
Abstract
Objective
Recurrent bacterial vaginosis (RBV) after antibiotic treatment has relapse rates of 35% within 3 months and 60% within 12 months. A medical device containing polycarbophil, lauryl glucoside, and glycerides (PLGG) inhibits bacterial growth and has mucoadhesive properties. This study examined the efficacy of the device in women with RBV.
Methods
This post-market clinical follow-up study comprised two phases. The first phase was an interventional, open-label, non-controlled, multicenter study enrolling 56 women. The second phase was an observational 10-month follow-up without treatment.
Results
After three cycles of PLGG treatment, recurrence was identified in 8 of 54 evaluable patients (14.81%). A positive effect on lactobacilli in the vaginal secretions was observed in 26 of 39 patients (66.67%). Among 35 patients observed after stopping PLGG treatment, one case of RBV (2.86%) was observed after 4 months, and an additional six cases (17.14%) were observed after 10 ± 2 months. Therefore, no recurrence was evidenced in 12 subjects (34.28%) at the end of the study.
Conclusion
The use of PLGG vaginal ovules in the treatment of BV reduces the rate of recurrence and apparently produces a positive effect on the vaginal microbiota.
Introduction
The vaginal microbiome, characterized by the dominance of Lactobacillus species, can change its composition under the influence of a range of exogenous and endogenous factors, increase vaginal pH, and produce unfavorable conditions for the survival of lactobacilli. Then, the altered vaginal ecosystem permits the replacement of lactobacilli with anaerobic bacteria such as Gardnerella vaginalis (GV), Atopobium vaginae (recently reclassified as Fannyhessea vaginae), 1 Ureaplasma urealyticum, and Mycoplasma hominis. 2 Disruption of the normal vaginal microbiota produces dysbiosis, such as bacterial vaginosis (BV), which is the most common cause of abnormal vaginal discharge during childbearing age, representing 16% to 30% of all cases. 3 Moreover, BV has been linked to serious conditions, including pelvic inflammatory diseases, postoperative infections, the acquisition and transmission of human immunodeficiency virus (HIV), preterm birth, 4 and several adverse pregnancy outcomes. Even if 50% of women have no symptoms, the most reported complaints are abnormal watery, gray vaginal discharge, and fishy odor. The diagnosis is generally based on the presence of three of four Amsel criteria (high vaginal pH, abnormal gray discharge, positive amine test, and presence of clue cells on wet mount microscopy), which has a sensitivity of 92%. 5 The etiology and pathogenesis of BV are not completely understood because several risk factors have a determining role. Thus, the available treatments are not yet always effective, resulting in a high recurrence rate. 6 Recurrent bacterial vaginosis (RBV) is defined as two or three episodes of BV per year.7,8 RBV and abnormal vaginal microbiota can be associated with a history of BV, a regular sex partner, and female sex partners. The use of hormonal contraception has a negative association with recurrence. Reported recurrence rates reach 35% within 3 months, 9 50% within 6 months, 8 and 60% within 12 months. 9 It was proven that the tendency to relapse is essentially linked to the ability of GV (and to a lesser extent of A. vaginae) to strongly adhere to mucous membranes, producing a long-lasting biofilm.10,11
Metronidazole (systemic or topical), tinidazole (systemic), and clindamycin (systemic or topical) are equally suggested as first-line treatments. 12 Although standard antibiotic regimens can decrease the load of pathogens, it was demonstrated that bacterial biofilm can persist on the vaginal epithelium, thus facilitating recurrence after treatment. For this reason, it is suggested by several studies 10 that the use of products that can create a barrier effect against bacterial biofilm formation and permanence could be useful for preventing recurrence. These elements (i.e., lysozyme, thymol, bromelain, and polycarbophil) are widely used in daily practice by thousands of gynecologists in Europe with the caveat to administer them no later than 24 hours after antibiotic treatment. We performed a systematic review of the literature on products that can create a barrier effect against bacterial biofilm formation, finding that they can improve the efficacy of BV treatment. Unfortunately, there are little data supporting a decrease in the recurrence rate with their administration after antibiotic therapy.
