
Abstract
Objective: The objective of this study was to test the effect of an online education intervention on providers’ attitudes, beliefs, knowledge, and practices pertaining to antenatal physical activity. Study design: A sample of 181 providers (ie, obstetricians, family medicine physicians, and certified nurse-midwives) was directed to view an online training on antenatal physical activity guidelines, counseling methods, and resources. Providers completed surveys before and 12 weeks after viewing the educational website material. Repeated-measures analyses were conducted to examine the effects of the online education. Results: A total of 164 providers (87.2%) completed baseline and follow-up surveys. After viewing the online training, participants more strongly agreed that it was their responsibility to encourage engagement in antenatal physical activity (P = .02) and believed that women would follow their advice about beginning antenatal physical activity (P = .01). Viewing the website material facilitated an increased confidence in ability to effectively talk with overweight and obese women about physical activity (P = .04) and more frequent advising to begin a moderate-intensity physical activity program for sedentary women (P = .02). Knowledge on antenatal physical activity guidelines also improved. Conclusion: Findings suggest that online educational interventions may be an effective tool in altering providers’ knowledge and practices pertaining to antenatal physical activity.
‘Providers can play a significant role in relaying evidence-based prenatal health behavior information to pregnant women, especially given that a majority of pregnant women report that their health care provider has great influence on their beliefs regarding behavioral change.’
Introduction
There are many maternal benefits associated with antenatal physical activity, such as reduced excessive antenatal weight gain,1,2 improved course of delivery, 3 reduced incidence of gestational diabetes mellitus, 4 preeclampsia, 5 reduced physical discomforts associated with pregnancy, 6 and many psychological benefits.7,8 Moreover, among women free of obstetric complications, physical activity during pregnancy poses no risk to fetal outcomes, even among women who initiate physical activity at various points during pregnancy. 9 Despite these recommendations, only 15% of pregnant women meet guidelines for leisure-time physical activity 10 ; pregnant women engage in less-regular antenatal physical activity than their nonpregnant counterparts 11 ; and activity levels tend to decrease throughout pregnancy. 7 These low rates may, at least partly, be a result of the fact that many health care providers are unaware of the national guidelines for antenatal physical activity and/or may not feel confident in their ability to provide counseling on antenatal physical activity.12-16 Both the American Congress of Obstetricians and Gynecologists (ACOG) and the Department of Health and Human Services (DHHS) recommend engagement in regular antenatal physical activity for women without obstetrical complications,17,18 specifically at least 30 minutes of physical activity on most if not all days of the week, with a goal of a total of 150 minutes of moderate-intensity exercise per week. Given the numerous benefits of being active during pregnancy coupled with the current low rates of antenatal physical activity, it is clear that pregnancy is a critical time in a woman’s life to engage in physical activity. 7
There is a lack of patient knowledge concerning the safety of exercising during pregnancy, and pregnant women state that receiving information about the safety of exercising during pregnancy would facilitate engagement in physical activity.19-21 Limited findings suggest that pregnant women typically learn about physical activity from friends and family more often than from providers, and the information they receive tends to be inaccurate, often discouraging them from exercising. 22 Providers can play a significant role in relaying evidence-based prenatal health behavior information to pregnant women, especially given that a majority of pregnant women report that their health care provider has great influence on their beliefs regarding behavioral change. Studies have demonstrated that brief counseling on behavioral change by providers increases the likelihood that the patient will adopt the behavior. 23 Unfortunately, providers’ knowledge may not be congruent with current recommendations based on national guidelines. Recent studies have shown that a significant number of providers have limited knowledge of antenatal physical activity guidelines, may not be aware that heart rates can go above 140 beats per minute (bpm), and lack confidence in providing counseling, and the majority fail to discuss physical activity with sedentary women.24-26
Given providers’ frequent contact and informative position, they are poised to increase women’s understanding, beliefs, and behaviors related to antenatal physical activity. However, little is known about current attitudes, beliefs, and practices among providers on antenatal physical activity. Extant studies consist of convenience samples of obstetricians in private/small group practices.25,26 A recent study by Leiferman et al 24 found that the majority of providers correctly believe that regular prenatal physical activity is associated with numerous improved maternal and child outcomes. However, 30% to 40% of providers lack confidence in providing antenatal physical activity counseling, and approximately 60% often fail to talk with sedentary women about becoming physically active. 24 Clearly, there is a need to enhance both knowledge and skill building for antenatal physical activity counseling among providers.
