
Abstract
The aim of this study is to investigate whether there are associations between physical fitness and loneliness in older adults, and whether these associations are mediated by psychological distress, an important factor which remains still controversial in this population. One hundred and thirteen older adults (71.71 ± 6.66 years; 75 women), were evaluated of physical fitness (cardiorespiratory fitness, balance, and upper limb strength), loneliness, and psychological distress (depression, anxiety, and stress). Independent mediation analyses were run with PROCESS macro for SPSS. Cardiorespiratory fitness, balance, and upper limb strength significantly and negatively predicted depression (all P < 0.050). Balance predicted significantly and negatively anxiety (P < 0.050). Depression predicted significantly and positively loneliness. Although we did not find any direct effect between physical fitness and loneliness, mediation analyses indicated that lower levels of cardiorespiratory fitness, balance and upper limb strength were associated with higher loneliness via higher levels of depression. These findings support the idea that psychological distress (particularly depression) has an important role in the link between physical fitness and loneliness in older adults.
“Depression was a common significant mediator in the relationship between cardiorespiratory fitness, balance and upper limb strength with loneliness.”
Introduction
Loneliness is defined as an unpleasant experience of a discrepancy between one’s desired and actual network of social relationships. 1 This negative feeling tends to increase with age 2 with prevalence data around 25-30% in older adults (individuals aged 60 and older),3,4 which makes it a relevant problem because of the number of people affected, but also because of the negative consequences on health.
In line with this, previous research has suggested that loneliness is associated with a poorer perceived health, 5 and a high risk for cardiovascular disease. 6 But the importance of loneliness in older adults has been centered on the associations established with mental health problems such as psychological distress (including anxiety, depression, and stress symptoms). 7 For example, some studies have shown that the association between loneliness and depression is bidirectional but stronger and more robust for depression as the initial symptom. 8 Similarly, Domènech-Abella et al. 9 found a longitudinal association between experiencing loneliness and higher likelihood of suffering from an anxiety disorder 2 years later. In the same way, other studies have reported that loneliness and perceived stress mutually predict each other over time. 10
In this context, regular physical activity has emerged as a strategy able to mitigate loneliness and mental health problems.11-14 The importance of physical activity is explained because it increases and/or preserves levels of functionality and physical fitness. Physical fitness can be defined as having the strength, balance, cardiorespiratory fitness, mobility, and coordination necessary for performing activities of daily living, thus allowing for physical independence and preserved quality of life.15,16 Physical fitness is an important marker of health in aging,17,18 and lower levels of physical fitness may contribute to loneliness through reduced capability to join in common social activities such as going out with friends, visiting relatives or traveling. However, there is still a scarcity of studies that look at the possible links between levels of physical fitness and feelings of loneliness. A prospective cohort study found that decrease in upper limb strength may be independently associated with a modest increase in loneliness among men below the age of 80 years. 19 Another interesting study found that cardiorespiratory fitness was the most efficient variable as loneliness predictor, followed by upper limb strength. 20 These studies highlight the importance of physical fitness in older adults in reducing their loneliness risk. Conversely, other authors found no relationship between physical fitness and loneliness status. 21 Therefore, these conflicting findings point out the need to go deeper into this topic.
