
Abstract
Prospective studies examining postpartum weight retention (PPWR) in relation to the appropriateness of gestational weight gain (GWG) and leisure-time physical activity (LTPA) during pregnancy and postpartum are lacking. While utilizing varying estimates of prepregnancy weight, we sought to prospectively examine associations among the aforementioned variables. Our sample consisted of a subset of women from the Archive for Research on Child Health Study (n = 68). Prepregnancy weight was obtained via questionnaire and birth certificates. GWG (2 estimates) was calculated by subtracting prepregnancy weight estimates from weight at delivery and classified as “excess” or “not excess.” Pregnancy and postpartum LTPA were self-reported and dichotomized at recommended levels. Prepregnancy weight estimates were subtracted from self-reported postpartum weight to calculate 2 estimates of PPWR at 6 months. Linear regression was used to examine relationships among GWG and LTPA, and PPWR. Estimates of excess GWG were associated with increased PPWR (mean difference = 3.3-8.9 kg), even after adjustment for prepregnancy body mass index and breastfeeding. Meeting pregnancy and postpartum LTPA recommendations did not significantly predict PPWR. Our findings highlight the importance of encouraging appropriate GWG and provide insight into the impact varying estimates of prepregnancy weight may have when exploring associations among these variables.
‘Specifically, researchers are investigating postpartum weight status because one of the most common, long-term health issues women face is an increase in body weight after pregnancy.’
Introduction
To date, most research on the appropriateness of maternal gestational weight gain (GWG) has focused on determinants and consequences during pregnancy or at delivery. However, with the rising prevalence of obesity among women of childbearing age 1 and the high incidence of women gaining excess weight during pregnancy, 2 many researchers have shifted their attention to the mother’s postpartum health status. Specifically, researchers are investigating postpartum weight status because one of the most common, long-term health issues women face is an increase in body weight after pregnancy. 3 Excess body weight is problematic because of its direct relationship with metabolic and cardiovascular disease development later in life. 4 Weight in the postpartum period in excess of prepregnancy body weight has been termed postpartum weight retention (PPWR). In fact, researchers have suggested that pregnancy is a potential risk factor for obesity development in women of childbearing age because of PPWR. 5 The postpartum period has been previously defined as up to 6 weeks postpartum. 6 However, it has been suggested that failure to return to prepregnancy weight by 6 months postpartum is associated with long-term obesity and adverse health outcomes.7-9 The amount of weight retained has been shown to be quite variable, with one review article reporting a range from 26.5 kg gained to 12 kg lost at 1 year postpartum, as compared with prepregnancy body weight. 10 Many studies report an average PPWR of only 0.5 to 3.0 kg; however, approximately 20% of women may retain at least 5 kg at 6 to 18 months postpartum. 11 The cause of PPWR is multifaceted; however, it has been proposed that one potential pathway is through excessive GWG. 12
In general, results from observational studies have shown a consistent positive relationship between GWG in excess of the Institutes of Medicine (IOM) recommendations and PPWR.2,4,7-10,13-17 Even though GWG explains a large part of the variance in PPWR, other lifestyle factors, such as leisure-time physical activity (LTPA), dietary habits, and breastfeeding, may play a role. Unfortunately, researchers studying PPWR have not typically considered the influence of LTPA. Results from observational studies that have examined the association between postpartum LTPA and PPWR have yielded consistent inverse relationships at varying postpartum time points (6 weeks to 10 years).7,10,17-20 However, prospective studies that examine PPWR in relation to both LTPA during pregnancy and postpartum are lacking. Furthermore, the combined effects of pregnancy LTPA, postpartum LTPA, and appropriateness of GWG on PPWR have not been examined. Gaining more insight into the interrelationships among the appropriateness of GWG, LTPA participation during pregnancy and the postpartum period, and PPWR could help inform future research, clinical practice, and interventions designed to promote appropriate maternal body weight changes. Therefore, the purpose of this study was to prospectively examine the effects of GWG, and pregnancy and postpartum LTPA on PPWR at 6 months postpartum, with varying estimates of prepregnancy weight.
Methods
Study Sample
Our study sample is a subset of women recruited in the ongoing Archive for Research on Child Health (ARCH) pregnancy cohort. This prospective pregnancy cohort, which began in 2008, interviews women at first prenatal visit in 3 clinics in Lansing, Michigan; archives urine and blood at 2 points in pregnancy; and obtains placenta samples. Mothers and infants are followed into childhood. The purpose of the cohort is to serve as a resource to examine research questions in maternal and child health that require information collected in real time in pregnancy. The institutional review boards of Michigan State University and Sparrow Hospital approved the protocols and procedures of the ARCH study.
ARCH study women are recruited, provide consent, and are enrolled at an average of 13 weeks of gestation. The participating clinics are a university faculty obstetric clinic, hospital residency clinic, and county health department clinic. Participants must be ≥18 years of age and able to answer a survey in English.
Inclusion criteria for our analyses were participation in ARCH, singleton term (>37 weeks) live birth, and availability of the following data: self-reported pregnancy and postpartum LTPA, linked birth certificate data to calculate GWG, and self-reported 6-month postpartum body weight. Basic demographic data on maternal age, ethnic/racial group, education level, and marital status were collected at enrollment.
