
Abstract
Non-communicable diseases (NCDs) are the leading cause of illness and death worldwide, and in Qatar, their burden is rising due to rapid urbanization, shifts toward Westernized diets, sedentary lifestyles, and cultural influences. Using data from the Global Burden of Disease Study 2021, this study examined the NCD burden in Qatar, including the burden of cardiovascular diseases, type 2 diabetes, cancer, chronic respiratory diseases, neurological conditions, and mental health disorders attributable to dietary risks, low physical activity, smoking, and high body-mass index (BMI). In 2021, lifestyle-related risk factors were responsible for 64.8% of NCD deaths and 33.2% of DALYs in Qatar. High BMI emerged as the top contributor, accounting for 24.5% of deaths and 13.9% of DALYs, followed by poor diet and smoking. The burden of high BMI-related NCDs increased over the past 30 years, with a 71.4% increase in deaths and a 54.3% rise in DALYs, while the impact of smoking declined. Compared to other Gulf Cooperation Council countries, Qatar had a higher NCD burden, particularly for cardiovascular diseases and diabetes linked to obesity. These findings highlight the need for coordinated public health action, aligned with Qatar’s National Health Strategy and the Doha Declaration on Lifestyle Medicine.
Keywords
“High BMI was the predominant risk factor, driving a significant burden of CVD, T2DM, and cancer, while smoking had a particularly high impact on males.”
Introduction
Non-communicable diseases (NCDs) pose a significant global health burden, accounting for at least 43 million deaths in 2021, which represents 75% of all non-pandemic-related deaths worldwide.1,2 A major concern is the high rate of early deaths, with 18 million people dying from NCDs before turning 70. 2 Between 2010 and 2021, disability-adjusted life years (DALYs) from NCDs increased by 17 6% globally. 3 Cardiovascular diseases (CVDs), cancer, chronic respiratory diseases and type 2 diabetes (T2DM) collectively account for 80% of all premature NCD-related deaths, reinforcing their central role in the global health agenda. 2 Collectively, these NCDs in addition to mental health disorders, have been estimated to cost US$ 47 trillion between 2010-2030 globally, an average of more than US$ 2 trillion per year. 4 The Middle East, particularly Qatar and other Gulf Cooperation Council (GCC) countries, is experiencing a rapid surge in NCD burden.2,3 CVD, T2DM, cancer, and respiratory diseases have become leading causes of morbidity and mortality in the GCC region. 5
Unhealthy diets, low physical activity, tobacco use, and high body-mass index (BMI) are key contributors to disease progression and mortality. 6 The rising NCD burden is fueled by shifts in lifestyle behaviors linked to urbanization, globalization, and higher socio-economic status. 7 Primarily driven by nutritional transitions and sedentary lifestyles, 8 the GCC nations are facing a rapidly growing epidemic of lifestyle-related diseases, with some of the highest obesity rates in the world, driving a surge in NCDs. 2 Obesity prevalence in the member nations has reached up to 40%. 9 Qatar specifically faces a significant burden of CVDs, cancer, T2DM, respiratory diseases, and mental health disorders, largely driven by unhealthy lifestyle.10,11 For instance, 46.1% of adult women (≥18 years) and 35.9% of adult men have obesity, exceeding the regional averages of 10.3% for women and 7.5% for men.12,13 Qataris typically consume diets high in meat, sugar, and sodium, while being insufficient in calcium and fiber, and these dietary patterns are compounded by low levels of physical activity. 14 Despite significant progress in tobacco control, 15 Qatar still has a high tobacco use prevalence of 25.2% in 2019. 16
The Doha Declaration 2024 on Lifestyle Medicine, 17 issued by The Global Alliance for Lifestyle Medicine, presents a critical global call to action to address the escalating burden of NCDs. The call stresses that, despite advancements in medical care, NCDs continue to rise, largely driven by modifiable lifestyle factors. This trend emphasizes the urgent need for a paradigm shift—one that moves beyond conventional disease management to proactively integrate evidence-based lifestyle interventions into health care systems.17,18 In alignment with this global commitment, the Qatari Ministry of Public Health’s National Health Strategy 2024-2030 has identified the promotion of healthy behaviors as one of its three Strategic Priority Areas. This strategic focus aims to mitigate the high burden of NCDs by embedding preventive and lifestyle-based interventions at both clinical and population levels. 19 Further reinforcing this shift, the recently launched National Action Plan on Obesity, T2DM, and Modifiable Risk Factors for Atherosclerotic Cardiovascular Disease (ASCVD) 2024-2030 19 prioritizes lifestyle-based strategies as fundamental to addressing the burden of NCDs.
To support the implementation of these strategies and actions, we aim to provide comprehensive evidence on the burden of NCDs in Qatar, particularly CVD, T2DM, cancer, mental health disorders, neurological disorders, and chronic respiratory diseases, attributable to lifestyle risk factors (smoking, diet, low physical activity, and high BMI). Using the Global Burden of Disease (GBD) study, the analysis collated data on mortality and DALYs attributable to these risks. Furthermore, the burden of these diseases and risk factors are compared with the average of the GCC, including its other 5 member nations (Bahrain, Kuwait, Oman, Saudi Arabia, and United Arab Emirates). Despite the rapid rise of lifestyle-related NCDs in Qatar, consolidated evidence quantifying their burden, especially in relation to regional GCC patterns, remains limited, a gap this work aims to fill.
Methods
Overview
All analyses in this study were conducted exclusively using estimates from the Global Burden of Disease (GBD) 2021 dataset. We extracted country-specific burden of disease data for Qatar from the GBD 2021 study using publicly available resources, including the Global Health Data Exchange (GHDx), GBD Results, and GBD Compare. These data were primarily derived from vital registration systems, supplemented by sample registration, censuses, surveys, surveillance systems, registries, and verbal autopsies. The complete list of GBD 2019 data sources for Qatar is available on the GHDx platform (https://ghdx.healthdata.org/geography/qatar). GBD provides comprehensive estimates of global risk exposure and the associated health burden, integrating all relevant available data. It quantified deaths and DALYs (the sum of years of life lost due to premature mortality and years lived with disability) for 88 behavioral, metabolic, environmental, and occupational risk factors across 288 causes of death or injury. These estimates encompassed 204 countries and territories, organized into 21 regions and 7 super-regions, with subnational analyses available for 21 locations. The detailed methodology used in the GBD study has been published elsewhere.20,21 The GBD framework categorizes all risk factors into a hierarchical structure with 4 levels: Level 1 includes 3 broad risk factor categories; Level 2 consists of 20 specific risk factors; Level 3 further disaggregates 9 of the 20 Level 2 factors into 42 sub-risk factors; and Level 4 expands on 9 Level 2 factors and 37 Level 3 risks. 20
Unhealthy Lifestyle Factors and Disease Burden
For Qatar, 437 data sources (https://ghdx.healthdata.org/geography/qatar) were used to assess the burden of disease and attributable risk factors between 1990 and 2021. In this study, the extracted metrics included all-cause and cause-specific mortality, as well as DALYs, for the 6 most common NCDs in Qatar—CVD, T2DM mellitus, cancer, chronic respiratory diseases, neurological disorders, and mental disorders—attributable to 4 lifestyle risk factors: dietary risks, low physical activity, smoking and high BMI (Figure S1). We initially considered 5 commonly studied lifestyle factors from the literature: diet, alcohol consumption, physical activity, smoking, and high BMI6,7 to include in this study. However, alcohol was excluded due to its very low consumption in Qatar. The burden of disease attributable to these lifestyle factors were compared with those of 5 other GCC countries over the same period.
