
Abstract
Purpose
Chronic diseases contribute to high death and disability rates around the globe. Rural areas of the southern United States have limited resources and disproportionately worse health outcomes, and increased prevalence of modifiable disease risk factors. The purpose of this study was to evaluate the effects of an online lifestyle medicine program on the dietary and social support health behavior determinants of rural adults.
Design
A randomized controlled trial was conducted to test the lifestyle medicine intervention among rural participants (n = 80) randomized to either an intervention (n = 40) or waitlisted control (n = 40) group. Participants in the intervention group received a lifestyle medicine program via an online group-based format.
Results
Data were analyzed using mixed-effects models for repeated-measures (MMRM) to evaluate intervention effects over time. The analysis showed significant intervention effects for primary outcomes regarding dietary produce health behavior determinants and secondary social support outcomes. The intervention, or experience over time, may have shifted certain behaviors and knowledge domains.
Conclusion
Participants of the web-based lifestyle medicine intervention had positive improvements in dietary and social support determinants of health behaviors. The results can facilitate future intervention development and implementation among rural populations.
“For most of the social support subscales, the intervention group showed greater improvements in scores across time points.”
Background
Chronic diseases impact public health by attributing to 43 million deaths globally, requiring ongoing medical treatment, limiting daily activities, and contributing to disability and rising healthcare costs.1-3 In the United States, cardiovascular disease, diabetes, and cancer are the leading causes of death, and the prevalence of these conditions is high as more than half of adults have been diagnosed with at least one chronic disease and just under half are managing two or more.1,4 Although medical advances have progressed to improve treatment options and contribute to longer lifespans, investment in prevention is minimal, and chronic disease rates are projected to rise, especially in underserved areas.2,5,6 For example, rural populations have limited access to healthcare and preventive health services and resources while simultaneously bearing a disproportionate and persistently increasing burden of chronic diseases.7-9 Such disparities have been associated with increased prevalence of behavioral risk factors as people living in rural areas are more likely to use risky substances, have a poor diet, get insufficient sleep, and be overweight and physically inactive.7,8,10
Health behaviors have several multi-faceted and interactive factors that vary throughout the life course. The Theory of Planned Behavior explains that psychosocial determinants, including attitudes, norms, perceived behavior control, and intentions, have crucial roles in shaping lifestyle choices and behaviors. 11 Attitudes involve personal values and intrinsic beliefs about health behaviors while norms are personal perceptions about what significant others, such as family members and friends, think should be done regarding lifestyle choices along with individual motivations to comply. 11 The findings of a qualitative study involving rural participants of a nutrition and cooking intervention indicated that subjective norms were mostly influenced by family members and further motivated by traditional cooking methods, highlighting the importance of family in dietary behaviors. 12 Perceived behavioral control is described as personal belief regarding ability to perform recommended health behaviors and include perceptions about ease and difficulty in carrying through. 11 For example, the affordability of food and concerns about wasting food can diminish perceived behavioral control about diet, especially for people having lower socioeconomic status, and facilitators include affordable ingredients that are locally available. 12 The interplay among attitudes, norms, and perceived behavioral control helps form decisions that motivate lifestyle changes and develop intentions which are antecedents of health behaviors. 11
Social support is a notable protective factor that plays a role in shaping health behaviors, reducing disease risk, buffering stress, and enhancing resilience, leading to improved relationships and resource sharing that collectively impact health.13-15 In fact, higher levels of social support are inversely associated with lower chronic disease rates. 14 Social support fulfills belongingness needs, enhances coping, and reduces stress levels and related contributory health issues.16-18 The four defining attributes of social support that are facilitative toward healthier behaviors include emotional, instrumental, informational, and appraisal support. 19 Within the context of social networks, emotional support encompasses the provision of caring and trust, and instrumental support involves tangible resources. 19 Informational support comprises information provided to people that can facilitate problem-solving, and appraisal support provides information to promote affirmation. 19
Interventions that influence attitudes, norms, and perceived behavior control may positively impact intentions that lead to sustainable health behavior modifications and reduce chronic disease risk. The American College of Lifestyle Medicine (ACLM) recommends reducing chronic disease development and exacerbation based on the six pillars consisting of regular physical activity, plant-based diet, adequate sleep, stress management, avoidance of risky substances, and positive social networks.20-24 Previous research has shown that interventions using a lifestyle medicine approach are cost-effective and can facilitate modification of unhealthy behaviors and reverse disease development and progression.1,6,25-28 However, studies have tested the effects of lifestyle medicine interventions mostly on dietary and physical activity outcomes among primarily urban populations.29-32
The impact and efficacy of lifestyle medicine programs have not been adequately explored among rural populations where resources are limited and outcomes are among the worst. This information can facilitate the development of targeted programs that address modifiable chronic disease factors and enhance overall health. Therefore, the purpose of this analysis was to evaluate the effects of an online group-based lifestyle medicine intervention among rural adults by determining the impact on dietary produce determinants, including attitudes, norms, perceived behavior control, and intentions, and examining social support factors associated with improving dietary and physical activity behaviors. Reporting for this randomized controlled trial adhered to the CONSORT-SPI guidelines. 33
Methods
The theoretical framework that guided the study was the Integrated Model of Behavioral Prediction (IMBP) which expands upon the Theory of Planned Behavior and describes that health behaviors are influenced by intentions along with environmental constraints and skills, such as necessary knowledge and abilities to engage in lifestyle recommendations.11,34 Intentions are influenced by attitudes, norms, and perceived behavioral control which are, in turn, affected by distal variables, such as past behavior, perceived risk, culture, media, and health programs.
