
Abstract
Intrinsic capacity (IC) is defined as the set of individual physical and mental abilities, the preservation of which will influence functional skills throughout aging. Therefore, it is important that its assessment be incorporated into healthcare services to support the adoption of preventive approaches in the field of gerontology. This study aimed to evaluete the factors associated with good intrinsic capacity (IC) among community-dwelling older adults participating in social groups in Brazil. This is a cross-sectional study that assessed the 5 domains of IC, using validated instruments, and analyzed the association of the total IC score with sociodemographic data, health conditions, history of falls, mobility in the living space and balance. 170 individuals aged 72.3 (±8.0) years participated in the study, mostly female. Half of the subjects had preserved IC, who showed better performance in all domains. The factors negatively associated with IC were an income below the minimum wage (OR 0.026 [0.002-0.296]) and number of comorbidities (OR 0.691 [0.536-0.890]), while the number of surgeries (OR 1.326 [1.058-1.661]) and good balance (OR 1.417 [1.216-1.651]) were positively associated with IC. These results point to specific strategies to address the demands of the population in the pursuit of IC preservation.
“Regression analysis showed that low income was strongly associated with reduced odds of preserved intrinsic capacity.”
Introduction
Aging is a complex individual event where there is both the onset of physiological declines and changes in social positions and motivational priorities. 1 New perspectives in gerontology present the maintenance of functional ability as synonymous with healthy aging, being closely associated with the possibilities valued by the person. 2 Functional ability is the result of the interaction between the individual characteristics of the older person and the environmental factors in which they are inserted, in a continuous and variable process over the years. 3 The set of individual characteristics, both physical and mental, is called intrinsic capacity (IC), which is composed of 5 domains that interact with each other, resembling the theory of aging: cognitive, locomotor, sensory, psychological, and vitality capacity.4,5
IC is presented as a positive approach strategy on aging as it emphasizes health attributes, and the physiological reserve developed and maintained throughout life. 4 It is influenced by both biological and socioeconomic and environmental factors and depends on social determinants in health and public policies. It therefore needs to be often monitored and preserved throughout the course of life. In face of this need, the WHO 1 launched the ICOPE (Integrated Care for Older People) strategy, a set of guidelines to operationalize integrated actions at the primary level of health care with focused on preserving the IC of older people living in the community, or to seek mechanisms to maintain functional ability if damage to the IC is already installed. How these strategies are approached will depend on the context of each country. 4
Among health promotion strategies, social groups have been a stimulated option throughout Brazil, because they can provide physical, mental and social benefits to older people. 6 Santos et al. 7 highlight that the active person, who is a member of strengthened social networks, experiences the aging process in a different way from the one who does not participate. In addition, preventive activities developed in groups have a low cost and high effectiveness in the health and quality of life of this population. 8
Considering the foregoing, the objective of this study was to investigate the factors associated with good IC among older people participating in social groups in Amazonas - Brazil.
Materials and Methods
This was a cross-sectional study conducted from September 2022 to May 2023 at a living center in Amazonas. People aged 60 years or older, of both sexes and who participated in some group at the site were included in the study. People who were experiencing acute symptoms at the time of the approach, such as severe pain, fever or dyspnea, were excluded, as well as those who had advanced changes in speech, hearing, or cognition that may make communication impossible, and those with uncompleted assessments.
For the sample calculation, the number of people registered in the center (1000 older) was considered. To obtain an 80% confidence level and the alpha error probability of 5%, expecting a prevalence of IC decline of approximately 25% 9 and predicting potential losses in the order of 10%, the minimum total sample size was 131 (one hundred and thirty-one) subjects.
After invitation, appointments were made following the availability of the participants. Assessments were performed at 1 or 2 times so that the routine activities were not impaired, and a maximum period of 10 days was adopted for the completion of the assessment protocol.
Instruments and Variables of Interest
After formal agreement, demographic, socioeconomic (years of study, income, social support, and socialization) and health conditions (health perception, level of physical activity, smoking, alcohol consumption, comorbidities, medications, surgeries, pain, sleep problems, and leisure activities) were collected. IC’s domains, life space mobility, balance and history of falls were also assessed.