Exposure Levels and Data Sources
To estimate the mean exposure for each risk factor, systematic literature reviews were conducted to identify relevant studies published or included since GBD 2021. These studies were integrated with data from additional sources, including household and health examination surveys, censuses, ground-based and remote sensing data, and administrative records. A Bayesian hierarchical meta-regression model, DisMod-MR 2.0, was applied to estimate exposure levels of unhealthy lifestyle risk factors by age, sex, and year. 20 In simple terms, this model combines data from multiple sources to produce the most reliable estimates for each population group. The analysis followed a four-level hierarchical structure—global, super-region, region, and country. DisMod-MR 2.0 incorporates tabulated unhealthy risk factors along with uncertainty estimates and consists of 2 main components. The first component employs a mixed-effects meta-regression model, where sex and covariates are included as fixed effects at the super-region, region, and country levels. The second component follows a cascading approach, sequentially refining the model by restricting data to a specific year-sex stratum and a particular hierarchical level (e.g., country). This approach enhances the precision of country-level estimates by incorporating local data while leveraging information from higher geographic levels. When country-specific data for Qatar were unavailable, exposure estimates were derived from the regional (North Africa and Middle East) or global levels, with adjustments made for country-level covariates. 20
The proportion of disease burden that could have been averted if exposure levels had remained at the level associated with the lowest risk of unhealthy lifestyle risk factors was estimated. This optimal exposure level, referred to as the theoretical minimum risk exposure level (TMREL), corresponds to the intake associated with the lowest risk across all diseases (Table S1). 20 The determination of TMREL involved a two-step process. First, prospective observational studies were utilized to identify the intake level linked to the lowest risk for each disease outcome. Second, a weighted average of these disease-specific optimal intake levels was computed, with weights assigned based on the proportion of deaths from each disease relative to the total deaths attributed to the exposure at the global level. To account for uncertainty, a range extending 20% above and below the weighted mean was applied. 20
Estimating Effect Sizes
To derive relative risk (RR) estimates for risk–outcome relationships, GBD study integrates data from various primary sources, including randomized controlled trials, cohort studies, pooled cohort analyses, case–control studies, and systematic reviews summarizing RRs through meta-analyses. 20 Estimates were generated for risk–outcome pairs that were already included in GBD 2021, based on associations classified as convincing or probable according to the assessment criteria and methodology of the World Cancer Research Fund.20,22 The availability of data sources for estimating both RRs and exposure levels varied depending on the specific unhealthy lifestyle factor considered. 20
Estimating the Effect of Unhealthy Lifestyle on Disease Burden and Uncertainties
Methods of GBD to estimate the disease burden (fatal and non-fatal) associated with all risk factors are described elsewhere.
20
The analysis was conducted within the framework of comparative risk assessment (CRA), which is designed to estimate the impact of risk factors. The key inputs for quantifying the proportion of disease burden attributable to dietary risks included: (1) the exposure level for each dietary risk factor (
The PAF for a given unhealthy lifestyle risk factor
The attributable burden was estimated by applying the PAF to the total burden, measured in terms of deaths and DALYs.20,21 Data on DALYs and mortality were obtained from GBD 2021 studies.21,23
Presentation of Estimates
The estimated burden attributable to unhealthy lifestyle factors in 2021 is presented as absolute counts, crude proportions, and age-standardized population attributable fractions. Age standardization was performed using the GBD standard population structure to account for differences in age distribution across populations. 23 Temporal trends were assessed by reporting the total percentage change between 1990 and 2021. All estimates were derived as the mean of 500 Monte Carlo simulations, with 95% uncertainty intervals (UIs) defined by the 2.5th and 97.5th percentiles of the distribution. 20 The analysis adhered to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) (Table S2). 24 Data processing was performed using R (R Core Team, 2024; R version 4.4.2).
Results
Burden of Lifestyle-Related Diseases
Overall NCD Burden
Crude Number, Percentage of Deaths, Disability-Adjusted Life Years (DALYs) and Uncertainty Intervals (UIs) of Non-communicable Disease Attributable to Lifestyle Risk Factors in Qatar, 2021
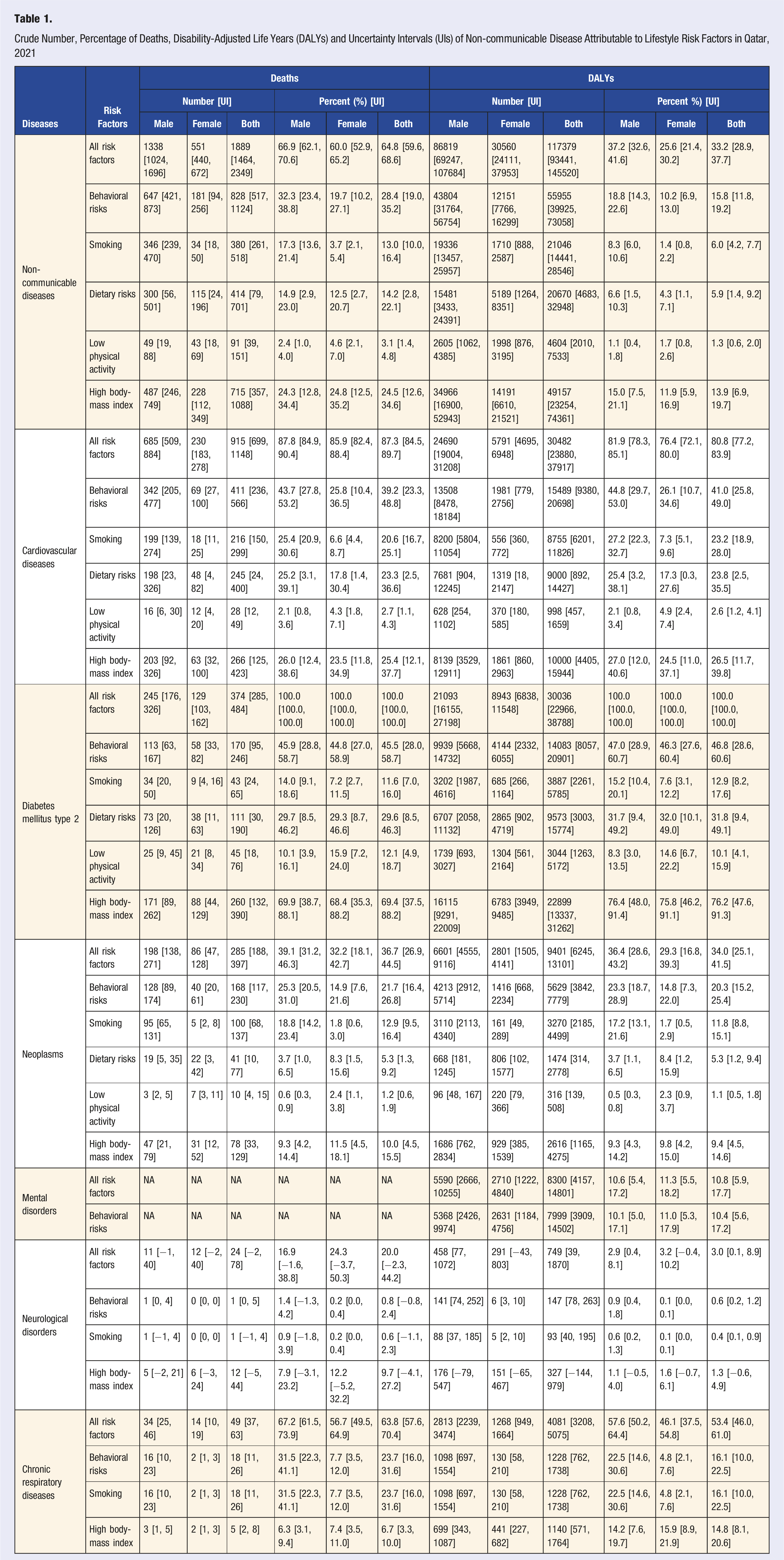
Behavioral risks contributed to 828 NCD deaths (28.4% [UI: 19.0, 35.2]) and over 55,955 NCD DALYs (15.8% [UI: 11.8, 19.2]), with males being disproportionately affected. High BMI had the largest impact, contributing to 715 deaths (24.5% [UI: 12.6, 34.6]) and 49,157 DALYs (13.9% [UI: 6.9, 19.7]). Dietary risks were the second major contributor, leading to 414 deaths (14.2% [UI: 2.8, 22.1]) and 20,670 DALYs (5.9% [UI: 1.4, 9.2]). Smoking had a higher impact on males, causing 346 deaths (17.3% [UI: 13.6, 21.4]) compared to only 34 deaths (3.7% [UI: 2.1, 5.4]) in females, totaling 380 deaths (13.0% [UI: 10.0, 16.4]) and 21,046 DALYs (6.0% [UI: 4.2, 7.7]). Low physical activity had a smaller effect, contributing to 91 deaths (3.1% [UI: 1.4, 4.8]) and 4604 DALYs (1.3% [UI: 0.6, 2.0]) (Table 1).