34
However, in addition to influencing intentions, perceived behavioral control, or belief in one’s own ability to perform the recommended behavior, independently predicts actual behaviors.
34
For example, higher levels of perceived behavioral control are associated with increased likelihood of successfully performing a recommended health behavior. CONSORT 2025 flow diagram.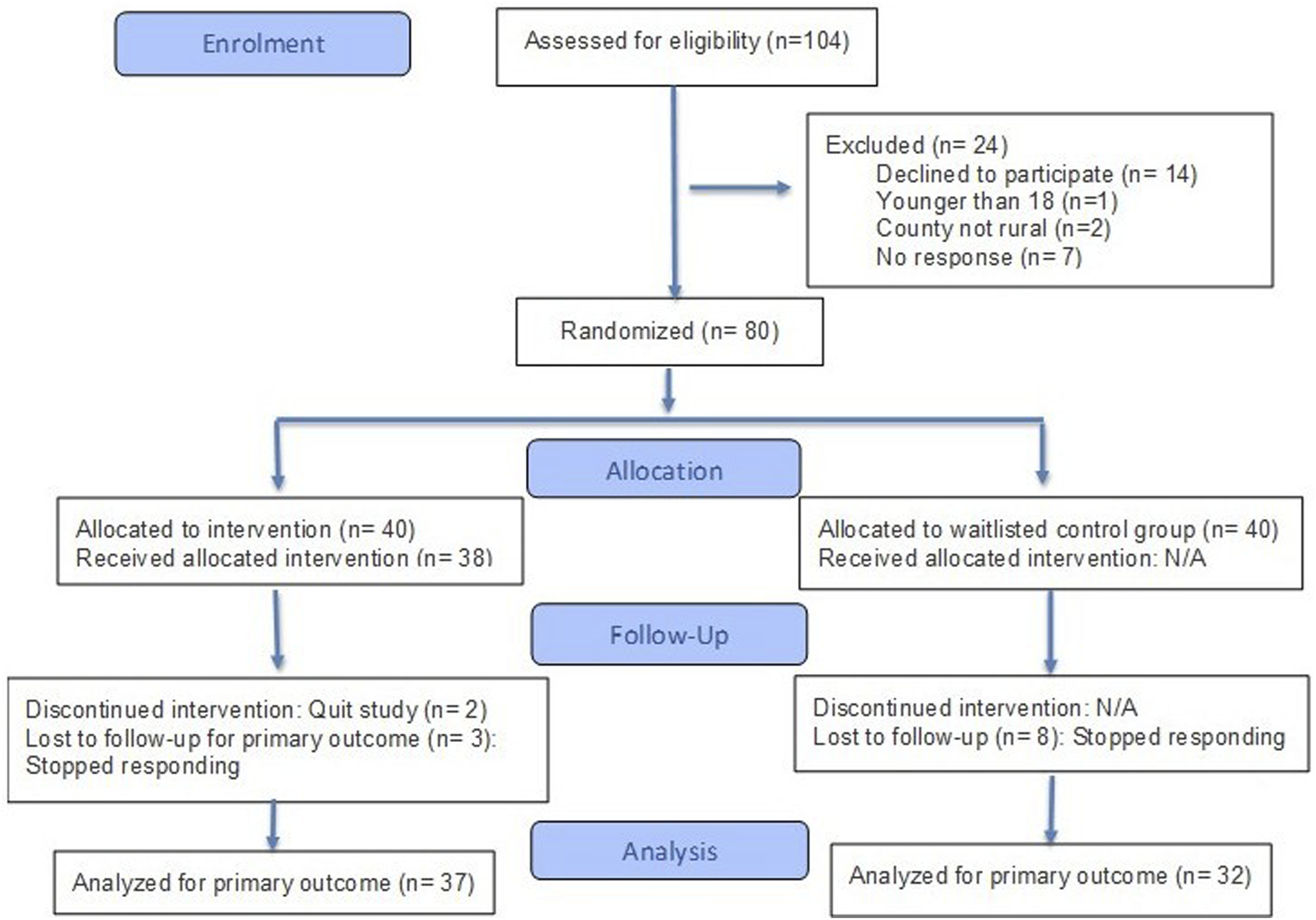
Design and Sample
A pilot randomized controlled trial was used to evaluate the effect of an online group-based lifestyle medicine program on dietary health behavior determinants (attitudes, norms, perceived behavioral control, and intentions) and social support among rural adults in the southeastern United States. The study began in September 2022 and ended in May 2024. Using mixed-effects models for repeated-measures (MMRM), we calculated power using the approach of Lu, Luo, and Chen 35 as implemented in the longpower package. Assuming a two-sided α = .05, four waves of data with unstructured within-subject correlation, heterogeneous residual variances, and observed retention, a total of ≈57 participants (28 per group) would be required to detect a 2-point difference on the primary outcome with 80% power. With our achieved N = 80 (40 per group) sample, the study retained >90% power to detect a 2-point difference and maintained ≥80% power for differences as small as ∼1.75 points, representing the minimal detectable effect size under our analytic design. We targeted a 2-point difference on this scale as a clinically meaningful, distribution-based effect corresponding to a small-to-moderate standardized change (∼0.3-0.5 SD) commonly used in behavioral trials to denote meaningful improvement in proximal psychosocial determinants. These calculations account for all available data under missing-at-random assumptions through full-information maximum likelihood (FIML) and are therefore consistent with our analytic strategy and the results from a similar study and intervention. 36
After the study received institutional review board (IRB) approval from Florida State University, potential participants were recruited from public and community areas in rural counties as determined by Rural Urban Continuum Codes (RUCC). 37 Recruitment methods included active recruitment in rural housing and public areas and passive recruitment using posted flyers in clinical and community settings and advertisements in local newspapers and social media platforms. Eligible participants could speak, write, and understand English, were at least 18 years of age, resided in a rural southern county, had access to a computer with internet service or smartphone with cellular data, and had at least one chronic disease risk factor or diagnosis, including prediabetes, overweight, smoking, hypertension, chronic disease family history, and elevated cholesterol. After providing informed