This study reports the results of the POLARIS (Polybactum® to assess Recurrent Bacterial Vaginosis) study, which evaluated the ability of a medical device containing polycarbophil, lauryl glucoside, and glycerides (PLGG) to reduce BV recurrence during follow-up after one course of antibiotic therapy. The tested product (Polybactum®, Effik Italia S.p.a., Cinisello Balsamo, Milan, Italy) is already marketed as a Class IIa medical device in several European countries. The rationale for using the vaginal mucoadhesive PLGG as the product in this study relates to its ability to act as a mechanical barrier against colonization by pathogens. In fact, PLGG has three key actions: i) it exhibits selective bacteriostatic activity against GV while sparing the normal vaginal microbiota, i.e., lactobacilli; ii) it does not increase vaginal pH, thus improving the microbiological parameters and maintaining a hostile environment for the recolonization of the vagina by the polymicrobial microbiota involved in BV; and iii) the marketed formulation of PLGG also contains lauryl glucoside (LG), a nonionic surfactant with tensioactive properties that can enhance the barrier effect by reducing surface tension. 13 PLGG exerts no systemic effect because of its inability to cross the epithelium, and it has good local tolerance even after prolonged exposure. Additionally, it does not cause any irritation of the vaginal wall, it has no toxic effect on epithelial cells, and it does not trigger sensitivity reactions. 14
Materials and methods
Study design
The POLARIS study protocol was described in a recent publication. 15 It was planned with an open-label, non-controlled design in Italy and Romania. In the first phase, each patient completed three cycles of treatment with PLGG after signing the informed consent form, followed by 1 month of no treatment. In the second phase, follow-up without treatment continued for an additional 9 months only in the three Romanian centers (www.clinicaltrials.gov as NCT02863536). Therefore, each patient could undergo 10 months of follow-up without treatment: 30 days from the end of the third cycle of PLGG to day 78 ± 6 and 9 ± 2 months from that date to the final visit. In the follow-up period, only subjects who completed the first phase and voluntarily consented to participate in the observational part of the study were included. To minimize the loss to follow-up, the personnel of each site was carefully trained regarding communication with the patients and the implementation of different strategies during the study period, i.e., kind reminders by phone 2 days before each scheduled visit, collection of information from relatives, and refund for travel to people living away from the sites. In addition, if a patient missed a scheduled visit, the site staff was instructed to call her promptly at different hours of the day, leaving voice messages and inviting her to the site.
The study received formal approval from the National Agency for Medicines and Medical Devices of Romania (Agentia Nationala a Medicamentului si a Dispozitivelor Medicale) and was notified to the Italian Ministry of Health. The local Ethics Committees (ECs) of the investigational sites approved the study in Romania (EC Clinica Medicală Dr. Crișan, 29 July 2016; EC Clinica Medicală Dr. Biriș, 24 October 2016; and EC Clinica Medicală Dr. Sîrbu, 22 August 2016) and Italy (EC Area 1 in Milan, 14 December 2016 [#8643/2017]; EC Lazio 1 in Rome, 15 February 2017 [#566/2017]). The study was amended (on 14 March 2018) to allow for 10 months of follow-up without treatment and to include an interim analysis at 6 months of enrollment, the results of which have been published. 16 All patient details were de-identified. The reporting of this study conforms to the STROBE guidelines. 17 Following the new European Union Medical Device Regulation, this trial is defined as a post-marketing clinical follow-up study.
Participants
Women older than 18 years with RBV were consecutively included in the interventional first phase of the study. The diagnosis of BV was based on the Amsel criteria, which were assessed 6 to 9 days before baseline. The Amsel criteria as originally reported 18 include the presence of clue cells on wet mount microscopy as one of the four criteria for diagnosing BV. FDA guidelines 19 require the presence of clue cells and that they comprise more than 20% of all epithelial cells. The latter was used as a criterion by the five centers involved in the study, and it was therefore reported in the study protocol even though it can underestimate RBV cases. Antibiotic therapy consisted of vaginal metronidazole (5 g of 0.75% gel once daily for 5 days or 500-mg ovules once daily for 7 days). The inclusion criteria were RBV (at least two episodes of BV in the previous 12 months, including the episode treated before baseline), age of ≥18 years, a signed informed consent form (ICF), and no lactation or no amenorrhea in lactating women. The exclusion criteria were as follows: known allergy to metronidazole or the tested PLGG ingredients, pregnancy, candidiasis or mixed vaginitis, HIV or other immunodeficiencies; sex work; ongoing menstrual bleeding or premenopause/menopause, current clinical trial participation or participation in the previous month, unwillingness to sign the ICF; and >16 or ≤ 5 days between the last day of the last menses and the baseline visit. This last criterion was necessary to avoid bias in case menstrual bleeding occurred during the first PLGG cycle and led to an interruption of its administration.
