
Abstract
Bacterial vaginosis (BV) is the most prevalent vaginal infection of reproductive-aged women, with unclear causes and links to adverse gynaecological health outcomes. Fluctuations in gut microbiota from dietary carbohydrate intake may alter the vaginal microbiota. This systematic review aimed to identify an association between BV and dietary carbohydrate intake, Glycaemic index (GI) and Glycaemic Load (GL), total sugars, and dietary fibre. A literature search was conducted in April 2022 using MEDLINE, CINAHL, and Scopus databases. The pre-determined inclusion criteria were females, nutritional intake, diet, macronutrients, BV, and vaginal dysbiosis. The risk of bias was assessed using the AXIS tool for cross-sectional studies, and the CASP tool quality assessed the case-control. Four studies met the inclusion criteria: 3 cross-sectional and 1 case-control. The findings showed a positive association between higher GL intake and BV and an inverse association between higher dietary fibre intake and BV. However, the overall risk of bias was moderate to high. While a diet high in fibre may be protective and high GL may increase BV risk, the limited and inadequate quality evidence means these findings should be interpreted with caution. Further research is necessary to confirm these associations and inform dietary recommendations.
‘Dietary modifications may have therapeutic benefits for patients with re-occurring BV’.
Key Points
(1) A diet higher in fibre intake may help reduce the risk of re-occurring bacterial vaginosis. (2) A higher glycaemic load diet may be associated with an increased risk of bacterial vaginosis. (3) Nutritional advice on diet quality (fibre intake and glycaemic load) could be a beneficial element in the prevention of re-occurring bacterial vaginosis.
Introduction
Bacterial vaginosis (BV) is a condition in which there is dysbiosis in the vaginal microbiota, 1 with BV being the most prevalent vaginal infection in women of reproductive age. 2 The prevalence in the UK is between 10%–20% 1 and based on the NHANES 2001-2004 3 study, 29.2% of women between the ages of 14-49 were affected and 84% reported to be asymptomatic. Additionally, BV is more prevalent among women of colour, however there is limited understanding of the cause. 4
BV is not a sexually transmitted disease (STI); however, it can be transmitted through intercourse 5 and is known for being highly persistent even after treatment6,7 with no clear aetiology. Risk factors include vaginal douching, 8 having new or multiple partners, 9 smoking, using a copper intrauterine device, menstruation, and semen in the vagina. 10
BV has been associated with serious adverse health outcomes. These include increased risk of infertility11,12; adverse pregnancy outcomes 13 ; pelvic inflammatory disease (PID) 14 ; endometriosis 15 ; human immunodeficiency virus (HIV) 16 and STIs including chlamydia, gonorrhoea 17 and human papillomavirus (HPV). 18 Additionally, symptoms, such as a fishy odour, 8 have caused feelings of embarrassment for women and has negatively impacted their self-esteem and sex life. 19
Even though it is diagnosed in millions of women every year, BV continues to be a condition that is ill-defined, unclearly diagnosed, and poorly treated. 20
Gut Microbiota & BV
There is emerging evidence suggesting an important relationship between nutrition and the gut microbiota, with diet having an important role in mediating the microbial system of the gastrointestinal tract. 21 Scott et al. 22 suggest that altering the amount and/or type of dietary carbohydrate can have a serious impact on the composition of the gut. Additionally, Bernalier-Donadille 23 indicates that the available substrates for gut fermentation, such as plant polysaccharides, are correlated with the metabolic functions of the human gut microbiota affecting overall health.
A potential explanation for the association between carbohydrate and BV is the microbial system of the gastrointestinal tract being linked to the vaginal microbiota. Antonio et al., 24 found similarities between Lactobacillus bacteria species in the vagina and rectum, suggesting that the gut microbiota could serve as a source for vaginal colonisation via the rectum. This is also supported by Marrazzo et al. 25 who found that non-BV women may acquire BV via extravaginal colonisation of BV associated bacteria. This suggests that alternations to the gut microbiota via dietary carbohydrate may cause changes to the vaginal microbiota causing BV. Although this may provide a temporary explanation of the relationship between the gut and vaginal microbiota, evidence is still limited, and more research is needed.
An article review by Mizigier et al. 26 examined the role of diet and probiotics in the prevention and treatment of BV in non-pregnant women and adolescent girls. Regarding the influence of dietary carbohydrate on BV, it was stated that the development of abnormal vaginal flora was promoted by the dietary intake of simple sugars, and that maintaining a low dietary glycaemic load would benefit the vaginal area by preventing pathogenic microorganisms becoming established and reducing the inflammatory response. It was also suggested that as prebiotics, which can include types of dietary fibre, can benefit the gut microbiome and overall health, they may be able to promote vaginal health; however, the review did not provide specific details on the link between prebiotics and BV or vaginal health more widely.
