
Abstract
Objective
We aimed to examine the relationship between the prevalence of functional dyspepsia (FD) and lifestyle habits, to identify social factors that may contribute to psychosocial disorders.
Methods
We enrolled 759 university freshmen in this study, who were categorized into the FD group and healthy group. All participants completed the validated Self-Rating Depression Scale and Self-Rating Anxiety Scale questionnaires, to assess lifestyle and social factors among participants.
Results
The proportion of participants with FD was 16.86%, and 67.97% were women. Diet irregularities and sleep impairment may have an effect on FD. Tea consumption may play a role in preventing FD. Participants with FD were more likely to have mood disorders than healthy participants. Most participants with FD who had mood disorders experienced mild anxiety or depression. Participants’ main sources of stress arose from daily life, development, social life, life events, and participants’ daily schedule.
Conclusion
Sex and lifestyle habits, including sleeping patterns and dietary habits, can have an impact on FD. Social stress and mood disorders also have an effect on FD. FD may be prevented by adjusting lifestyle habits and psychological counseling.
Introduction
Functional dyspepsia (FD) is highly prevalent worldwide. The prevalence of FD varies worldwide; in Western countries, the FD prevalence ranges between 10% and 40% and between 5% and 30% in Asia.1,2 Although FD rarely leads to death, it can have an effect on patient quality of life.3,4 To date, no effective treatment to manage this disease is available. 5 Western lifestyle habits, which include consumption of certain types of food, alcohol, and tobacco, are frequently associated with FD symptoms.6,7 However, the relationship between Eastern lifestyle habits and FD remains unknown.
The first Rome classification system was published in 1990; subsequently the Rome I, Rome II, and Rome III classifications were published in 1992, 1999, and 2006, respectively. 8 With publication of the Rome IV classification in 2016, the definition of FD has become clearer and better defined. 9 The mechanism of FD is not well understood but it is known that FD can be caused by motility disorders, acid disorders, and Helicobacter pylori infection, among other causes. However, a significant association has been identified between psychosocial disorders and FD.10–12 The physical symptoms of FD may lead to mood disorders in affected individuals, such as anxiety or depression. This adds to health care costs for patients with FD, in addition to those associated with managing their dyspepsia symptoms.13,14 Psychosocial disorders may result in disturbance of the brain–gut axis, which may lead to FD-associated gastrointestinal symptoms. 15 There are many factors, such as social stress, that are closely associated with anxiety and depression. Thus, clarifying the association between mood disorders and FD and the impact of mood disorders on patients with FD will enable development of effective FD treatment.16,17 The prevalence of FD and mood disorders and the factors affecting patients with FD in Asia, especially China, remain unknown.
In this study, we aimed to examine the prevalence of FD, to identify the relationship between Eastern lifestyle habits and FD, and to identify social factors contributing to psychosocial disorders among patients with FD in China.
Methods
Participants
In this study, we enrolled freshmen at Xi’an Medical University during September to December 2018. Participants were diagnosed with FD using the Rome IV criteria; other diseases were ruled out based on results of the following physical examinations: electrocardiogram, abdominal ultrasound, X-ray scan, and blood tests. Participants were divided in two groups: the FD group and the healthy group.
This study was approved by the Institutional Ethical Committee of Xi’an Medical University. Informed consent was obtained from all participants before the study began.
Lifestyle factors
All participants were assessed with respect to their lifestyle habits, including sleeping pattern, dietary habits (such as having a preference for spicy, hot, raw or cold, or deep-fried foods, dairy foods or products, tea or coffee, chocolate, and other foods), smoking status, and alcohol consumption.
Self-Rating Depression Scale (SDS) and Self-Rating Anxiety Scale (SAS)
All participants were administered the approved Chinese version of the Zung Self-Rating Depression Scale (SDS) and Self-Rating Anxiety Scale (SAS), to identify participants’ anxiety and depression status. Specialist physicians explained the questionnaires to participants such that they were able to complete the examinations independently, without interference from external factors. Using the completed questionnaires, physicians calculated the standardized SAS and SDS scores using the following formula: Y = int (1.25X). SAS and SDS scores above 50 points indicate the presence of anxiety or depression; a score of 50–59 indicates mild anxiety or depression, 60–69 points indicates moderate anxiety or depression, and a score higher than 70 points indicates severe anxiety or depression.18,19
Investigation of social stress factors
All participants were assessed for social stress, including academic stress and the stresses of daily life, development, social life, family, life events, and of their daily schedule.
Statistical analysis
All statistical analyses were conducted using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as mean ± standard deviation (SD). Categorical variables are expressed as frequency and percentage. The t-test was used to compare continuous variables. To compare categorical variables, we used the χ2 test and rank test. A two-sided P value <0.05 was regarded as statistically significant.
