
Abstract
Muscle-strengthening exercises (MSE) improve muscular strength, balance, endurance, mental health, and decrease the risk of noncommunicable diseases. Studies show that immigrant Black women do not adhere to MSE guidelines. The purpose of the study is to determine the associations between demographic, socioeconomic, and community-level characteristics in African-born Black immigrant women meeting guidelines and to describe their perceptions and attitudes towards MSE. Data were collected using an online cross-sectional survey from 220 African-born Black immigrant women. Covariates included sociodemographic characteristics, health behaviors, and anthropometrics. Descriptive statistics, Chi-square tests and multiple logistic regression analyses were performed. NVivo was used to analyze the qualitative data. About 47.3% met the MSE guidelines. Age, perception of weight, PA with a member of household, PA with someone outside of household, and the built environment were associated with MSE engagement. Former and current drinkers, those living with a chronic disease and those who used their built environment less were more likely to meet guidelines. Notions of health and fitness, ideal body image perceptions, knowledge gaps, time constraints, and perceived difficulty of MSE were cited as reasons for not meeting guidelines. African-born Black immigrant women care about health and interventions can capitalize on this to promote increased participation.
“Younger women have been found to engage in high impact and vigorous activity at higher rates than older women.”
Background
The Physical Activity Guidelines for Americans recommend that adults perform muscle-strengthening exercises that involve all major muscle groups at least two days per week, in addition to at least 150 minutes of moderate-intensity aerobic activity or 75 minutes of vigorous-intensity activity per week (MVPA). 1 Muscle-strengthening exercises (MSE), also called resistance exercise/training, strength training/exercise or muscle-strengthening activities, 2 have been shown to improve muscular strength, balance, endurance, mental health, overall quality of life, and reduce the risk of cardiovascular diseases, diabetes, and cancer.3-5 Evidence demonstrates that these benefits are independent of other types of physical activity (PA). 6 Although MSE benefits physical health and adherence has increased by approximately 10 percentage points among U.S. adults, 7 prevalence of MSE is generally lower, even among those who meet other PA guidelines.5,8
Previous studies have shown race, gender, age, education, body mass index (BMI) to be significant factors in MSE adherence.3,7,9 Men, non-Black individuals, those with a higher education attainment, and younger participants are more likely to meet MSE guidelines. 3 Population data on MSE rates consistently reveal that men are more likely to meet MSE guidelines compared to women, with 34.4% of men and 24.5% of women in the US meeting the guidelines. 9 Immigrants10,11 and Black/African American women12,13 engage in PA at lower rates than their White counterparts and women identifying as Black generally do not adhere to MSE guidelines. 3 Research consistently demonstrates that immigrant populations have lower levels of PA compared to their native-born counterparts, and some studies hypothesize that the low levels might be attributed to their lack of knowledge about the benefits.10,12 Immigrant communities exhibit a higher susceptibility to cardiovascular diseases compared to native-born groups, underscoring the value of MSE for maintaining health. 10 After adjusting for income, education, marital status, age, and sex, African immigrants were less likely to meet MVPA guidelines compared to their African American counterparts. 14
In addition, meeting MVPA guidelines has been shown to increase the likelihood of meeting MSE guidelines, 7 and only 13% of Black/African American women met the full PA guidelines compared to 18% of Latina women and 28% of Latino/African American men. 15 Race, income and gender have been shown to interact in PA adherence, and poor Black women were less likely to meet PA guidelines. 12 For African American/Black women, additional barriers to meeting MSE guidelines may include limited time due to expected gender roles, hair care and maintenance, concerns about appearing masculine, discouragement from family members, insufficient familiarity with MSE, and the perception that these activities are male-oriented.16-18 For Black immigrant women, income has been shown to have a weaker association with PA engagement compared to other groups.19,20 However, little is known about how these demographic, socioeconomic, and community-level factors jointly influence MSE adherence among African-born Black immigrant women, a gap that this study aims to address.
As census data and population research in the US use the Office of Management and Budget’s (OMB) racial and ethnic categories, and the Black/African American category includes African Americans, African immigrants, Afro Caribbeans and other Black populations in the US, Black is the umbrella term used in most studies. Therefore, there is scarce research on the MSE of African-born Black immigrant women. The goal of this paper is to determine the associations between demographic, socioeconomic, and community-level characteristics in meeting muscle-strengthening guidelines and to describe the perceptions and attitudes toward MSE of African-born Black immigrant women over the age of 18. Understanding these factors may assist in creating culturally specific interventions to increase MSE participation among this population.