Specific Disease Burden
All risk factors combined led to 915 CVD deaths (87.3% [UI: 84.5, 89.7]) and 30,482 DALYs (80.8% [UI: 77.2, 83.9]), with males accounting for the majority of the burden. Among individual risk factors, smoking was responsible for 216 deaths (20.6% [UI: 16.7, 25.1]) and nearly 8755 DALYs (23.2% [UI: 18.9, 28.0]), while dietary risks accounted for 245 deaths (23.3% [UI: 2.5, 36.6]) and 9000 DALYs (23.8% [UI: 2.5, 35.5]). Low physical activity had a relatively smaller impact, contributing to 28 deaths (2.7% [UI: 1.1, 4.3]) and 998 DALYs (2.6% [UI: 1.2, 4.1]). High BMI was the dominant risk factor for CVD, contributing to 266 deaths (25.4% [UI: 12.1, 37.7]) and nearly 10,000 DALYs (26.5% [UI: 11.7, 39.8]). T2DM due to all risk factors led to 374 deaths (100.0% [UI: 100.0, 100.0]) and 30,036 DALYs (100.0% [UI: 100.0, 100.0]). High BMI contributed to 260 deaths (69.4% [UI: 37.5, 88.2]) and nearly 22,899 DALYs (76.2% [UI: 47.6, 91.3]). Behavioral risks overall accounted for 168 cancer deaths (21.7% [UI: 16.4, 26.8]) and 5629 cancer DALYs (20.3% [UI: 15.2, 25.4]). Smoking was the leading behavioral risk factor for cancer-related deaths, contributing to 100 deaths (12.9% [UI: 9.5, 16.4]) and 3270 DALYs (11.8% [UI: 8.8, 15.1]), with a higher impact on males. High BMI also contributed to 78 cancer deaths (10.0% [UI: 4.5, 15.5]) and 2616 cancer DALYs (9.4% [UI: 4.5, 14.6]) (Table 1).
Disease Burden by Age
In younger individuals (15-49 years), high BMI, dietary risks, and smoking were the predominant contributors to both DALYs and mortality, particularly for CVD. In middle-aged adults (50-69 years), behavioral risks—including smoking, dietary risks, and low physical activity—had the greatest impact on the burden of NCDs and CVD. By contrast, in older adults (70+ years), mortality was predominantly linked to smoking-related CVD, with deaths accounting for 12.7% in males and only 5.3% in females. Furthermore, high BMI contributed to 26.8% of NCD deaths in females and 21.5% in males in this age group (Figure 1). Burden of disease (deaths and disability-adjusted life years) attributable to lifestyle-related risk factors by age and sex in Qatar, 2021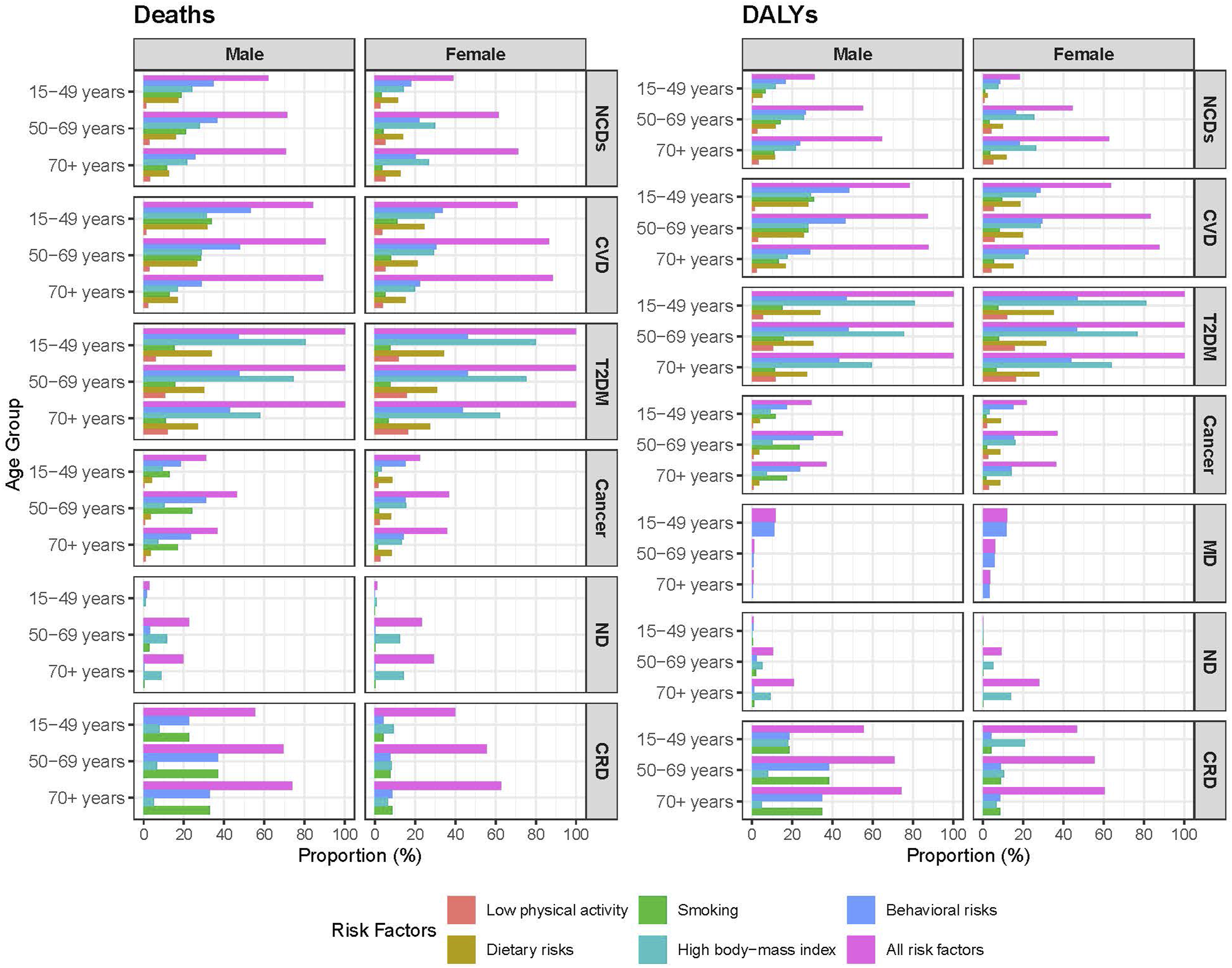
BMI-associated NCD mortality was highest in the 50-69 age group, accounting for 29.9% of deaths in females and 27.8% in males. Smoking-related NCD DALYs was 14.3% in males vs only 3.1% in females aged 50-69 years. Dietary risks contributed to 18.5% and 28.0% of DALYs in females and males aged 15-49 years, respectively. Smoking was the primary contributor to CVD burden, with 13.2% DALYs in males and only 5.3% in females within the 50-69 age group. Smoking also accounted for 30.8% of CVD DALYs in males but only 9.4% in females aged 15-49 years (Figure 1).