Results
Prevalence of FD
A total of 759 university freshmen participated in this study, 287 (37.81%) men and 472 (62.19%) women. Participants were aged 17 to 22 years, with mean age 18.39 ± 1.00. A total 128 (16.86%) participants were categorized in the FD group, 41 (32.03%) men and 87 (67.97%) women (χ2 = 7.1722, P < 0.05). Female participants experienced FD more frequently than their male counterparts.
Lifestyle habits
Among the 128 participants in the FD group, 44.53% (57/128) had insomnia, which was much higher than in the healthy group (174/631, 27.58%) (χ2 = 14.4504, P < 0.05). Freshmen who had sleeping problems were more likely to have FD.
In the FD group, only 58.59% (75/128) of participants ate regular meals; 67.83% (428/631) of healthy participants ate meals on time (χ2 = 4.0603, P < 0.05). A total 52.34% (67/128) of participants with FD preferred specific types of food; however, only 40.41% (255/631) of healthy participants had such preferences (χ2 = 6.2022, P < 0.05). A preference for spicy, hot, raw, or cold foods and dairy foods or products was associated with FD (χ2 = 21.0500, P < 0.01) (Table 1). Drinking tea was associated with FD (χ2 = 2829.8800, P < 0.01); however, there was no association between coffee and FD (χ2 = 0.6515) (Table 2). There was no significant difference between the FD group and healthy group with respect to smoking and alcohol consumption (χ2 values 0.2740 and 0.0313, respectively) (Table 3).
Dietary habits in participants with functional dyspepsia and healthy participants.

FD, functional dyspepsia.
*χ2 = 21.0500, P < 0.01.
Beverage consumption habits in participants with functional dyspepsia and healthy participants.

FD, functional dyspepsia.
*χ2 = 2829.8800, P < 0.01.
#χ2 = 0.6515, P > 0.05.
Smoking and alcohol consumption in participants with functional dyspepsia and healthy participants.
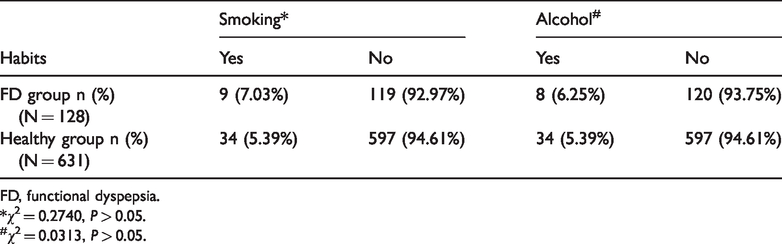
FD, functional dyspepsia.
*χ2 = 0.2740, P > 0.05.
#χ2 = 0.0313, P > 0.05.
Prevalence of mood disorders
Both mean SAS and SDS scores were higher in the FD group than in the healthy group (t values 6.944 and 6.751, respectively; P < 0.01 for all) (Table 4). Compared with scores among the general Chinese population (n = 1158, norm score 29.78 ± 0.46), mean SAS scores were higher in the FD group.
Mean SAS and SDS scores.

FD, functional dyspepsia; SDS, Self-Rating Depression Scale; Self-Rating Anxiety Scale.
*t = 6.944, P < 0.01.
#t = 6.751, P < 0.01.
A total 59.38% of participants with FD had mood disorders; this was much higher among participants in the healthy group (59.38% vs. 22.98%, respectively; χ2 = 68.2974; P<0.05). Most participants with FD who had a mood disorder had mild anxiety (35/39, 89.74%) or depression (54/65, 83.08%) (Table 5).
Mood disorder levels among participants with functional dyspepsia.

*χ2 = 68.2974, P < 0.05.
Social factors
The proportion of patients who experienced mild social stress was higher among participants with FD than that among their healthy counterparts. The frequency of stress arising from daily life, development, social life, life events, and participants’ daily schedule was much higher for freshmen with FD (z values −3.445, −2.040, −3.151, −3.702, and −3.738, respectively; P<0.05 for all). However, there was no significant effect on FD of academic stress and family stress (z values were −1.684 and −0.932, respectively) (Table 6).
Social stress in participants with functional dyspepsia and healthy participants.