Patients who completed the interventional phase of the study without any recurrence were eligible to participate in the observational follow-up, thus having a total of 10 months without any treatment.
Two participating sites were located in Italy (coordinator site Vittore Buzzi Hospital in Milan and AIED Centre in Rome), and three sites were Romanian private clinics specialized in gynecology (Clinica Medicală Dr. Crișan, Clinica Medicală Biriș, and Clinica Medicală Dr. Sîrbu). Following the indications recently reported in the clinical research literature, 20 the trial was performed as a partnership between an academic research organization (Department of Clinical Trials of the University of Medicine and Pharmacy Victor Babeș in Timisoara, Romania) and an independent international contract research organization (Opera CRO, a Tigermed Group company, Timișoara, Romania). In this model, the Department of Clinical Trials was the direct contact with the investigator coordinator of the study at Vittore Buzzi Hospital in Milan and was involved in the selection and training of Investigators and co-investigators of the sites. The Department of Clinical Trials also assured the correct application of ethics requirements and shared scientific information throughout the study period. Meanwhile, the CRO provided the infrastructure for efficient trial execution, site monitoring, data management, and statistical analysis. The model assigning the scientific activity to the investigators linked to the Department of Clinical Trials and management responsibility to the CRO could also clear the charge of the sponsor. In fact, the role of the sponsor was only to offer the tested medical devices and a partial grant as support to the trial without any potential misunderstanding related to influence or potential persuasion in the study design, data collection, interpretation, or sharing for publication.
For administrative reasons, the centers in Italy could only participate in the first interventional phase of the study, and thus, the patients enrolled at the two Italian sites were not included in the follow-up period.
The trial was conducted from 8 September 2016 (first visit of the first patient) to 18 October 2018 (last visit of the last patient).
Interventions
Before any procedure related to the study, each patient was informed about the purpose of the trial, the risks, and the benefits and was requested to consent by signing the ICF. An additional detailed ICF was signed by the patients at the beginning of the follow-up period. The administration of PLGG vaginal ovules started within 12 and 24 hours after the end of metronidazole vaginal treatment and continued for three menstrual periods (72–84 days). The duration of each cycle of treatment was 1 week, with one ovule each inserted into the vagina on days 1, 4, and 7. At the baseline visit, the investigator delivered nine ovules to each patient for the whole study duration (three ovules for three cycles). This dose was the same as that indicated on the instructions for use of PLGG on the market and given by gynecologists in their clinical practice. The investigator also advised the patient to lay in a supine position for a couple of minutes after the ovule was inserted. The baseline visit and the first cycle of PLGG vaginal ovule fell within 6 and 16 days after menstrual bleeding and after the end of metronidazole treatment. In the second and third cycles, PLGG vaginal ovules were administered immediately after the end of the previous menstrual bleeding. In any case, the investigator could decide to stop administering the medical device for safety purposes or to prescribe other therapies if considered necessary for the patient’s health. The following treatments were not allowed: other products or medications to treat BV, etonogestrel/ethinyl estradiol vaginal ring (e.g., Nuvaring®, Merck & Co., Inc, Rahway, NJ, USA) or intrauterine devices, vaginal tampons, oral or vaginal antibiotic treatments or other vaginal therapies (such as spermicide), and vaginal or oral probiotics (e.g., vaginal lactobacilli).
Primary and secondary outcomes
The study included a baseline visit (day 0), a visit after 30 days after stopping PLGG treatment (day 78 ± 6), and a visit at the end of the follow-up period (month 10 ± 2 ). Three phone calls with the patient were planned during the interventional phase of the study: 28 ± 1 days after the last day of the last menses, 28 ± 1 days after the first phone call, and 28 ± 1 days after the second phone call. Two additional phone calls were requested at months 4 and 7 during the follow-up period. During any phone call, the investigator checked if the patient had BV symptoms and, if so, scheduled an unplanned visit to confirm the diagnosis of BV based on the Amsel criteria.