Methods
Data were collected using a confidential, online cross-sectional survey. Participants were recruited via Qualtrics, a third-party provider, that targets specific respondent groups within its study panels. Respondents were eligible if they were born in a country on the African continent, over 18 years of age, identified as Black women, and could read and write English. There were no additional exclusion criteria. Data for this paper were part of a larger study on PA engagement among African-born Black immigrant women in the US. Informed consent was obtained from all participants. This study was approved by the authors’ Institutional Review Board (#23-E-131 and IRB-FY25-625).
Measures
Muscle-Strengthening Exercise
Participants completed the long version of Muscle-Strengthening Exercise Questionnaire (MSEQ) developed by Shakespeare-Drury and colleagues.
21
Participants were initially asked, “Do you usually do muscle-strengthening exercise?” and if they answered yes, other MSE questions followed assessing
Moderate and Vigorous Intensity Physical Activity
Participants were asked, “In the past two weeks, how many days per week have you engaged in any physical activities?”, “How often (how many times a week) do you do
Covariates
Participants provided their age, marital status, education, income, English proficiency, years in the US, date of arrival in the US, caregiving for under 18, caregiving for household, alcohol consumption, smoking, self-perception of body weight, desire to alter weight, and whether they engage in PA with a member of the household and/or with individuals outside of the household. Self-reported height and weight were used to calculate BMI. Perception of the neighborhood-built environment was assessed by asking participants, on a five-point Likert scale (ranging from “strongly disagree” to “strongly agree”), how much they agreed with six statements regarding the accessibility, usage, and safety of nearby parks, playgrounds, sidewalks, trails or paths. The responses were summed, and the median was used to create a dichotomous variable representing “low use” versus “high use.”
Statistical Analysis
Descriptive statistics included frequencies and proportions for categorical variables, and means and standard deviations for continuous variables. Chi-square tests were used to examine the associations between key participant characteristics and MSE. Multiple logistic regression analyses were performed to identify factors independently associated with MSE. With the exception of the MVPA variable, a confounding factor, all variables (age, marital status, education, English proficiency, years in the US, income, alcohol consumption, smoking, vaping, perception of health and weight, living with a chronic disease, BMI status, PA with a member of the household and with someone outside of the household, and built environment) were retained in all the regression models regardless of statistical significance in the bivariate analysis. The corresponding odds ratios (ORs), 95% confidence intervals (CIs), and p-values were reported. Model goodness of fit was evaluated using the Hosmer-Lemeshow test. Multicollinearity among independent variables was examined using the variance inflation factor (VIF), with values >4 considered indicative of collinearity. No collinearity was detected among the variables. P-values <0.05 were considered statistically significant. All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC).
Open-ended questions were initially coded manually to create a codebook, after which themes were imported into NVivo 1.7.1 for further analysis. The first author and two other researchers reviewed initial themes and reached consensus through discussion for data triangulation and to reduce bias. NVivo was then used to facilitate subsequent steps in the qualitative data analysis, including axial and selective coding.
Results
Characteristics of the Study Sample by Strength Guidelines (N = 220).
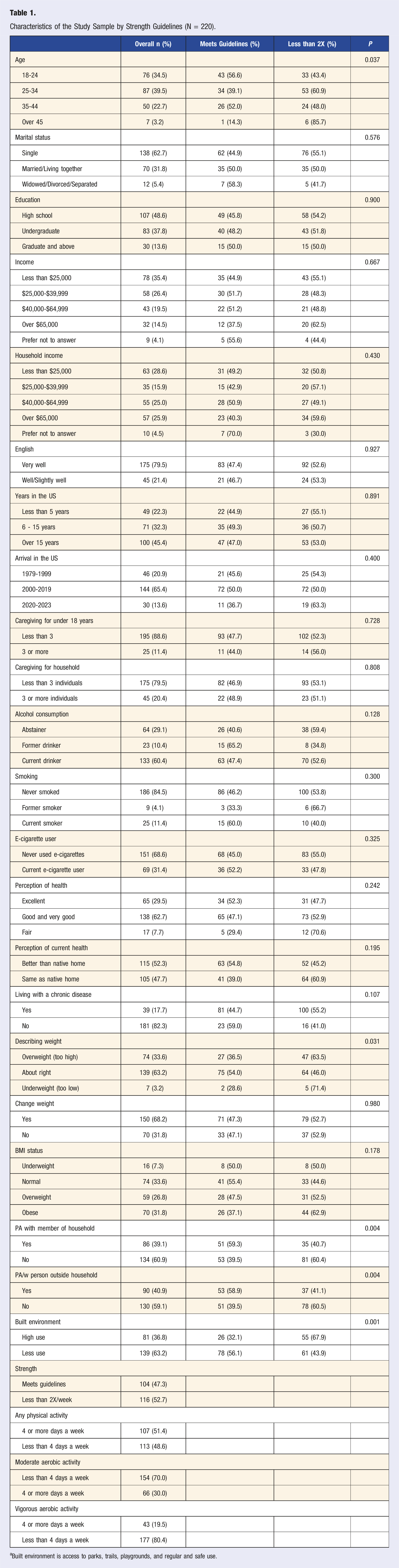
aBuilt environment is access to parks, trails, playgrounds, and regular and safe use.
