyond averting and mitigating health-related risk factors and outcomes associated with the prevention and management of chronic diseases. 1 While there are some body image prevention and intervention programs that target adult female populations and address low BA, such interventions are limited in number and population diversity.28,29 Recent efforts have been made in female rheumatoid arthritis populations to reduce the prevalence of negative body image, particularly considering the influence of body functionality on adult’s self-perception of body image. 30 However, the impact of changes in overall BA scores on mental and physical health outcome measures has not been clearly established. Therefore, this study aims to determine how HWC impacts BA and to evaluate the connection between this change and the mental and physical health factors supported by HWC.
Current Study
The present study examines the use of HWC as a form of intervention to increase BA. 31 Building on previous interventions that specifically targeted BA, this intervention took a holistic approach to HWC, with coaches providing health screening, education, and goal setting in line with participant needs and preferences. This study fills a gap in the existing literature by increasing our understanding of the relationship between HWC and body image. Specifically, the present study 1 examined the relationship of a 3-month HWC program on BA and 2 assessed how change in BA score was related to physical and mental health at baseline. Our primary hypotheses were that 1: a HWC program would be related to a positive change in BA score, 2: high levels of anxiety or depression at baseline would positively affect this change, and 3: physical health status at baseline as measured by steps per minute and sit-to-stand would negatively affect the positive change in BA.
Methods
Participants
A total of 100 women aged 23 to 80 years old (M = 51.9, SD = 13.8) were included in the secondary analysis of women in the Montana Journey to Wellness. The participants in the Montana Journey to Wellness were recruited from a predominantly white population, with 89.9% identifying as White, 7.1% as American Indian or Alaska Native, and 3% as other. To be eligible to participate in the program, individuals must receive a referral from a medical provider and a diagnosis of one or more health-related chronic risk-factors or diseases (e.g., hypertension, obesity, type 2-diabetes). Recruitment materials were disseminated through word of mouth, e-newsletter across the hospitals, and medical provider offices.
Measures
Data capturing physical and mental health status were collected. Measures on physical health included the sit-to-stand test, the two-minute march test, body mass index (BMI, kg/m2), and body composition (% body fat). Measures on psychological health included depression, anxiety, and BA scores. Demographic information also was collected. Baseline (pre intervention), 3-month (post intervention) data, and consent to participate was collected via Qualtrics surveys.
Body Appreciation (BA)
The validated 13-item Likert-type scale was used to assess BA in participants. 18 Respondents were asked questions regarding their opinions on their bodies, with responses based on a 5-point-scale ranging from 1 Never to 5 Always. BA was indicated by the means of the items, with higher scores indicating higher levels of BA in participants. The Cronbach’s alpha reliabilities for BA was 0.93. 18
Anxiety
The 7-item General Anxiety Disorder-7 (GAD-7) scale was utilized to assess participants’ anxiety at baseline. 32 Respondents were asked about their recent experience of anxiety symptoms. Responses were provided using a 4-point-scale ranging from (0) not at all to 3 nearly every day. Anxiety was indicated by the sum of the 7 items, resulting in a score between 0 and 21.30,31 We utilized the established cutoffs to identify different levels of anxiety.32,33 More specifically, a score of 0-4 was considered minimal anxiety, a score of 5-9 was considered mild anxiety, a score of 10-14 was considered moderate anxiety, and a score of 15 or above was considered severe anxiety. 31 The Cronbach’s alpha reliability for GAD-7 was 0.89.32,33
Depression