Diet-Related NCD Burden
The burden of CVD attributable to dietary risks was consistently higher among males compared to females. Among males, low whole grain intake accounted for 16.2% of deaths and 16.9% of DALYs, while among females, these figures were 10.5% and 11.1%, respectively. High consumption of sugar-sweetened beverages was attributable to 9.2% of T2DM deaths and 10.9% of DALYs. This was closely followed by low intake of whole grains, which accounted for 14.9% of deaths and 15.0% of DALYs. Diets high in processed and red meat also contributed significantly, with attributable fractions ranging from 4.4% to 5.6% for deaths and 5.0% to 6.1% for DALYs. Unlike CVD, the sex-specific differences in T2DM burden were less pronounced. High consumption of red meat was accounted for 5.8% of cancer deaths and 6.2% of cancer DALYs among female. In contrast, males experienced a lower burden from red meat consumption (1.5% of deaths and DALYs). Diets low in fruits, vegetables, and fiber had minimal impact on cancer burden, with attributable fractions consistently below 0.3% (Figure 2). Burden of non-communicable diseases attributable to dietary risk factors in Qatar, 2021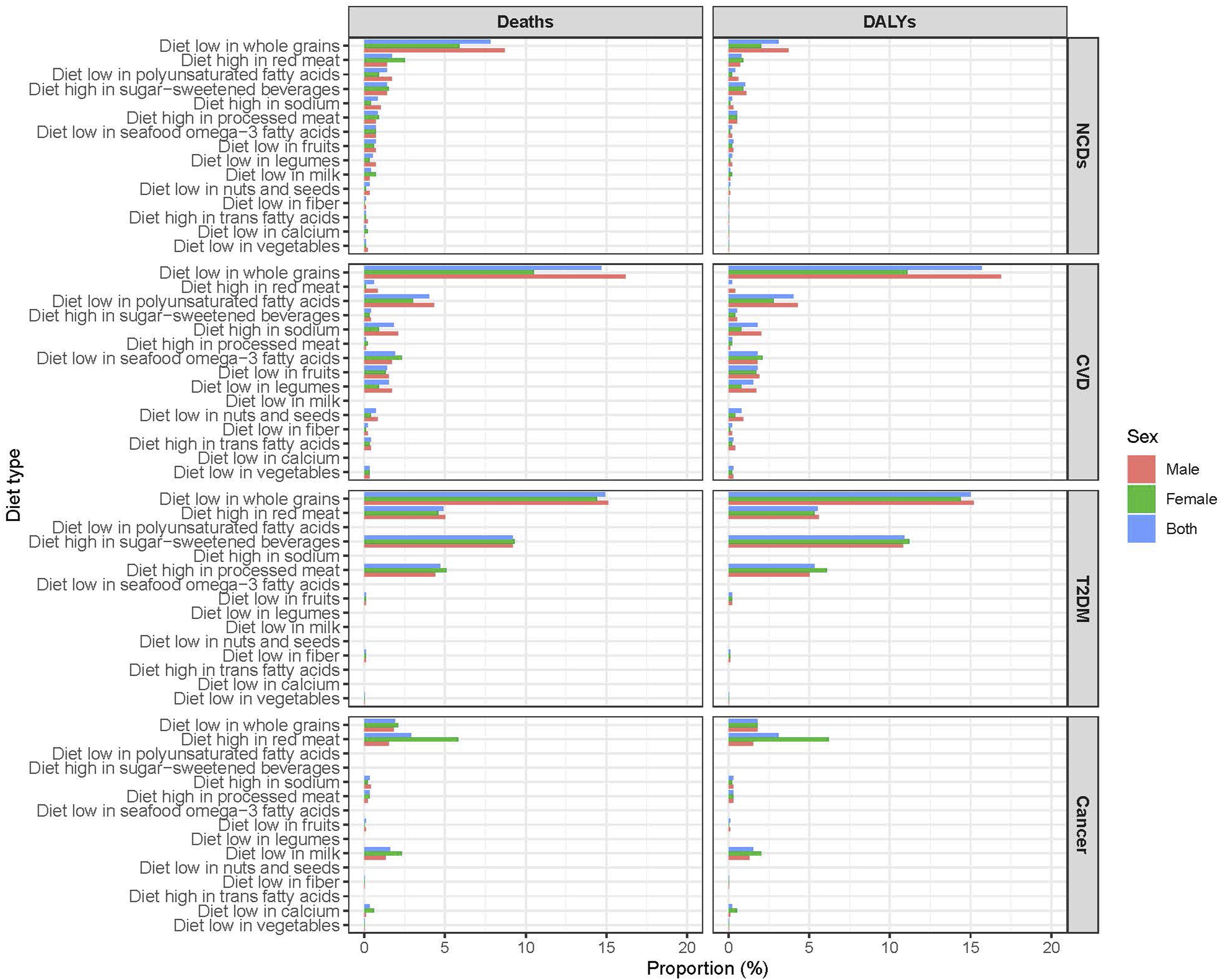
Trend of Lifestyle-Related Disease Burden, 1990-2021
Overall Trend
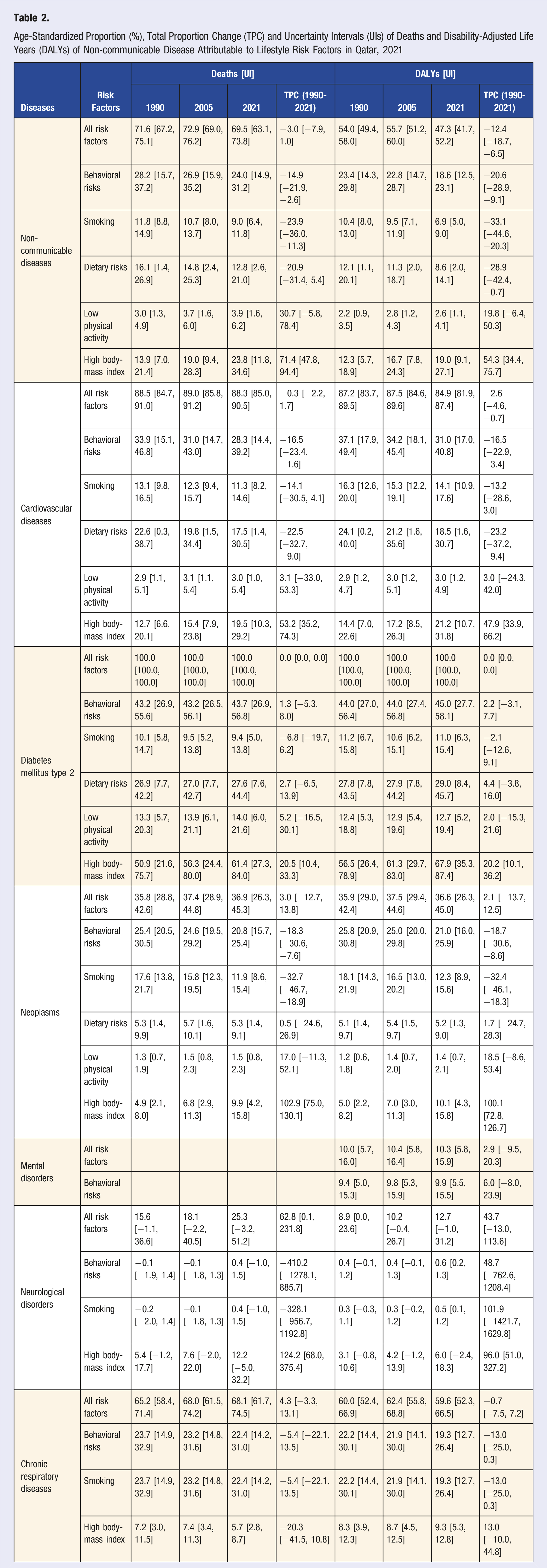
Age-Standardized Proportion (%), Total Proportion Change (TPC) and Uncertainty Intervals (UIs) of Deaths and Disability-Adjusted Life Years (DALYs) of Non-communicable Disease Attributable to Lifestyle Risk Factors in Qatar, 2021
Disease-Specific Trend
The proportion of CVD deaths and DALYs due to all risk factors remained relatively stable. However, notable declines were observed in dietary risks and smoking, which decreased by 22.5% [UI: −32.7, −9.0] and 14.1% [UI: −30.5, 4.1], respectively. In contrast, high BMI-related deaths increased by 53.2% [UI: 35.2, 74.3], and DALYs rose by 47.9% [UI: 33.9, 66.2]. The proportion of T2DM deaths attributable to behavioral risks, including dietary risks and low physical activity, showed marginal increases. T2DM death attributable to dietary risks increased by 2.7% [UI: −6.5, 13.9], while low physical activity-related deaths rose by 5.2% [UI: −16.5, 30.1]. The most pronounced change of T2DM burden was observed in the impact of high BMI, which increased by 20.5% [UI: 10.4, 33.3] for deaths and 20.2% [UI: 10.1, 36.2] for DALYs. The contribution of smoking to cancer-related deaths and DALYs declined by 32.7% [UI: −46.7, −18.9] and 32.4% [UI: −46.1, −18.3], respectively. However, high BMI-associated cancer deaths and DALYs more than doubled over the three-decade period, with deaths rising by 102.9% [UI: 75.0, 130.1] and DALYs by 100.1% [UI: 72.8, 126.7]. For neurological disorders, the burden attributable to high BMI increased markedly, with deaths and DALYs rising by 124.2% [UI: 68.0, 375.4] and 96.0% [UI: 51.0, 327.2], respectively (Table 2).