Physical activity level was assessed through the International Physical Activity Questionnaire - IPAQ Short Version,10,11 being considered the metabolic equivalent of the task (MET) for the classification of participants in high, moderate or low physical activity.
Considering the heterogeneity in the IC assessment protocols, we sought to elect the instruments that objectively evaluated the 5 IC’s domains recommended by step 2 of the ICOPE strategy 4 : cognitive, psychological, sensory, vitality, and locomotion.
Cognitive assessment was performed using the 10-point Cognitive Screener (10-CS), 12 which assesses temporal orientation in day, month, and year, category fluency, and 3-word recall, whose total score is adjusted for the level of education.
The psychological assessment was performed using the geriatric depression scale – 15-item GDS, with the cut-off point starting from 5 points for suspected depression.13,14
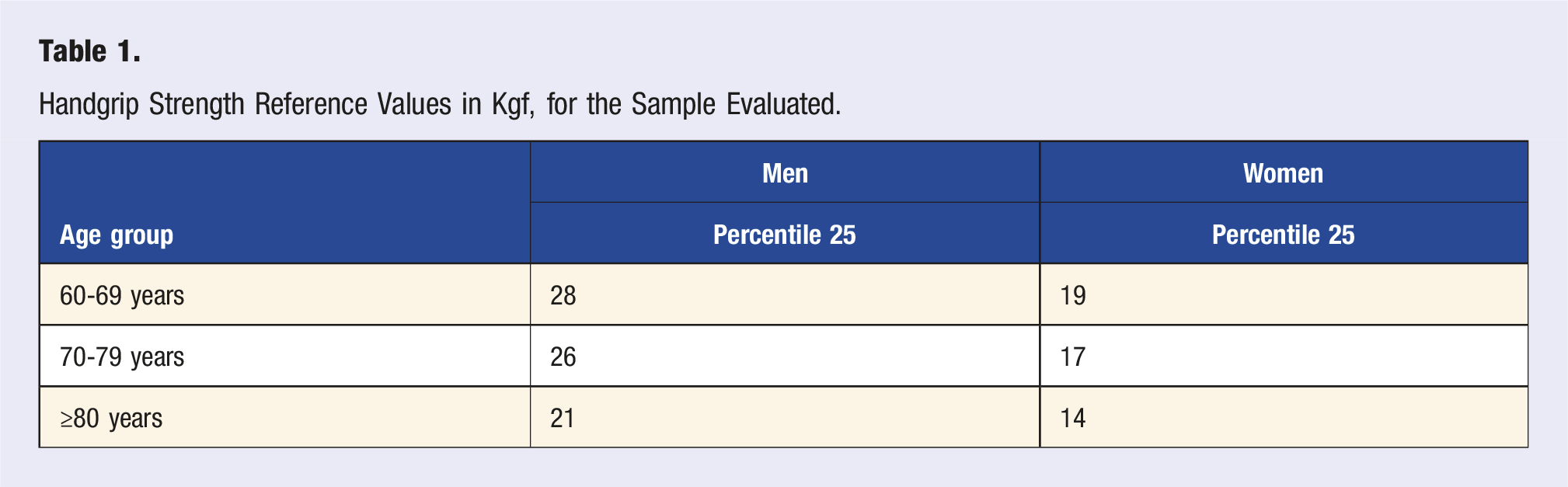
In the sensory domain, visual acuity was assessed using the simple visual table of the 4 “Es” (4), and hearing was assessed by means of the whisper test, 15 with normal hearing acuity being considered a three- to four-word repetition on each side. 4
Locomotion was evaluated through the Short Physical Performance Battery - SPPB, whose version adapted for Brazilians by Nakano 16 showed good reliability. This is a battery that measures timed performance in 3 tasks: Semi-static balance, 4-meter gait speed test, and 5-time chair stand and sit test.
Handgrip Strength Reference Values in Kgf, for the Sample Evaluated.