consent, participants were randomized to either an intervention or waitlisted control group using a random number table sequence generated by a computer (Figure 1). The parity of the 5-digit numbers in the sequence determined the allocation of participants to either the intervention (even parity) or waitlisted control (odd parity) group. The beginning random number sequence was randomly selected from the table and was checked to ensure the parity imbalance did not exceed 2. Participants and study personnel were aware of group allocation to either the intervention or waitlisted control group, and no masking of group assignment was done.
Measures
Participants in both intervention and waitlisted control groups completed a baseline survey that collected information about sociodemographic characteristics and risk factors. The baseline and study outcome surveys were completed online by both groups. Participants in the intervention group completed surveys online at baseline, post-intervention, one month after post-intervention, and 6-month post-intervention. Participants in the waitlisted control group completed the same surveys online at similar time points. A research assistant telephoned participants in the event of inadvertently missed survey items, and participants received a gift card incentive after completing online surveys at each time point.
The instruments used to measure outcomes for this study were consistent with the major components of the theoretical framework used to guide the study: attitudes, norms, perceived behavioral control, and intentions. 34 The measures were deemed reliable and valid from previous research. The 5-a-Day Questionnaire measured the primary study outcome regarding dietary produce determinants consistent with recommendations for consuming a more plant-based diet. The 12-item scale had good internal reliability for attitudes (α = .79), norms (α = .77), perceived behavioral control (α = .81), and intentions (α = .74) when tested in a similar population. 38 The range of possible scores for each subscale varied regarding attitudes (4-28), norms (3-21) and perceived behavioral control (3-21), and intentions (2-14). We designated the produce attitudes subscale of the 5-a-Day Attitudes instrument as the primary outcome, with the remaining seven psychosocial and social support measures analyzed as secondary outcomes. The Social Support to Eat Better and Move More (SSEBMM) instrument was used to measure secondary outcomes of social support in dietary and physical activity health behavior changes. 39 The 10-item scale had excellent reliability overall (α = 0.96) and for the informational support (α = 0.97), emotional support (α = 0.96), and encouragement (α = 0.97) subscales. 39 The ranges for the subscales were informational support (3-21), emotional support (4-28), and encouragement (3-21). For all measures, higher scores indicate better outcomes.