In a literature review by Barrientos-Duran et al., 27 modifiable and non-modifiable factors that could affect vaginal microbiota homeostasis were considered which included probiotics and diet. The discussion relating to diet was predominately based on BV studies that found nutrients such as Beta-carotene, vitamins (A, B, C, and E) and minerals (zinc and calcium) connected to the reduction of BV prevalence and overall vaginal wellness. However, GL was referred to with a higher GL being related to BV progression and persistence, but no further information on dietary carbohydrate intake was discussed. Furthermore, the use of prebiotics, and dietary fibre, and how these may influence BV was not discussed.
To the best of the researchers’ current knowledge, there is no systematic review assessing the association between dietary carbohydrate and BV. The aim of this review is to identify if there is an association between BV and dietary carbohydrate intake, including GI and GL, total sugars, and dietary fibre.
Methods
This review was conducted and reported using the PRISMA 2020 checklist 28 to support transparency in reporting. 29
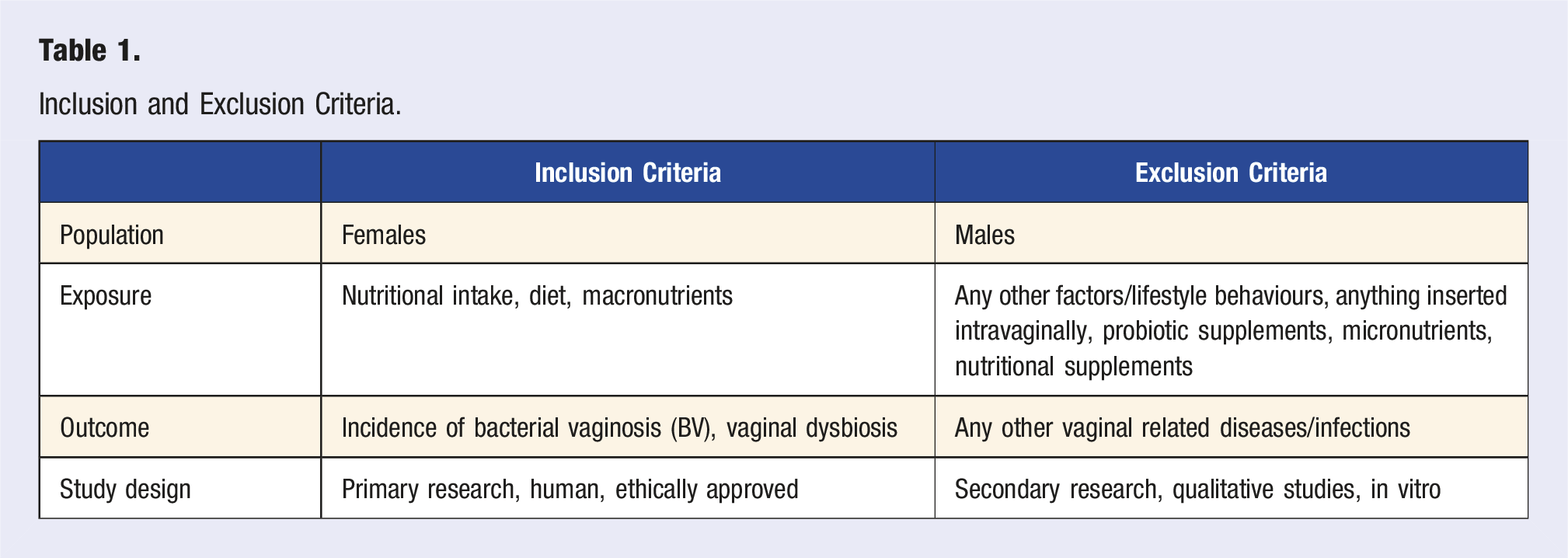
Eligibility Criteria
Inclusion and Exclusion Criteria.
Search Strategy
A full search strategy was developed by testing and refining it to achieve relevant studies (Supplement 1). MEDLINE, CINAHL, and Scopus health care databases were used for the search in April 2022. Limiters used were Human, English language and Females and to ensure that no studies were missed, the timeframe was not limited to the publication date. Lastly, after the title and abstract were screened, the reference lists of the studies were also searched for additional relevant studies.
Data Extraction
The data extraction tool used was created for this review by piloting it on an included study and adapting it accordingly to ensure its usability 31 (Supplement 2). The adaptation primarily focused on retrieving the appropriate details of assessment methods and specific results. The data extracted included study and participant characteristics, assessment methods for BV and dietary exposure, and results relating to BV comparison, dietary carbohydrate intake, GI and GL, total sugars, and dietary fibre. They were grouped into GI&GL and carbohydrates, total sugars and fibre for synthesis. Only one reviewer screened each record and summary tables were used to display data.