Factors Associated With Strengthening Exercises (N = 220).
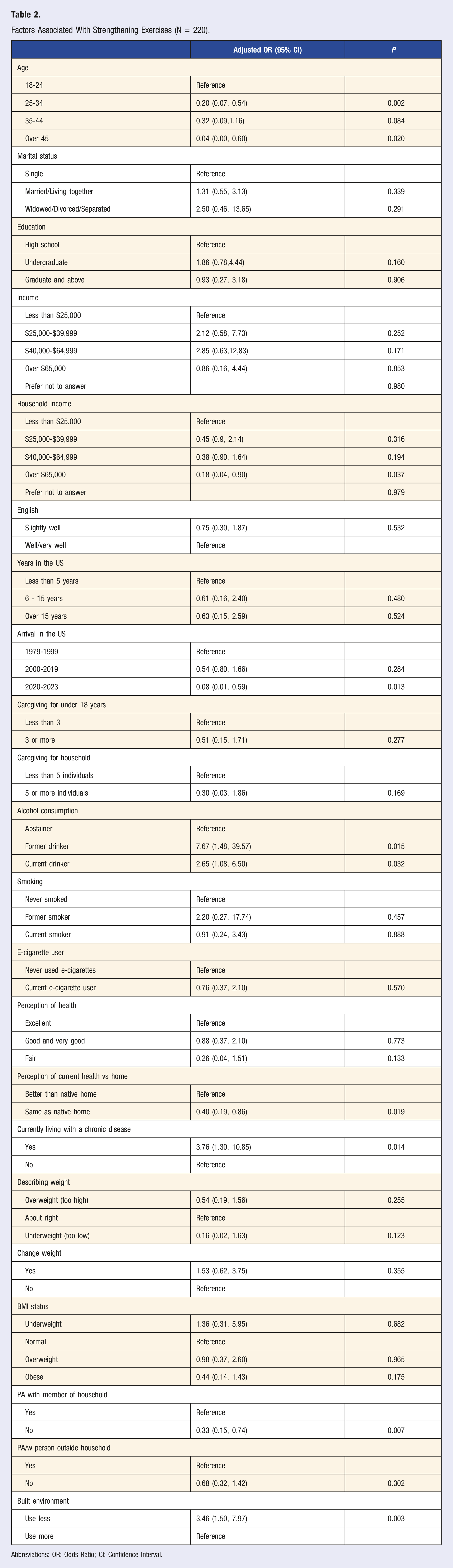
Abbreviations: OR: Odds Ratio; CI: Confidence Interval.
Participants who perceived their health as the same as it was in their native country (OR 0.40, 95% CI 0.19-0.86; P = 0.019) were less likely to meet strengthening guidelines compared to those who perceived their health as better than in their native country. Participants currently living with a chronic disease (OR 3.76, 95% CI 1.30–10.85; P = 0.014) were three times more likely to engage and meet the recommended guidelines compared to those who are not living with a chronic disease. Those who did not engage in PA with a household member (OR 0.33, 95% CI 0.15-0.74; P = 0.007) were less likely to meet strengthening guidelines compared to those who did. Participants who used their built environment less (OR 3.46, 95% CI 1.50-7.97; P = 0.003) were three times more likely to meet strengthening guidelines compared to those who utilized the built environment more frequently.