To provide accurate and effective counseling, providers must be aware of the most current recommendations, including the benefits and risks to engaging in physical activity during pregnancy. In addition, they need to feel confident in providing brief counseling to help a patient come up with an exercise plan and refer patients to community resources for antenatal physical activity. Web-based information and continuing medical education (CME) opportunities informing providers of the current guidelines and methods for providing antenatal physical activity counseling is one potential avenue to improve rates of antenatal physical activity counseling during pregnancy.
Given the limited time available to spend with women in most primary care settings, one can only realistically expect providers to provide brief counseling on antenatal physical activity; thus, educating providers on the most efficient and effective counseling techniques is critical. The purpose of this study was to test the effects of online educational materials (ie, website and CME information pertaining to antenatal physical activity current guidelines, community resources, and brief counseling methods) on providers’ (ie, obstetricians, family medicine practitioners, and certified nurse-midwives) attitudes, beliefs, knowledge, and practices regarding antenatal physical activity.
Materials and Methods
Prior to conducting this investigation, the study protocol was approved by the institutional review board at the respective institution in Denver, CO. A provider was eligible to participate in the study if he/she was a physician (ie, practicing in obstetrics or family medicine) or a certified nurse-midwife (CNM) who was currently practicing in the Denver-Aurora Metropolitan Statistical Area. Eligible providers who met the study inclusion criteria were identified through the local chapters of the American Academy of Family Medicine, Certified Nurse Midwives, and the American College of Obstetricians and Gynecologists. A total of 575 providers (212 family medicine practitioners, 259 obstetricians, and 104 CNMs) were asked to participate in the study. Providers completed a survey at baseline and then again approximately 3 months after participating in online education about antenatal physical activity. The survey was developed from an initial pool of approximately 75 items based on formative work and a previously published survey. 26 An expert panel then pilot tested the survey providing both quantitative and qualitative feedback. Standard item-scale diagnostics and panelist ratings informed the retention of items. More data about survey development and baseline results have been previously presented. 24 At baseline, 188 providers in 1 of 3 specialties (ie, 91 obstetricians, 40 midwives, and 57 family medicine physicians) completed a 39-item survey to assess their current attitudes (eg, “It is an important responsibility of mine to discuss physical activity with my pregnant women”), beliefs (eg, “Exercise during pregnancy improves the health for the mother”), perceived barriers (eg, “To what extent does a) insufficient time, b) inadequate knowledge, and c) uncertainty skills/uncertainty about available resources prevent you from administering physical activity counseling to your pregnant women”), knowledge of guidelines and contraindications to exercise during pregnancy, and current practices (eg, providing counseling, handouts, referrals) pertaining to antenatal physical activity counseling (for more details about the baseline survey please see Leiferman et al 24 ). The majority of questions had 5-point Likert response sets. On completion of the survey, providers were directed to the study website (http://mybabymymove.ucdenver.edu/) to receive online education on current guidelines, safety considerations, and resources (eg, patient handouts, local and national resources) as well as an optional 1-credit CME opportunity pertaining to antenatal physical activity counseling using the 5As framework. 27 The study website houses information regarding current antenatal physical activity guidelines, contraindications to exercise, and benefits of physical activity as well as provides physical activity resources (eg, patient handouts, links to community resources). The website also houses a 1-credit CME that aims to (1) increase provider awareness of the 2002 ACOG and 2008 DHHS guidelines for antenatal physical activity, (2) increase knowledge regarding benefits of antenatal physical activity, (3) develop skills to increase self-efficacy and intent to provide antenatal physical activity counseling, and (4) identify local and national resources for promotion of antenatal physical activity. The main objective of the CME is to enhance providers’ knowledge on the current antenatal physical activity guidelines and how to assess physical activity status, develop an exercise prescription, help patients agree on goals and overcome perceived barriers, and arrange for necessary support via community resources and patient handouts. The web-based CME conveyed evidence-based practices targeting critical information in multiple formats—powerpoint slides, text, and case-based video vignettes—and took approximately 30 minutes to complete.