The calculation of the total IC score was operationalized based on the proposal of López-Ortiz et al.,
20
where each domain received a score of 0 to 2. The IC score resulted from the sum of the scores of the 5 domains, being classified in: Bad IC (0-4 points), mildly altered IC (5-8 points), and good IC (9-10 points) (Figure 1). Adapted from López-Ortiz et al. (2022). 10-CS: 10 point Cogntive Screener; GDS-15: Geriatric Depression Scale; SPPB: Short Physical Performance Battery; 4Es: simple visual table of the 4 “Es”; MNA: Mini Nutritional Assessment®; HST: handgrip strength test.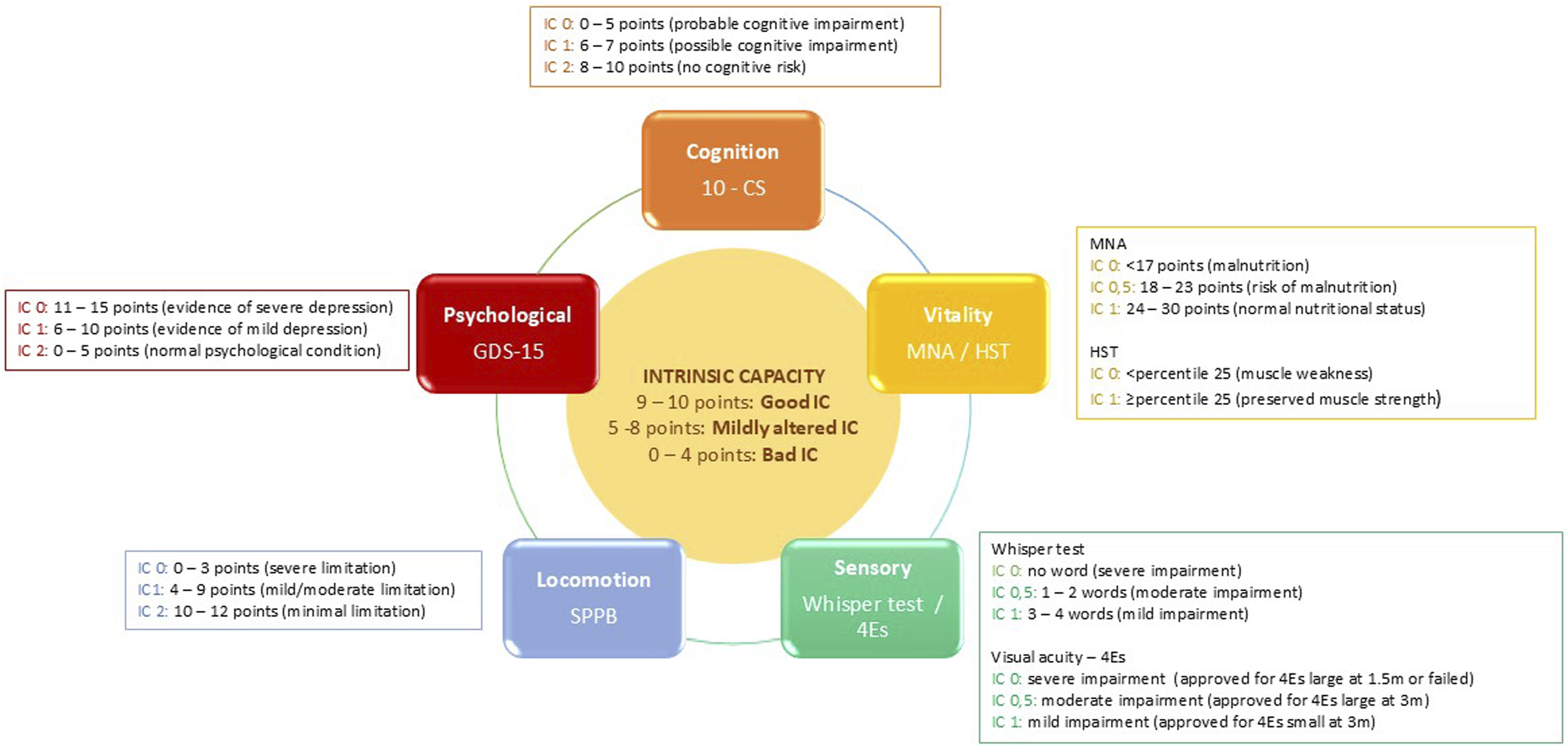
Lifespace mobility was analyzed through the instrument “The university of Alabama at Birmingham Study of Aging life-space Assessment” (LSA), validated for the Brazilian population by Simões et al. 21 It considers mobility in 5 levels of living space, from house rooms (level 1) to places outside the city (level 5). For this study, the maximum life-space level was recorded, with or without personal or equipment assistance.