Intervention
Participants randomized to the intervention group received six group-based educational sessions delivered via Zoom application by a registered nurse interventionist using an online multimedia format with interactive strategies to promote evidence-based content delivery as well as engagement and discussion. The sessions lasted approximately 90 minutes each and consisted of information about chronic diseases such as cardiovascular disease, diabetes, and stroke to facilitate understanding and provide context. Each Zoom session also addressed at least one chronic disease risk factor consistent with the six ACLM pillars. 20 For example, sessions promoted healthy dietary patterns, such as eating a plant-based diet, reducing cholesterol and sodium intake, reading food labels, and choosing healthy foods when shopping on a budget or dining out. Other sessions addressed strategies for reducing stress, being physically active, improving sleep habits, embracing social support interactions with family and friends, avoiding being overweight or obese, and quitting or never starting harmful substances. The sessions also included rationales to help participants understand linkages between health behaviors and chronic diseases and interactive discussions about rural sociocultural context and ways to overcome rural challenges and motivate healthier choices. During and after the sessions, participants had the opportunity to ask questions and discuss content topics, if desired, with the interventionist and each other. Participants also received text messages as well as handouts each week by email that reinforced the educational material provided during the sessions. The waitlisted control group participants received the intervention sessions once data collection was completed across the four time points.
Analytic Strategy
Data were analyzed using SPSS Version 29.0. Prior to hypothesis testing, descriptive statistics were computed for all study variables. Group differences in baseline demographic characteristics were assessed using independent-samples t-tests for continuous variables (e.g., age) and chi-square tests for categorical variables (e.g., gender, education, and race). When assumptions of normality or expected cell counts were not met, nonparametric alternatives (e.g., Mann–Whitney U tests) were employed, and effect sizes (e.g., Cohen’s d, Cramér’s V, or Hedge’s g) were reported to quantify group differences. We used Little’s MCAR test to evaluate the plausibility of missing completely at random (MCAR) across outcomes. Because MCAR is a stricter condition than the missing-at-random (MAR) assumption required for full-information maximum likelihood, non-significant results support MCAR, while significant results indicate only that MAR remains the more realistic assumption.
To evaluate the effects of the intervention over time, a series of mixed-effects models for repeated-measures (MMRM) were estimated across eight outcome variables: produce attitudes, subjective norms, perceived behavioral control, behavioral intentions, informational support, emotional support, encouragement, and social support for dietary and physical activity behaviors. Each MMRM analysis included one within-subjects factor (Time: T1–T4), one between-subjects factor (Group: intervention vs waitlisted control), and race as a covariate (to account for group inequivalence with this factor). Unlike traditional repeated-measures general linear models, which requires complete cases and assumes sphericity, MMRM provides greater flexibility by modeling within-subject correlations directly. MMRM also estimates model coefficients using full-information maximum likelihood (FIML) estimation, which accounts for all available data and reduces bias from missing observations by incorporating participants’ partial outcome trajectories. Main effects of time, race, group, and Group × Time interactions were examined for each construct. Partial eta-squared (η2) was used to estimate effect sizes for within-subjects and interaction terms. Semi-partial r2 values were used to estimate effect sizes for fixed effects, and estimated marginal means and standard deviations were examined to interpret the direction and magnitude of observed effects. Significant Group × Time interactions indicated differential change trajectories attributable to intervention exposure, while main effects reflected overall shifts in outcomes across the sample. Where appropriate, follow-up comparisons of estimated marginal means across time points were reviewed to clarify temporal trends within each group. Because two sets (i.e., “families”) of four outcome variables were examined, the overall Type I error rate may be inflated above the nominal α = .05. Analyses designated produce attitudes as the primary outcome with remaining outcomes as secondary. Secondary endpoints were grouped a priori into construct families that share theory and measurement (behavioral determinants: norms, PBC, intentions; social support: informational, emotional, encouragement, and composite). Because endpoints within a family are correlated, we evaluated multiplicity within families using Bonferroni-adjusted α = .0125 (four families). This approach controls the relevant family-wise error while avoiding over-penalization from treating correlated outcomes as independent; all findings remained significant under this conservative check.