The validated 9-item depression scale, Patient Health Questionnaire-9 (PHQ-9), was used to measure depression in participants. 34 Respondents were asked recent frequency of depressive symptoms. Responses were provided using a 4-point-scale ranging from (0) not at all to 3 nearly every day. The responses of the 9 items were summed, with a maximum score of 27 points. A score of 10 or higher was considered mild major depression; a score of 15 or higher indicated moderate major depression, and a score of 20 or higher indicated severe major depression. 35 The Cronbach’s alpha reliabilities for PHQ-9 was 0.89. 36
Sit-to-Stand
The sit and stand test were used to assess leg strength, endurance, balance, and overall physical activity level. It is a physical performance test where participants go from a seated position to a standing position repeatedly for 20 seconds.37,38
Two-Minute Step
The two-minute step test is an exercise capacity test that requires the participant to march in place as fast as they can while raising their knees to a height midway between their patella and iliac crest when standing.38,39 A systematic review of functional capacity exercise tests found that higher scores on the two-minutes step are a marker of higher activity and fitness level. 40
Body Mass Index
The Body Mass Index (BMI) is a ratio of a participant’s weight to height squared. BMI has historically been used to assess an individual’s risk of weight related illnesses. 41 Although BMI fails to distinguish between body fat, muscle mass, or bone, it is a well-accepted marker to identify increased risk of obesity-related disease, health conditions, and mortality, specifically with a BMI ≥30.0 kg/m2. 42
Body Composition
Body fat percentage was measured using the Tanita BIA-bioelectrical impedance analysis 570 (Tanita, Tokyo Japan). Bioelectrical impedance has been found to be a valid form of body fat percentage measurement in comparison to other methods like skinfold fat and hydrostatic weighing.42-44
Demographics
Age and ethnicity were acquired using self-reported data collected at baseline.
Procedure
The Montana Journey to Wellness program was informed by an existing coaching program, Journey to Wellness, which is based on HWC concepts. 31 The program provides opportunities for exercise and education on nutrition, disease management, stress management, and risk factor modification. All coaches were Wellcoaches certified® wellness coaches (https://www.wellcoaches.com/) with at least one year of coaching experience and a bachelor’s or advanced degree in a health-related field. Health and wellness coaching incorporates motivational interviewing, mindfulness, goal setting, visioning, positivity, and participant accountability.2,45,46 Participants had access to bi-weekly 30-45-minute coaching sessions, based on their individual needs. While the primary focus of these sessions was physical activity and exercise training; goals, plans, and coaching session content was tailored to each participant following the initial intake visit. BA was not a formal focus of the intervention or coaching sessions, but data at pre and post intervention was collected. Baseline and post program information was collected during two 90-minute coaching sessions.
Statistical Analysis
Participant information was collected using Qualtrics (Qualtrics, Provo, UT), while the analysis was conducted using RStudio (RStudio, Boston, MA). Before analysis all data collected was checked for missing and outlier values, and normality. Descriptive statistics were run for all continuous variables. For any categorical variables frequencies were run. Less than 3% of data used for analysis was missing at random, therefore no data was imputed. 47 To ascertain the change in BA following HWC, paired t-tests were conducted. To further examine the association between physical health and mental health on the changes in BA, multiple statistical procedures were conducted. First, the change in BA for each participant was calculated. Next, correlations between physical health measures, mental health measures, and changes in BA were conducted. Finally, stepwise, step-backwards, and step-both linear regressions were conducted, with change in BA as the dependent variable, and health measures as independent variables to select dependent variables for the final model. 48 Only variables with P < 0.05 were included in the final model.
Results
Descriptive Statistics and Correlation to Change in BA of Dependent Variables.