On the other hand, physical fitness is also a strong predictor of mental health in older adults. 22 In this regard, recent evidence has shown the important protective role of physical fitness on psychological distress in aging. For instance, the systematic review of Kandola et al. 23 found a longitudinal association between cardiorespiratory fitness and the risk of depression and anxiety. Zasadska et al. 24 demonstrated a relationship between low muscle strength measured with the handgrip strength test and intensified depressive symptoms in older population. Likewise, other authors have reported that the 5 times sit-to-stand test—a measure to assess lower limb strength—is a predictive tool for depression in older adults. 25 Moreover, impaired body balance is among the most common causes of falls and negatively influence psychological distress.26,27
Summarizing, both physical fitness and loneliness are related to psychological distress in aging, but the association between physical fitness and this feeling of loneliness is still controversial. Thus, we tested a mediational theoretical model (Figure 1) in which we hypothesized that physical fitness would have an indirect impact on loneliness trough the effect on psychological distress (i.e., depression, anxiety, and stress). To the best of our knowledge, no studies have investigated this model before in older adults. Graphic of the hypothesized mediation model.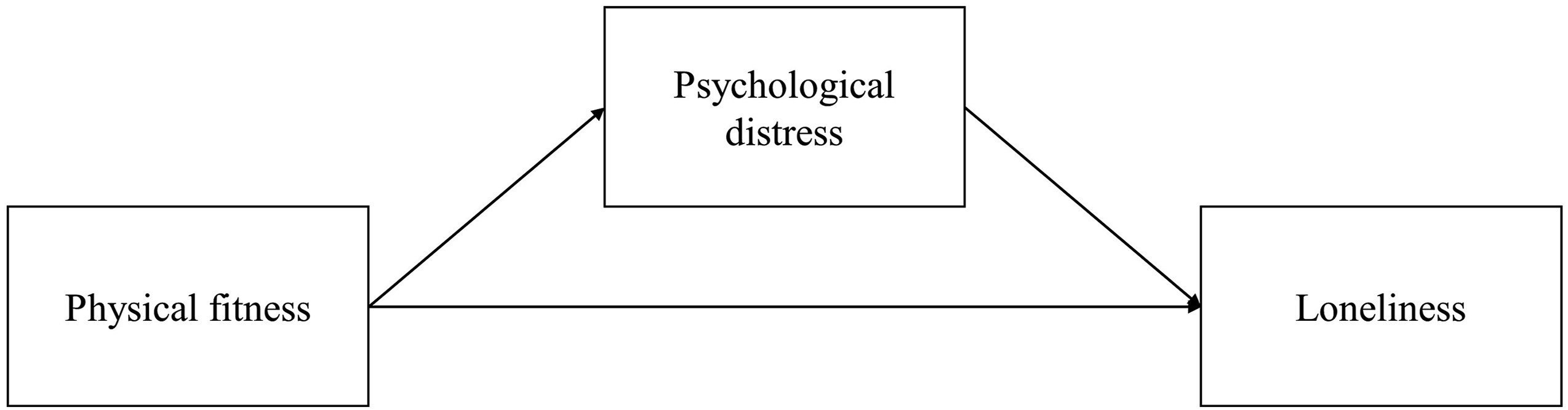
Methods
Data Source and Study Population
A total of 130 older adults participated in this study. They were recruited through a local public university and public health care facilities in Valencia, Spain (from September 2022 and September 2023). Recruitment was based on a medical derivation regarding the following criteria: aged 60 years or older and able to participate in 1 session of physical exercise. Exclusion criteria were presence of any disorder that would prevent physical activity, and present at least a 24-point cut-off in the Mini Mental State Examination 28 since participants needed a minimum cognitive status to face the questionnaires and functional test. Based on meeting these criteria, all participants received information from their primary care physician about their participation in a research program. Seventeen individuals did not meet the inclusion/exclusion criteria. Ultimately, a total of 113 participants (71.718 ± 6.66 years; 75 women) were included in the statistical analyses.
The study adopted a cross-sectional design with 2 days of data collection separated by about 48 hours. Blood pressure, oxygen saturation and heart rate were measured on both days, after 10 minutes of rest. For the final analysis, the average of the 2 days was taken. The first day of assessment included height and body composition by bioimpedance followed by the questionnaires of cognitive status, loneliness, and psychological distress. Finally upper limb strength was assessed. On the second day, participants were evaluated for balance, lower limb strength and cardiorespiratory fitness. All measurements were performed under standardized conditions and testing sessions were scheduled at similar time of the day for each participant in fasting conditions to minimize potential effects of diurnal variation. 29
All participants were informed about the experimental procedure and signed the written consent of this study that complies with the ethical standards of the Declaration of Helsinki 2013 and was approved by the ethics committee of the Hospital Clinico Universitario INCLIVA.