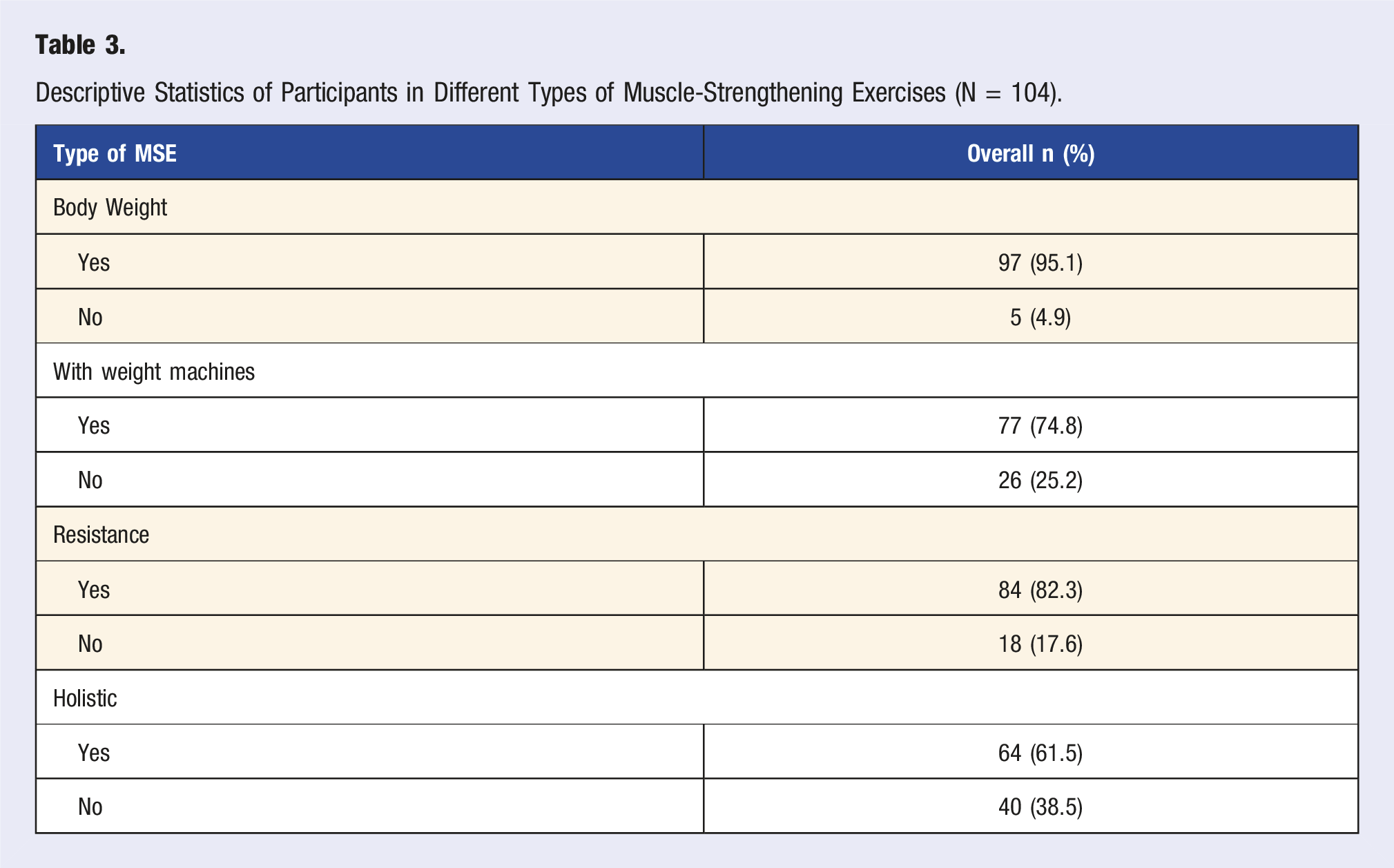
Descriptive Statistics of Participants in Different Types of Muscle-Strengthening Exercises (N = 104).
Perceptions of MSE engagement of African-born Black immigrant women in the US (N = 220).