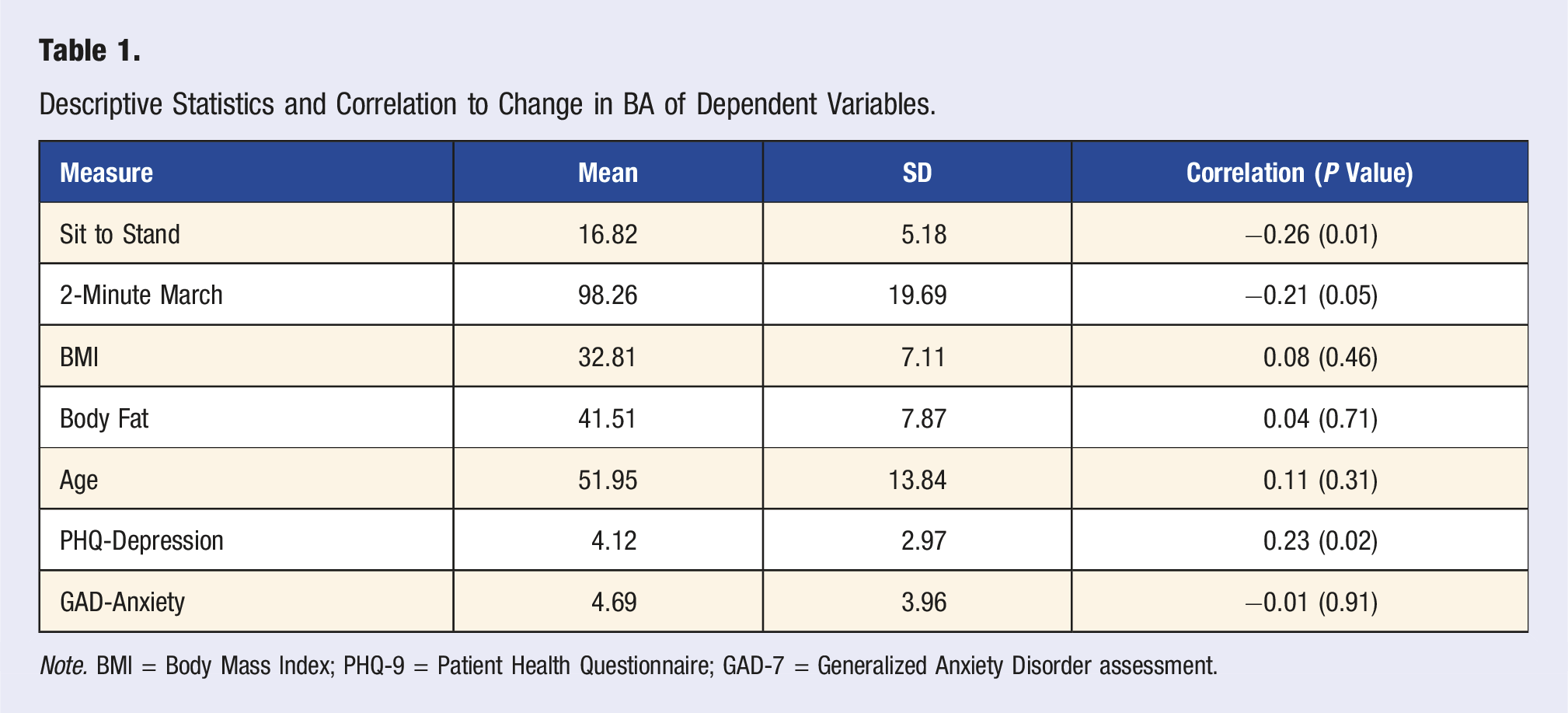
Note. BMI = Body Mass Index; PHQ-9 = Patient Health Questionnaire; GAD-7 = Generalized Anxiety Disorder assessment.
Total Linear Regression.