Approximately 3 months after completing the baseline survey and being directed to the study’s website, a follow-up survey was mailed to all 188 providers who completed the baseline survey. Respondents were contacted via email (n = 171; 91%) and postal service mail because a small group of participants did not provide an email address (n = 17). After 2 contact attempts by email, those who did not respond were mailed a hard copy of the survey.
Study data were collected and managed using the Research Electronic Data Capture System (REDCap), a secure, web-based application designed to support data capture for research studies. 28 Prior to completing the web-based survey, participants were presented with an information page that included an informed consent form describing the purpose of the study, criteria for participation, confidentiality measures, incentive details, and contact information for the principal investigator and study coordinator. Participants were also reminded that their responses pertained to only pregnant women who were free of obstetric complications. Agreement to participate was confirmed by clicking on a “Continue” button, which directed users to the survey. After completing the survey, participants were redirected to a separate, secure web page, where they entered their name and email address; this information was needed to receive the incentive (a $15 gift card). Contact information was stored in a separate database such that it could not be linked to survey responses. Individuals who elected to complete the paper survey provided written informed consent, and data were entered using double data entry into the REDCap database. The majority responded by web (n = 147; 89.6%), with only 10% (n = 17; 10.4%) completing the paper surveys. Descriptive statistics and standardized paired t tests were computed using SAS Version 9.2. Data were collected at the completion of each CME by individual