Prepregnancy Anthropometrics
To obtain a measure of prepregnancy body size, women were asked, via questionnaire at enrollment, to report their prepregnancy height and weight. Prepregnancy body weight was also abstracted from each woman’s birth certificate after delivery. Birth certificate prepregnancy body weight is a relatively new vital record, and the method of determination (self-reported at delivery or abstracted from medical records) cannot be stated with certainty. For this study, the research team calculated prepregnancy body mass index (BMI) as weight in kilograms divided by height in meters squared, using both measures of prepregnancy body weight. These variables were termed enrollment prepregnancy BMI and birth certificate prepregnancy BMI. Women were categorized as underweight, normal weight, overweight, or obese, according to the classifications developed by the World Health Organization and adopted by the IOM for GWG recommendations21,22 (underweight: <18.5 kg/m2; normal: 18.5-24.99 kg/m2; overweight: 25-29.99 kg/m2; obese: ≥30 kg/m2).
Pregnancy LTPA
Women were asked to report LTPA participation during pregnancy at study enrollment via questionnaire. They were asked to report any physical activity, exercise, and sports that they took part in during their free time. Moderate activities were described as ones that cause a small increase in breathing or heart rate, whereas vigorous activities were described as those that cause a large increase in breathing or heart rate. Examples of both moderate and vigorous activities were provided to assist women in distinguishing intensity level. If women reported participating in either moderate or vigorous LTPA, they were asked to report days per week and typical time (hours and minutes) spent doing moderate and/or vigorous activities in 1 day. Minutes per day of moderate and vigorous LTPA were multiplied by the number of days per week to obtain minutes per week of moderate and vigorous LTPA. Pregnancy LTPA was categorized as either “not meeting recs” if a woman reported less than 150 minutes of moderate and vigorous LTPA per week during pregnancy or “meeting recs” if a woman reported participating in at least 150 minutes of moderate and/or vigorous LTPA during pregnancy, in accordance with the 2002 guidelines published by the American College of Obstetricians and Gynecologists (ACOG). 23
Gestational Weight Gain
GWG was calculated in 2 ways. Values for GWG were calculated by subtracting prepregnancy weight (self-reported at study enrollment or abstracted from birth certificates) from weight at delivery (abstracted from birth certificates), and were referred to as “enrollment GWG” and “birth certificate GWG.” For each participant, adequacy of GWG (via both calculation methods) was evaluated based on prepregnancy BMI-specific 2009 IOM recommendations. To maximize statistical power and focus on predicting excess GWG, values were categorized as “excess” or “not excess,” using the upper limit of the 2009 IOM recommended range in a given BMI category as a cut-point 22 (Table 1).
Categorization of Gestational Weight Gain.
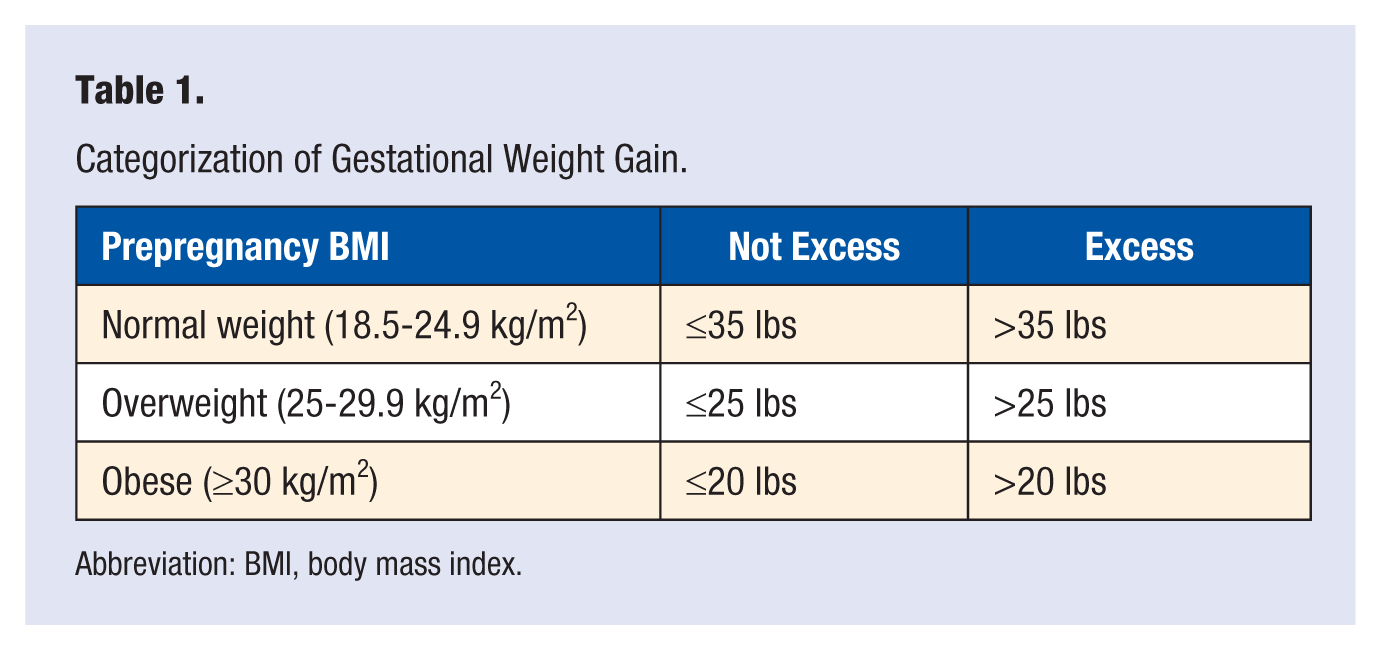
Abbreviation: BMI, body mass index.