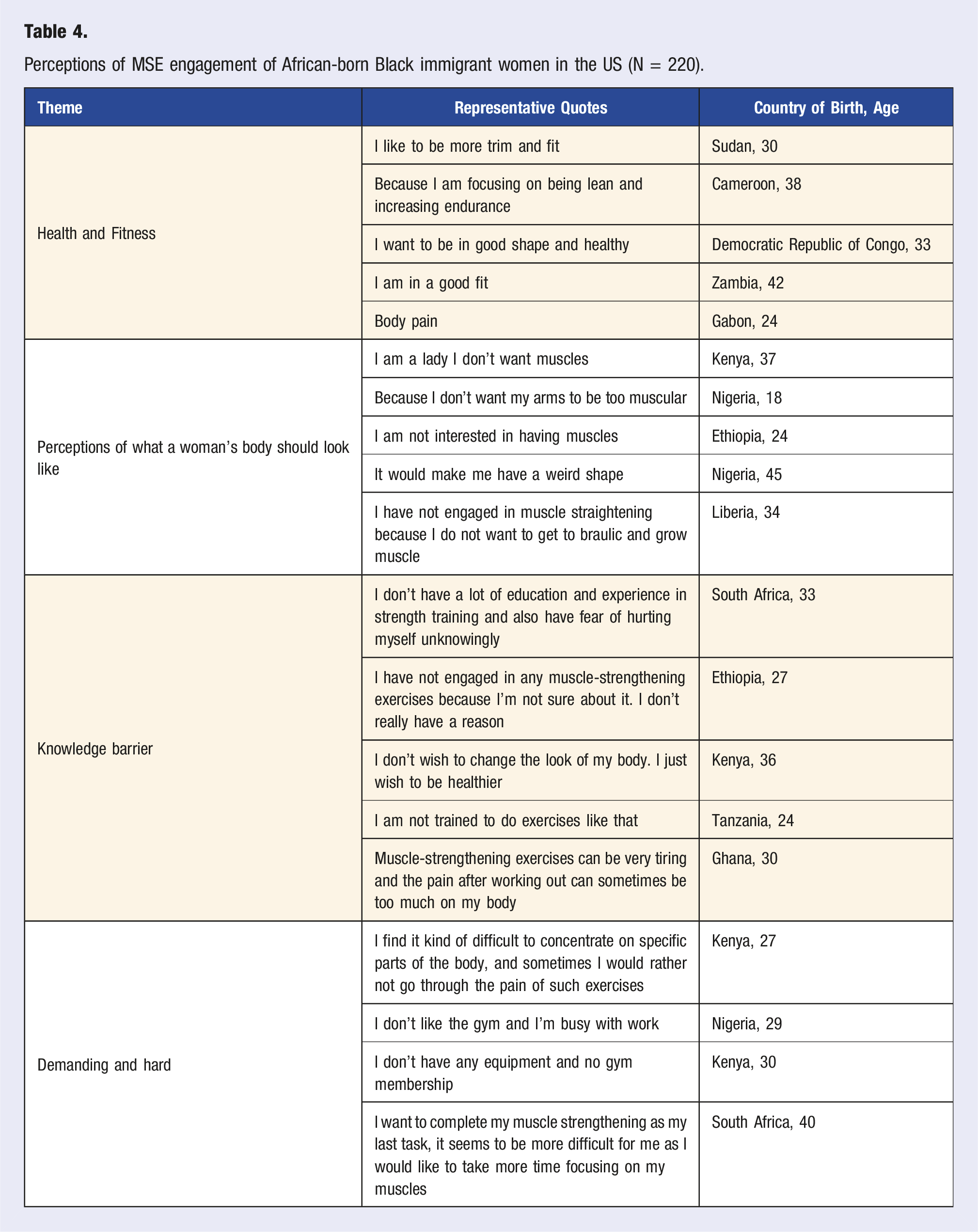
Health and Fitness
A qualitative analysis of the data showed that most immigrant women were concerned about their health even though they did not engage in any MSE. Statements such as “Because I am focusing on being lean and increasing endurances[sic]” indicate that they are doing other activities. In general, while about 76% of the participants in the study considered themselves active, only about 50% engaged in MVPA 4 or more times per week. More participants appear to be meeting the PA guidelines through MVPA than MSE. Even though some did not engage in MSE, they understood the value of health and fitness, as participants stated their aspiration for better health by saying, “I want to be in good shape and healthy” (Democratic Republic of Congo, 33) or perceived themselves to be healthy by stating “I am in good fit[ness]” (Zambia, 42).
Perceptions of Ideal Body Image for Women
Many respondents stated that they did not engage in MSE because of concerns about ideal body shape. Several expressed belief that these exercises might modify their shape, “would make me have a weird shape” (Nigeria, 45) or that they would lose their feminine look as expressed by the participant who said, “I am a lady I don’t want muscles” (Kenya, 37) and another who stated, “I have not engage[d] in muscle straightening because I do not want to get too braulic [to be muscular or very buff ] and growing muscle” (Liberia, 34).
Knowledge Barrier
Several participants stated that they were not knowledgeable enough about MSE or had not had enough experience to engage, as one participant stated, “I am not trained to do exercises like that” (Tanzania, 24). This also brought along the fear of injuring themselves. One participant stated, “I don’t have a lot of education and experience in strength training and also have a fear of hurting myself unknowingly” (South Africa, 33). Others’ lack of knowledge about MSE was a deterrent as indicated by the participant who stated, “I have not engaged in any muscle strengthening exercises because I’m not sure about it. I don’t really have a reason” (Ethiopia, 27).