Age- and Sex-Specific Trends
The age-standardized mortality burden attributable to all risk factors exhibited an overall decline, decreasing from 71.6% in 1990 to 69.5% in 2021. In the 15-49 age group, the proportion of NCD deaths due to all risks increased from 57.4% in 1990 to a peak of 63.1% in 1995, followed by a gradual decline to 57.4% in 2021. A similar trend was observed in DALYs, which rose from 28.3% in 1990 to 33.7% in 1995 before steadily decreasing to 29.8% in 2005 and continuing on a downward trajectory. Among individuals aged 50-69 years, deaths attributable to all risk factors remained relatively stable, fluctuating between 73.6% and 74.7% until the early 2000s before experiencing a steady decline to 68.6% in 2021. A similar but less pronounced pattern was observed in the 70+ age group, where the proportion of deaths declined from 73.2% in 1990 to 70.9% in 2021 (Figure 3). Trend of age-standardized, sex-specific proportion of deaths and disability-adjusted life years (DALYs) of non-communicable disease attributable to lifestyle risk factors in Qatar, 1990-2021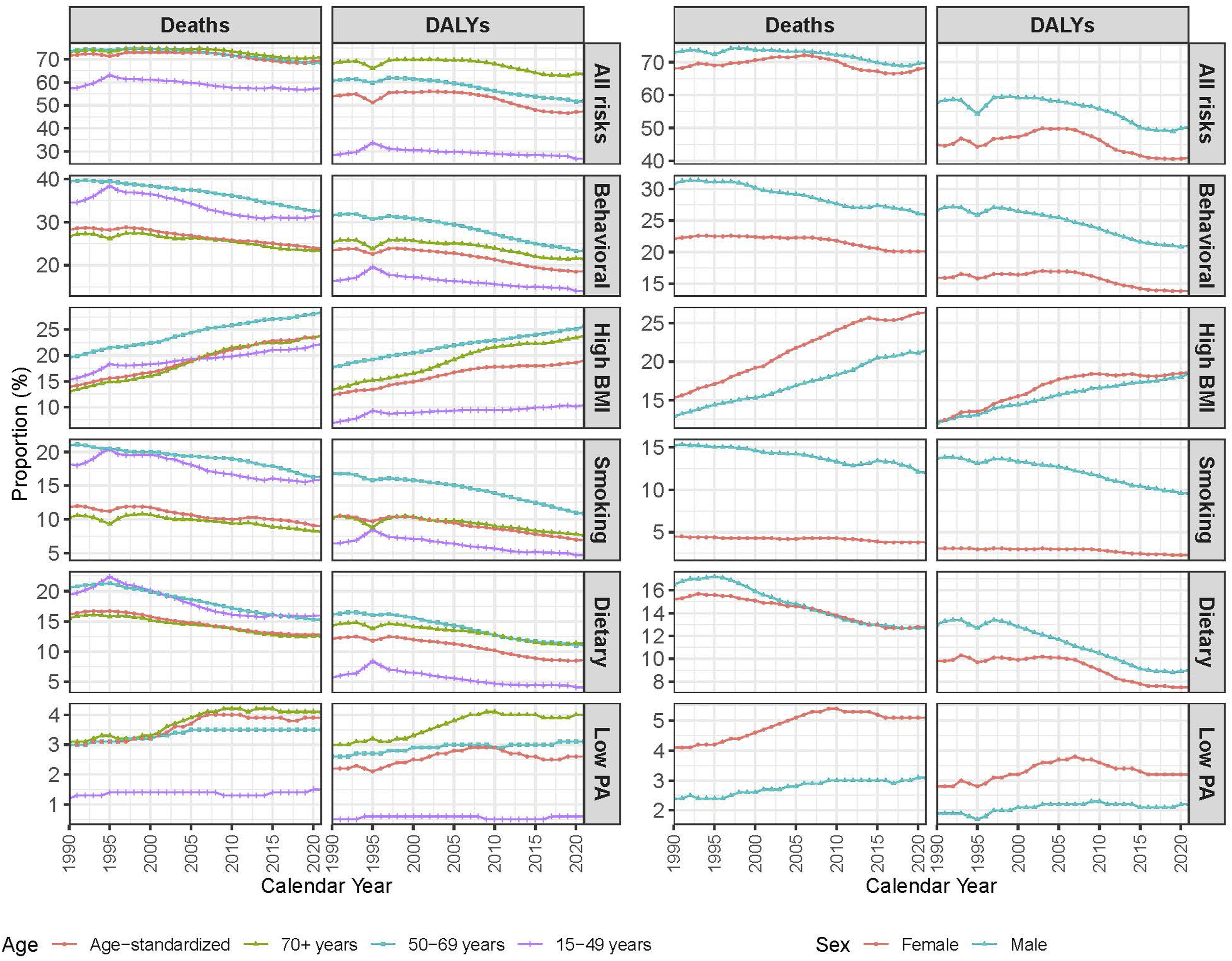
The age-standardized proportion of NCD deaths attributable to all risk factors among males declined from 72.9% in 1990 to 69.9% in 2021, while among females, it remained relatively stable (68.1% in 1990 to 68.2% in 2021). NCD DALYs decreased from 57.9% to 50.3% in males and from 44.9% to 40.9% in females between 1990 and 2021. In males, NCD deaths attributable to behavioral risks dropped from 31% in 1990 to 26% in 2021, while lower and stable trend was found in females over the same period. The impact of specific behavioral risks varied, with smoking-related deaths declining steadily (particularly in males), whereas NCD deaths attributable to high BMI and low physical activity showed an increasing trend in both male and female (Figure 3).