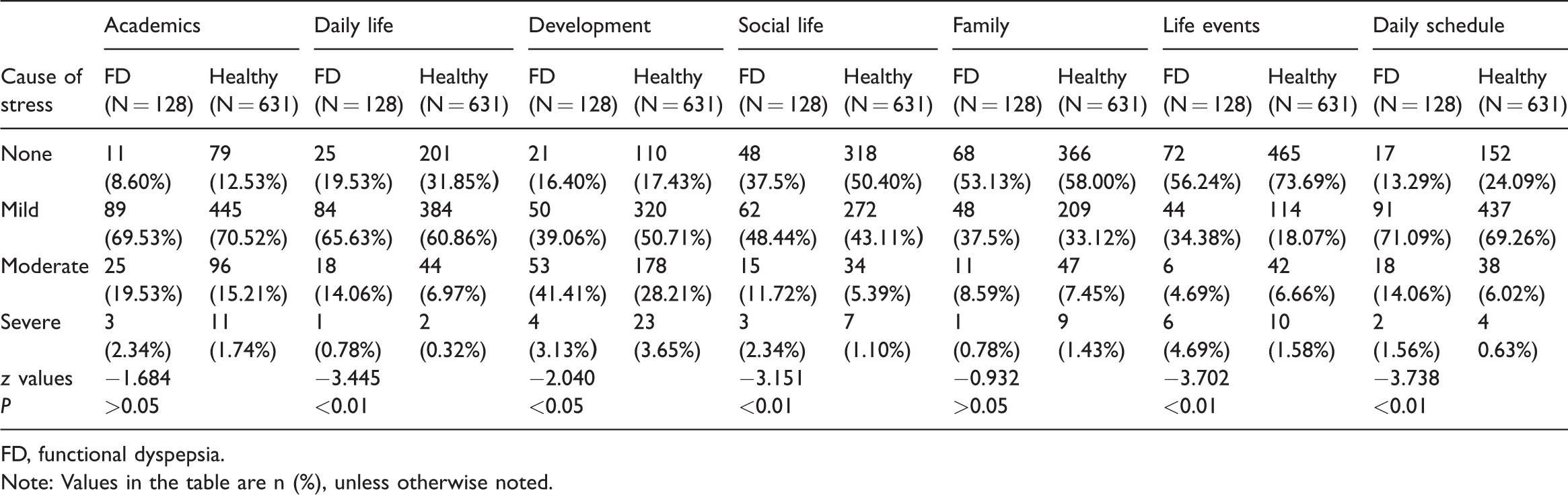
FD, functional dyspepsia.
Note: Values in the table are n (%), unless otherwise noted.
Discussion
FD is a functional gastrointestinal disorder and involves no organic changes. The mechanism of FD is still unknown, but it is very common in populations globally. 20 The prevalence of FD varies from 7% to 45% worldwide.21,22 A large-scale study in France reported an FD prevalence of about 15% to 21%. 23 In Korea, the prevalence of FD is about 46.5%. 5 Multicenter prevalence studies are lacking in China. In our single-center study, the prevalence of FD in younger people was 16.86%, and most individuals diagnosed with FD were women. Our results are the same as those of a previous study.4,24,25 Sex-related differences might have an effect on biological factors, acquired risks, psychosocial characteristics of gastrointestinal symptoms, and healthcare-seeking behavior. 25
Recent studies have suggested that lifestyle and dietary patterns can modify gastrointestinal motor and sensory function, which may have an impact on FD symptoms. The Western diet, which includes fatty foods, alcohol, milk and dairy products, coffee, and red meat, is frequently associated with FD symptoms. 2 In comparison, wheat or grain-based foods, vegetables, and fruits are the main components of Eastern diets. Moreover, cooking styles in Eastern countries, especially in China, differ from those in Western countries. In the present study, we found that consumption of spicy, hot, raw, or cold foods and dairy foods or products were associated with FD symptoms. Tea may play a role in preventing FD; however, coffee had no effect on FD. Eating spicy, hot, raw, or cold foods and dairy as well as eating irregularly can induce FD symptoms, which might be related to hypersensitivity to gastrointestinal hormones and the slowing down of gastric emptying. Gluten and lactose intolerance as well as food allergies could be other important factors.1,6,26 Previous studies have suggested that smoking and alcohol consumption affect the prevalence of FD. Smoking could increase the risk of FD by as much as 50%, and alcohol consumption could lead to the development and aggravation of FD. 27 In our study, participants with FD were more likely to smoke and drink alcohol; however, there was no significant difference between these participants and their healthy counterparts.
Sleep dysfunction may upregulate proinflammatory cytokines, such as tumor necrosis factor-α, interleukin (IL)-1, and IL-6, which can have a profound impact on FD symptoms. 28 Recent studies also suggest that sleep impairment and psychological stress might lead to the development of FD and mood disorders.29,30 In our study, we confirmed that participants who had sleeping problems were more likely to have FD.
FD has been classified as a psychosomatic disease, and the results of the present study showed that anxiety and depression were more common among participants with FD than in healthy people. Most participants with FD had mild anxiety and depression and experienced stress mainly owing to daily life, development, social life, life events, and their daily schedule. Studies conducted in Eastern and Western countries have similarly concluded that Axis I psychiatric disorders might be linked to the complex relationship between the brain and gut disorders.31–33
Conclusion
This study confirmed that the prevalence of FD in China is similar to that in other countries of Asia. Sex, lifestyle habits, including sleep patterns and dietary and drinking habits have an impact on FD. Individuals with FD are more likely to experience social stress and mood disorders. FD may be prevented by changing lifestyle habits and attending psychological counseling.
Footnotes
Acknowledgements
We should like to thank Rong Li, Hui-min Wang and Shu-yong Meng for their assistance with this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant from the Guangzhou Key Medical Discipline Construction Project Fund to Zhen-peng Huang.