online surveys to evaluate the participant’s learning (pretest/posttest) as well as to receive feedback on the perceived satisfaction and quality of the CME (data not reported here). Website access was evaluated by self-report data collected at the follow-up survey. Participants were asked whether or not they viewed the study’s website (yes/no).
Results
Of the follow-up sample of 164 providers, approximately half of the respondents identified as obstetricians (n = 78; 48%), whereas family medicine practitioners and CNMs comprised smaller proportions of the sample: n = 53 (32%) and n = 33 (20%), respectively. The majority of respondents were female (n = 116; 71%), white (n = 150; 93%), non-Hispanic (n = 156; 97%), and practicing in an urban setting (n = 93; 57%). See Table 1 for descriptive statistics for the full sample and by specialty. Providers had the option of viewing the website and/or completing a 1-hour CME to learn more about helping women set goals related to antenatal physical activity. Approximately 58% (n = 94) of the sample viewed the website, of which 36% (n = 34) viewed the CME portion as well.
Sample Description.
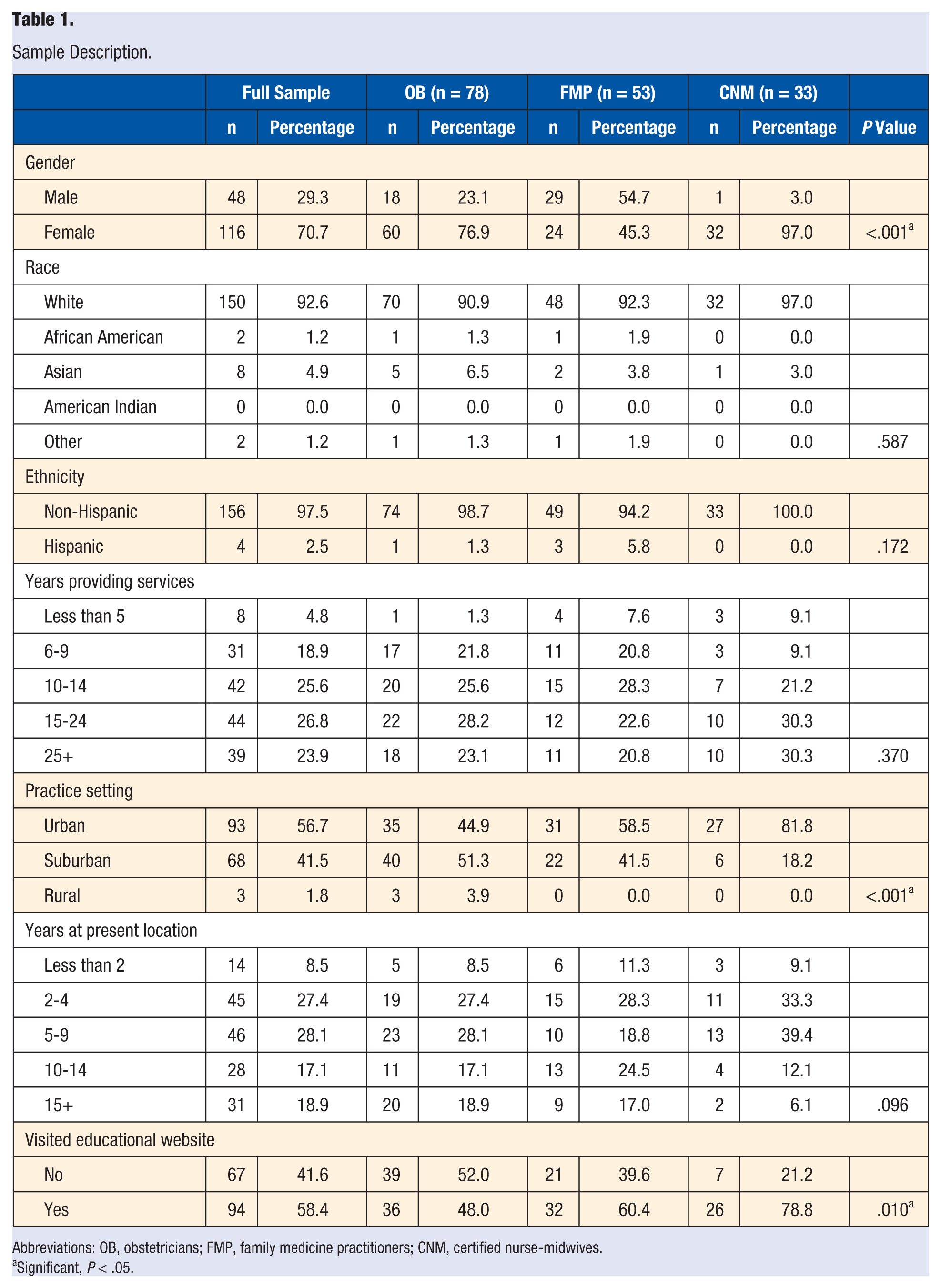
Abbreviations: OB, obstetricians; FMP, family medicine practitioners; CNM, certified nurse-midwives.
Significant, P < .05.
Mean differences in providers’ attitudes, beliefs, self-efficacy, and perceived barriers from pretest/posttest surveys are presented in Table 2. At baseline, most providers agreed that it was an important responsibility to discuss physical activity with their pregnant women and important to encourage them to engage in 30 minutes of physical activity each day. After visiting the website, participants more strongly agreed that it was their responsibility to encourage 30 minutes of physical activity (t = 2.36; df = 93; P = .02).
Attitudes, Beliefs, Self-efficacy, and Barriers Reported in Pretest and Posttest Surveys.