Balance was assessed through the Mini Balance Evaluation Systems Test - Mini BESTest, consisting of 14 items that generate a total score of up to 28 points, being greater the better the performance in the tests. 22 Its Brazilian version showed adequate reliability and validity of the construct. 23
To assess the history of falls, the following question was applied: “Had Mr(Mrs) ever fallen or had usually fallen over the last 6 months?”, with a fall defined as “unintentional displacement of the body to a level below the starting position, caused by multifactorial circumstances, whether or not resulting in damage.” 24
Data Analysis
In descriptive analysis, categorical data were expressed by absolute and relative frequencies, and continuous data by means and standard deviations (SD). For comparative analysis of potential associated factors, individuals were assigned to 2 groups: preserved (good IC—score of 9 to 10 points) and impaired intrinsic capacity (poor or mild IC—score of 0 to 8 points); chi-squared tests of independence and t-Student were employed to analyze categorical and continuous variables, respectively.
Finally, a multivariate logistic regression analysis was developed to test the association between IC and the other independent variables. This analysis was performed in stages, in which the variables that presented significance in the univariate analyses were inserted, and 4 models were proposed: model 1 containing socioeconomic variables; model 2, where health variables were added; model 3, in which variables regarding balance and mobility in the life space were added; and the final model, with the variables that had significant relationship to the IC score in the previous models.
The performance of the final regression model was evaluated using the values of chi-square and Nagelkerke’s R2. Analyses adopted statistical significance level P < 0.05 and were developed using the SPSS statistical software version 20.0.
Results
A total of 170 individuals aged 72.3 (±8.0) years, mostly female (71.8%), who practiced more than one activity, were distributed in physical activities (gymnastics, hydrogymnastics, Pilates, dance, elaborate gymnastics, and walking), cognitive activities (memory workshop and literacy), and artistic/recreational activities (singing, handicraft and games) participated in the study.
Distribution of Older Subjects Participating in the Study Regarding Intrinsic Capacity (IC) Domains and Score.
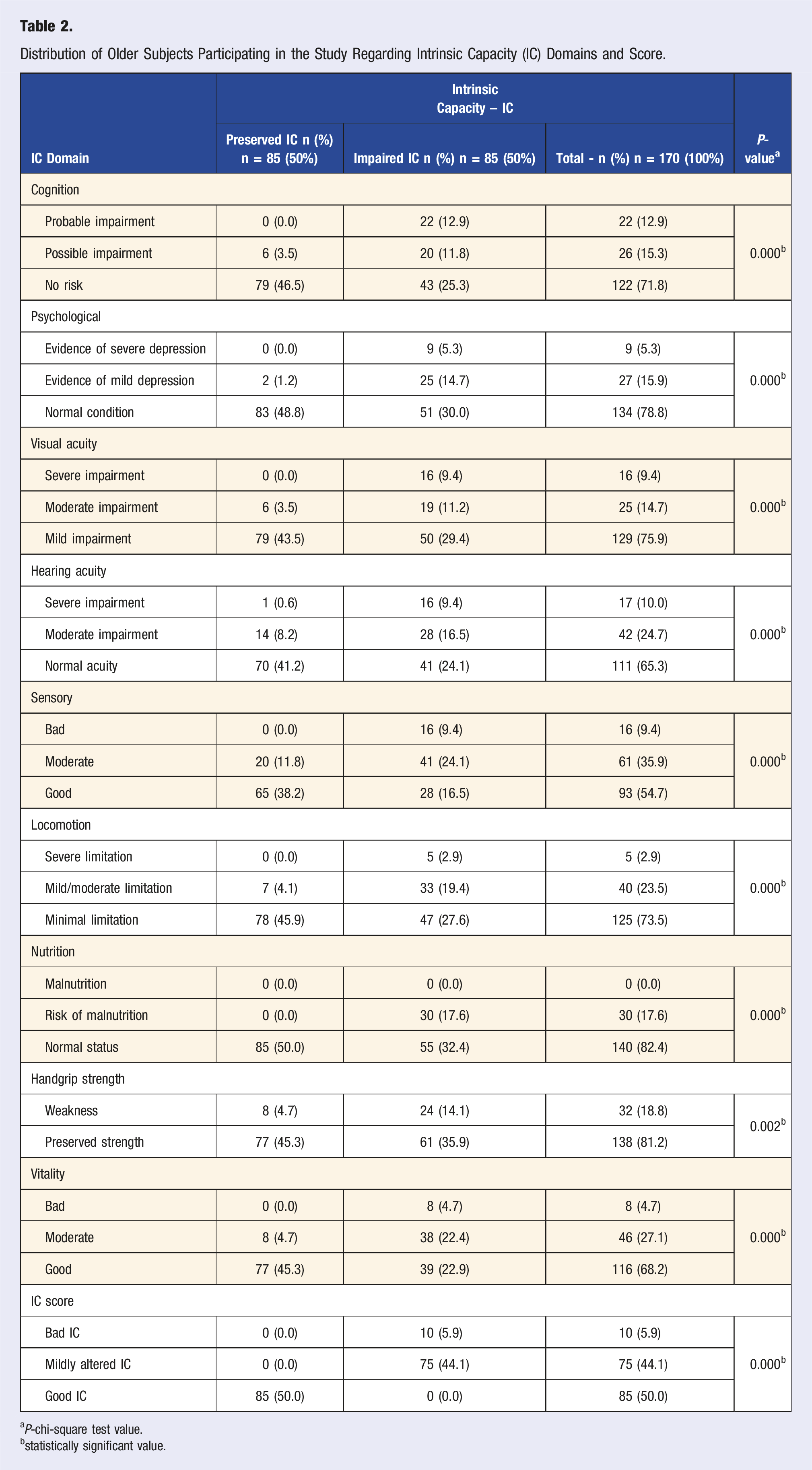
aP-chi-square test value.
bstatistically significant value.
Aspects Associated With IC Among Older People Participating in the Study.
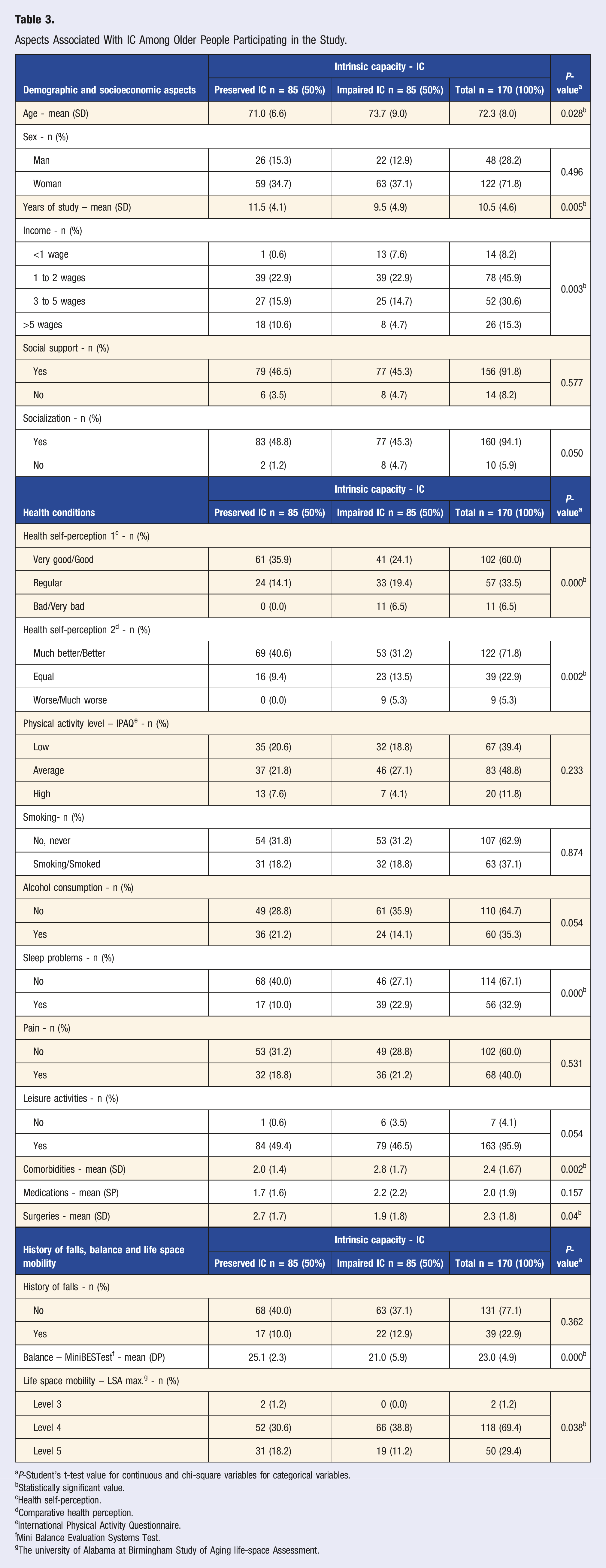
aP-Student’s t-test value for continuous and chi-square variables for categorical variables.