The primary outcome was the recurrence of BV identified by the Amsel criteria, 18 as determined in planned (baseline, day 78 ± 6 and month 10 ± 2) or unscheduled visits. A positive diagnosis of BV required three of the following four criteria: vaginal pH greater than pH 4.5; clue cells comprising ≥20% of all epithelial cells in the vaginal fluid; presence of white and thin vaginal discharge, and fishy odor in the whiff test. The vaginal microbiota was measured as a secondary outcome at baseline, on day 78 ± 6, and in month 10 ± 2. The assessment was quantitative and scored on a four-point scale from the lowest to the highest concentrations as follows: absent, 1+, 2+, 3+, and 4+. Healthy microbiota should have lactobacillary grade I (numerous pleiomorphic lactobacilli, no other bacteria) or IIa (mixed flora, but predominantly lactobacilli). 21 The remaining secondary outcomes (signs and symptoms of BV: vaginal discharge, erythema, burning, dyspareunia) were measured at baseline and at 30 days after stopping PLGG treatment (day 78 ± 6). Vaginal discharge over the last 24 hours was measured using an analogic three-point scale as follows: 0 = not present or physiological in quantity, color, and type; 1 = mild abnormal (abnormal quantity with normal color and type); and 2 = abnormal quantity, color, and type. Erythema was evaluated using an analogic five-point scale as follows: 0 = no symptoms; 1= slight; 2 = moderate; 3 = marked; and 4 = very marked. Burning intensity over the last 24 hours was assessed using an analogic five-point scale as follows: 0 = not present; 1 = mild; 2 = moderate; 3 = severe; and 4 = unbearable. Dyspareunia was evaluated by a dichotomic scale (0 = absent, 1 = present). The secondary outcomes also included the patient’s assessment of the global efficacy of treatment at the last visit using a four-point scale as follows: 1 = very good improvement; 2 = good improvement; 3 = moderate improvement; and 4 = negligible improvement.
Safety was evaluated by collecting and evaluating the adverse events that occurred during the whole study period and by a global assessment of safety performed by Investigators using an analogic four-point scale (1 = excellent, 2 = good, 3 = fair, 4 = poor).
Sample size determination and statistical methods
According to published data, it was considered that the mean recurrence rate of BV after a first episode ranged 30% to 50% within 3 months after appropriate antibiotic therapy.10 Patients were not allowed to use any oral or vaginal antibiotic therapy after metronidazole treatment during the three cycles of PLGG treatment (approximately 3 months). Thus, a mean recurrence rate of 40% was realistic in this study. In addition, data previously collected on recurrence rates post-treatment with PLGG vaginal ovules (Effik Italia SpA, unpublished data) evidenced a 2% correlation between paired observation and after applying continuity correction. Thus, the study would have required a sample size of 44 pairs to achieve a power of 80% and a one-sided significance of 5% for detecting a difference of 0.25 between marginal proportions. We expected a potential dropout rate of 20%, and thus, we aimed to enroll 55 patients (one-group chi-square test). At the 95% confidence interval, the level of significance was <0.05.
The data between visits for the primary objective were analyzed by a t-test or chi-square test for quantitative variables. For binary and qualitative variables, McNemar’s test and a symmetry test, respectively, were applied. The time to event for BV recurrence was analyzed using Kaplan–Meier curves. All tests were two-sided, and the nominal level of α was 5%. P-values were not adjusted for multiplicity for the primary outcome. For secondary objectives, statistical tests included, but were not limited to, the chi-square test and McNemar’s test for categorical data and a linear mixed effects model analysis. If a subject was missing information for one or more variables, the missing data were not replaced even after resolution of the related queries. If a subject violated the inclusion/exclusion criteria, the respective data were excluded from the analysis. Statistical analysis was performed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Patient disposition
Fifty-six patients were enrolled in the interventional phase of the study. Two patients were excluded from the analysis because they did not complete all PLGG vaginal ovule administration cycles (dropout not related to safety issues), and 54 patients were considered evaluable. Because of administrative reasons, the patients belonging to the Italian centers were not included in the follow-up period, and therefore, only 35 patients were considered evaluable in this second phase of the study. The study flow chart is presented in Figure 1.

Flow diagram of the POLARIS study.