Postpartum Weight Retention and LTPA
Participants enrolled in the ARCH study received follow-up phone calls at 6 months postpartum by a trained member of the ARCH staff. Women contacted at 6 months postpartum were asked to self-report weight and LTPA. Prepregnancy weight (self-reported at enrollment and abstracted from birth certificates) was subtracted from self-reported postpartum weight to calculate 2 different estimates of 6-month PPWR for each individual, termed enrollment PPWR and birth certificate PPWR. The LTPA questions from the enrollment questionnaire (described previously) were used to assess postpartum LTPA. Six-month postpartum LTPA was categorized as “not meeting recs” or “meeting recs,” depending on whether either moderate or vigorous physical activity guidelines were achieved (moderate: 150 minutes per week; vigorous: 75 minutes per week 24 ). Women were also asked if they had breastfed their infant. Information regarding this practice was available as a dichotomous variable (yes/no). Women were also asked about their fruit and vegetable intake. Servings of fruits and vegetables per day were combined and available as a continuous variable (servings per day).
Statistical Analyses
Descriptive statistics were calculated for all variables of interest. Women lost to follow-up were compared with women in our analytic sample to assess differences from the original cohort using a χ2 test, and effect sizes were calculated. PPWR (continuous variable) was normally distributed, so linear regression was used to test for main effects of GWG, and pregnancy and postpartum LTPA on the outcome measure of 6-month PPWR. Multicovariate linear regression was used to examine the effect of GWG, pregnancy LTPA, and postpartum LTPA on 6-month PPWR. GWG was expressed as a binary variable (“not excess” or “excess”) and LTPA was expressed categorically during pregnancy and at 6 months postpartum (“not meeting recs” or “meeting recs”). “Not-excess” GWG and “meeting recs” for pregnancy and postpartum LTPA were referent categories. 95% CIs for the regression coefficient were calculated. Covariates (race, parity, Women, Infants, & Children (WIC) enrollment, smoking, gestational age, birth certificate and enrollment prepregnancy BMI, fruit/vegetable consumption, and breastfeeding) were investigated for their potential roles as confounders. Criteria for covariate inclusion in the analytic models were as follows: (1) does not function as a mediator or collider, (2) biological rationale for potential confounding based on previous literature, and (3) a statistically significant association with PPWR or alters other main effect estimates by more than 10% in the current data set. An α level of P ≤ .05 was used to determine statistical significance.
Results
Because few women had a prepregnancy BMI that was classified as underweight (n = 7), they were excluded from our analyses. Self-reported pregnancy LTPA data that were ≥3 SDs above the mean (self-reported estimates not within reason) were also excluded (n = 5). In addition, 67 women were unable to be contacted in the postpartum period. Attempts to contact women occurred via telephone, email, and postal mail. Women were telephoned at various times of the day at all numbers traceable to their name, including those found in the white pages. Because postpartum weight and LTPA were not available for these women, they were not included in our analyses. A flowchart of included/excluded participants appears in Figure 1.
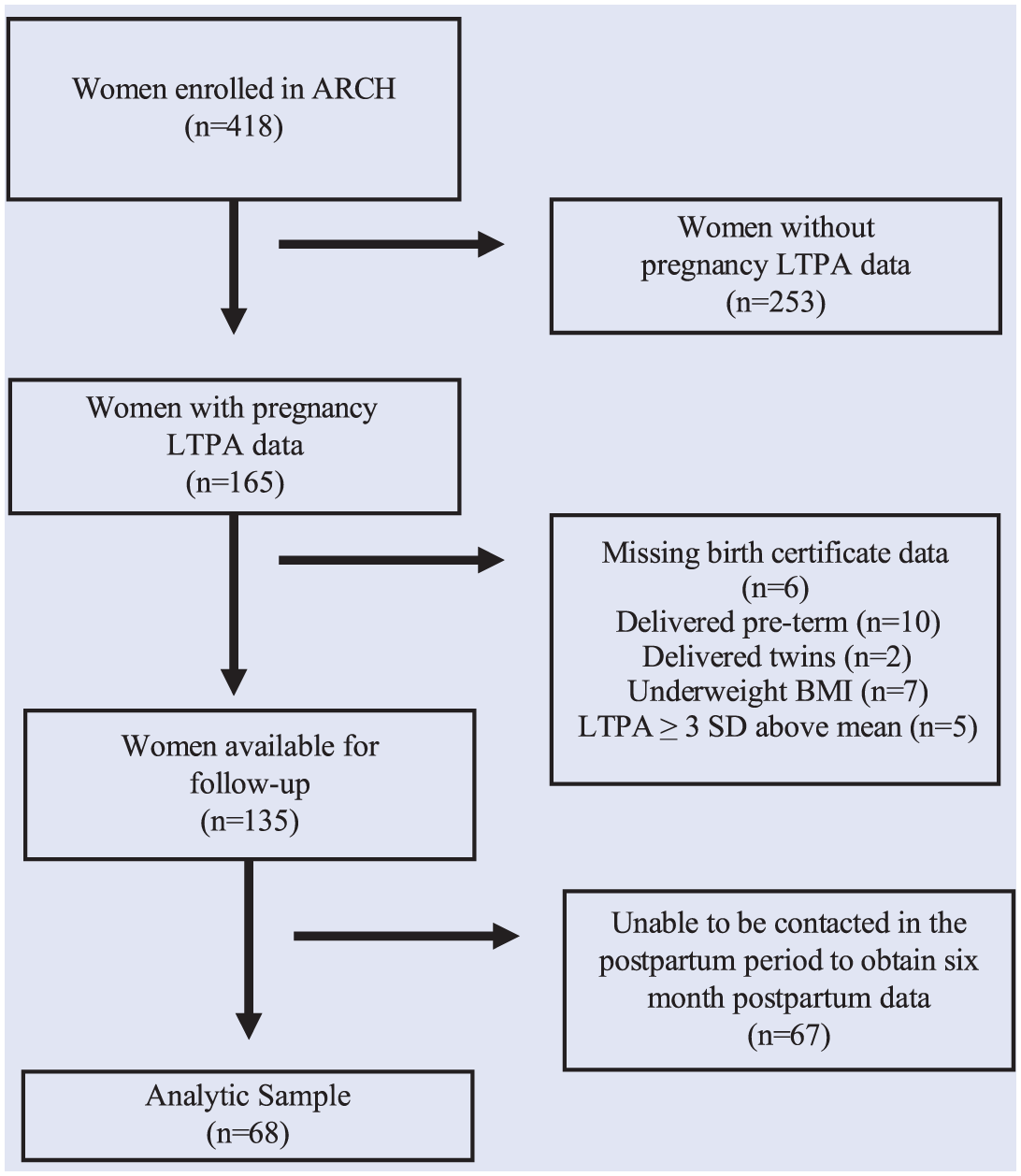
Flowchart of women included in the analytic sample (n = 68).