Results
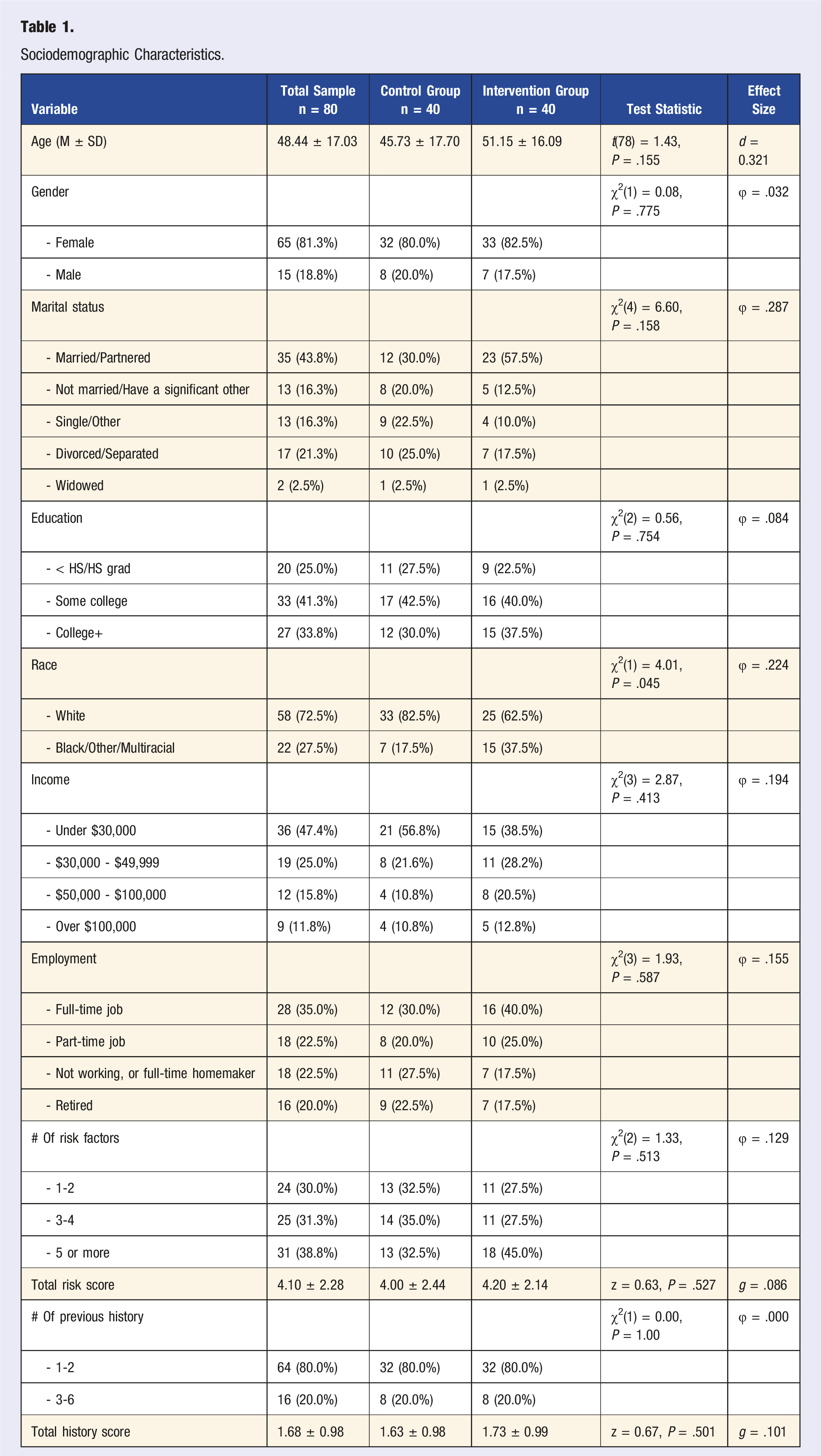
Sociodemographic Characteristics.
Attrition for the primary outcome (produce attitudes at T4) was 17.5% in the control group (7 of 40) and 7.5% in the intervention group (3 of 40). This difference was not statistically significant (χ2 = 1.83, df = 1, P = .18; Fisher’s exact P = .31). To further evaluate missingness, we conducted Little’s MCAR tests across outcomes. Results suggested that some outcomes were consistent with MCAR (e.g., social norms: χ2 = 8.63, df = 8, P = .37; perceived behavioral control: χ2 = 8.33, df = 8, P = .40; intentions: χ2 = 7.56, df = 8, P = .48; encouragement: χ2 = 13.46, df = 8, P = .10), while others rejected MCAR at the α = .05 level (produce attitudes: χ2 = 18.15, df = 8, P = .02; informational support: χ2 = 18.16, df = 8, P = .02; emotional support: χ2 = 15.75, df = 8, P = .046; SSEBM total: χ2 = 16.12, df = 8, P = .041). Because MCAR is a stricter condition than MAR, and attrition was modest and not significantly different across groups, we conclude that MAR remains a plausible assumption for the FIML approach used in our multilevel models.