Lack of Time and Difficulty
Associated with the knowledge barrier was the belief that perceived difficulty of MSE and time associated with carrying out the activities. Overall, 70% of participants reported engaging in moderate activity less than 4 days per week, and 80% reported engaging in vigorous activity 3 or fewer days per week. One participant noted, “I don’t like the gym and I’m busy with work” (Nigeria, 29) and another reasoned, “I want to complete my muscle strengthening as my last task, it seems to be more difficult for me as I would like to take more time enduring on my muscles” (South Africa, 40).
Discussion
In this study, 47.3% of the African-born Black immigrant women met the MSE guidelines, which is substantially higher than the national average for adults 18 years and over. In 2020, only 31.0% of U.S. adults met the MSE guidelines. 22 While historical trends show an overall increase in MSE in the entire population, men consistently report higher prevalence rates than women.7,23 From 1988 to 2018, the prevalence of men meeting MSE increased from 21.2% to 29.9%, while for women, the prevalence increased from 14.4% to 24.3%. 7 African immigrants have been shown to have better health profiles than their native-born counterparts,19,24,25 and African women specifically have a more holistic understanding of health, 26 as supported by our participants’ desire to be both healthy and in shape (e.g., “I am underweight and would like to be healthy, also I want to build muscle (Nigeria, 20)” and “To tone and just be healthy overall (South Africa, 30).”
Research also indicates that African women place a high value on preserving mobility and avoiding medication,27,28 therefore, interventions that emphasize the health benefits of MSE may be well received by this population. This is evident in our study as participants living with a chronic illness were more than three times likely to engage in MSE. Commodore-Mensah and colleagues 26 found some difference in their study of how African immigrant men and women view health, differences that might explain their engagement in MSE. They found that women were more likely to define health in more holistic terms and while men referred to physical strength.
Bodyweight exercises were the most popular mode of MSE in our sample. These exercises do not require any specialized equipment, are easier to access, and can be practiced anywhere. Bodyweight exercises can also require less technical expertise since participants are not confronted with operating machines or figuring out the correct amount of resistance. Using weights and other strength equipment requires skill and women tend to be novice users of exercise equipment. 18 Some studies have also revealed that women, in general, might see gyms and lifting weights as male spaces and, hence, not want to spend as much time in them.16,18
Holistic resistance exercises were the least frequently reported modalities among the participants. This may be attributed to the examples provided in the survey (Yoga, Pilates, and taichi), are both limiting and unfamiliar to this population. While studies on yoga in minority populations are limited, 29 some studies found that while yoga is popular among women, it is practiced most commonly by non-Hispanic white persons in the US,29,30 and long term practitioners of yoga have also been found to be college educated and higher earners.29,31 Another study of low-income African-American women found that many had limited knowledge of yoga, found it cost prohibitive, and lacked representation of diverse bodies. 32 It is also most often associated with other lifestyle choices, such as vegetarianism and veganism 28 or faith 32 and in some African countries, meat is seen as a status symbol and therefore an important part of nutrition, and faith and spirituality may be seen as separate from PA.
Another factor contributing to the limited adoption of yoga by this population could be media depictions of yoga practitioners in the US which usually feature white, thin women, as well as its commercialization for physical fitness leaves out a more holistic approach to health, which is important for this population.29,33 In a study of Congolese immigrants in the US, 34 participants listed dance as being very common within their country, a shared sentiment across many African cultures. 35 Dance is also very popular among women aged 25-75 years, ranking second after walking. 36 Understanding the types of holistic activities common among African immigrant women is necessary to ensure that surveillance studies capture culturally appropriate activities. Expanding the definition of holistic activities to include African dance or other culturally appropriate activities could address this gap.