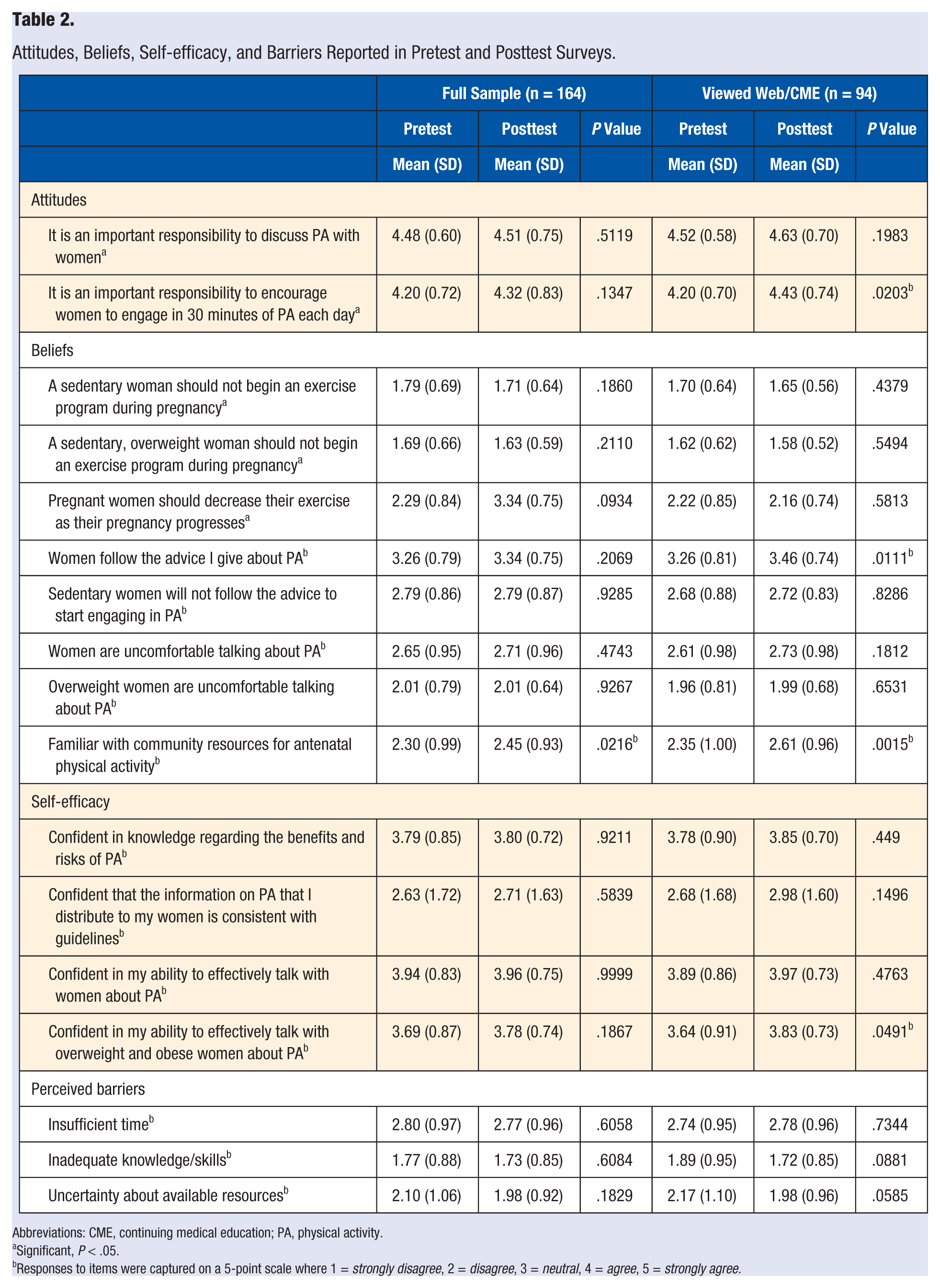
Abbreviations: CME, continuing medical education; PA, physical activity.
Significant, P < .05.
Responses to items were captured on a 5-point scale where 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
At baseline, most providers believed that sedentary/overweight women who are free of obstetric complications should begin an exercise program. Most believed that overweight and/or sedentary women are uncomfortable talking about antenatal physical activity and that they will not follow the advice to start engaging in antenatal physical activity. After viewing the website, providers were more likely to believe that women would follow their advice on physical activity (t = 2.59; df = 92; P = .01). At the posttest, all providers reported increased familiarity with community resources (full sample: t = 2.32, df = 158, P = .02; web only: t = 3.27, df = 90, P = .001).
At baseline, most providers reported a medium (ie, 3 to 4 on a 5-point scale, where 5 was the greatest confidence and 1 was not confident) level of confidence in their knowledge regarding the benefits and risks of physical activity, their ability to effectively talk with women about physical activity, and their ability to effectively talk with overweight and obese women about physical activity. Respondents were least confident that the information they distributed to their patients who are pregnant was consistent with current guidelines about antenatal physical activity. After viewing the website, there was a significant increase in providers’ confidence in their ability to effectively talk with women who are overweight or obese about physical activity (t = 1.99; df = 91; P = .049).