Demography and baseline data
No relevant findings were recorded in patients’ medical history or during the physical examination. The baseline demographic data of patients and the number of episodes of BV in the 12 months before enrollment are reported in Table 1. No enrolled patient was considered a smoker (≥5 cigarettes/day) or abuser of alcohol or drugs. As required by the exclusion criteria, no woman was a sex worker. All patients received standardized guidelines for intimate hygiene (e.g., avoid douching) at baseline. No relevant concomitant medication was recorded during the screening evaluation or during the study period.
Demographics of the treated population.
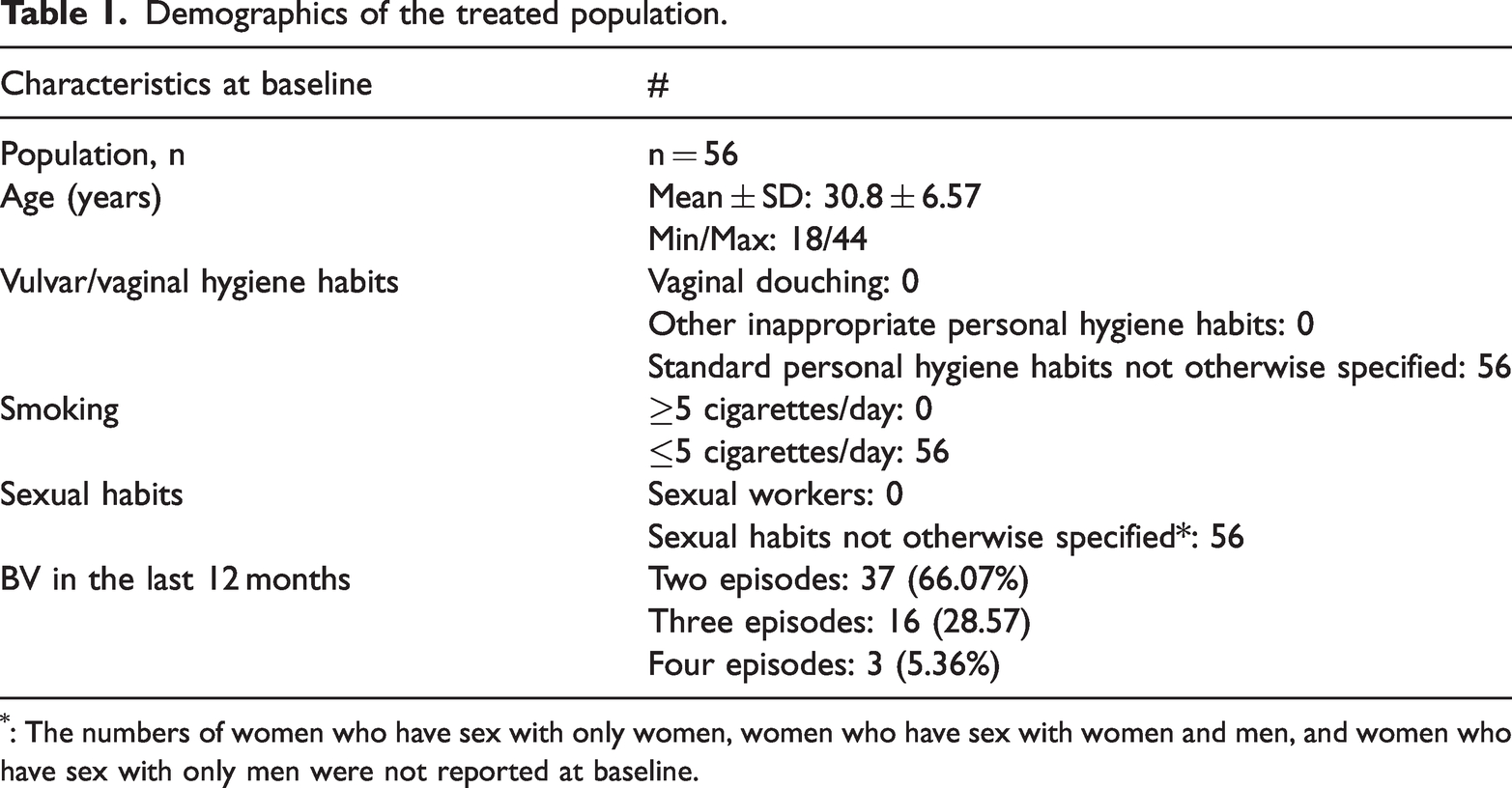
: The numbers of women who have sex with only women, women who have sex with women and men, and women who have sex with only men were not reported at baseline.