Independent Variables
Physical Fitness was Assessed Through the Following Tests
Dependent Variables
Mediation Variables
Other Variables
On both days, as soon as they arrived at the facility where the tests were carried out, the participants rested for 10 minutes in a chair. Arterial oxygen saturation (SpO2) and Heart Rate (HR) were determined with a pulse-oximeter attached in the middle finger of the left hand (WristOx2-3150; Nonin, Plymouth, MN, USA), in a sitting position. Blood pressure was also measured 3 times on the left arm with the arm tensiometer Omron M3 Intellisense (HEM-7051-E) (Omron Health care, Kyoto, Japan). In addition, we retained the mean values of systolic and diastolic blood pressure (SBP, DBP) to characterize the sample. On first day and after these assessments
Statistical Analysis
We performed the data analysis using SPSS v. 27 (IBM Corp, 2020; Armonk, NY, USA) employing a statistical significance at P < 0.05. Descriptive analyses were calculated to describe the sample characteristics. The missing values of the item questionnaires were replaced by the item dimension means (2 missing values for DASS-21; 1 for depression and 1 for stress), or the total score mean (6 missing values for the R-UCLA). A post-hoc power analysis was conducted to evaluate whether the sample size was sufficient for testing the hypothesized model adequately. To this end, the achieved power to detect misspecification of a model with a sample size of n = 113, and df = 111 was calculated for the corresponding to Root Mean Square Error of Approximation = 0.06 on an alpha error of 0.05. This post-hoc was conducted with a semPower package in R. Concerning the hypothesized model (Figure 1), we tested the mediation model, assessing psychological distress (i.e., depression, anxiety, and stress) as the mediator in the relationship between physical fitness and loneliness, using the PROCESS macro 35 with 5000 bootstrap samples and unstandardized regression coefficients (model 4). 36 Independent mediations were run for every physical fitness variable. All the effects were evaluated through 95% bias-corrected confidence intervals (CIs). Effects were considered significant if their confidence intervals did not include zero.
Results
Participant Characteristics.
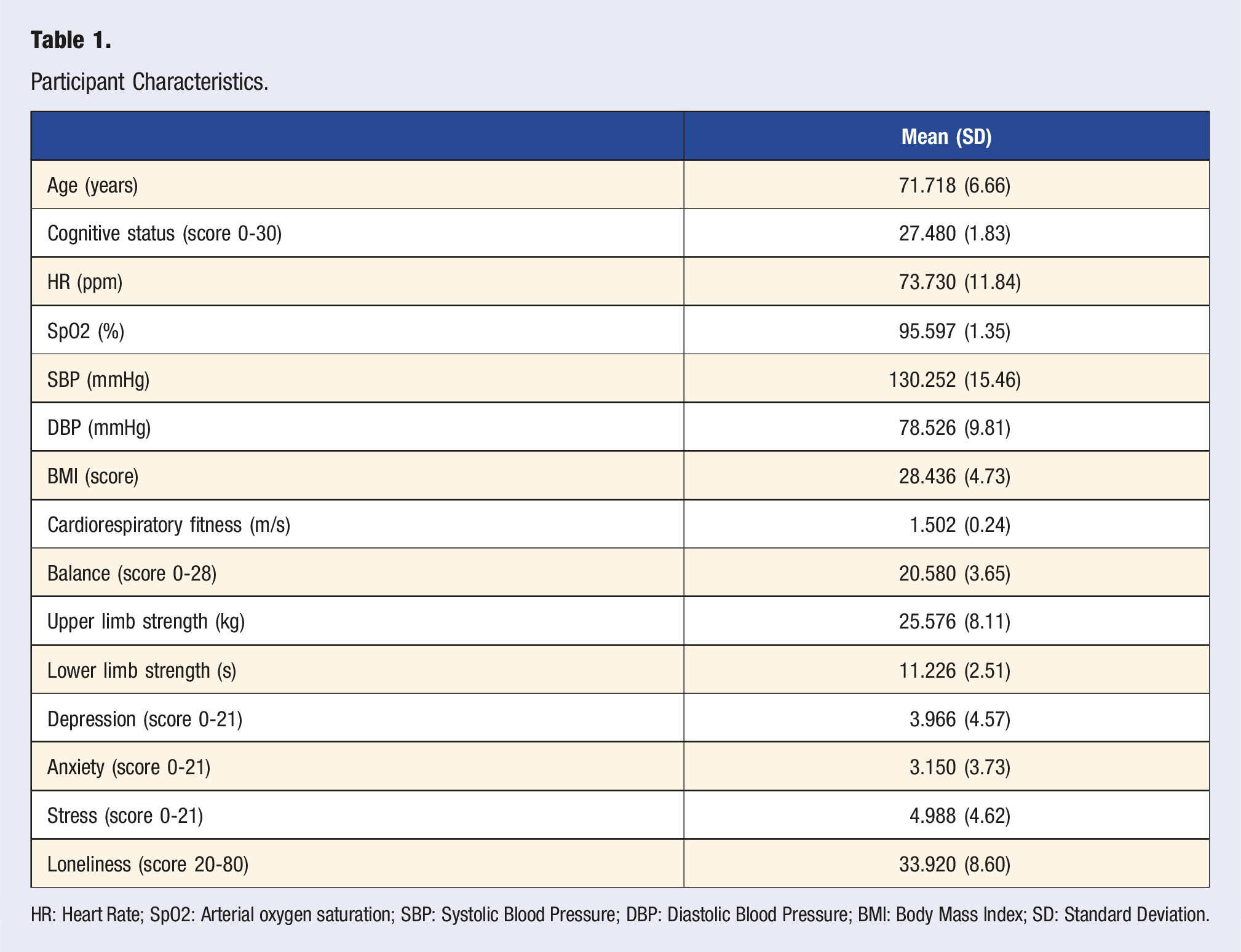