bStatistically significant value.
cHealth self-perception.
dComparative health perception.
eInternational Physical Activity Questionnaire.
fMini Balance Evaluation Systems Test.
gThe university of Alabama at Birmingham Study of Aging life-space Assessment.
There was no significant difference between the IC groups in sex, occupation, social and social support, physical activity level, smoking, alcohol consumption, number of medications, pain, leisure habits and history of falls (Table 3).
Multivariate Logistic Regression Models to Assess Factors Associated With Intrinsic Capacity Among Older Individuals Participating in the Study.
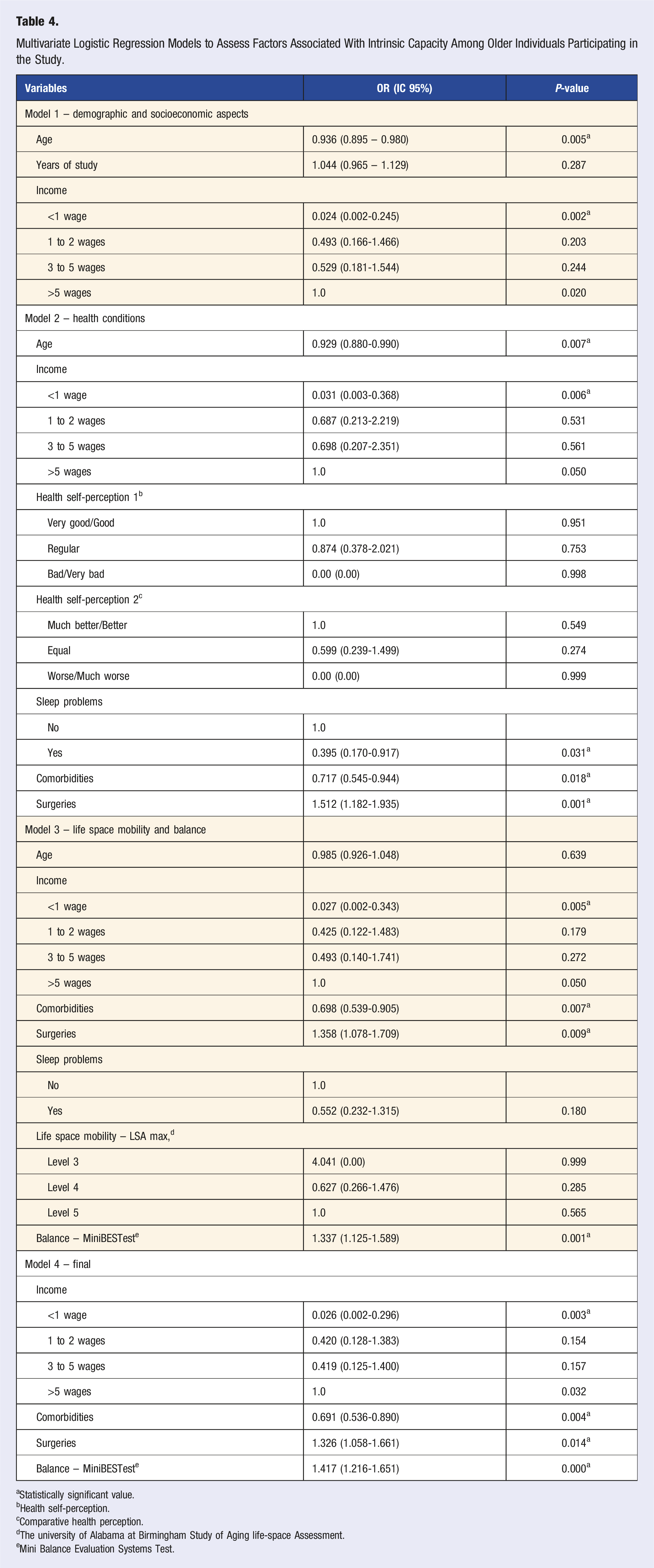
aStatistically significant value.