Providers’ perceived barriers to providing antenatal physical activity counseling are shown in Table 2. Providers indicated that insufficient time and, to a lesser extent, uncertainty about available resources and inadequate knowledge/skills were barriers to providing antenatal physical activity counseling. Providers who viewed the website reported lower uncertainty about available resources and inadequate knowledge and skills pertaining to antenatal physical activity counseling, both trending toward significance (t = 0.51, df = 161, P = .06; t = 1.72, df = 91, P = .08, respectively). As displayed in Table 1, there were significant differences in percentages of providers who viewed the website, with more of the CNMs viewing the website (79%; n = 26) when compared with family medicine practitioners (60%; n = 32) and obstetricians (48%, n = 37; F = 4.72; df = 2; P = .01).
Table 3 provides results for knowledge and practice outcomes. At baseline, for the full sample, the majority of providers were able to identify exercises that are considered safe for pregnant women (90%; n = 169), the warning signs to terminate exercise (71%; n = 133), and contraindications to antenatal physical activity (86%; n = 162). However, at baseline, approximately 30% (n = 56) did not know when to terminate physical activity during pregnancy, and about 57% (n = 107) were not familiar with the current recommendations regarding heart rate during exercise. Many providers also reported less familiarity with DHHS guidelines for 150 min/wk of physical activity (52%; n = 98 correctly responded) and the current heart rate recommendations (43%; n = 81 correctly responded). Knowledge improved on the posttest for all providers for 3 items: the identification of safe exercises (t = 2.72; df = 163; P = .007), familiarity with DHHS guidelines for 150 min/wk of physical activity (t = 7.00; df = 162; P < .0001), and heart rate recommendation (t = 2.52; df = 162; P = .01). There was a slight change (although insignificant) in the percentage of patients with whom the provider discussed antenatal physical activity from baseline to follow-up assessment (67.4% at baseline to 68.9% posttest) and a larger change among providers who viewed the website (67.3% at baseline to 80.0% posttest).