Primary efficacy outcome
According to the analysis of the primary objective, a recurrence was noted in 8 of 54 evaluable patients (14.81%) at the visit on day 78 ± 6. These results represented a significant decrease with respect to the rate of 40% reported in the literature and confirmed the results of the interim analysis. 16 Thus, the 3-month BV recurrence rate of 14.81% must be related to treatment with PLGG vaginal ovules for 2 months plus 1 month without any treatment.
Among the 35 patients who completed the interventional phase of the study without recurrence and continued the follow-up period without treatment, only one patient (2.86%) had RBV after 4 months. This rate was maintained for 6 months when six additional cases (17.14%) were evidenced at the final visit (10 ± 2 months). Therefore, considering the 16 patients who withdrew (45.71%), no recurrence rate was detected in 12 subjects (34.28%) at 10 ± 2 months after the discontinuation of PLGG treatment. These data confirm and demonstrate the effectiveness of PLGG vaginal ovules in reducing the rate of relapses in the long term.
Kaplan–Meier analysis highlighted the reduction in the percentage of patients without RBV over time, and Figure 2 presents a comparison of the recurrence rate of BV for each visit. The treatment compliance rate (defined as the total number of administered ovules divided by the total number of given ovules in the interventional study) was 97.82% (493 of 504 ovules) for all enrolled patients, and the rate was 100% (486 of 486 ovules) among subjects who completed the study.

Bacterial vaginosis recurrence rate changes between visits after stopping PLGG treatment.
Secondary efficacy outcomes
The data for evaluating lactobacilli present in vaginal secretions were collected only in the Romanian sites during the interventional phase of the study (from baseline to day 78 ± 6) because of logistical reasons. Among 39 patients, the evidence indicated a beneficial or neutral effect of the treatment on lactobacillus counts in 26 patients (66.67%), whereas their counts increased in 13 patients (33.33%; chi-square test, P = 0.054). Comparing lactobacillus counts between baseline and the final visit of the interventional study, significant differences were observed between visits (Stuart–Maxwell asymptotic marginal homogeneity test, P = 0.011). The effect of the treatment on lactobacillus counts between baseline and the visit at day 78 ± 6 is graphically presented in Figure 3a.

(a) The change in the lactobacillus count in the interventional phase of the study from baseline to day 78 ± 6 days and (b) The change in the lactobacillus count after stopping PLGG treatment from day 78 ± 6 to month 10 ± 2. PLGG, polycarbophil, lauryl glucoside, and glycerides.
Data were also collected for 17 subjects who completed follow-up and attended the final visit in month 10 ± 2 (Figure 3b). There were no statistically significant differences in lactobacillus count changes between visits (Maxwell–Stuart asymptotic homogeneity test, P = 0.306).
The lactobacillus count at different visits (baseline, day 78 ± 6, and month 10 ± 2) is reported in Figure 4.

Lactobacillus count at baseline, on day 78 ± 6, and in month 10 ± 2 (data from 17 subjects who completed the final visit at 10 ± 2 months). The quantitative assessment was scored as follows: +1 or +2 (normal), numerous pleiomorphic lactobacilli, no other bacteria or clue cells or hyphae, lactobacillary grade I or IIa; +3 (partially impaired), population of lactobacilli severely decreased, lactobacillary grade IIb; +4 (pathological), lactobacilli severely depressed or absent because of overgrowth of other bacteria, clue cells (>20%), or hyphae, lactobacillary grade III 21 .
Results related to symptoms associated with BV (vaginal discharge, burning, erythema, and dyspareunia) in the first phase of the study are reported in Figure 5. The patients’ global assessment of efficacy on day 78 ± 6 was very good, good, moderate, and negligible for 74.07%, 12.96%, 7.41%, and 5.56% of patients, respectively.

Vaginal discharge, burning, erythema, and dyspareunia from baseline to day 78 ± 6.