Group Equivalence
Between-group comparisons revealed no statistically significant differences in age, gender, education level, marital status, income, employment status, or number of risk factors. Participants in the intervention group were slightly older on average (M = 51.15, SD = 16.09) than those in the waitlisted control group (M = 45.73, SD = 17.70), although this difference was not statistically significant. Race was the only variable to show a statistically significant difference between groups as 82.5% of participants in the waitlisted control group identified as White compared to 62.5% in the intervention group. Race was subsequently added to MMRM analyses as a covariate to account for group inequivalence. No other significant group differences were observed in the number or severity of risk or history scores, including total risk and total history.
Dietary Produce Outcomes
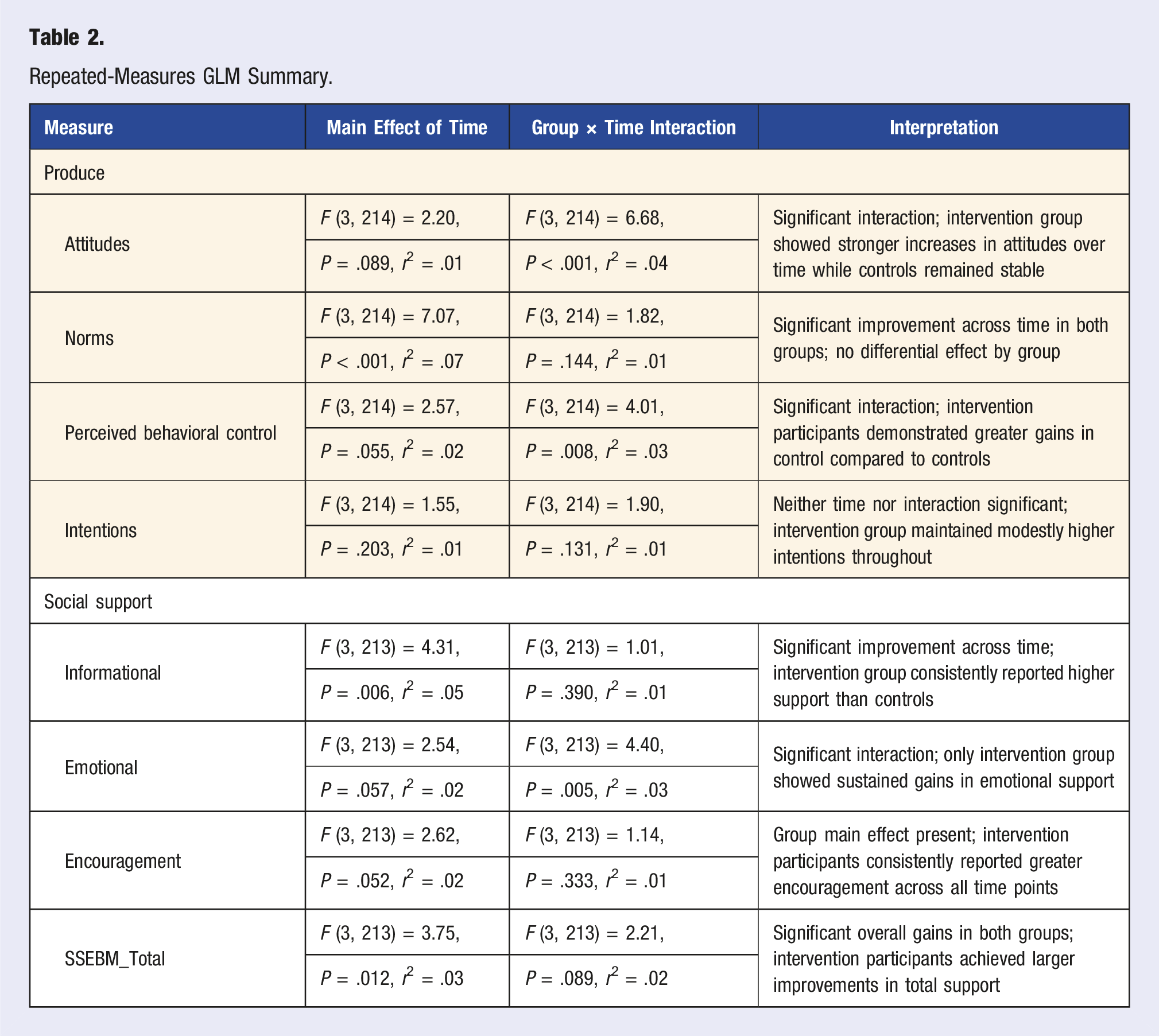
Repeated-Measures GLM Summary.