Sex-Specific Trend
Among males, NCD deaths due to high BMI rose from 12.7% in 1990 to 20.3% in 2021, while among females, the increase was from 14.8% to 21.5% over the same period. CVD deaths due to high BMI followed a similar trend, increasing from 12.7% to 20.3% in males and from 14.6% to 21.2% in females, highlighting the worsening obesity epidemic. T2DM deaths related to high BMI saw the most dramatic increase in males (54.2% to 64.8%) and in females (56.0% to 67.4%). Cancer mortality attributable to high BMI doubled in both males (5.6% to 10.5%) and females (6.2% to 12.1%). Neurological disorder deaths due to high BMI more than doubled both in males (4.2% to 8.8%) and females (4.5% to 9.6%). Smoking-related deaths have declined more significantly in males compared to females. Among males, smoking-related NCD deaths dropped from 15.2% in 1990 to 11.2% in 2021, whereas in females, the decline was smaller (4.5% to 3.1%). Smoking-related cancer deaths in males declined significantly (24.6% to 17.2%), while in females, it remained much lower and stable at around 1.8%. NCD deaths due to poor diet declined from 12.5% to 10.3% in males and from 14.7% to 10.5% in females. CVD deaths due to dietary risks dropped from 22.6% to 17.3% in males and from 21.1% to 16.9% in females. However, T2DM mortality linked to dietary risks remained high, increasing from 27.5% to 28.4% in males and from 29.2% to 30.1% in females. Cancer deaths due to dietary risks remained stable for both males (6.0% to 5.9%) and females (5.8% to 5.7%) (Figure 4). Sex-specific trend of age-standardized proportion of deaths and disability-adjusted life years (DALYs) of non-communicable diseases attributable to lifestyle risk factors in Qatar, 1990-2021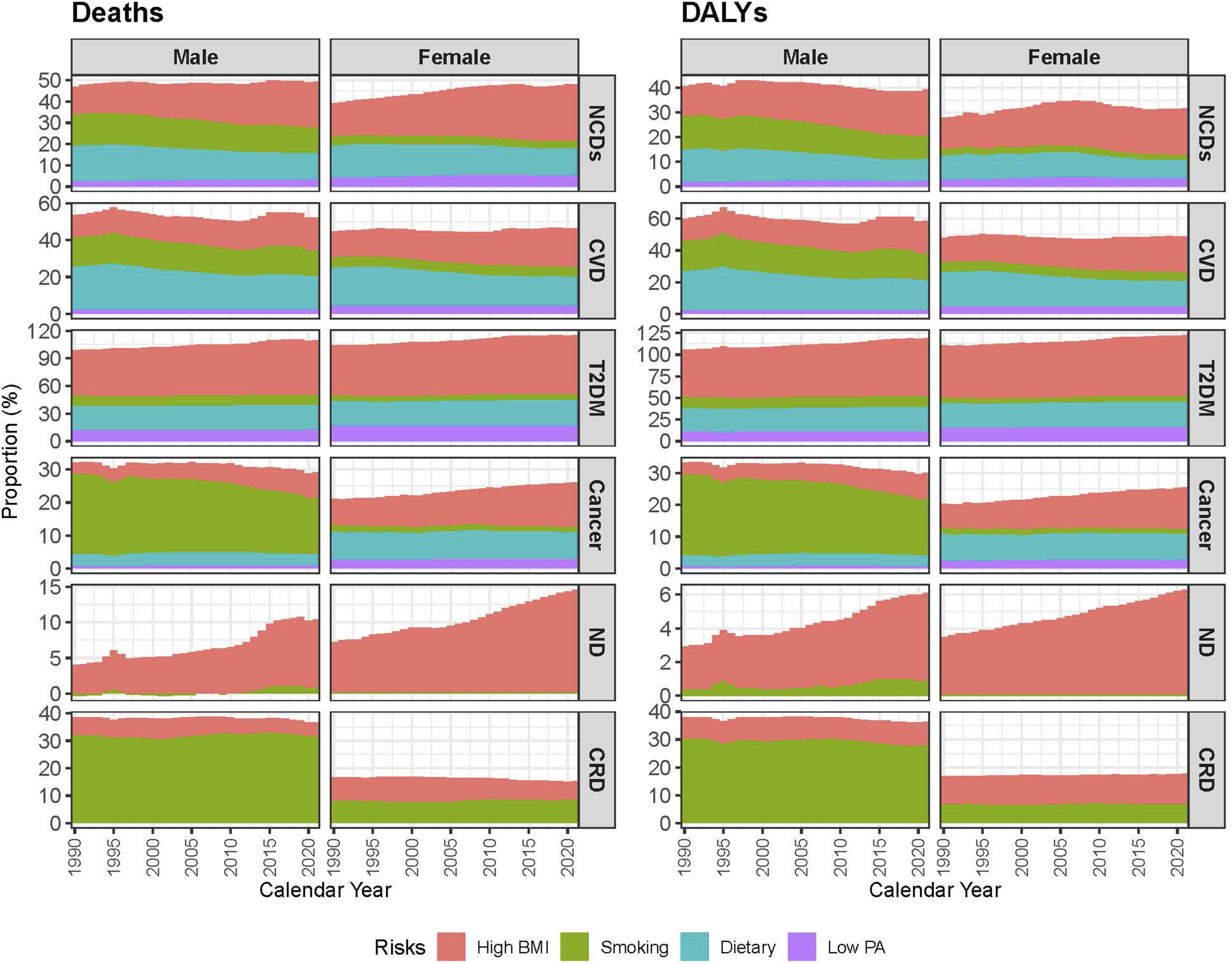
Comparison With GCC Countries
NCDs accounted for the majority of deaths in Qatar, primarily driven by high BMI, dietary risks, and smoking. Between 1990 and 2021, NCD deaths due to all risk factors in Qatar increased from 65.9% to 72.1%, surpassing the GCC average (71.4%). High BMI’s contribution to CVD deaths in Qatar saw a substantial rise from 12.9% in 1990 to 22.5% in 2021, exceeding the GCC average (21.3%). T2DM-related deaths due to high BMI surged from 50.2% to 63.4% Smoking-related cancer deaths dropped from 19.5% in 1990 to 15.2% in 2021, mirroring GCC-wide reductions. However, high BMI-related cancer deaths in Qatar nearly doubled from 4.2% to 8.5%, surpassing the GCC average (7.8%) (Figure 5, S2 and S3). Trend of age-standardized proportion of deaths and disability-adjusted life years attributable to lifestyle factors among members of the gulf cooperative council, 1990-2021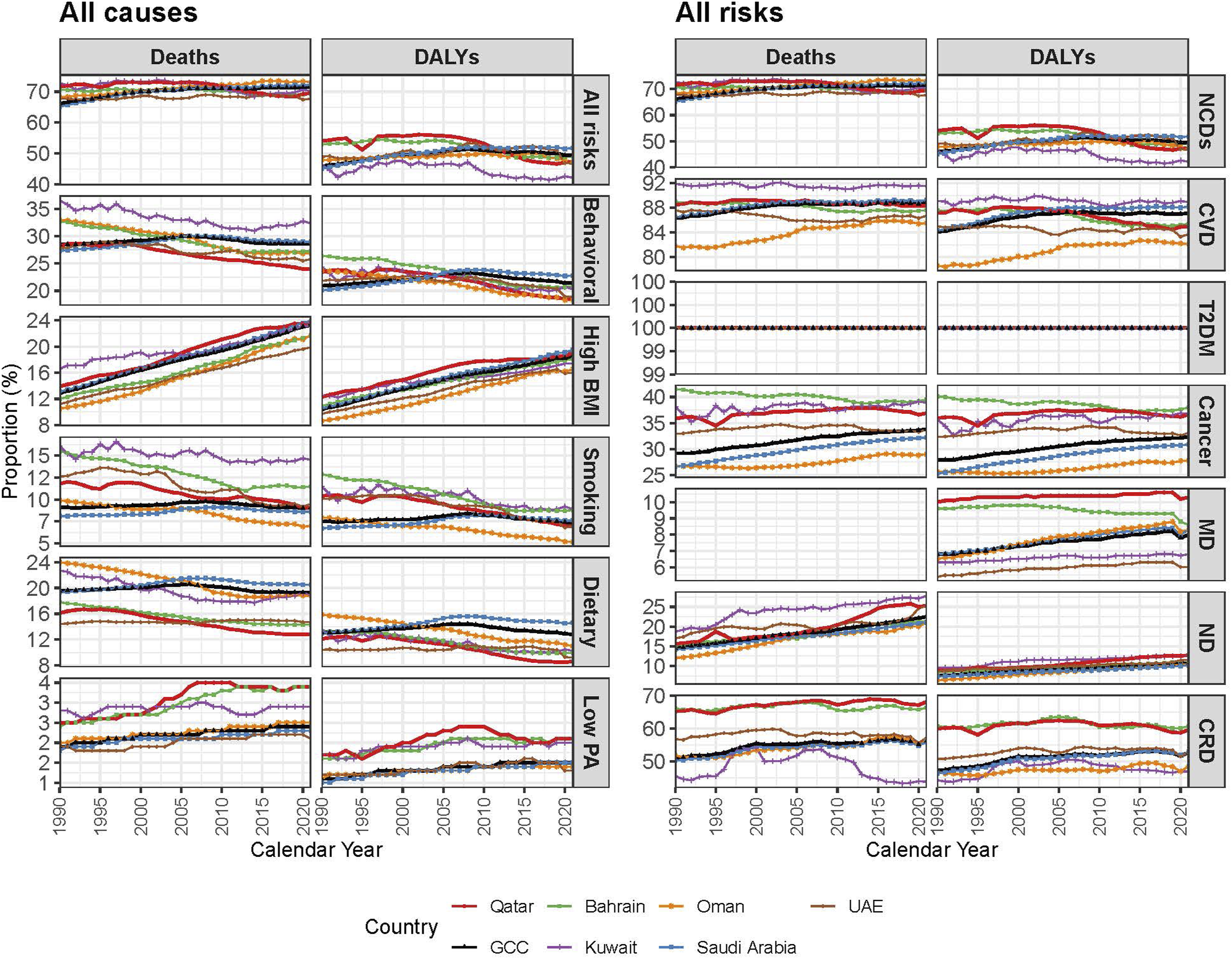
NCDs also accounted for the majority of DALYs in Qatar, increasing from 48.2% in 1990 to 52.3% in 2021, exceeding the GCC average (51.8%). NCD DALYs attributable to high BMI has shown the sharpest rise among NCD risk factors, increasing from 9.7% in 1990 to 18.4% in 2021, surpassing the GCC average (17.9%). The burden of T2DM-related DALYs due to high BMI rose from 50.2% in 1990 to 63.4% in 2021. Smoking-related cancer DALYs declined from 19.5% to 15.2%, but high BMI-related cancer DALYs nearly doubled from 4.2% to 8.5% (Figure 5, S2 and S3).