Safety outcomes
In the investigators' global assessment, safety was rated as excellent, good, and fair by 83.64%, 10.91%, and 5.45% of investigators, respectively, on day 78 ± 6 . Only two adverse events were reported in the first interventional phase of the study, and no adverse events were evidenced during the follow-up period without treatment. The two adverse events (mild local itching and mild viral respiratory infection) were considered unrelated to the tested medical device, proving its safety. Patients recovered from symptoms after a few days, and in both cases, the investigator eliminated the possibility of BV recurrence.
Discussion
BV treatment is usually effective, as evidenced by a reported cure rate of 80% to 90% at 1 month, although a recurrence rate of 35% at 3 months is also reported. 9 Additionally, a BV recurrence rate of up to 60% has been evidenced within 12 months. 9 Therefore, it is necessary for the scientific community to explore alternative methods of BV treatment because the current approach is unsatisfactory for preventing recurrence.
This is the first study to evaluate the clinical efficacy of PLGG vaginal ovules in the treatment of RBV. A large proportion of women (34.28%) clinically cured after metronidazole vaginal treatment, confirming the results of the interim analysis, 16 and three cycles of PLGG had no relapse of BV during 10 months of follow-up without treatment. A wide range of factors, including sexual habits, smoking, and personal hygiene habits can increase vaginal pH, making conditions unfavorable for lactobacilli and allowing the growth of predominantly anaerobic bacteria such as GV, resulting in BV.22,23 GV plays a central pathogenetic role in BV. Some GV strains can produce a biofilm together with other bacteria, thereby protecting against lactic acid and hydrogen peroxide, and this phenomenon can lead to BV recurrence. Biofilm is a structured community of microorganisms in a self-produced extracellular matrix that is adherent to the surface of epithelial cells.22,23 Biofilm deficiencies represent an important factor in the pathogenesis of BV, and they are not well managed by existing therapies. In addition, it is reported that GV secretes the enzyme sialidase, which degrades sialoglycoproteins in the mucus layer, releasing sialic acid, which is further degraded by aldolases and lyases expressed by bacteria. 24 This hydrolytic activity leads to degradation of the mucus, resulting in biofilm formation and inflammation. This situation can lead to inadequate treatment and can represent a potential determinant of recurrence.
The components of PLGG (polycarbophil, lauryl glucoside, glycerides) can have synergistic effects. Indeed, lauryl glucoside exerts a peculiar bacteriostatic action that can inhibit GV growth. It was proven that GV growth is reduced by contact with PLGG for 48 hours. 13 Meanwhile, polycarbophil, a nontoxic agent, acts as a mechanical barrier against colonization by pathogens and lauryl glucoside, a non-ionic surfactant, reinforces the effect of polycarbophil by reducing surface tension. 13 We hypothesized that the combination of these elements is critical for the peculiar mucoadhesive property of the product, allowing it to impair the formation of biofilm by pathogenic bacteria. BV can recur because of inadequate restoration of a lactobacillus-dominant vaginal microbiota or because of ineffective treatment.
The study demonstrated that the use of PLGG vaginal ovules in the treatment of BV reduces the recurrence rate. In prior studies, recurrence rates of 35% and 60% 9 were reported at 3 and 12 months, respectively, reinforcing our results of recurrence rates of 15% and 50% at 3 and 10 months, respectively.
In addition, treatment with three cycles of PLGG vaginal ovules, although limited by the small sample analyzed (35 patients), appears to induce considerable stability in the vaginal lactobacillus microbiota even during the follow-up period without treatment. The absence of an untreated control group is the main limitation and weakness of this study. To avoid this potential bias, the untreated control group could have comprised patients treated with antibiotics for the last recurrence prior to the baseline visit who did not subsequently receive PLGG vaginal ovules. However, we did not apply this strategy because, in our opinion, it would be unethical to enroll patients with a history of two or more episodes of RBV (as required by the study inclusion criteria) as a control group. An alternative strategy could be to give the control group a maintenance prophylactic antibiotic regimen for 4 to 6 months after antibiotic treatment for the last recurrence prior to baseline. In fact, twice-weekly vaginal metronidazole gel 0.75% has proven effective in preventing recurrence in approximately 70% of women with RBV. 25 Unfortunately, this approach would likely be rejected by the majority of women enrolled (especially in the Romanian sites), which could have affected recruitment rates. We believe that a control group could be successfully used in a future trial comparing two different treatments for the prevention of RBV. Obviously, this trial should have an adequate sample size exceeding that in our study.