Results of Knowledge and Current Practices Reported in Pretest and Posttest Surveys.
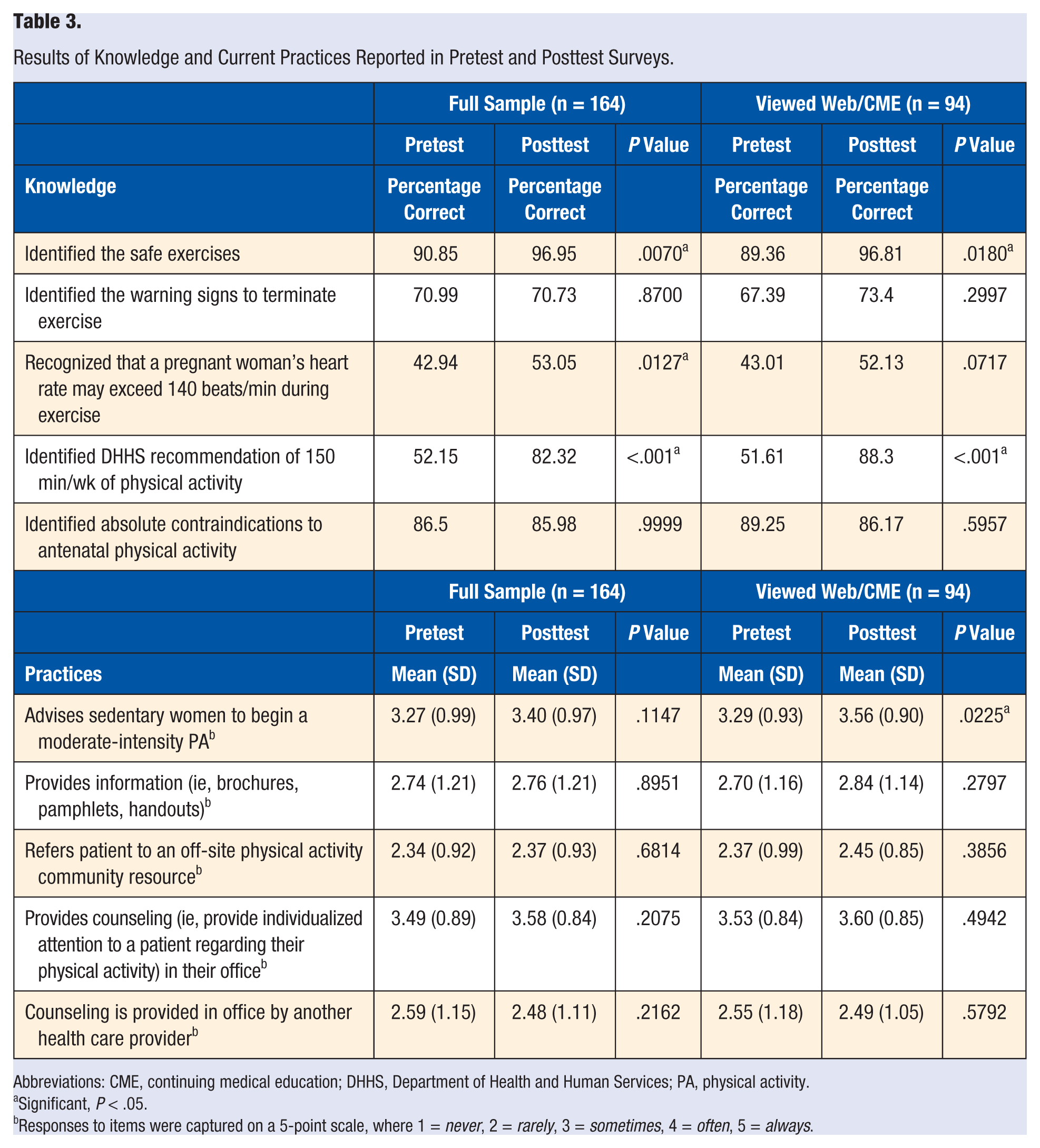
Abbreviations: CME, continuing medical education; DHHS, Department of Health and Human Services; PA, physical activity.
Significant, P < .05.
Responses to items were captured on a 5-point scale, where 1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always.
Table 3 displays providers’ current practices. Providers indicated that they specifically discuss physical activity with two-thirds of their pregnant women. Providers also stated that they sometimes advise sedentary women to begin physical activity and provide counseling regarding physical activity (means were between 3.2 and 3.5 on a 5-point scale, where 3 = sometimes and 4 = often). After viewing the website, providers were more likely to advise sedentary pregnant women to begin antenatal physical activity (t = 2.32; df = 90; P = .02). Overall, providers indicated that they rarely to sometimes provide information, refer a patient to an off-site resource, or refer to another health care provider for physical activity (means were between 2.3 and 2.8 on a 5-point scale, where 2 = rarely and 3 = sometimes).
Conclusions
Despite the numerous benefits associated with antenatal physical activity, rates among pregnant women are low. Recent studies have shown that a significant number of providers have limited knowledge of antenatal physical activity guidelines, may not be aware that heart rates can safely go above 140 bpm during exercise, and lack confidence in providing counseling; the majority fail to discuss physical activity with sedentary women.24-26 In this study, we demonstrate that a low-intensity web-based intervention directed at providers improved knowledge, perception of importance, confidence in counseling, and reported rates of counseling for antenatal physical activity.