Among women meeting the eligibility criteria, some were unavailable for follow-up in the postpartum period. Relative to women in the follow-up sample (n = 68), those lost to follow-up were less educated, and fewer met pregnancy LTPA recommendations (Table 2). Although differences were not statistically significant in prepregnancy BMI and GWG, more women in our follow-up sample were normal weight and fewer had excess GWG, compared with our non–follow-up sample (Table 2).
Comparison of Maternal Characteristics for the ARCH Participants Included in the Follow-up and Non–follow-up Samples.
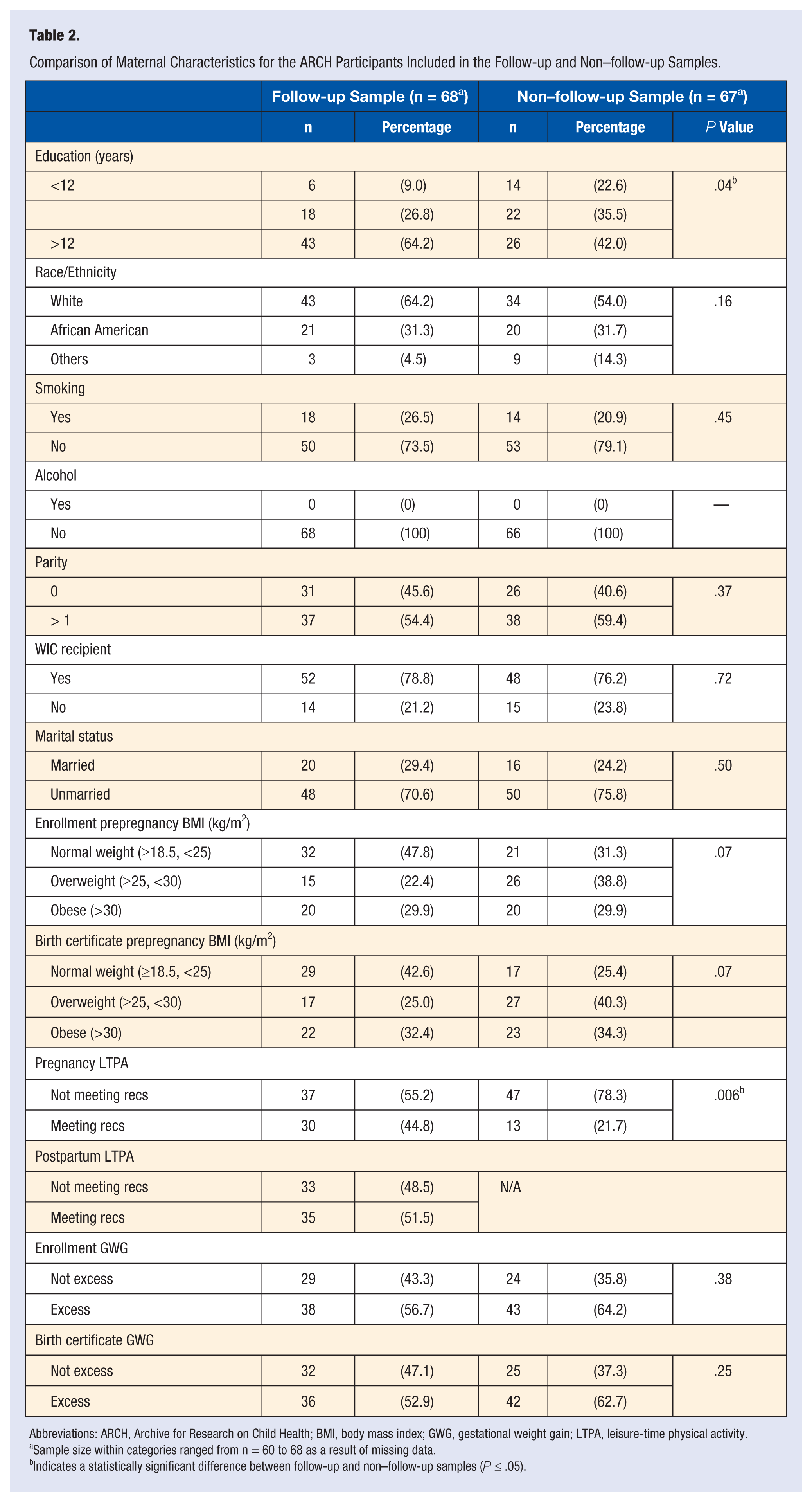
Abbreviations: ARCH, Archive for Research on Child Health; BMI, body mass index; GWG, gestational weight gain; LTPA, leisure-time physical activity.