Support Outcomes
The intervention group showed greater gains over time than the waitlisted control group in emotional support, encouragement, and social support, with both reaching or approaching significant Group × Time effects. Race was included as a covariate in all models. Informational support revealed significant main effects of group (P = .039) and time (P = .006), with intervention participants reporting higher scores from T1 (M = 16.20, SE = 0.89) to T4 (M = 18.70, SE = 0.76), compared to the waitlisted control group (T1 M = 15.80, SE = 0.93; T4 M = 16.70, SE = 0.84). Emotional support showed a significant Group × Time interaction, (P = .005), with intervention participants showing steady increases (T1 M = 21.80, SE = 1.15; T4 M = 25.40, SE = 1.07), while the control group remained flat or declined slightly (T1 M = 21.40, SE = 1.21; T4 M = 20.90, SE = 1.15). For encouragement, a significant group main effect was observed (P = .006), with intervention participants consistently reporting higher scores across all time points (T1 M = 17.20, SE = 0.87; T4 M = 19.30, SE = 0.67) relative to controls (T1 M = 16.50, SE = 0.91; T4 M = 17.00, SE = 0.74). Finally, total scores for the SSEBMM scale demonstrated a significant main effect (P = .018) and time effect (P = .012). The intervention group improved substantially from T1 (M = 55.20, SE = 2.79) to T4 (M = 63.40, SE = 2.41), whereas the waitlisted control group’s change was minimal (T1 M = 53.70, SE = 2.94; T4 M = 54.70, SE = 2.64).
Discussion
Public health programs that address multiple risk factors are scarce in rural locations, and little is known regarding the impact of lifestyle medicine interventions on rural populations. This study helps to bridge this gap and provides information about the effects of an online group-based lifestyle medicine intervention on southern rural participants’ attitudes, norms, perceived behavioral control, intentions and social support. The Integrated Model of Behavioral Prediction framework used to guide the study explains that these determinants are antecedents of health behavior changes. 34 The findings showed a significant intervention effect for attitudes and perceived behavioral control regarding plant-based dietary recommendations and a significant time effect for norms. Although norms and intentions did not show a significant intervention effect, the intervention group had greater improvements than control. Emotional support associated with dietary and physical activity changes also improved. The increases in scores for these variables were indicative of changes in intensity across time points. The intervention, or the experience over time, may have enhanced awareness or shifted certain behaviors and knowledge domains.
The participants in the intervention group showed improved attitudes about consuming produce and moving toward behavior changes regarding plant-based dietary recommendations. There were statistically significant time effects for norms regarding consuming recommended daily servings of produce and leaning toward a plant-based diet. Although there were improvements in the norms of those in the intervention group, the increases in scores shown by the control group over time may have been related to the question-behavior effect, similar to the Hawthorne effect, from study participation and answering survey questions about eating fruits and vegetables. 40 Since norms are influenced mostly by family members, 12 actively involving family members in health behavior interventions may be crucial for future intervention planning and success. For example, in a qualitative study of rural heart failure patient-family caregiver dyads, family caregivers reportedly cooked diet-appropriate meals and helped with purchasing healthy, low-sodium foods. 41 Further, cultural differences may influence the impact of lifestyle interventions. Previous research showed improved attitudes, norms, perceived behavioral control, and intentions among rural African Americans after participating in a cardiovascular health promotion intervention. 42 In comparison, a study among urban Iranian participants of an educational disease reduction intervention showed improved norms, perceived behavioral control, and intentions, but not attitudes. 43
The Integrated Model of Behavioral Prediction explains that, similar to attitudes and norms, perceived behavioral control influences intentions, but an important difference is that perceived behavioral control also directly and independently influences health behaviors. 34 The findings of this study indicated that participation in the intervention facilitated statistically significant changes in perceived behavioral control for the intervention group participants compared with those in the control group. In previous research, perceived behavioral control was deemed an important predictor of dietary and physical activity health behavior changes and intentions.44,45 Although there were no statistically significant effects for produce intentions, the intervention group showed improvements in scores from baseline to the 6-month post-intervention time point while the control group stayed relatively the same with a slight decrease in scores from baseline. Although intentions to adopt healthier behaviors may be sincere, barriers faced by people living in rural areas can hinder translation into action. Rural areas have greater barriers to health care access that, in addition to having fewer healthcare facilities and providers, factors such as lower percentages of car ownership and having to travel longer distances to health services and pharmacies also impede optimal health and well-being.41,46