Discussion
This study provides a comprehensive assessment of NCD burden attributable to lifestyle-related risk factors in Qatar. Behavioral risk factors accounted for 64.8% of all deaths and 33.2% of DALYs in 2021. High BMI was the predominant risk factor, driving a significant burden of CVD, T2DM, and cancer, while smoking had a particularly high impact on males. The burden varied across age groups, with younger individuals (15-49 years) predominantly affected by high BMI, dietary risks, and smoking, whereas middle-aged adults (50-69 years) experienced the highest proportion of NCD burden from smoking, dietary risks, and low physical activity. Among older adults (≥70 years), mortality was largely attributable to smoking-related CVD. Over the past 3 decades (1990-2021), the burden of NCDs attributable to key lifestyle-related risk factors has undergone significant shifts, with reductions in smoking- and diet-related mortality, contrasted by a significant rise in obesity-related morbidity and mortality. While age-standardized deaths due to smoking declined by nearly a quarter (23.9%) and dietary risks by 20.9%, the impact of high BMI surged, with deaths increasing by 71.4% and DALYs by 54.3%. High BMI-related CVD deaths and DALYs rose substantially, showcasing the growing obesity epidemic. A similar trend was observed in cancer and neurological disorders, where high BMI-related deaths more than doubled, contrasting with declining smoking-related cancer mortality. The findings highlight the urgent need for targeted interventions to reduce exposure to modifiable lifestyle risk factors, with a particular focus on addressing obesity, improving dietary quality, and implementing effective tobacco control measures. These findings also highlight an epidemiological transition where the gains from reductions in behavioral risk factors (e.g., smoking) are being offset by the escalating impact of obesity, necessitating urgent, multifaceted public health interventions.
The Sustainable Development Goals (SDGs) 3, 25 which focuses on health, builds upon the Millennium Development Goals by adopting a more comprehensive framework for health promotion and disease prevention. 26 However, NCDs driven by unhealthy behaviors remain a significant global challenge. A shift in health-related behaviors is essential to reducing premature NCD mortality, yet evidence suggests that modifying population-level lifestyle patterns remains difficult, impeding progress toward the SDGs. 27 Moreover, achieving these global targets requires substantial financial investment, strong political commitment, and innovative funding mechanisms. 28 In line with global trend, 20 our findings indicate that lifestyle-related risk factors contribute to nearly two-thirds of all NCD-related deaths and approximately one-third of DALYs in Qatar. As observed in many other regions, NCDs impose a considerable economic burden on Qatar’s government, encompassing health care costs, early retirement benefits, social care, and welfare support.11,19 A report by Qatar’s Ministry of Public Health estimated that in 2019, NCDs accounted for approximately US$5 billion, equivalent to 2.7% of the country’s gross domestic product (GDP). This financial strain is largely attributable to modifiable lifestyle factors, including poor dietary habits, tobacco use, and physical inactivity. 11
A poor diet contributes to more deaths worldwide than any other risk factor.20,29 Similarly, a suboptimal diet is the leading behavioral risk factor for deaths in Qatar, followed by tobacco use and low physical activity. 2 Although reductions in diet-related NCD mortality have been observed over the past 3 decades in Qatar, it is important to note that the contribution of the diet-related burden of disease may have been underestimated due to the limited availability of country-specific dietary data for Qatar. The dietary data were primarily derived from global and super-regional consumption patterns, with country-specific information obtained from the Qatar STEPs NCD Risk Factors Survey 2012 30 and the Qatar Global School-Based Student Health Survey 2011-2012. 31 The reliance on these sources may not fully capture the dietary patterns and nutritional transitions unique to the Qatari population, potentially leading to an underestimation of the true burden of diet-related NCDs. Different from other countries, Qatar has a food subsidy program which led to its high consumption of sugar. Based on the 2012 survey, the total purchased sugar consumption under the food subsidy program was 119.2/person/day. 32 Nevertheless, the burden of disease attributable to these risk factors remains substantial, highlighting the urgent need for enhanced surveillance systems and more representative dietary data to inform targeted public health interventions.
Efforts to mitigate the diet-related burden of disease in Qatar require a comprehensive, multi-sectoral approach that enhances the food environment, promotes healthier consumption patterns, and implements evidence-based policy interventions. Expanding domestic food production through modern agricultural techniques such as greenhouses and advanced irrigation systems is crucial for ensuring the availability of nutrient-dense foods despite environmental constraints. 33 Furthermore, promoting local food markets and implementing targeted incentives to encourage the consumption of nutrient-dense foods represent viable strategies for shifting dietary patterns toward healthier choices. However, dietary habits in Qatar remain suboptimal, as evidenced by a high prevalence of inadequate intake of key food groups essential for health.14,32 Over 83% of the adult population does not adhere to dietary recommendations for vegetables, fruits, whole grains, legumes, and high-fiber foods.30,34 Frequent consumption of sugar-sweetened beverages and confectioneries is reported by 50-72% of the population, while 47% report frequent intake of fast foods. 34 The burden of diet-related health risks is further compounded by the high prevalence of overweight and obesity, affecting up to 70% of adults.9,34 Given the established association between suboptimal diet and NCD, 29 urgent measures, including culturally appropriate nutrition education, policy reforms targeting food environments, and sustainable public health strategies to enhance dietary quality and overall health outcomes, are needed to address this dietary shortfall. Concurrently, initiatives such as the fat, sugar, and salt reduction initiative play a pivotal role in curbing excessive consumption of harmful dietary components, including trans fats and sodium. 35
Taxation policies on unhealthy food products represent an effective fiscal tool to reduce consumption of harmful dietary components, yet their design significantly influences the effectiveness. The excise tax on sugar-sweetened beverages introduced in Qatar in 2019 and revised in 2024 36 aligns with global best practices and has demonstrated potential in reducing sugar-sweetened beverages intake and associated health risks. However, relying solely on price-based taxation may lead consumers to opt for cheaper, yet equally unhealthy alternatives. Evidence from Saudi Arabia suggests that sugar-sweetened beverage taxation effectively reduced soft drink sales, 37 but the WHO recommends a tax structure based on sugar content rather than price alone to maximize public health benefits. 38 Additionally, earmarking tax revenues for health initiatives, as seen in countries like the Philippines and Egypt, can enhance public acceptance and strengthen health system financing.39,40 Beyond taxation, reducing salt consumption through industry reformulation efforts, such as Qatar’s initiative to decrease salt in bread by 30%, demonstrates a proactive approach to mitigating hypertension and CVD risk.35,41 Given the dietary shifts in the region towards processed foods high in sugar, sodium, and unhealthy fats, Qatar’s ongoing efforts to regulate the food industry, improve food accessibility, and promote healthier consumption behaviors are essential for reducing the growing NCD burden and achieving long-term health improvements.