Sample size within categories ranged from n = 60 to 68 as a result of missing data.
Indicates a statistically significant difference between follow-up and non–follow-up samples (P ≤ .05).
At study enrollment, mean (±SD) maternal age was 25.5 ± 5.3 years. Prepregnancy BMI according to birth certificate and self-report at enrollment were 27.8 ± 6.6 kg/m2 and 27.5 ± 7.0 kg/m2, respectively. The percentage of normal-weight, overweight, and obese women in our sample (via prepregnancy BMI) and women who experienced excess GWG varied according to the estimate of prepregnancy weight used (Table 2). Furthermore, average 6-month PPWR differed slightly according to which estimate of prepregnancy weight was utilized in the calculation. As such, PPWR was 2.7 ± 9.7 (range = −20 to +43) kg when using prepregnancy weight abstracted from the birth certificate and 3.6 ± 8.7 (range = −22 to +27) kg according to enrollment prepregnancy weight. PPWR estimation methods did not differ by prepregnancy BMI category (P = .29) or LTPA participation (P = .43). Results of linear regression showed that birth certificate excess GWG was associated with PPWR (R2 = 0.12-0.21; Table 3).
Associations Among GWG Category, Pregnancy LTPA, Postpartum LTPA, and 6-Month PPWR (n = 68).
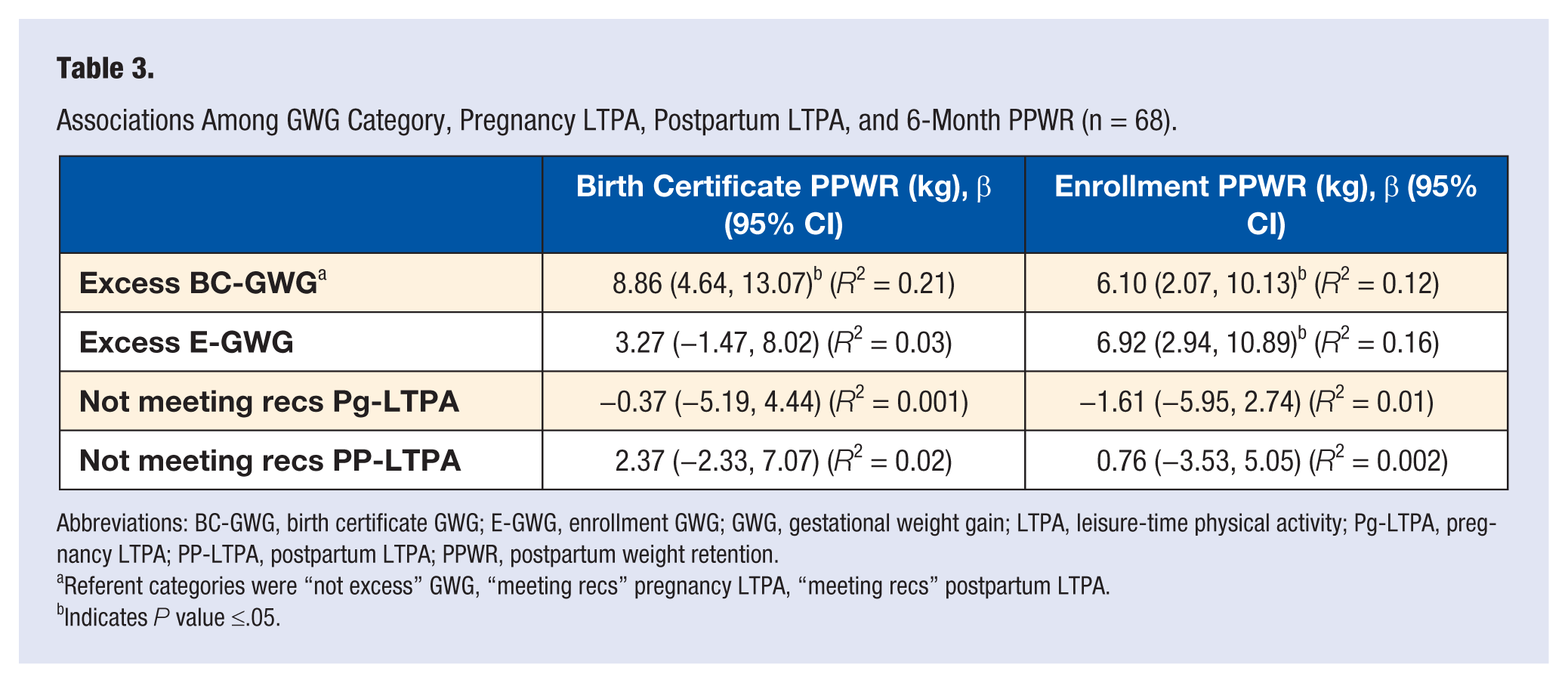
Abbreviations: BC-GWG, birth certificate GWG; E-GWG, enrollment GWG; GWG, gestational weight gain; LTPA, leisure-time physical activity; Pg-LTPA, pregnancy LTPA; PP-LTPA, postpartum LTPA; PPWR, postpartum weight retention.
Referent categories were “not excess” GWG, “meeting recs” pregnancy LTPA, “meeting recs” postpartum LTPA.
Indicates P value ≤.05.