For most of the social support subscales, the intervention group showed greater improvements in scores across time points. For informational support, there was a significant time effect but no interaction effect. However, the statistically significant interaction effect noted for emotional support indicated that the intervention promoted improvements for the intervention group while the control group scores stayed relatively the same or slightly decreased. The intervention group also showed higher scores for the encouragement subscale and total for the social support measure. Social support networks help shape health behaviors, but they can vary among rural groups. 47 Informal social support systems, including family and friends, are typically perceived as strong in rural communities although some may display within-rural differences. 48 However, the limited access to preventive health educational programs in underserved areas impacts the availability of evidence-based and current health recommendations to maintain healthy lifestyles.9,49
Achieving healthier outcomes and attaining longer lives free from preventable chronic diseases are public health goals delineated and strived toward by the United States and other nations globally.3,50 The persistently elevated premature death rate among rural residents serves as a critical indicator and suggests that chronic diseases could be prevented, delayed, or managed through effective interventions and improved access to public health services and resources. 49 Lifestyle medicine interventions can promote healthier behaviors and have beneficial impact for all people throughout the life course by cultivating health literacy for improving lifestyle choices. For example, women typically provide food for their families, and their learning new health information and skills can positively influence the nutritional behaviors of children and adult family members through ripple effects with potentially lasting generational health effects.43,51 Social support inherent within families and proactive health literacy from educational interventions have been associated with increased intake of fruits and vegetables among rural groups. 52
While this study provides insight into the effectiveness of lifestyle medicine interventions in rural populations, some strengths and limitations are noted. A major strength of this study was the randomized controlled trial design having both an intervention and control group with representative sample sizes to study intervention effects. Conversely, the focus on a rural group limited generalizability among dissimilar populations and the potential for cross-contamination among participants living in tight-knit rural communities.
Although attrition rates were descriptively higher in the control group (17.5%) than in the intervention group (7.5%), this difference was not statistically significant, suggesting that missingness was not systematically related to treatment group. Little’s MCAR tests showed mixed results across outcomes, but given that MCAR is more restrictive than MAR and attrition was modest, MAR remains a reasonable assumption for our FIML approach. Nonetheless, we acknowledge that mechanisms not at random (MNAR) cannot be ruled out, and larger confirmatory trials should incorporate additional sensitivity analyses (e.g., pattern-mixture or MNAR models).
Despite the evaluation of multiple outcomes introduces the risk of Type I error, the robustness of findings across conservative correction methods (i.e., Bonferroni adjustment with all P-values remaining <.001) strengthens confidence in the validity of the observed effects. Although we adjusted for race to address a baseline imbalance, more rigorous approaches such as stratified randomization will be used in future trials to prevent such imbalances. Additional re-analyses (e.g., propensity score methods) were outside the scope of this intervention study. There was a small percentage of male participants in this study which is consistent with other findings regarding underrepresentation of men in health research studies. 53 Future research could explore strategies to include more males, outcomes in urban areas, and potential ripple effects within families and social networks. Changing health behaviors is challenging, and future studies could investigate whether improvements in psychosocial determinants induce sustainable health behaviors longitudinally after a year or longer.
The implications for health professionals include considerations that can be used for developing other preventive health programs intended for community dwelling adults in rural areas and elsewhere. Addressing complex rural health challenges requires multi-faceted interventions that consider determinants of health behavior change as well as the uniqueness of social, environmental, and economic contexts within diverse rural communities. This involves efforts to improve healthcare access, promote healthy lifestyles through health education, and build rural community capacity for promoting health and reducing disease risk. Lifestyle medicine programs hold promise for promoting health behavior modifications that can improve psychosocial factors theoretically linked to determine health behaviors. Since chronic diseases are becoming increasingly prevalent throughout the world, especially among underserved populations, evidence-based strategies are needed to reverse this alarming trend in rural areas and beyond.
Footnotes
Acknowledgments
We wish to acknowledge Krystal Williams and Gabrielle Hutchinson for their assistance on this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Florida State University Translational Health Research Seed Grant, funded by the FSU Office of Research: 046517.
Ethical Considerations
This research received approval from the Institutional Review Board (IRB) at Florida State University: (STUDY00003258; 13 July 2022).
Consent to Participate
Participants provided informed consent prior to any study activities.
Clinical Trial Registration
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request