HR: Heart Rate; SpO2: Arterial oxygen saturation; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; BMI: Body Mass Index; SD: Standard Deviation.
Pearson Associations Between Key Variables of Study.
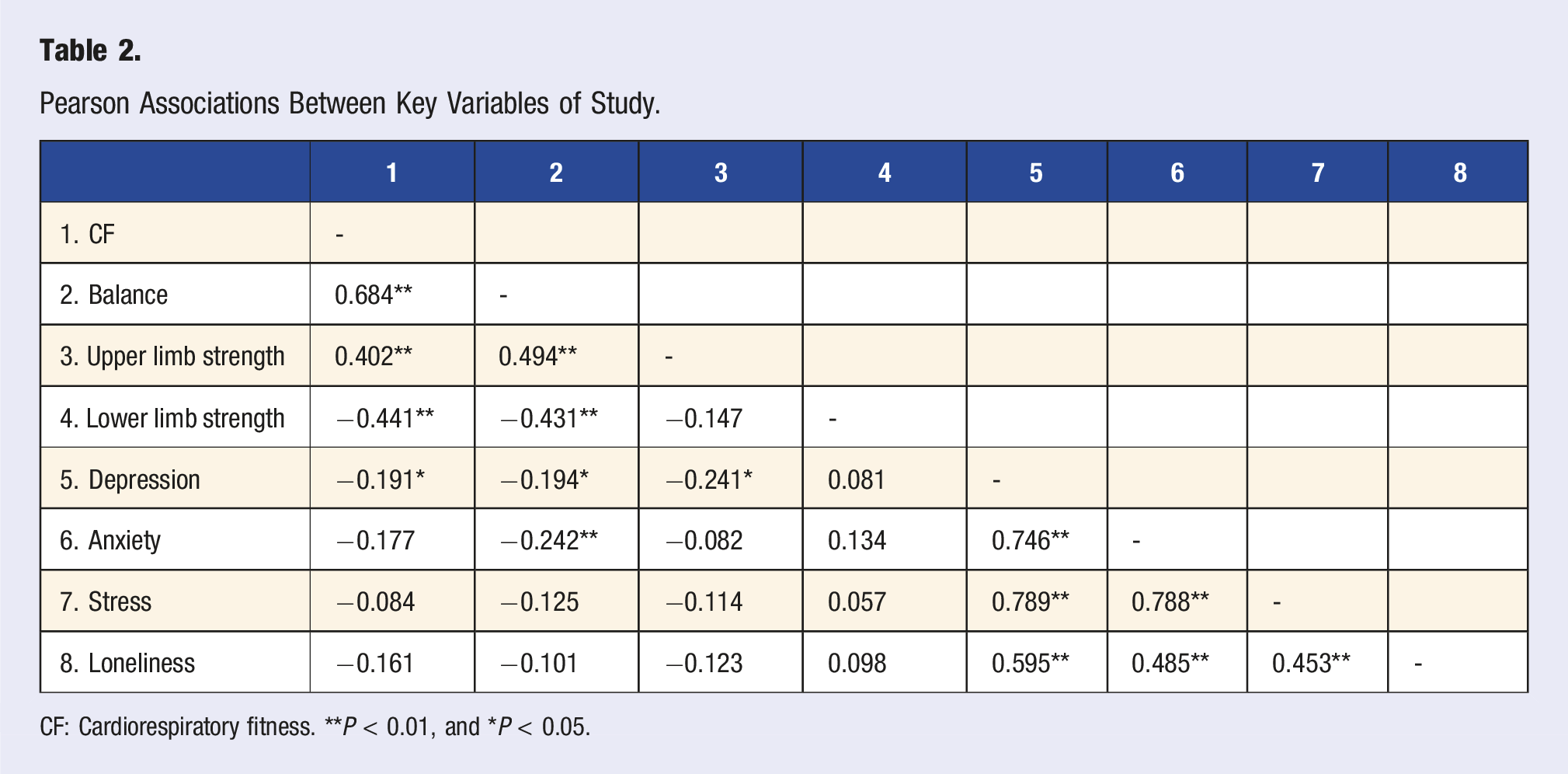
CF: Cardiorespiratory fitness. **P < 0.01, and *P < 0.05.
Although we found no significant correlations between physical fitness variables and loneliness, this is not a rigid requirement to establish the existence of an indirect effect. 37 Therefore, we proceeded to test the hypothesized model. To test whether psychological distress variables (i.e., depression, anxiety, and stress) could mediate the relation between physical fitness variables (cardiorespiratory fitness, balance, upper limb strength, and lower limb strength) and loneliness, mediation models were tested separately.
Regarding the direct effects, cardiorespiratory fitness, balance, and upper limb strength significantly and negatively predicted depression (see Figure 2A,2B, and 2C). Besides, balance also predicted significantly and negatively anxiety. However, we did not find any direct effect between lower limb strength and psychological distress indicators. Among psychological distress variables, only depression predicted