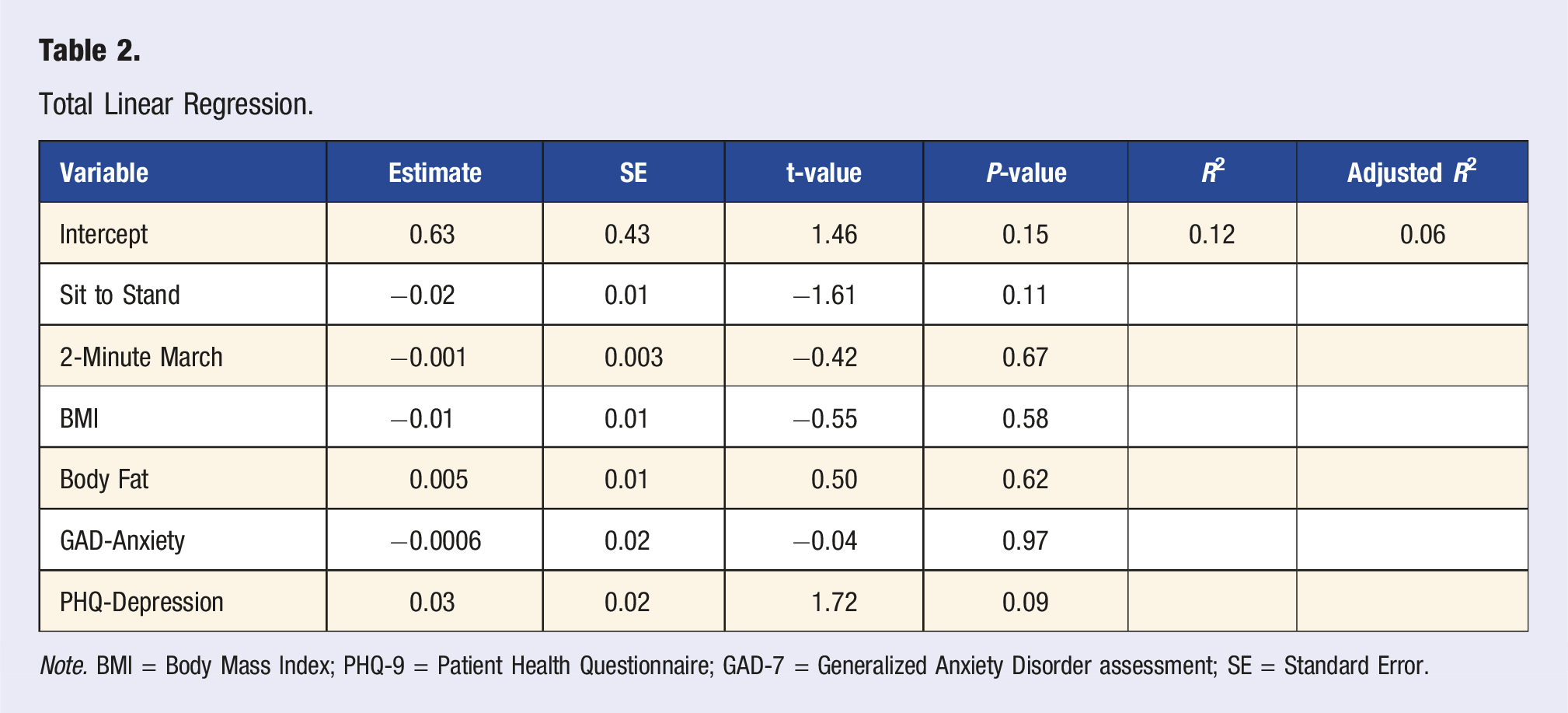
Note. BMI = Body Mass Index; PHQ-9 = Patient Health Questionnaire; GAD-7 = Generalized Anxiety Disorder assessment; SE = Standard Error.
Final Regression Model.