The findings of this study highlight the persistent burden of tobacco use on NCDs in Qatar, particularly among males, despite recent declines in smoking-related mortality. Smoking remains a major contributor to CVD and cancer-related deaths, especially among older adults (≥70 years). While the implementation of the 2002 anti-tobacco law, 42 Qatar Excise Tax Law in 2019, 36 and complete smoking bans in public places 15 represents significant policy efforts, tobacco use prevalence remains a concern.15,16 The overall tobacco use prevalence in 2019 was 25.2%, but it has declined compared to previous years 16 suggesting the effective tobacco control measures. Indeed, the declining trend in smoking-related deaths in our study suggests that existing tobacco control measures have had a positive impact; however, the continued burden among older adults and persistent exposure call for stricter enforcement of smoking bans and further taxation policies to meet the WHO-recommended minimum of 75% of the retail price. 15 Without sustained public health efforts, the gains in reducing smoking-related NCDs may be undermined by ongoing exposure to smoking.
Physical inactivity is a critical yet often underestimated 43 modifiable risk factor contributing to the rising burden of NCDs in Qatar. This underestimation is partly due to the scarcity of country-specific data, as seen with dietary risks. Nevertheless, while dietary risks and smoking are increasingly recognized as major public health concerns, low levels of physical activity remain a significant driver of CVD and T2DM. The global burden of disease attributable to low physical activity remains significant, with 0.83 million deaths and 15.8 million DALYs in 2019. 44 In the current study, 3.1% of deaths and 1.3% of DALYs were attributable to low physical activity in 2021, and these proportions have increased since 1990 in Qatar. According to the Qatar National Health Strategy 2018-2022, 44% of adults engage in insufficient physical activity, with particularly high levels of inactivity among women (83%). 45 The increasing burden of obesity-related NCDs in Qatar, alongside persistently low physical activity levels, highlights the urgent need for targeted policies that promote active transportation, community-based exercise programs, and workplace interventions to encourage physical movement.
Our findings show that the rising burden of high BMI poses a significant public health challenge, underscoring the urgent need for targeted interventions to mitigate the growing impact of overweight and obesity in the country.12,13,30 While weight loss can be achieved through lifestyle modifications (including a healthy diet and regular physical activity), pharmacological and surgical interventions are also effective strategies. Weight-loss medications approved for long-term use have demonstrated modest effectiveness in managing obesity. 46 However, their effects on cardiometabolic risk factors vary, with no single drug addressing all risk factors comprehensively. 47 Bariatric surgery, on the other hand, is a well-established intervention that leads to significant and sustained weight loss48,49 In Qatar, bariatric surgery is prevalent, with a reported level of 12%. 50 However, concerns remain regarding the long-term sustainability of weight loss achieved through both pharmacologic and surgical approaches. 51 Thus, despite the short-term benefits of these weight loss interventions, further research is needed to evaluate its long-term impact on major health outcomes, including CVD, cancer, mental health and other NCDs.51,52 Moreover, adiposity is not the sole determinant of disease risk, 20 which reinforces a comprehensive approach that prioritizes lifestyle modifications, including a balanced diet and regular physical activity, that may offer more sustainable and holistic health benefits than pharmacological or surgical interventions alone.51,53 Evidence suggests that adopting and maintaining healthy lifestyle behaviors remain the most effective strategies for preventing obesity-related diseases and promoting long-term health.51,54
Limitations
While the robust methodology of the GBD 2021 framework20,21 was leveraged to estimate the burden of disease associated with unhealthy lifestyle factors in Qatar, several limitations should be acknowledged. First, the availability and quality of country-specific data remain a challenge, potentially contributing to either overestimation or underestimation of disease burden estimates. Although UIs were incorporated to reflect these variations, gaps in locally representative data sources may have influenced the precision of the findings. Second, the estimation of RRs is subject to potential confounding and mediation effects that may not have been fully accounted for. The interdependence of dietary risk factors, such as the tendency for individuals with high fruit intake to also consume more vegetables, complicates the isolation of independent effects. Although major confounders were adjusted for through meta-analyses of observational studies, 20 the possibility of residual confounding cannot be ruled out.
Third, the use of universal effect sizes 20 for dietary and lifestyle risk factors across different populations presents a limitation, as the impact of these risks may vary due to genetic, cultural, and environmental differences. For instance, the metabolic and cardiovascular effects of high BMI may differ across population subgroups due to variations in body composition and metabolic adaptation. To enhance precision, the integration of region-specific risk estimates should be explored in future studies. Finally, the indirect effects of the COVID-19 pandemic on lifestyle-related risk factors were not fully captured. 20 The pandemic may have resulted in shifts in physical activity levels, dietary habits, smoking prevalence, and BMI distribution, but these dynamic changes were not explicitly incorporated into the estimates. As more data become available, future iterations of burden estimates should account for these evolving trends.
Conclusions
Despite these limitations, valuable insights into the health impact of modifiable lifestyle risks in Qatar have been provided in this study. The findings reveal the growing burden of lifestyle-related NCDs in Qatar, with high BMI emerging as the dominant risk factor, surpassing traditional risks like smoking and poor diet. While progress has been made in reducing smoking-related mortality, the increasing prevalence of obesity, physical inactivity, and unhealthy dietary patterns presents a significant public health challenge. The results highlight the urgent need for a comprehensive, multi-sectoral strategy integrating taxation, regulation, health promotion, and clinical interventions to address these modifiable risk factors. Targeted interventions should prioritize reducing obesity rates. Additionally, gender- and age-specific approaches, such as smoking cessation programs for males and weight management initiatives for middle-aged adults, are crucial for effective disease prevention. Given that the critical barrier to addressing lifestyle-related NCDs is the scarcity of high-quality, country-specific data on lifestyle behaviors, 20 researchers should explore lifestyle risk factors for NCDs using primary data. Systematic efforts to collect and organize local lifestyle risk factors data using up-to-date methods and technologies are essential.
Supplemental Material
Supplemental Material - The Impact of Unhealthy Lifestyle on the Burden of Non-Communicable Diseases in the State of Qatar: A Systematic Analysis of the Global Burden of Disease Study 2021
Supplemental Material for The Impact of Unhealthy Lifestyle on the Burden of Non-Communicable Diseases in the State of Qatar: A Systematic Analysis of the Global Burden of Disease Study 2021 by Yohannes Adama Melaku, Maya Bassil, Reema Fayez Abdulfattah Tayyem, Tahra ElObeid, Lijun Zhao, Sam Manger, Danny J. Eckert, Robert Adams, and Zumin Shi in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors acknowledge the Institute for Health Metrics and Evaluation (IHME) for providing access to the GBD data. We also thank the broader GBD collaborative network for their contributions to data collection, analysis, and interpretation.
Author Contributions
YAM: Conception, data collation and interpretation, first draft preparation, critical revision, content expertise and overall lead of the project. MB, RFAT, TE, LZ, SM, DJE, RA & ZS: Contribution to data interpretation, content expertise and critical revision of the manuscript. ZS: Conception, content expertise & supervision. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.