bHealth self-perception.
cComparative health perception.
dThe university of Alabama at Birmingham Study of Aging life-space Assessment.
eMini Balance Evaluation Systems Test.
Discussion
This study aimed to analyze the factors associated with good IC among older people participating in social groups. Among the factors evaluated, low income and number of comorbidities were negatively associated with preserved IC, while the number of surgeries and good balance were positively associated.
Half of the sample had preserved IC, higher than the prevalence described by Muneera, Muhammad e Althaf, 25 a prevalence of 24.56% among Indian older adults, possibly due to the peculiarities of the group evaluated in this study, pointing to the possible positive influence of the social groups on IC. Comparison with other studies was hampered by the heterogeneity of the methods to generate the IC score and classification.
Although a difference in age between groups was found, the final regression model ruled out the relationship between age and IC, as shown in the study conducted by Aliberti et al., 26 which reinforces the importance of considering biological and nonchronological age in the individualized measurement of IC, due to interferences distinct from physical, mental and social conditions, which characterize the heterogeneity of the aging process.
The predominance of women among participants reinforces other references that women seek more for better health conditions.27–29 However, sex was not an element associated with maintenance or decline of IC, which is aligned with the findings of the studies by Rao et al. 30 and Ma et al., 31 possibly because older men in this sample, like women, also engage in health-benefiting activities.
In both groups, most people reported incomes equivalent to 1 to 2 wages. Regression analysis revealed that having an income below the minimum wage could reduce the chance of having preserved IC by 38.46 times. This relationship was also cited in the results of Ma et al. 31 confirming the influence of income on health, which shows that public policies are still marked by strong inequities in the region. The study by Freire Junior et al. 32 highlighted the negative impact of living in regions with unfavorable socioeconomic conditions on gait performance, and this behavior may reflect on IC. In addition to the income itself, the perception of financial adequacy is another point related to the preservation of IC. 33
Although the majority reported high education, the relationship between the years of study and the IC was not supported by the model, probably due to education having less interference with the IC when interacting with income, again emphasizing that the socioeconomic disparities, which are marked in the North region of Brazil, may interfere with the health of the older population.
No association between smoking and alcohol consumption with IC was found in these people, although there are other studies26,27 pointing out both negative and positive relationships between these habits and the IC. It is possible that in this sample, the practice of physical activity has minimized the influence of these habits on IC. The more detailed description of current and/or past alcohol consumption (number of doses and frequency) and smoking (tobacco load) could reinforce this information.
In this study, everyone participated in the activities, causing no difference in the level of physical activity between the IC groups to be found. Despite the fact that there are studies depicting the relationship between moderate and vigorous physical activity and high IC,25,31 these studies did not evaluate participants in social centers, which makes it difficult to compare the results. Studies comparing older adults participating and not participating in social centers are suggested to confirm or rectify this finding.
The number of comorbidities had a negative relationship with IC, so each additional comorbidity offered a 1.44 reduction in the odds of having preserved IC. This relationship has been reinforced in the literature.26,33,34 Among the comorbidities, arterial hypertension, 35 chronic neuropathies 30 and osteoarthritis 31 were highlighted, in agreement with the present study. These results reinforce the importance of chronic condition prevention and control measures to prevent declines in IC. It is important to highlight, however, that comorbidities were assessed merely as a simple count, without using a validated instrument. The adoption of standardized measures could have enhanced the robustness and comparability of the findings, and future studies should incorporate validated tools for comorbidity assessment.