Risk of Bias Assessment
The risk of bias for included studies was assessed using the AXIS tool 32 for cross-sectional studies. The case-control was not assessed for risk of bias, it was only quality assessed with the CASP tool. 33
Results
Study Selection
Once duplicates were removed, the titles and abstracts of 590 studies were screened against the inclusion and exclusion criteria, with 7 studies remaining (Figure 1). They were sought for retrieval and full text screened; 3 did not assess BV, so they were excluded, and 4 eligible studies remained.34-37 Only one reviewer screened each record. Prisma flow chart.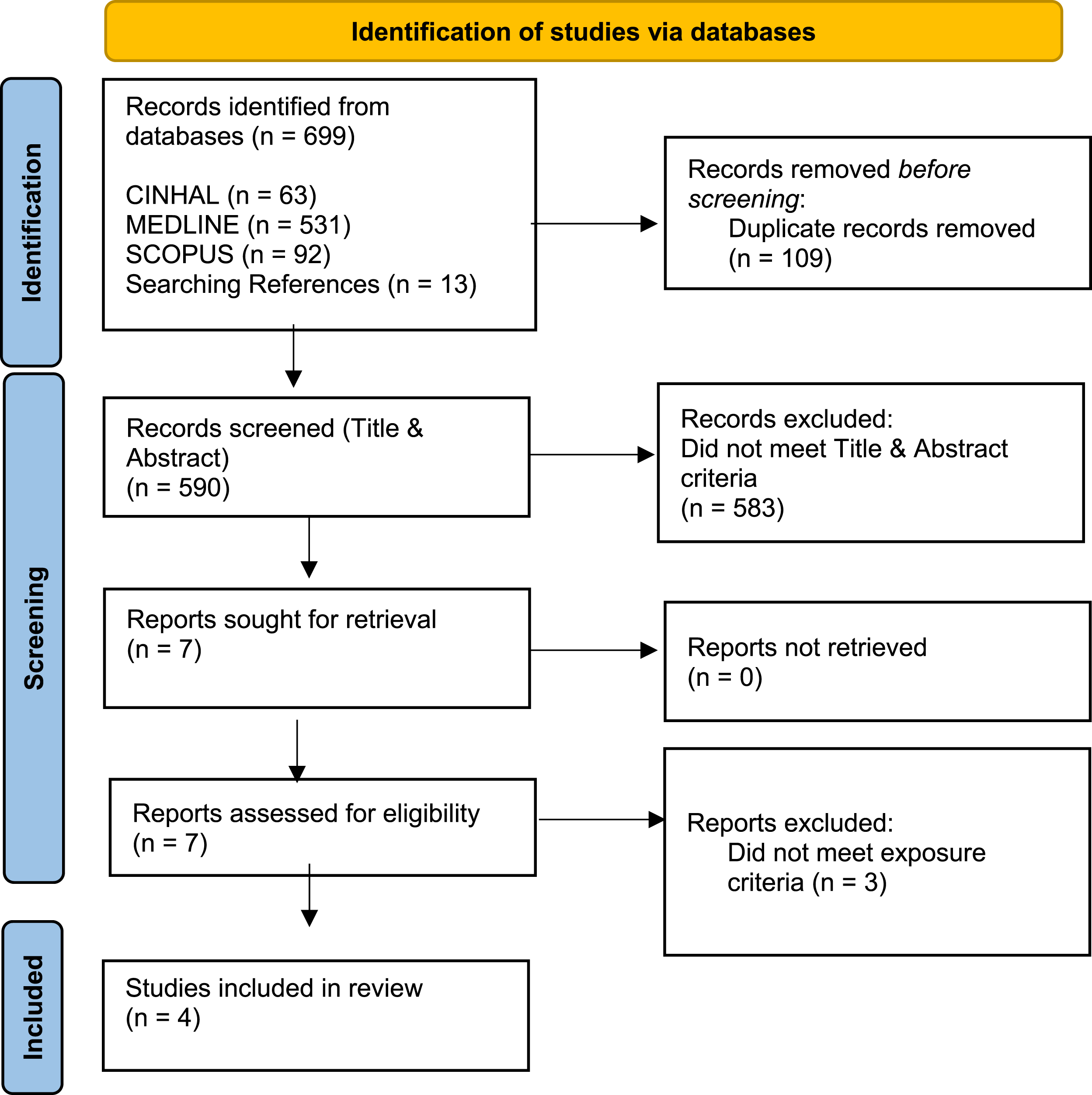
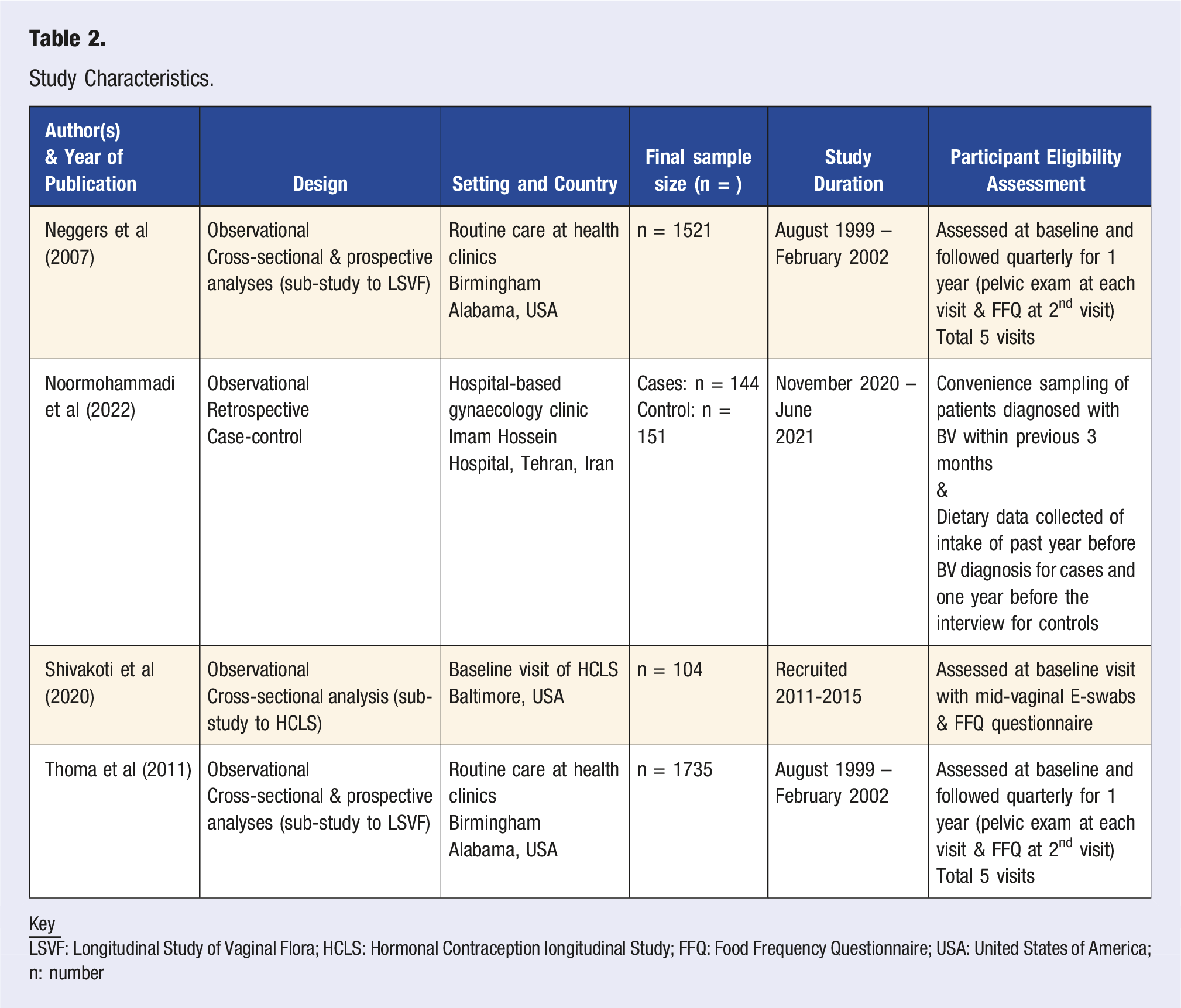
Study Characteristics
Study Characteristics.
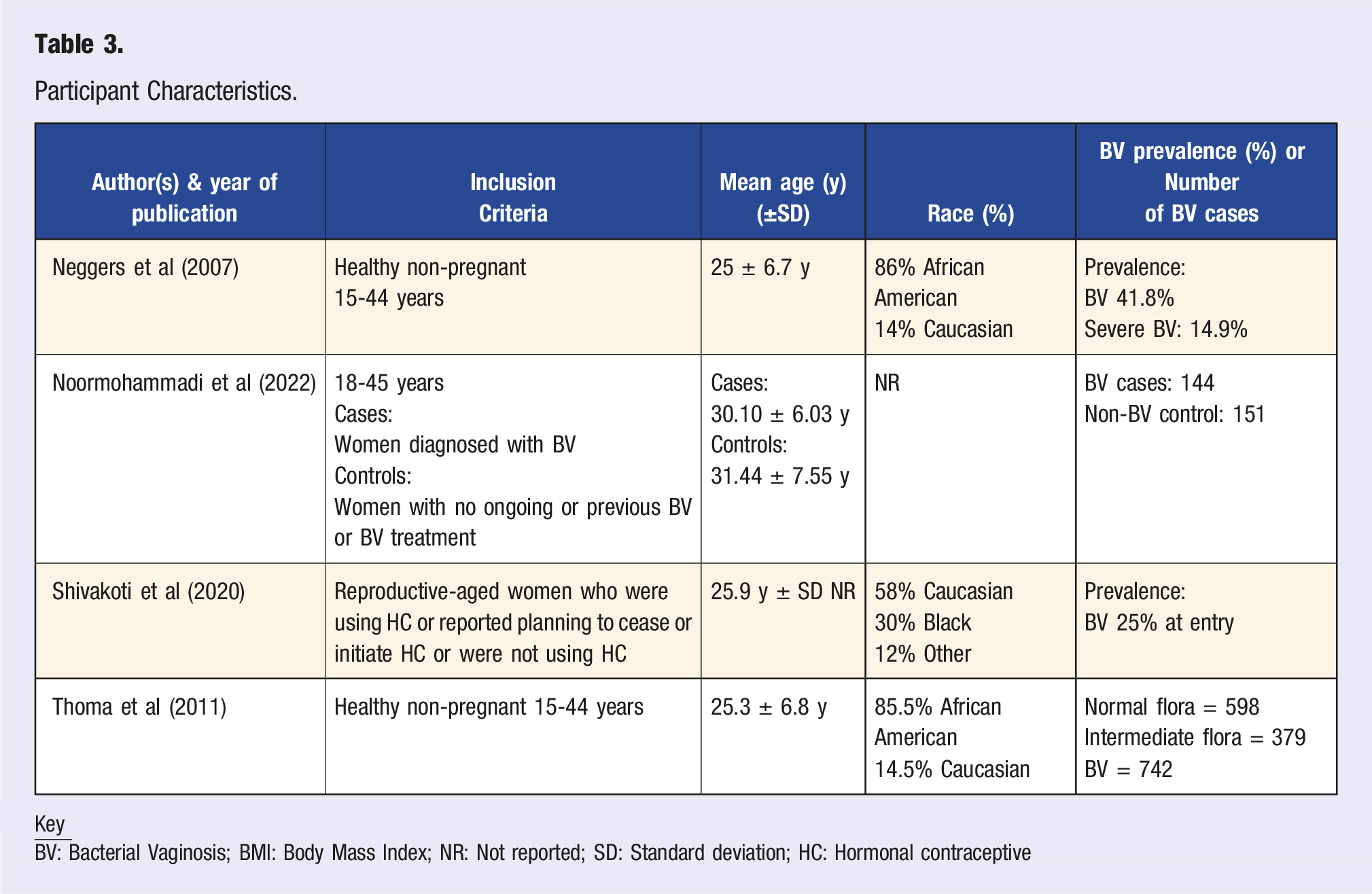
Participant Characteristics
Participant Characteristics.
Nutrient Results
GI & GL Results.
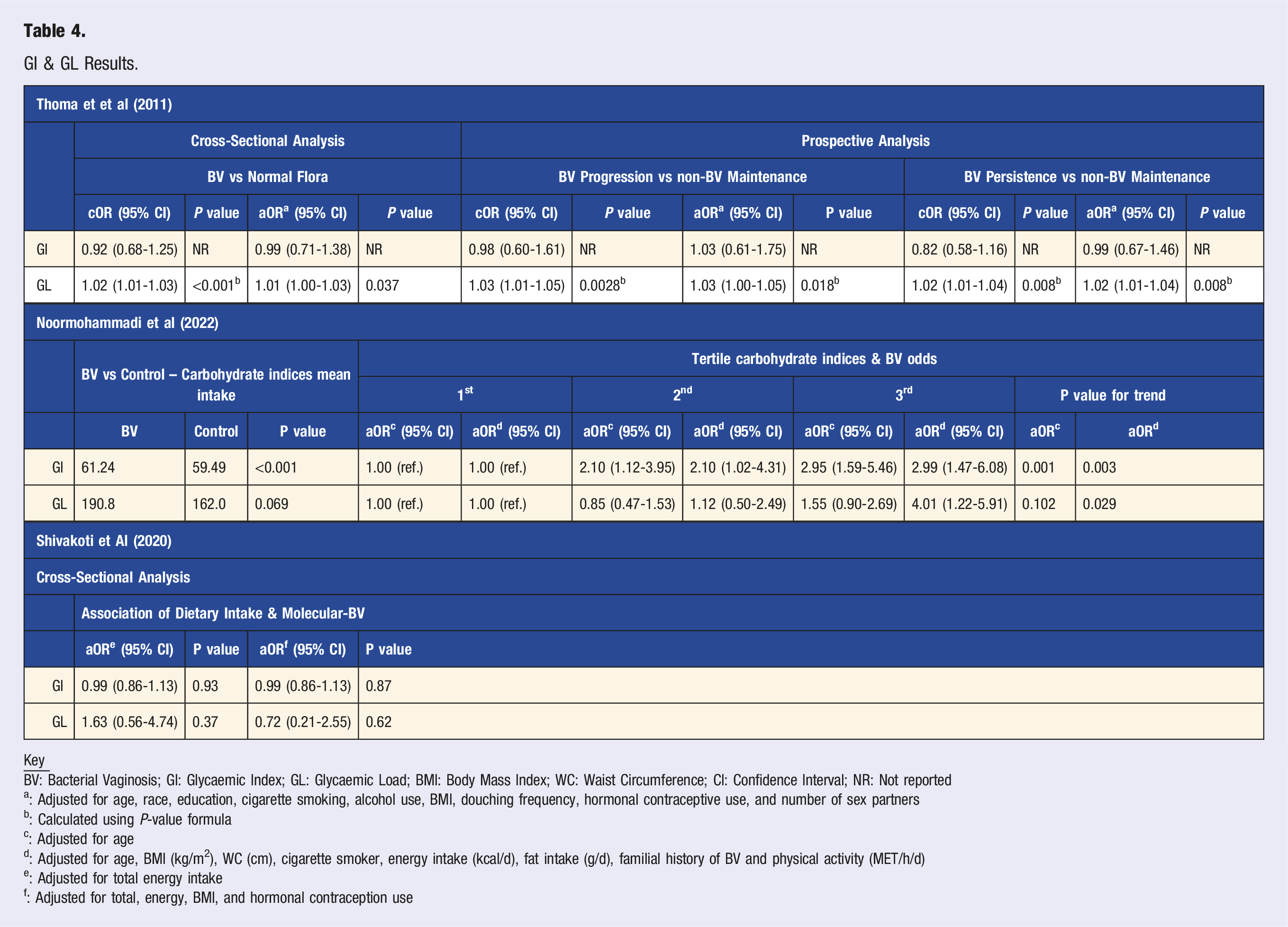
a: Adjusted for age, race, education, cigarette smoking, alcohol use, BMI, douching frequency, hormonal contraceptive use, and number of sex partners
b: Calculated using P-value formula
c: Adjusted for age
d: Adjusted for age, BMI (kg/m2), WC (cm), cigarette smoker, energy intake (kcal/d), fat intake (g/d), familial history of BV and physical activity (MET/h/d)
e: Adjusted for total energy intake
f: Adjusted for total, energy, BMI, and hormonal contraception use
Carbohydrate, Total Sugars & Fibre Results.