significantly and positively loneliness (Figure 2C). Lastly, no direct effects were observed between physical fitness and loneliness. Mediation models for the effect of physical fitness on loneliness, mediated by psychological distress. Significant effects are linked with continuous lines and bolded (p < 0.050). β: Beta coefficient; CI: Confidence interval. a) Mediation model between cardiorespiratory fitness, psychological distress, and loneliness; b) Mediation model between balance, psychological distress, and loneliness; c) Mediation model between upper limb strength, psychological distress, and loneliness; d) Mediation model between lower limb strength, psychological distress, and loneliness.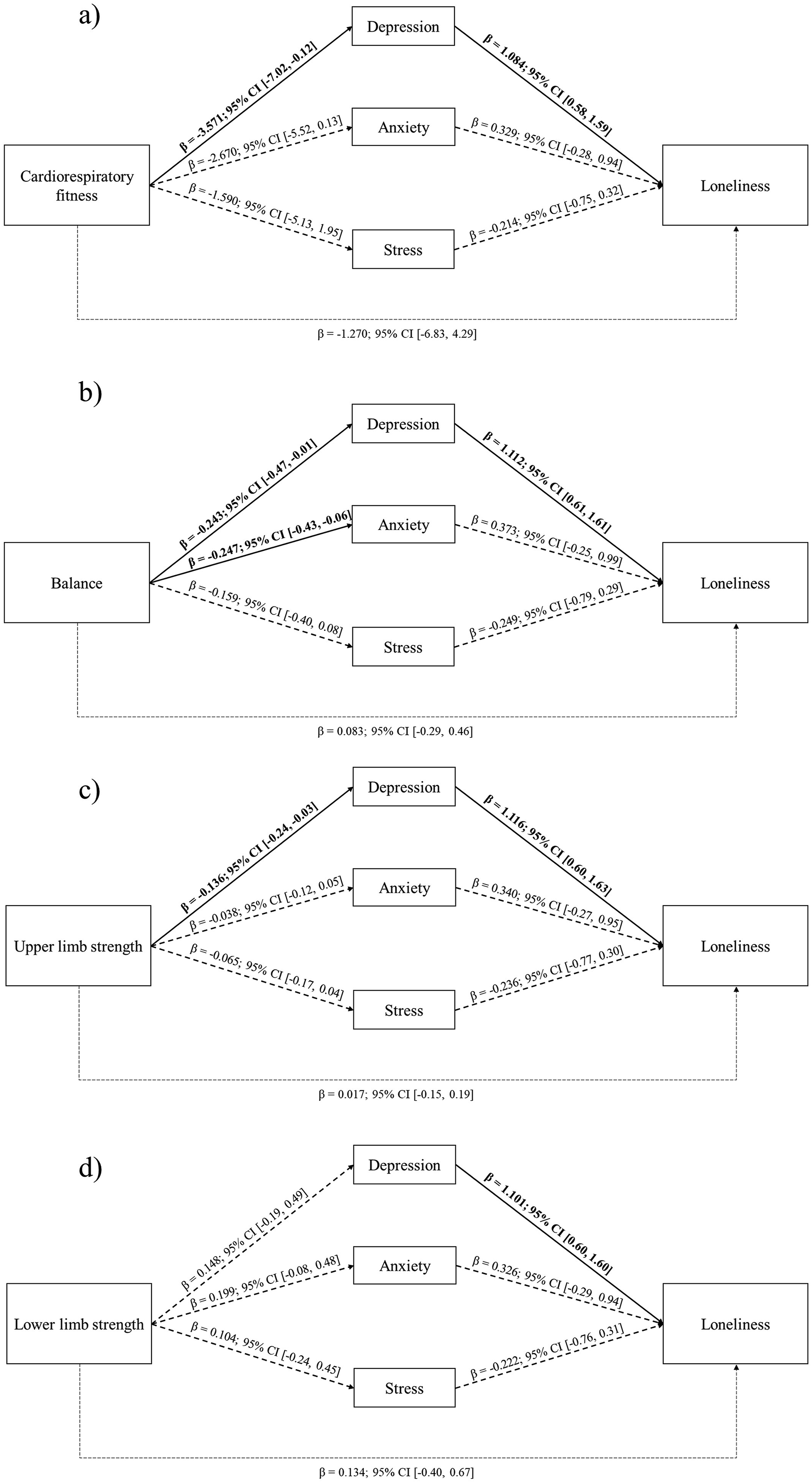
Regarding the indirect effects, a significant indirect negative effect was found for cardiorespiratory fitness (β = −3.873; 95% CI: −8.89, −0.30), balance (β = −0.270; 95% CI: −0.66, −0.03), and upper limb strength (β = −0.152; 95% CI: −0.31, −0.04) on loneliness via depression. Therefore, depression was a common significant mediator in the relationship between cardiorespiratory fitness, balance and upper limb strength with loneliness.