Curiously, the regression model revealed that subjects with the highest number of surgeries were more likely to belong to the IC preserved group at 1.32. A possible explanation is that the number of surgeries may be indicative of a better access to therapeutic resources and prevention of health problems. More detailed information about the type of surgery would allow 1 to confirm such information. No other report of this relationship was found in the literature searched.
No associations between IC and the presence of physical pain or sleep problems were confirmed in this study, which may be related to the lower frequency of these conditions among subjects in both groups, not impacting overall well-being. It is possible that information about the characteristics of pain and sleep changes such as duration, time, intensity, aggravating or mitigating factors may reveal this relationship.
The association between health self-perception and IC was not confirmed in the regression model, indicating that even if negative health perceptions were reported only by the impaired IC group, it is possible that positive perceptions were referred to by people with mildly altered IC, since it is a group that participates in health promotion activities.
Overall, the history of falls over the last 6 months was reported by 22.9% of the study participants, prevalence lower than that described by Ulian 36 in São Paulo, which was 36.8%. The lack of association between history of falls and IC in this study may be related to the cross-sectional design. It is possible that this relationship may be in longitudinal studies, such as that of Tay et al., 37 which reveals that a high IC reduces the chances of falls within 1 year.
Regarding the balance, considering the cut-off points of the Mini BESTest for the prediction of falls cited by Magnani et al., 38 group scores revealed mean values above the cut-off point in the preserved IC group, while in the impaired IC group the score was below the cut-off point, that is, higher risk of falls. In addition, the regression model pointed out that the increase in Mini BESTest score in a standard deviation increased the chance of having preserved IC by 1.41.
In both groups, most of the participants presented LSA at maximum levels (mobility beyond the neighborhood and beyond the city), reflecting good participation. Despite this, the relationship between maximum LSA and IC was not maintained in the multivariate model, possibly because it is a resultant factor not only of intrinsic factors, but also environmental and social factors. 39 Furthermore, the maximum level of participation, regardless of care, was considered in this analysis, and even subjects with impaired IC may have a high level of participation.
Study Advantages and Limitations
It is believed that this is one of the few studies focused on a more positive perspective of aging, focusing on the preservation of IC and its domains and, for this, used a public composed of active older people, in order to evaluate the possible changes in IC as early as possible to the installation of functional limitations.
Another advantage is that IC was the primary object of this research, which provided the opportunity for the adoption of an evaluation protocol with validated and objective instruments for the better detection of IC characteristics, aiming to contribute to the reduction of heterogeneity between the procedures adopted.
Despite the positive points, the results of this study must be interpreted considering some limitations, the first of which is the cross-sectional design of the study, given that the IC should ideally be evaluated longitudinally. However, these results may be the starting point for future longitudinal research.
In spite of the wide variety between procedures for obtaining the composite IC score, we decided to employ a simplified method in which possible differences in the interference of each domain in the total IC score were not accounted, what may have interfered with the results. However, a method already tested and employed by other authors was used, the proposal of which is to facilitate the assessment of IC in the practice of health services.
Another limitation concerns the way health conditions were analyzed. Smoking and alcohol consumption were recorded only in a binary form, without detailed information on intensity, duration, or lifetime exposure, which may have masked possible associations with IC. Similarly, comorbidities were analyzed only as the number of conditions, without applying a validated index, and the variable ‘surgeries’ was considered only as the total number of procedures, without specifying type or indication. These methodological choices limit the depth of the conclusions, reinforcing the need for more detailed approaches in future studies.
It is important to reinforce that these findings refer to a specific audience of older people from a city in Northern Brazil who participate in health promotion activities and cannot be generalized to the entire older population.
Conclusions
This study found preserved Intrinsic Capacity in half of the participants, who performed better in all domains when compared to participants with IC impairment. The factors negatively associated with IC were income below a minimum wage and number of comorbidities, while the number of surgeries and good balance were positively associated with IC. However, these associations must be interpreted with caution, especially regarding comorbidities, surgeries, and smoking and alcohol consumption habits, as they have not been examined in detail. Therefore, more in-depth and methodologically robust studies are necessary to confirm these findings and to clarify the factors associated with IC in older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Fundação de Amparo à Pesquisa do Amazonas (FAPEAM) (013/2022 – PQFAPEAM II/II).