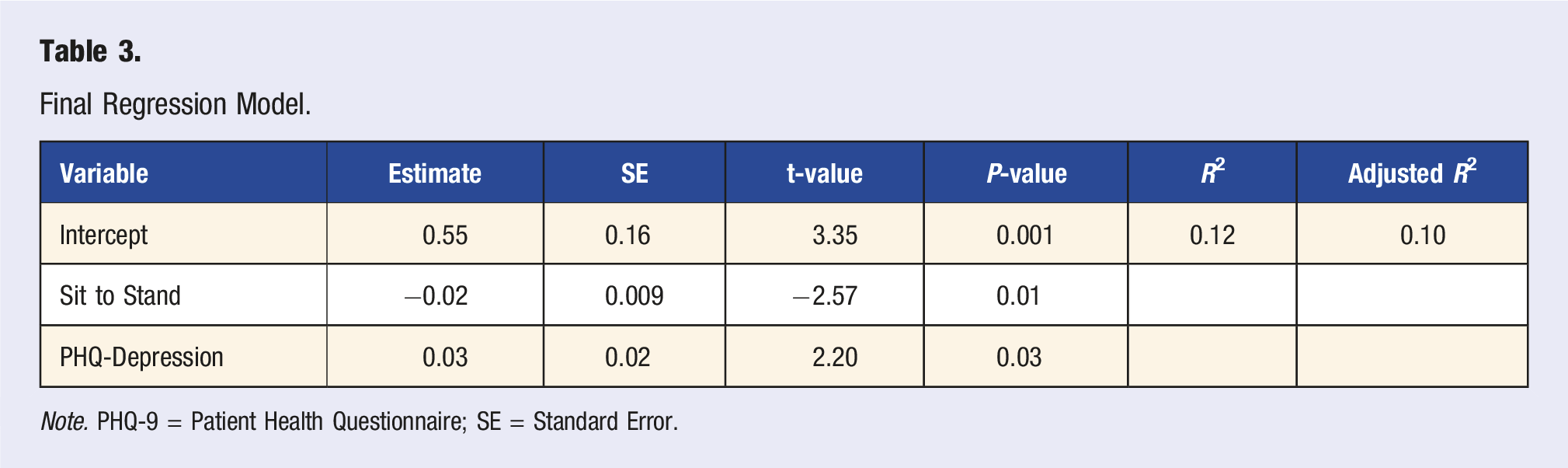
Note. PHQ-9 = Patient Health Questionnaire; SE = Standard Error.
Discussion
The overall goal of this study was to increase our understanding of the relationship between HWC and BA. Our team examined (1) the relationship between participation in a 3-month HWC program and BA and (2) how the change in BA score was related to physical and mental health at baseline. There were two key findings. First, participation in the HWC program was associated with increases in participants’ body appreciation. Second, higher levels of baseline depression scores were linked to greater improvements in BA important in supporting the potential benefits of health wellness coaching. However, without a control group, we cannot determine whether observed changes in BA were specifically due to the HWC intervention, or to natural changes or unmeasured factors. Future controlled studies are necessary to establish whether HWC causally improves body appreciation.
Findings from the step-backwards linear regression suggest that women with higher baseline depression may be particularly responsive to HWC interventions, though the mechanisms underlying this association remain unclear. The baseline depression finding indicates who may benefit most from HWC participation but does not explain how or why the intervention works. Potential mediating pathways—such as improved self-efficacy, reduced negative self-talk, or enhanced social connection, should be examined in future research to establish what aspects of participation in HWC programs lead to changes in BA.49-51
Results of the paired t-test found that there was a significant change in body appreciation in participants between baseline and post intervention timepoints. Given that BA is measured on a 5-point scale, the 0.36-point increase represents approximately a 7% improvement. However, as acknowledged in our limitations, the BA scale lacks established clinical significance thresholds. This effect size is comparable to other interventions specifically targeting body appreciation, which typically have reported small-to-medium effect sizes. 52
HWC has been shown to have positive effects on overall wellness in chronically ill populations such as those with heart disease, diabetes, and rheumatoid arthritis but current literature lacks a psychological perspective.25-27,29,53 These studies focused on measures of disease, medication compliance, and overall measures of health. Of note, none of these studies measured BA. If body image is part of wellness, as suggested in studies like those conducted by El Ansari et al (2014) and Becker et al (2019), the results of this study are in line with previous literature that find that interventions had a small magnitude.10,30,53 It is suggested that more concrete work surrounding body image and general wellness be conducted.