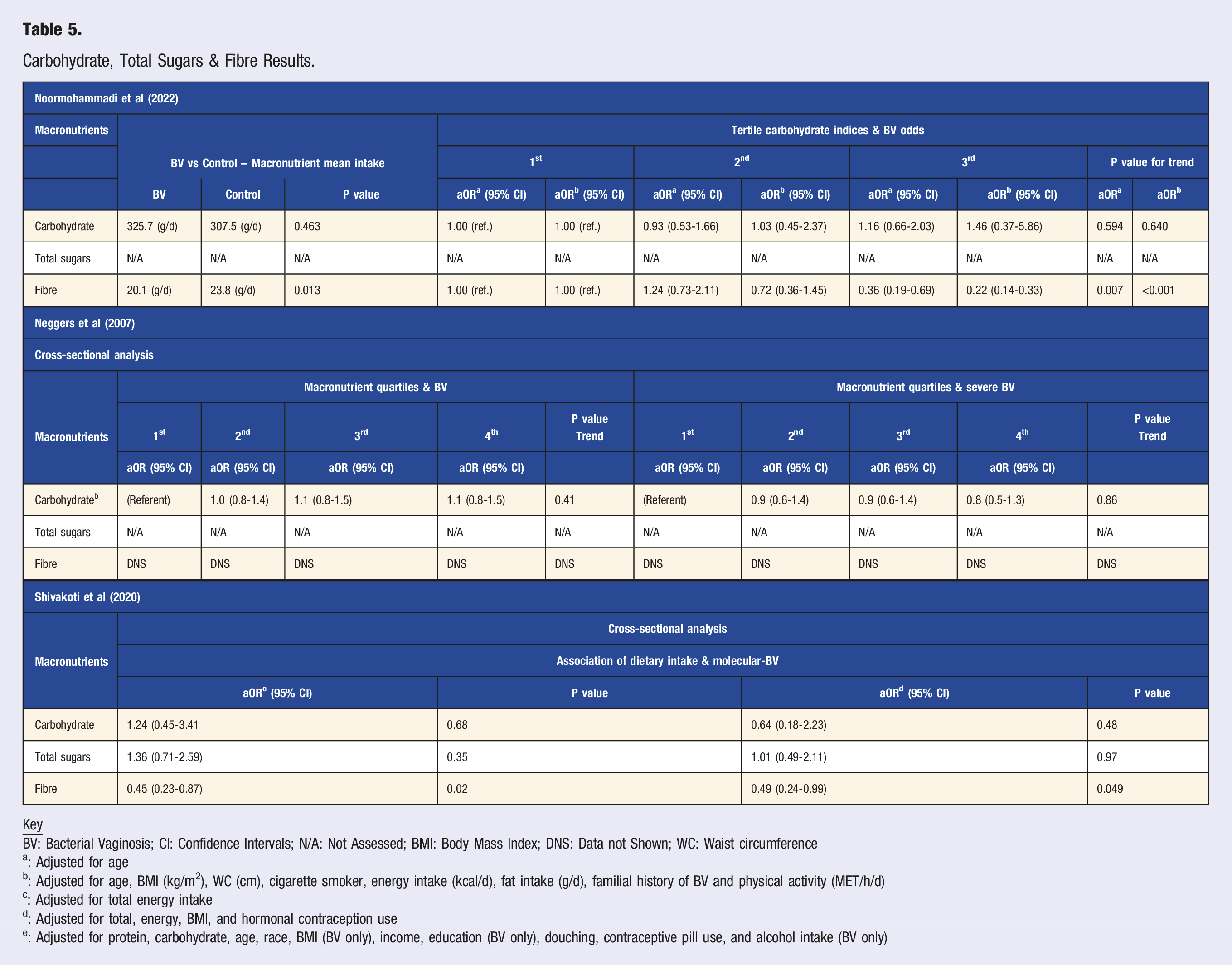
a: Adjusted for age
b: Adjusted for age, BMI (kg/m2), WC (cm), cigarette smoker, energy intake (kcal/d), fat intake (g/d), familial history of BV and physical activity (MET/h/d)
c: Adjusted for total energy intake
d: Adjusted for total, energy, BMI, and hormonal contraception use
e: Adjusted for protein, carbohydrate, age, race, BMI (BV only), income, education (BV only), douching, contraceptive pill use, and alcohol intake (BV only)
GI & GL
Noormohammadi et al. 34 compared the mean intake of GI and GL between BV cases and controls, the only statistically significant result was that BV cases were associated with a higher GI diet (P < 0.001). Carbohydrate tertile indices and their association with BV odds were also evaluated, and results adjusting for energy intake showed a significant association with BV in the higher GI tertile compared to lower (adjusted Odds Ratio (aOR) 2.95, Confidence Interval (CI) (1.59-5.46), P = 0.001) and after adjusting for other factors the results remained statistically significant (aOR 2.99, CI 1.47-6.08, P = 0.003). GL after adjusting for other factors was also statistically significant in the higher tertile (aOR 4.01, CI 1.22-5.92, P = 0.029).