Overall, cardiorespiratory fitness, balance, and upper limb strength accounted respectively for 3.7%, 3.8% and 5.8% of the variance in depression, and for 2.6%, 1.0% and 1.6% of the variance in loneliness.
Discussion
This study examines the relationships between different physical fitness variables (cardiorespiratory fitness, upper limb strength, lower limb strength and balance) and loneliness in older adults and explores whether psychological distress indicators (depression, anxiety, and stress) would mediate these relationships. Our results suggest that cardiorespiratory fitness, balance, and upper limb strength have an important effect on loneliness through depression. These findings contribute to the limited current literature on the association between physical fitness and loneliness in older adults, adding new knowledge about the impact of psychological distress. They also reveal a link between balance and both, anxiety and depression. Additionally, these findings have important public health implications, revealing a possible increasing feeling of loneliness derived from a poor physical and mental health during aging.
On the one hand, our results showed that cardiorespiratory fitness, balance, and upper limb strength were all negatively linked with depression in older adults. Furthermore, balance was also associated with anxiety. These findings confirm previously reported results in the literature that highlight the importance of physical fitness for mental health in older adults. For example, some studies have demonstrated that people with higher cardiorespiratory fitness are at a lower risk of developing depressive symptoms.38,39 Similarly, Marques et al. 40 systematic review findings suggest that muscular strength has a positive effect on reducing depression. Likewise, decreased balance significantly increases the risk of falls, leading not only to physical injuries but also to psychological consequences, such as an increase in depressive symptoms. 41 Consequently, interventions aimed at improving cardiorespiratory fitness, balance and muscular strength have the potential to promote mental health and prevent depression. 42
On the other hand, we found that depression was strongly associated with loneliness. The association between depressive symptoms and loneliness is consistent with previous research findings8,43 and can be understood through the lens of how depression affects interpersonal and cognitive functioning.8,44,45 However, neither anxiety nor stress were associated with loneliness in our study, contrary to other studies that have shown that increased anxiety can elevate levels of experienced loneliness. 46 It might be due to the low outcomes of anxiety and stress in our sample.
Since there are moderate to large associations between loneliness and the three psychological distress factors, reducing the incidence of mental health diseases is essential for mitigating the global mental health burden, 47 including the cost of unwanted loneliness. Indeed, in Western countries like Spain, physical and mental illnesses associated with this unwanted loneliness entail increasing morbidity and risk of death, consequently increasing costs and care resources. 48 Interventions aimed at fostering social connections and community involvement have been shown to improve both mental and physical health outcomes in this population. Therefore, creating accessible community programs that promote social integration for those with functional limitations (e.g., the older adults) is essential for enhancing quality of life and mitigating the negative effects of isolation. 49 This is a topic that remains to be explored.
Regarding the association between physical fitness and loneliness, we found a significant indirect negative effect for cardiorespiratory fitness, balance and upper limb strength on loneliness via depression. Thus, in agreement with our hypothesis, our results imply that while physical fitness may not directly influence loneliness, the presence of depressive symptoms associated to lower condition or unfit physical function among older adults can contribute to variations in loneliness. In other words, being fitter (better cardiorespiratory fitness, balance and upper limb strength) is associated with a lower risk of depressive symptoms, which in turn are associated with less perceived loneliness. Based on our findings, improvements in fitness may underlie improvements in depressive symptoms through various biological mechanisms (autonomic regulation, cortisol balance, inflammation reduction, BDNF secretion). 23 These changes in physical and emotional state would allow older adults to develop their activities in a larger living space, 50 understood as the physical and social extension in which people carry out their daily activities and consequently, could have a positive impact on the social ties and on perceived loneliness. When you feel good about your body and your functional ability, you have less fear of falling, less fear of going out, and improved self-esteem, which results in greater social involvement. 51 Maintaining/enhancing balance may play a key role through in reducing anxiety as well as depression. Accordingly, older adults who maintain a good physical fitness are indirectly less likely to loneliness because they are less likely to experience the depressive symptoms that precede loneliness.