Some studies have hypothesized that MSE can be more intimidating for novices since it requires a deeper knowledge and understanding of the associated terminology (e.g., repetitions, sets etc.), as well as knowledge of proper equipment use.4,16 Indeed, participants in this study who did not engage in MSE partially credited a lack of self-efficacy or appropriate knowledge. Participants noted not having enough education and experience and, therefore, having a fear of injury, feeling unsure of what to do, and an overall sense that these activities are not safe for them. Assertions such as “I don’t know where to start” (Sudan, 33) are an indication that education will have to be a first step in intervention for many. Educational programs will also need to focus on informing participants that these exercises do not necessarily need equipment and can be performed outside of the gym. 4 Personal coaching could also be encouraged. 37
Overall, exercises that target legs and abdominals were the most commonly reported, regardless of type of MSE. Women may focus on specific body parts to achieve a desired appearance. Participants noted: “I want to add in the right places, this will boost my confidence” (Nigeria, 45) and “I want to lose my stomach fat and cellulite (Nigerian, 19).” Interestingly, we found that while participants’ weight perception was linked to MSE, their actual BMI was not. Previous studies have noted that Black women view BMI standards, particularly the classification of “normal BMI,” as impossible to achieve and not reflective of how they view their bodies with respect to health status. 28 The findings indicate that self-perception of one’s body has a stronger effect on engagement in MSE than does BMI-based weight status.28,38 These perceptions might stem from the current emphasis on body shape and weight, 39 which has an emphasis on thinness. However, for most Black women, shape may be detached from weight in their perception of their body ideal.28,39,40 This indicates an emphasis on shape and not weight, an aspect not captured by BMI. It is crucial to acknowledge that BMI was not initially intended to evaluate health outcomes, and due to its two dimensional measure of body composition, it is a relatively crude index of adiposity and not reliable in differentiating between populations. 41
The relationship between body perception and culture has been noted. 42 However, there has been conflicting research regarding Black women’s notions of body size and acceptance of bigger bodies.28,42,43 On one hand, recent studies do show an increased preference for smaller body sizes by Black women, African women included.28,44,45 In addition, African communities also tend to appreciate and acknowledge different body types, 46 even with a preference for larger body types. Research on MSE reveals that women often fear becoming muscular or looking like men, and hence the opposition to engaging in MSE.15-17,23 Additionally, some women may also not be engaging in MSE as their primary goal might be to lose weight, and therefore engage more in aerobic activity18,23 as one participant stated, “Because I am focusing on being lean and increasing endurance” (Cameroon, 38). This view also has led to the critique of the negative effects of fitness, leading to women having a negative body image, 47
Conversely, women use varied terms to represent socially desired body types. For example, fat, “phat,” 48 and “thick,” 28 are used very differently. Neither “phat” nor “thick” refers to “being fat,” nor are they associated with overweight or obesity.28,48,49 According to Carter-Francique 48 and Gentles-Peart, 49 “thick” refers to the desire for Black women to have curves, to look a certain way but also be a healthy weight. This body shape has also been referred to as the “Coca-Cola bottle shape” in the Caribbean. 49 This is also a way that Black women present their femininity. 28 The desire and acceptance for larger bodies thus does not mean just any body type, but rather, as noted, a specific body type, one that is desirable to the community. For example, abdominal exercises may be executed for the desire to have a flat stomach/ small waist or doing squats and other exercises to make the gluteal muscles prominent. The spread of “Western culture and ideals” through globalization, which is leading to the “standardization” of thin and white bodies 39 as healthy and a norm, is leading to a change around the world, including for African immigrants where perceptions of bigger bodies as pretty and the norm is eroding42,45; and thus we see the increased desire to look a certain way. More research needs to be done on these two points of view, and any intervention to increase MSE in this population should consider their implications in addition to the functional aspects of MSE.
Younger women have been found to engage in high impact and vigorous activity at higher rates than older women. 50 We found that adults aged 25-34 years and over 45 were less likely to meet strengthening guidelines compared to younger adults (18-24 years). These results are consistent with findings from other studies.4,7 One possible explanation is that younger adults may be in college and therfore, have access gyms on their campus, be engaged in college sports or other college based organizations. 48 Also, at this age, childcare and other family responsibilities are less likely to be a major concern.
Income was not a critical factor in determining whether participants met the MSE guidelines, except that our study showed that participants earning over $65,000, about 14% of the study population, were less likely to meet MSE guidelines compared to those earning less than $25,000. The study also found that education did not have an impact on meeting MSE guidelines. While education attainment and higher income have been shown to improve PA engagement, studies have shown that for Black women, there is no statistically significant association between these factors and meeting PA guidelines, even as these factors have been shown to be important for other demographics. 11
Black immigrants often prioritize collectivism, 51 a characteristic that may explain why engaging in PA with others is a significant factor in meeting MSE recommendations. Having a partner is useful for accountability, 52 staying motivated, and for minorities, it might also contribute to feeling safe in different spaces. 53 For religious reasons, having a female partner or partners, is especially prudent. 37 In a study of Somali immigrants in the US, most reported increased comfort in the presence of a group of women. 37 This same sentiment was shared by African immigrants living in Indiana. 43 Some studies have noted that the gendered cultural expectations for women within their families and communities, where women bear large responsibility for caregiving, cooking, etc,50,54,55 may hinder participation in PA, including MSE. Some women also note that responsibilities, such as child care and transportation, shared collectively also increase the possibility of engaging in PA as this reduces the overall burden. 37 Overall, social support has been shown to be critical for Black women in engaging in PA. 11
Only 36.8% (n = 81) of the participants reported high use of their built environment, which included access to parks, trails, sidewalks, etc., and the built environment was negatively associated with meeting the MSE guidelines. Women who used the built environment frequently were less likely to meet the MSE guidelines compared to those who used the built environment more. Opportunities to engage in PA in nature are increased by functional features such as safety, 56 walkability 57 and access to parks, 58 however, what seems to be missing is the functionality to engage in MSE. Added investments into outdoor gyms may be a solution to increase participation. It is important to note that we did not ask participants where they engaged in MSE, and therefore we cannot conclude where they engaged in MSE.