To our knowledge there is no prior published study on the relationship between participation in a HWC program, BA, and functional physical health measures such as muscular or cardiovascular endurance (i.e., sit-to-stand and 2-minute march test). Given the current evidence on the positive benefits of physical activity behaviors that result from HWC-focused programs, our findings highlight that adults also accrue benefits that promote healthy reflection in a manner that promotes more positive appreciation. This is important because evidence suggests a relationship between body dissatisfaction and lower reported quality of life, higher rates of eating disorders, and higher rates of depression.13,14 Results of the stepwise linear regression suggest that women with higher muscular endurance at baseline experienced less improvement in body appreciation throughout the intervention. While this finding may seem contradictory to expectations, one possible explanation is a ceiling effect—participants with greater physical fitness may have already had relatively high body appreciation scores, leaving less room for measurable improvement. Previous research has shown a positive relationship between strength training and body appreciation, indicating that individuals who feel physically strong often report higher BA. 54 Therefore, it is possible that those with higher muscular endurance entered the program with elevated body image perceptions, resulting in smaller observed changes during the intervention.
Several implications can be drawn from the findings of this study. First, the experience of chronic illness may have a negative impact on people’s self-concept, as they experience such things as pain, discomfort, weight gain, changes in appearance, and a loss of control over their own bodies. The social stigma that comes along with illness may lead to other psychological destructive behaviors that impact self-esteem, loss of control over body and emotions, and/or feelings of personal failure.55-57 Nonetheless, as more findings become available on understanding how to promote positive health behaviors through health and wellness coaching, the importance of BA will remain an important area to explore and understand among middle-aged to older women at-risk for or with chronic health illness.
The Montana Journey to Wellness was a rural-focused intervention that focused on two geographically isolated communities that have large rates of uninsured, unemployed, and individuals living on the poverty line. To our knowledge, we have not identified other HWC programs that have conducted this collaborative approach to provide access and professional health services in adults at risk for chronic illness. The combined exploration of psychological and physical health measures, highlighting BA as an important factor, is also unique to this body of work within the HWC literature that may lead to other important research areas to explore.
In addition to the strengths of this study, the results must be interpreted within the study limitations. Limitations of this work include a lack on generalizability due to convenience sampling. This intervention did not include a control group, so we are unable to ascertain how effective the HWC intervention is compared to other interventions or no interventions. Additionally, this study only included chronically ill women in a rural setting, limiting the generalizability of the intervention to other populations. Furthermore, while the Body Appreciation Scale shows a positive upwards trend, it currently lacks a clinical significance scale, making it difficult to determine the practical or clinical importance of the observed changes in BA.
Conclusion
Results found that participation in a remote HWC program may improve body image, particularly among middle-aged and older adults with limited access to wellness resources. Our findings highlight that depression and physical fitness are key factors influencing the experienced changes of those within the HWC program, and women with higher initial depressive symptoms experienced the greatest improvements. The success of this program, delivered remotely and as an extension of an existing initiative, demonstrates its adaptability for diverse settings such as gyms, schools, and medical facilities. These results underscore the potential of HWC programs to address often-overlooked body image concerns in later adulthood and warrant further investigation through controlled trials.
Footnotes
Acknowledgments
We would like to acknowledge The Summit Medical Fitness Center from Logan Medical Health Care Center, Clark Fork Valley Hospital, and the Northern Rockies Medical Center for their collaboration and contribution of health and wellness coaches at each rural site within Montana. We would like to express our gratitude to the professional, certified health and wellness coaches leading within each site, for their passion, collaboration, and implementation of Montana Journey to Wellness, including but not limited to Catherine Lisowski, Michele Maher, Toni Altenburg, Aria Mangan, Sonya French, Holly Nickels, and Greg Vanichkachorn. Lastly, this project would have been possible without the funding award received from the HRSA Rural Health Care Services Outreach Grant, HRSA-18-030.
Author Contributions
Kathleen N Heeter—Conceptualization; Formal Analysis; Writing—Original Draft; Writing—Review and Editing
Kyle A. Kercher—Writing—Review and Editing
Jonathan T. Macy—Writing—Review and Editing
Angela Chow—Writing—Review and Editing
Brad Roy—Funding acquisition, Project Administration, Writing—Reviewing and Editing
Vanessa M. Martinez Kercher—Data curation, Funding acquisition, Writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bureau of Health Workforce; 5-d04-20-001.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.