It should be noted that the Amsel criteria list the presence of clue cells on wet mount microscopy as one of the four criteria instead of clue cells comprising ≥20% of all epithelial cells in the vaginal fluid (as reported in our study and in the FDA guidelines). 19 The use of this criterion might have led to underestimation of RBV cases.
Sexual habits are often a factor in BV recurrence, but unfortunately, we did not record the number of women who have sex with only women, women who have sex with women and men, and women who have sex with only men at baseline.
An additional limitation of the study was that the positive effect on the lactobacillus count was based on only 17 subjects (of 35) who completed the follow-up and attended the final visit at 10 ± 2 months.
Conclusions
This study supports the use of a specific vaginal product marketed as a medical device, which displayed a peculiar ability to create and maintain a protective vaginal barrier that inhibits the onset and recurrence of BV. The study demonstrated that the short-term performance of PLGG can persist for up to 10 months after treatment. Moreover, an optimal safety and tolerability profile was observed for PLGG well.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241239021 - Supplemental material for POLARIS: efficacy and safety of a vaginal medical device in recurrent bacterial vaginosis—a multicenter, open-label, non-controlled, study with 10 months of follow-up
Supplemental material, sj-pdf-1-imr-10.1177_03000605241239021 for POLARIS: efficacy and safety of a vaginal medical device in recurrent bacterial vaginosis—a multicenter, open-label, non-controlled, study with 10 months of follow-up by Filippo Murina, Paolo Inghirami, Marius Biriș, Daniela Sîrbu, Dionisio Franco Barattini, Luca Ivan Ardolino, Mario Mangrella, Elena Casolati, Serban Marius Roșu and Ciprian Crișan in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241239021 - Supplemental material for POLARIS: efficacy and safety of a vaginal medical device in recurrent bacterial vaginosis—a multicenter, open-label, non-controlled, study with 10 months of follow-up
Supplemental material, sj-pdf-2-imr-10.1177_03000605241239021 for POLARIS: efficacy and safety of a vaginal medical device in recurrent bacterial vaginosis—a multicenter, open-label, non-controlled, study with 10 months of follow-up by Filippo Murina, Paolo Inghirami, Marius Biriș, Daniela Sîrbu, Dionisio Franco Barattini, Luca Ivan Ardolino, Mario Mangrella, Elena Casolati, Serban Marius Roșu and Ciprian Crișan in Journal of International Medical Research
Footnotes
Acknowledgements
We thank Federica Sbrocca for medical writing, Luca Barattini for visualization and data management, Adrian Bratu for support in data management, and Marius Ardelean for statistical analysis.
Author contributions
Conceptualization, FM and SMR; methodology, FM, MM, LIA, EC, and DFB; formal analysis, FM, DFB, and SMR; investigation, FM, PI, MB, DS, and CC; writing—original draft preparation, FM, SMR, PI, MB, DS, CC, and DFB; writing—review and editing, FM, MM, LIA, EC, SMR, and DFB; supervision, FM; funding acquisition MM; project administration, DFB, MM, LIA, and EC. All authors have read and agreed to the published version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
FM, PI, MB, DS, SMR, and CC declare no conflict of interest. DFB is employed at Opera CRO, the Contract Research Organization that managed the study. EC is a medical consultant for Italfarmaco SpA. LIA and MM are employed at Italfarmaco SpA.
Funding
Effik Italia SpA, a company of Italfarmaco group (![]() ), the study sponsor, offered the tested medical devices and a partial grant support. The funder had no role in the design of the study, or in the collection, analyses, or interpretation of data, or in the writing of the manuscript, or in the decision to publish the results.
), the study sponsor, offered the tested medical devices and a partial grant support. The funder had no role in the design of the study, or in the collection, analyses, or interpretation of data, or in the writing of the manuscript, or in the decision to publish the results.
Supplementary Materials
The visual abstract in PowerPoint format and a table presenting the timing of the evaluations in the two study periods is available as supplementary material. The full protocol of the study was deposited in protocol.io (dx.doi.org/10.17504/protocols.io.81wgbybbqvpk/v1). In addition, the datasets analyzed are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.