Limitations and Strengths
One limitation for the study was the sample, which may not be representative of the African-born Black immigrant women in the US as convenience sampling was the only strategy employed. Qualtrics, a third party, was used as the physical location of the researchers limited access to a large immigrant community. The use of a third-party survey limits access to knowledge regarding recruitment methods and survey distribution. Nonetheless, this strategy is important as most studies focusing on African immigrants in the US tend to focus on African immigrant groups from a single country or region due to accessibility. However, a strength of the study is data collection from 33 distinct African countries, extending knowledge on immigrants from different places on the continent.
Another limitation of the study is the use of self-reported MSE data, as recall bias and likability bias have been noted in similar studies. Additionally, self-report of time spent on a particular muscle group can lead to unreliable estimates, especially since some MSE movements may overlap or be compounded. Nonetheless, a strength of the study was the use of the MSEQ which employs the correct nomenclature for these exercises, and hence increases validity, an aspect that is not always present in studies on MSE. 9 The MSEQ included examples of the types of exercises, which likely improved measurement accuracy.
To our knowledge, this is one of the few studies that focus specifically on African-born Black immigrants in the US, and their perceptions of muscle-strengthening exercises. African immigrants and Black women are both underrepresented in physical activity research and as such, barriers and facilitators to their participation are poorly understood. By specifically focusing on African-born Black immigrant women, our study fills a critical gap in understanding the heterogeneous characteristics of the Black population in the US, which is often overlooked and summed up under a unified category of Black/African American in health research.
Conclusions
Muscle-strengthening exercises are independently associated with positive health outcomes. 4 However, despite higher levels of MSE engagement among African-born Black immigrant women compared to the general population, promoting MSE remains essential. Self-reported limitations in MSE knowledge, a lack of access to gyms or equipment, and perceptions about body image were identified as key barriers to participation. Motivations for engaging in PA were largely driven by a desire to change body weight. Because women’s engagement in MSE and PA in general is shaped by body perceptions closely tied to their ethnic backgrounds, effective interventions must, therefore, consider these cultural influences. Additionally, this study highlights the importance of the built environment and social support in promoting PA among African-born Black immigrant women.
Findings from this study may be used to guide interventions to increase MSE participation in this population. Interventions, should be culturally tailored as they been shown to be effective in increasing PA among minority populations.15,59 These efforts should prioritize education while also addressing barriers to access. Participants also noted what they believed to be the time-demanding nature of MSE and PA in general; hence, a general exploration of MSE should be incorporated into the educational component. This study has shown that African-born Black immigrant women care about their health and fitness and understand the overall health benefits of PA. Future interventions can capitalize on this understanding to promote greater participation in muscle-strengthening activities. 60
Supplemental Material
Supplemental Material - Associations Between Demographic and Socioeconomic Factors, Perceptions, and Attitudes Towards Muscle-Strengthening Exercises Among African-Born Black Immigrant Women in the United States
Supplemental Material for Associations Between Demographic and Socioeconomic Factors, Perceptions, and Attitudes Towards Muscle-Strengthening Exercises Among African-Born Black Immigrant Women in the United States by Bose Maposa, Zelalem Haile, Dawn Graham, Emily Hill Guseman in American Journal of Lifestyle Medicine.
Consent to Participate
Informed consent was obtained from all individuals included in the study.
Footnotes
Author’s contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Bose Maposa. Quantitative data analysis was performed by Bose Maposa and Zelalem Haile with input from Emily Guseman. Qualitative data analysis was performed by Bose Maposa and Dawn Graham. The first draft of the manuscript was written by Bose Maposa and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the university Student Enhancement Award.
Ethical Approval
This study was approved by the authors’ Institutional Review Board (#23-E-131 and #FY25-625).
Data Availability Statement
The data supporting the study cannot be shared publicly as participants only consented to the research team accessing their data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.