The majority of providers in our study recognized the importance of antenatal physical activity. This is similar to previous work by Bauer et al, 26 who demonstrated that the majority of providers (i.e. MDs, DOs, and CNMs)—who completed a 31-item survey reported that antenatal physical activity was beneficial. However, our findings highlight that many providers have inadequate knowledge about antenatal physical activity, including failure to identify the DHHS and ACOG guidelines and not knowing that a pregnant woman’s heart rate may exceed 140 bpm during exercise. When asked about their practice with respect to antenatal physical activity, in our study, less than 70% of providers said that they specifically discussed physical activity. This is consistent with previous research suggesting that less than half of patients report that providers talked to them about physical activity or related health outcomes such as weight gain during pregnancy.24,29,30 This is also consistent with recent work by Bauer et al, 26 who found that 66% of physicians’ offices give guidance to pregnant women on exercise. However, Bauer et al 26 found that this percentage was much higher among CNMs’ offices, which reported that most (99%) provide guidance to their pregnant patients. A limitation to many of these previous studies focusing on patient-provider communication is the lack of understanding of the quality of guidance received. A recent study suggests that much of the guidance received is often limited to handouts in initial patient packets, with few patients receiving additional guidance. 31 In our study, rates were also low for providing information and referring to physical activity community resources. Our web-based intervention improved several of these factors. On completion of the intervention, providers significantly improved their recognition of the guidelines, their ability to identify exercises that are safe during pregnancy, and their familiarity with community resources for antenatal physical activity. These providers also demonstrated significant improvement in the belief about the importance of antenatal physical activity counseling and confidence in their ability to talk effectively with overweight and obese women about antenatal physical activity. However, there are several areas that did not significantly improve as a result of the intervention. There was no significant change in perceived barriers (although there was a trend effect in the expected direction) or the majority of questions targeting self-efficacy. This may, at least partly, be a result of the fact that not all providers who went to the website completed the CME, and most of the content about addressing barriers and enhancing self-efficacy was in the CME, not the website.
There are important limitations to our study. Although our response rate for the follow-up survey was high for participants who completed the baseline survey, the response rate for the baseline survey was fairly low. This may have biased the study population toward participants who were more eager to learn about the topic. Fewer than half of obstetricians viewed the website, in contrast to almost 80% of CNMs and 60% of family medicine practitioners. This may have been a result of increased knowledge at baseline or time constraints affecting the obstetricians disproportionately. Given the small numbers, we were not able to determine the impact of the CME versus that of the informational website. Because participants were not randomized to the web-based intervention, the differences between groups may reflect differences in baseline knowledge or interest. Our study did not look at patient outcomes to determine whether the intervention targeting providers increased actual counseling rates or the amount of antenatal physical activity. Finally, this study was conducted in a single sample with no control group; thus, the intervention should be replicated in controlled trials as well as in other settings.
Although, to our knowledge, we are the first to utilize a web-based education module and CME in the area of antenatal physical activity, online education is increasingly popular among providers as a way of attaining knowledge and earning CME credits. 32 However, few studies have assessed the impact of online education on knowledge, attitudes, and behaviors. 33 In a recent review of 15 studies, the majority of web-based CMEs demonstrated significant improvement in measured general outcomes of improving knowledge and changing clinical practice. 34 In a recent study, a web-based, case-based CME for providers successfully increased referrals for smoking cessation as well as improved attitudes and self-efficacy for delivering tobacco-related interventions. 35 Taken together, these findings suggest that online education is a desirable method for provider education. Our web-based intervention shows promise as an acceptable and effective method to improve knowledge, attitudes, and behavior among providers.
Implications for Practice
In this study, we demonstrate that a low-intensity web-based intervention significantly improved knowledge, attitudes, and reported practices for antenatal physical activity among providers. This is an important finding, given the evidence that brief counseling on behavioral change by health care providers increases the likelihood that women will adopt behaviors. Because of the public health impact of these prenatal health behaviors on numerous positive maternal and child outcomes and the lack of pregnant women currently meeting recommended guidelines, there is a definite need to develop a high-quality curriculum aimed at helping providers gain the knowledge and necessary skills to promote positive behavioral change among their pregnant patients. The present study was the necessary step in beginning to help providers feel more confident in promoting physical activity among their pregnant patients. Unfortunately, there is an inherent tension in providing comprehensive care in a time-limited health care environment. Offering web-based trainings are challenged with developing effective algorithms to promote provider-patient communication pertaining to prenatal health behaviors. However, it is necessary that health care providers become familiar with evidence-based approaches to behavioral change and are given efficient ways to use these approaches to improve provider-patient communication and, ultimately, promote positive behavioral change among their patients.
Footnotes
Authors’ Note
This work was supported by Grant AHRQ #1R03HS018595.