In this manner, interventions aimed to maintaining physical fitness could be vital in preserving functionality and mental health in aging populations.13,52 Functional problems are related to depression 53 and social isolation. 54 Hence, by enhancing physical fitness, older adults sustain higher levels of functionality, reducing the need for assistance with daily activities and potentially delaying the transition to assisted care. Regular exercise is the main pathway to improve physical fitness and functionality and a comprehensive biopsychosocial treatment strategy applicable to a diverse array of chronic diseases. In fact, some authors have shown how holistic interventions based on exercise and socialization combined with health education can help to improve loneliness and fitness in older adults.55-57 In this way, enhancing physical fitness through physical exercise and physical activity is central to an integrated approach to healthy aging, addressing both physical and psychological aspects of health.58,59 Therefore, improved physical fitness contributes positively to mental health and supports greater social engagement, which leads to better overall health.60,61 Our results highlight the importance of integrating physical, psychological, and social interventions to prevent low levels of fitness, and high levels of psychological distress and loneliness in older adults.
The strengths of this study include an adequate sample size in terms of statistical power, and the use of objective tests to assess physical fitness in older adults. However, this study has several limitations. First, the sampling method and inclusion criteria may have created a risk of bias because the examined participants wanted to participate in a session of physical exercise and is very likely that participants with some degree of social isolation, and with moderate to high levels of psychological distress did not want to participate in the study. Moreover, a major part of the sample was female, so sex-differences could influence our results. But the reality is that more and more women take part in physical exercise activities (and cultural and social activities). Surely a gendered look at physical exercise programmes would be of interest, as we could find differences in the type of programmes that some people like more. Another potential limitation is the wide age range of participants (range: 60-88 years old) as there could exist physical and mental differences between them. Furthermore, our sample present low general levels of psychological distress and good levels of physical fitness, so future studies should investigate these associations with clinical populations. Importantly, the cross-sectional design of our analyses prevents us from inferring causal relationships as we possess only a singular snapshot of data. Eventually, a major flaw in this study is the lack of confounders in the mediation analyses. Future studies with robust longitudinal designs that incorporate significant sociodemographic and socioeconomic covariates into these analyses will need to confirm the associations found, thus contributing to the development of knowledge in this field.
In conclusion, our results support that the associations between some physical fitness variables (i.e., cardiorespiratory fitness, balance and upper limb strength) and loneliness were mediated by depression. As such, exercise interventions can help older adults in maintaining and enhancing physical fitness and mental health and live independently and social connected for longer periods, supporting healthy and successful aging. This work adds to the growing literature illustrating the predictive utility of physical fitness in social and mental health. Future studies should deep into how physical fitness might prevent loneliness in the long term. Succeeding to fill this knowledge gap can contribute to promote successful aging globally in the Decade of Healthy Ageing and thus achieve some Sustainable Development Goals (SDGs) as good health and well-being (SDG 3), gender equality (SDG 5), or reduced inequalities (SDG 10).
Footnotes
Acknowledgments
The authors would like to thank all the older adults who participated in the study, as well as general practitioners in the health care centers and The GESMED Foundation (Gestió Socio Sanitaria al Mediterrani) for their continuous support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Conselleria d'Educació, Investigació, Cultura i Esport, CIACIF/2022/368; 2023-2027; Banco Santander; Research Projects in Social Engagement 2022 from Banco Santander - Universitat Jaume I; Gestió Socio Sanitaria al Mediterrani Foundation (GESMED).
Ethical Considerations
All participants were informed about the experimental procedure and signed the written consent of this study that complies with the ethical standards of the Declaration of Helsinki 2013 and was approved by the ethics committee of the INCLIVA (May 2022 and September 2022).
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the conditions provided by the INCLIVA (May 2022 and September 2022) Human Research Ethics Committee. However, final data analysis will be made available on request.