Thoma et al. 35 in the cross-sectional analysis compared the odds of intermediate or BV flora to normal flora per 10-unit increase in GI and GL. For the crude results, although P-values were not reported, higher GL was positively associated with BV compared to normal flora (crudes Odds Ratio (cOR 1.02, CI 1.01-1.03. P≈<0.001). This approximation was calculated using the CI 1.01-1.03 and cOR 1.02 and the P-value calculation formula. 38 For adjusted results, higher GL was also positively associated with BV compared to normal flora (aOR 1.01, CI 1.00-1.03, P = 0.037).
In the prospective analysis the association between GI and GL with BV progression, persistence and resolution over time was examined. For crude results the P values were not reported, and GI results were not statistically significant; however, higher GL was positively associated with BV progression (cOR 1.03, CI 1.01-1.05, P≈0.0028) as well as persistence (cOR 1.02, CI 1.01-1.04, P≈0.008). For adjusted results, GI results were not statistically significant, however, for higher GL there was a positive association with BV progression (aOR 1.03, CI 1.00-1.05, P≈0.018) and persistence (aOR 1.02, CI 1.01-1.04, P≈0.008). All approximate P-values in the prospective analysis were calculated using the same formula. 38 The results from Shivakoti et al. 36 had no statistical significance.
Carbohydrate, Total Sugars and Fibre
Noormohammadi et al. 34 compared the mean intake of carbohydrate and fibre intake in BV cases vs controls. Statistical significance was associated with a higher fibre intake in controls (P = 0.013). After adjusting for energy intake, the analysis of carbohydrate tertiles and BV odds revealed a statistically significant association, with lower odds of BV observed in the highest fibre tertile (aOR 0.36, CI 0.19-0.69, P = 0.007) and still after further adjustments (aOR 0.22, CI 0.14-0.33, P=<0.001). No other results were statistically significant.
Shivakoti et al. 36 examined carbohydrate, total sugars, and fibre intake with BV odds. In results adjusted for energy intake, a higher total fibre intake was inversely (aOR 0.45, CI 0.23-0.87, P = 0.02) associated with BV. For further adjustments a higher total fibre intake was still inversely associated (aOR 0.49, CI 0.24-0.99, P = 0.049). No other results were statistically significant.
Neggers et al. 37 looked at BV in relation to carbohydrate and fibre trends. The carbohydrate results were not statistically significant, and the fibre results were not reported.
Risk of Bias
The quality of the studies was varied. Thoma et al. 35 and Neggers et al. 37 were found to have a high risk of bias and Shivakoti et al. 36 was found to have some concerns using the AXIS tool (Supplement 4). For Noormohammadi et al., 34 only a quality assessment was completed using the CASP tool (Supplement 5).
The studies did not justify their sample size nor was it clear how participants were selected, even though the sample was from an appropriate population, potentially causing selection bias. 39
All the cross-sectional studies35-37 had concerns with reporting their data; basic data often was not presented or only briefly mentioned potentially leading to missing data bias 40 ; only Shivakoti et al. 36 presented all the data that was analysed and performed a sensitivity analysis.
Discussion
This review aimed to identify whether there is an association between dietary carbohydrate and BV. Overall, the results suggest that a higher GL diet may be positively associated with BV and a diet high in fibre may have an inverse effect on BV.
Noormohammadi et al. 34 found that the higher tertile of GL intake was positively associated with BV odds in adjusted results and Thoma et al. 35 supported this as participants with BV (odds, progression, persistence) were positively associated with a higher GL diet (Table 4). However, Shivakoti et al. 36 did not find this association, but the evidence could suggest an association between GL and BV.