Based on maternal reports, the average amounts of moderate and vigorous LTPA performed during pregnancy and at 6 months postpartum were 293 ± 378 (range = 0-1500) and 410 ± 593 (range = 0-2400) minutes per week, respectively. Total minutes of pregnancy and postpartum LTPA were not significantly correlated (r = 0.19). Pregnancy LTPA was not significantly associated with weight retained at 6 months postpartum. Additionally, meeting LTPA recommendations at 6 months postpartum was not significantly related to PPWR (Table 3).
Finally, we examined the effect of GWG category, pregnancy LTPA, and postpartum LTPA on the outcome of 6-month PPWR. Excess GWG was the only significant covariate in this model (β estimates ranged from 6.48 to 8.91, depending on estimate of GWG and PPWR utilized). In this model, 6-month PPWR was not significantly related to pregnancy or 6-month postpartum LTPA. The variance that was explained by the effect of these covariates differed according to estimates of GWG and PPWR but ranged from 6% to 22%.
Among the covariates considered for confounding (race, parity, WIC enrollment, smoking, gestational age, birth certificate and enrollment prepregnancy BMI, fruits/vegetable consumption, and breastfeeding), only enrollment prepregnancy BMI category was significantly related to enrollment PPWR (P = .04; overweight and obese women retained less weight than normal-weight women). Enrollment prepregnancy BMI remained significant when modeled with GWG (enrollment and birth certificate), pregnancy LTPA, and postpartum LTPA with the outcome of enrollment PPWR. Although breastfeeding was not significantly related to either estimate of PPWR (P = .76 to .94), it altered some main-effect estimates by more than 10% when predicting enrollment PPWR. Adjusted models can be found in Table 4.
Adjusted Multiple Linear Regression Analyses Examining the Relationships Among GWG Category, Pregnancy LTPA, and Postpartum LTPA on the Outcome of 6-Month PPWR (n = 68).
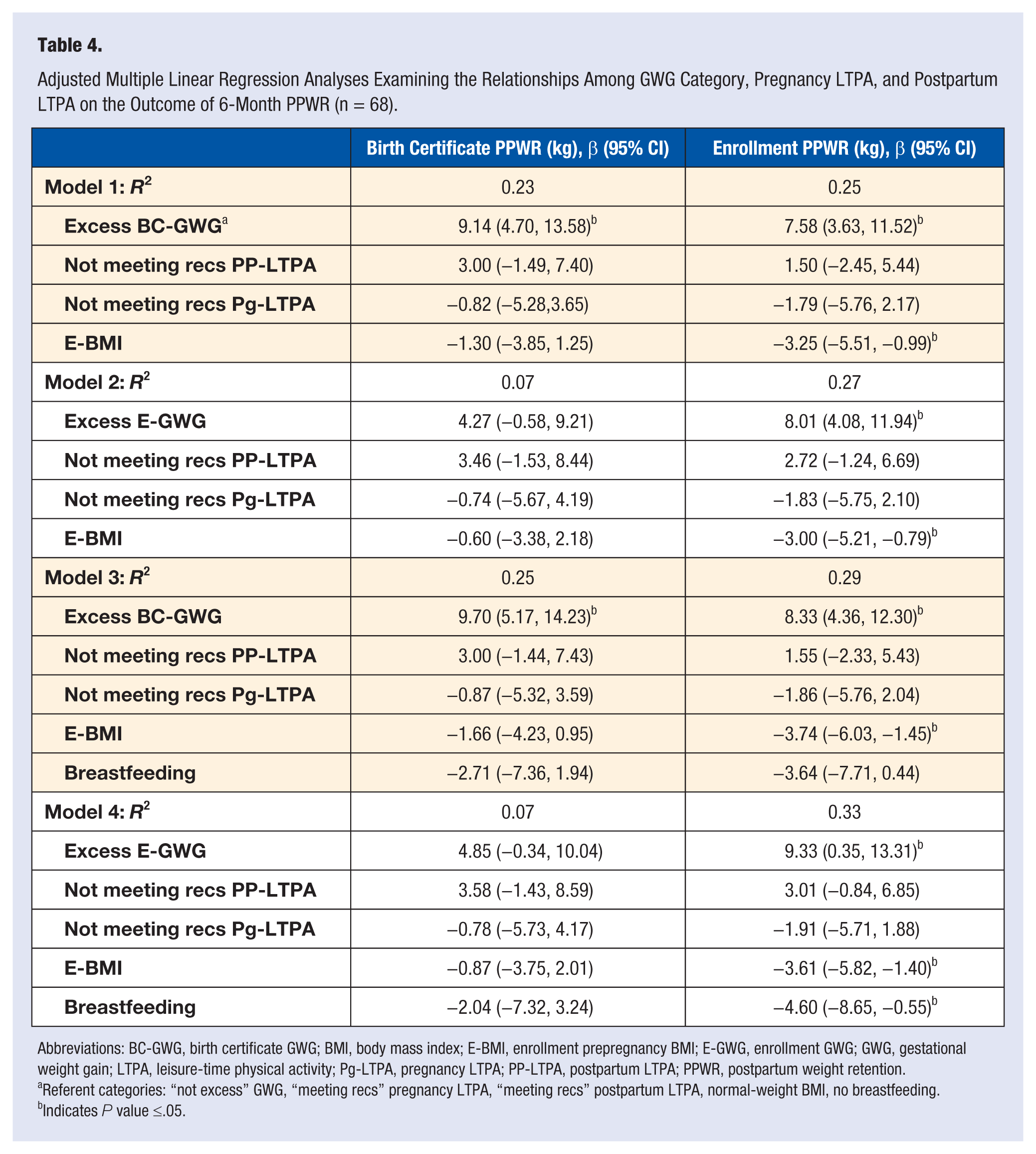
Abbreviations: BC-GWG, birth certificate GWG; BMI, body mass index; E-BMI, enrollment prepregnancy BMI; E-GWG, enrollment GWG; GWG, gestational weight gain; LTPA, leisure-time physical activity; Pg-LTPA, pregnancy LTPA; PP-LTPA, postpartum LTPA; PPWR, postpartum weight retention.