There are two difference types of dietary carbohydrate: digestible and non-digestible. Digestible carbohydrate are comprised of starches and sugars, such glucose, fructose, sucrose, and lactose. 21 The amount and type of carbohydrate in a meal can influence someone’s glycaemic response. 41 The GL score indicates how fast glucose enters the bloodstream of a particular food as well as how much glucose per serving is supplied; it gives a more accurate picture of how the dietary carbohydrate impacts blood sugar levels. 42 When glucose stimulates insulin release, it has been found to potentially cause oxidative damage leading to increased inflammation, due to continuous exposure to hyperglycaemia.43-45 As the inflammation can affect the gut microbiota 46 ; it is possible that constant exposure to high-GL foods affects bacterial colonisation in the vagina due to impaired immune response.24,25 Additionally, studies have found that digesting high levels of glucose, fructose, and sucrose increased the abundance of Bifidobacteria, and decreased Bacteroides in the gut, possibly altering both microbiomes.47,48 However, these are theories and do not directly justify the association.
Noormohammadi et al. 34 found a higher fibre intake in controls than in BV cases (Table 5). In the carbohydrate tertile analysis, lower BV odds were associated with high fibre intake for both adjusted models (Table 5). Shivakoti et al. 36 supports this as the cross-sectional analysis found an inverse association between fibre intake and BV odds in both adjusted models (Table 5). Neggers et al. 37 assessed fibre but did not report the results.
This association may also be related to the gut and vaginal microbiota. Fibre is the non-digestible type of dietary carbohydrate, which is metabolised by specific species of gut microbiota via anaerobic fermentation. 49 Dietary fibre has a vital effect on the diversity and composition of the microbiome, providing fermentation opportunities. 49 It has been found to modulate the gut towards a healthier composition,49-51 which may, in turn, affect bacterial colonisation in the vagina towards a Lactobacillus-dominated composition via the rectum.
Consuming higher amounts of dietary fibre has the potential to alter the nutritional function of the intestine which promotes the growth of beneficial gut bacteria. 52 Noormohammadi et al. 34 found that women with BV had an average intake of 20.1 g/day and the control had 23.8 g/day, a difference of 3.7 g/day, while Shivakoti et al. 36 found the median intake of fibre was 9.6 g/day per 1000 kcal/day. The recommended fibre intake for an adult in the UK is 30 g/day, 53 and currently adults in the UK between 19 to 64 years have a mean intake of 19.7 g a day. 54
Confounding factors should also be considered. 55 Hormonal contraception (HC) can influence BV occurrence, as both progesterone and oestrogen can cause different mechanisms that can increase the posibilities of vaginal dysbiosis. 56 Therefore, it is important that HC was adjusted for as it could affect the outcome of the results. Shivakoti et al, 36 Neggers et al 37 and Thoma et al. 35 adjusted for HC, however, Noormohammadi et al. 34 did not, resulting in possible errors in outcome measurements.
Strengths and Limitations
A strength of this review is that it sought to investigate the association between dietary carbohydrate intake and BV which is a topic that has received little attention in the field of women’s health. It also highlights the need for further research concerning women’s health and the influence of dietary intake on women’s sexual health. The review utilised a comprehensive database search with clear inclusion criteria (Table 1) to ensure relevant studies were identified. To enhance its transparency, the CRD 57 guidance for reporting methodology was used as well as the PRISMA 2020 28 checklist.
Limitations of the review included limiting the search to studies reported in English causing language bias. 58 Furthermore, a limited number of studies were found which hindered interpretation, synthesis and analyses of the results. Only one reviewer screened records and collected data putting the review at risk of selection bias. 39
Conclusion and Future Research Recommendations
The results suggest that a higher GL diet may have a positive association with BV incidence, there is an inverse association with BV and a diet higher in fibre. However, the included studies were of moderate to poor quality, so even though the results are interesting they need to be interpreted with caution.
Based on the results of the present review, specific dietary recommendations cannot be made. However, as discussed, the gut microbiome composition is significantly affected by dietary changes, and potentially the vaginal microbiome. Specifically, some studies21-23 show that dietary fibre has a positive effect on the gut microbiome, and Noormohammadi et al. 34 found that the control group had a 3-4 g/day higher fibre intake than the BV group. Therefore, women should be advised to monitor their dietary carbohydrate intake specifically focusing on dietary fibre and aiming to achieve current dietary recommendations.
Dietary modifications may have therapeutic benefits for patients with re-occurring BV. Given the sparse research into dietary intake and its relation to women’s gynaecological health, future research is recommended.
Supplemental Material
Supplemental material - Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review
Supplemental material for Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review by Marie-Hannah Baliakas and Robert Davies in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental material - Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review
Supplemental material for Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review by Marie-Hannah Baliakas and Robert Davies in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental material - Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review
Supplemental material for Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review by Marie-Hannah Baliakas and Robert Davies in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental material - Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review
Supplemental material for Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review by Marie-Hannah Baliakas and Robert Davies in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental material - Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review
Supplemental material for Carbohydrate Intake and Bacterial Vaginosis: A Systematic Review by Marie-Hannah Baliakas and Robert Davies in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
Conceptualisation: Marie-Hannah Baliakas, Robert Davies; Methodology: Marie-Hannah Baliakas, Robert Davies; Formal analysis and investigation: Marie-Hannah Baliakas; Writing - original draft preparation: Marie-Hannah Baliakas; Writing - review and editing: Marie-Hannah Baliakas, Robert Davies; Supervision: Robert Davies.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that all data generated or analysed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.