Referent categories: “not excess” GWG, “meeting recs” pregnancy LTPA, “meeting recs” postpartum LTPA, normal-weight BMI, no breastfeeding.
Indicates P value ≤.05.
Discussion
Our purposes were to examine if (1) the appropriateness of GWG, (2) pregnancy LTPA, and (3) postpartum LTPA were associated with 6-month PPWR using prepregnancy weight estimates determined via self-report at enrollment and abstracted from the birth certificate. Our findings indicated that GWG in excess of IOM recommendations was significantly associated with an increase in PPWR. LTPA participation during pregnancy and at 6 months postpartum was not associated with PPWR. When we modeled GWG, pregnancy LTPA, and postpartum LTPA together, excess GWG remained significant, even after adjusting for prepregnancy BMI category and breastfeeding. For all analyses, the magnitude of associations depended on the estimate of prepregnancy weight that was used to estimate GWG and PPWR.
Because prepregnancy weight was available from 2 sources, we calculated 2 different values for prepregnancy BMI, GWG, and PPWR. Consequently, our prevalence estimates of excess GWG, BMI categorizations, and mean PPWR varied slightly according to the source of prepregnancy weight estimate (self-reported at enrollment or abstracted from the birth certificate). To date, evidence is not available to comment on the validity of prepregnancy weight on the birth certificate in the state of Michigan. The origin of birth certificate prepregnancy weight is somewhat ambiguous because practices within and across hospitals are not consistent. Ideally, prepregnancy weight is abstracted from medical records, but often, maternal self-report before or after delivery is utilized.
On average, values for enrollment prepregnancy weight were lower than values abstracted from birth certificates. This resulted in average enrollment PPWR being slightly higher than average birth certificate PPWR, but the difference between PPWR measures did not differ significantly as a function of prepregnancy BMI category or LTPA participation. Furthermore, main effect estimates from our linear regression analyses varied among GWG, prepregnancy BMI, and PPWR estimations. These findings indicate that the methodology utilized to obtain prepregnancy weight is an important factor to consider when attempting to explain variance in PPWR within and across research studies. To our knowledge, ours is the first study to utilize 2 different estimates of prepregnancy weight to calculate GWG, prepregnancy BMI, and PPWR. Before birth certificate abstracted prepregnancy weight may be used with confidence in future studies, research is needed to validate birth certificate prepregnancy weight, particularly in hospitals with varying birth certificate recording processes. Therefore, for our analyses, we chose to calculate our outcome measure of PPWR with both self-reported enrollment (prior to 14 weeks gestation) and birth certificate prepregnancy weight to explore the effect on our estimates.
Regardless of which prepregnancy weight estimate was used, we found a consistent, positive association between GWG in excess of IOM recommendations and PPWR at 6 months. Moreover, excess GWG explained more variance in PPWR than any other covariate in the models. This finding has been observed consistently in several observational studies.2,4,7-10,13,15 -17 For example, Linne et al8,10,15 demonstrated this relationship in a series of articles utilizing data from the Stockholm Pregnancy and Women’s Nutrition (SPAWN) study. Women from SPAWN were studied originally during pregnancy and followed up at 6 months, 1 year, and 15 years postpartum. Regardless of prepregnancy BMI, women who experienced excess GWG retained more weight at each postpartum follow-up time point, even after controlling for the number of pregnancies after the index child. In addition, a recent meta-analysis supported our findings and those from other observational studies. The investigators showed that women with GWG in excess of IOM recommendations retained significantly more weight at a range of postpartum time points (6 months through 15 years postpartum). 25 The positive association between excess GWG and PPWR is so strong and consistent that it has been suggested that excess GWG is one of the strongest predictors of PPWR. 3
When we investigated whether self-reported LTPA participation during pregnancy or at 6 months postpartum was associated with PPWR, we found that LTPA participation at both time points was not significantly associated with 6-month PPWR. However, an association between postpartum LTPA and PPWR has been found previously, and results have demonstrated an inverse relationship at time points ranging from 6 months to 10 years postpartum.7,10,18-20,26 Although postpartum LTPA was not significantly associated with PPWR, our linear regression estimates were in the expected direction. Specifically, women who met recommendations retained less weight than women who did not (birth certificate PPWR: 1.5 vs 4.0 kg; enrollment PPWR: 3.2 vs 3.9). However, our model explained a very small portion of the variance in PPWR (R2 = 0.002-0.015). Therefore, our linear regression did not model the data well, and the average PPWR value among women meeting guidelines was not significantly lower than those who did not meet guidelines at 6 months postpartum. Post hoc testing revealed that our power to detect differences in PPWR between postpartum LTPA categories was 0.064. Consequently, our small sample size likely limited our ability to detect a significant difference between LTPA categories.
Compared with postpartum LTPA, the role of pregnancy LTPA in reducing PPWR is less studied. In fact, we are among the first to prospectively investigate self-reported minutes per week of moderate and vigorous LTPA during pregnancy in relation to PPWR. Pereira et al 20 examined change in LTPA from prepregnancy through 6 months postpartum using a prospective cohort design. They assessed LTPA at each trimester and found that a decline in LTPA levels during pregnancy was associated with increased body weight retention during the first 6 months of the postpartum period. In our sample, LTPA was assessed at 1 time point, which was early in pregnancy (<14 weeks gestation). Therefore, it is likely that some women decreased LTPA or stopped exercising altogether later in pregnancy, and our measure lacked sensitivity to investigate the association between changes in pregnancy LTPA across trimesters and PPWR. Change in activity volume is important to consider because continuation of LTPA throughout pregnancy may be associated with the likelihood of women engaging in LTPA during the postpartum period. However, as noted within our results, total minutes of pregnancy and postpartum LTPA were not significantly correlated (r = 0.19). Although purely speculative, if we had obtained a measure of pregnancy LTPA representative of all trimesters, our correlation coefficients may have been different. In addition, investigating the association between LTPA across pregnancy and the appropriateness of GWG is also imperative because GWG might mediate the relationship between pregnancy LTPA and PPWR. Although we did not find significant associations between pregnancy LTPA or postpartum LTPA and PPWR, the importance of LTPA in eliciting body weight change should not be ignored by researchers or health care providers.
Although there are general guidelines for participation in LTPA during pregnancy from the ACOG, 23 specificity regarding the approach and timing to safely resume LTPA in the postpartum period are lacking. This lack of clarity regarding resumption of physical activity in the postpartum period may lead to inconsistent or erroneous recommendations from health care providers to new mothers. Research indicates that, in general, US women feel that resumption of LTPA is safe at 3 months postpartum, even if they continue to breastfeed. 27 However, many women have difficulty initiating LTPA in the postpartum period.10,20 Therefore, it is important that health care providers strive to effectively communicate the benefits of LTPA at a time in the postpartum period when it is safe to do so and are receptive to their patients’ concerns.
Our findings have important clinical and public health implications. First, it is important that health care providers effectively communicate GWG guidelines to their patients and encourage a healthy weight gain over the course of pregnancy. Encouraging appropriate GWG in all BMI categories (not only among obese women) is essential. This is supported by our findings of PPWR being significantly and inversely related to BMI category. Studies show that regardless of prepregnancy BMI, women who do not return to their prepregnancy weight within the first year after delivery tend to retain significantly more weight over time (up to 15 years postpartum).4,7,28 Furthermore, increases in body weight, resulting from PPWR, have been observed after each subsequent pregnancy in multiparous women.3,12 Because many women gain excess weight while pregnant and retain much of it after each delivery, pregnancy has been proposed as a potential risk factor for obesity. 12 However, recent work by Robinson et al 29 suggests that childbearing among contemporary women may not be a risk factor for obesity among all women. The authors theorize that, within at-risk subpopulations, GWG may simply be a marker for excess PPWR and obesity later in life. Although further research is needed to more confidently identify at-risk subgroups, available data indicate that it is important for health care providers to not only encourage appropriate GWG but also be open to discuss postpartum behaviors that may help their patients return to prepregnancy weight. Behaviors that may assist in achieving a negative energy balance, such as LTPA and breastfeeding, should be encouraged to women of all body sizes, and particularly those who gained too much weight during pregnancy and experience PPWR. Additionally, because guidelines for resumption or initiation of LTPA in the postpartum period are somewhat ambiguous, health care providers must take time to implement individualized patient approaches because LTPA recommendations in the early postpartum period will likely vary among new mothers.
There are several study limitations worth noting. Our inability to obtain postpartum follow-up data on our entire cohort is the most significant limitation. Women lost to follow-up differed from those in our analytic sample with regard to several characteristics. For example, women not included in our analyses were less active during pregnancy and, therefore, may have also been less active at 6 months postpartum. Consequently, our findings were likely affected, and the influence of LTPA may have been obscured. Other limitations include the self-reported and recalled nature of body weight and LTPA, assessment of LTPA via questions not previous validated, small sample size, and inability to follow our entire cohort farther into the postpartum period. Additionally, we were not able to include serial measures of postpartum body weight in this study. This is an important variable for future researchers to consider, particularly because some studies have shown PPWR to continue to decrease up until 1 year postpartum.13,25 Although we collected data on postpartum diet quality (fruit/vegetable consumption) and breastfeeding, future research should expand these measures when possible to obtain estimates of caloric intake and duration/exclusivity of breastfeeding. Additionally, prospective studies with larger sample sizes are needed that carefully quantify energy intake versus expenditure and include serial measurements of body weight (prepregnancy through postpartum).
In spite of these limitations, study strengths include a prospective design, consideration of covariates for confounding, and a racially and economically diverse sample. In addition, ours is one of only a few studies to consider the combined effect of GWG, pregnancy LTPA, and postpartum LTPA and, to our knowledge, the first to utilize 2 estimates of PPWR as our outcome measure. However, validation studies are needed to assess the validity of prepregnancy weight abstracted from the birth certificate. Exploring the interrelationships among GWG, pregnancy LTPA, postpartum LTPA, and PPWR has important implications for public health and clinical practice. To affect population health and better inform interventions and practice, research with improved methodology is needed to test and refine our findings.
Footnotes
Acknowledgements
The Archive for Research on Child Health is a project of the Department of Epidemiology and Biostatistics, Michigan State University (PI: Nigel Paneth MD, MPH) and has been supported by the following units of MSU: The Office of the Vice President for Research and Graduate Studies, the College of Human Medicine, the Departments of Psychology and Kinesiology, and the Institute for Health Care Studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.