
Abstract
Keywords
“Psychological health factors and only psychological aspects of diet but not actual diet behavior were associated with infertility. Given the multifactorial nature of infertility.”
Introduction
Infertility affects approximately 17% of reproductive-aged women worldwide. 1 Common causes include genetic conditions (eg, Turner syndrome), structural abnormalities (eg, uterine anomalies, endometriosis, pelvic adhesions, tubal occlusion), hormonal imbalances (eg, polycystic ovarian syndrome [PCOS]), and modifiable lifestyle factors (eg, obesity, smoking, excessive alcohol use). 2 Among these, PCOS is a leading cause, affecting up to 20% of reproductive-aged women. 3
While genetic, structural, and hormonal factors associated with infertility are well-established, growing evidence suggests that modifiable lifestyle factors of diet and psychological well-being have a role in reproductive health. 4 Dietary patterns and body mass index (BMI) impact fertility. Diets high in refined sugars, processed foods, trans fats, alcohol, and caffeine are associated with insulin resistance, systemic inflammation, and hormonal imbalances that impair ovulation and embryo quality.4-6 Overweight and obesity are associated with lower fertility and lower clinical pregnancy rates, even in the absence of other comorbidities. 7 In contrast, adherence to anti-inflammatory diets, such as the Mediterranean and ketogenic diets, are linked to improved ovulatory function and increased pregnancy rates. 8
Individuals experiencing infertility report higher levels of stress, anxiety, and depression compared to those not experiencing infertility. 9 Elevated stress and anxiety are associated with delayed conception and reduced success rates with in-vitro fertilization (IVF) treatments. 10 Also, almost one-third of women undergoing infertility treatment have symptoms of depression. 11
Despite increasing recognition of the influence of diet and psychological health on fertility, there does not appear to be any studies that simultaneously examine both factors in relation to infertility. This study aims to assess the association of both dietary patterns and psychological health with infertility.
Methods
This was a cross-sectional anonymous survey conducted at a public hospital located in a Long Island suburb of New York City. Participants were women of reproductive age (18-34 years) who presented for routine care at an outpatient clinic. The only exclusion criteria was a current pregnancy. Data were collected from January 2024 through April 2025. Ethics approval was received from the hospital Institutional Review Board. Informed consent was obtained.
Demographic variables included age (years) and race/ethnicity (White, Black, Hispanic, Asian/Asian American, South Asian [e.g., India, Pakistan], or Other). Medical history variables included self-reported diagnoses of diabetes, chlamydia or gonorrhea, pelvic inflammatory disease (PID), Turner’s syndrome, endometriosis, uterine fibroids, and PCOS, all measured as no versus yes. Anthropometric data were self-reported, including height and weight, which were used to calculate BMI.
Dietary variables included perceived self-reported overweight status (no/yes), trying to lose weight (no/yes), and dietary self-monitoring behaviors of daily calorie counting (no/yes). Participants were asked about daily consumption frequency of various food groups: carbohydrates, fats, and proteins (none, some, mostly, or all), and specific food items of fruits, vegetables, fish, soda, fast food, desserts, alcohol, and coffee (no vs yes). Use of a ketogenic diet was defined as reporting “none” or “some” for carbohydrates, “some” or “mostly” for protein, and “mostly” or “all” for fats. This classification aligns with the macronutrient distribution typical of ketogenic diets, which emphasize high fat (approximately 70-80% of total daily calories), moderate protein (10%-20%), and low carbohydrate intake (5-10%). 12 Use of a Mediterranean diet was defined as reporting “yes” to daily consumption of fruits, vegetables, and fish. This approach reflects components commonly emphasized in Mediterranean diet scoring systems, which consider frequent intake of these food groups as indicative of adherence. 13
Psychological health status was assessed using three reliable and validated instruments. Depression was measured using the Patient Health Questionnaire-9 (PHQ-9), a 9-item scale measured on a 4-point Likert-type scale ranging from 1 = not at all to 4 = nearly every day; a score of ≥10 indicated moderate or greater depressive symptoms. 14 Cronbach alpha in our sample was 0.85. Anxiety was measured using the Generalized Anxiety Disorder-7 (GAD-7), a 7-item scale (GAD-7), measured on a 4-point Likert-type scale ranging from 1 = not at all to 4 = nearly every day; a score of ≥10 indicated moderate or greater anxiety symptoms. 15 Cronbach alpha in our sample was 0.90. Stress was measured using the 4-item Perceived Stress Scale (PSS-4), which assesses how frequently individuals feel overwhelmed or unable to control important aspects of their life. Items are measured on a 5-point Likert-type scale ranging from 0 = never to 4 = very often. Two items are reverse coded. A score of ≥6 was used to categorize participants as experiencing high levels of perceived stress. The PSS-4 is associated with long-term health outcomes, including increased mortality in chronic disease populations. 16 Cronbach alpha in our sample was 0.62.
The outcome variable was infertility (no/yes). Infertility was defined as self-reported clinical diagnosis or lack of conception for more than one year with at least 18 months elapsed time since the last birth. The 18-month threshold was selected to account for the natural suppression of fertility in the immediate postpartum period due to factors such as breastfeeding-associated anovulation and delayed return of ovulation. 17 Participants in the above classification who were currently using contraception were considered fertile.
Mean and standard deviation were used to describe the continuous variables. Frequency and percentage were used to describe the categorical variables. Analysis of variance compared the continuous variables. The Peason chi-square statistic compared the categorical variables except when expected cell size was less than 5 and where the Fisher’s exact test was used. Any variable statistically significant between those with and without infertility was included in a multivariate logistic regression analysis. Sample size was determined based upon sample sizes used in similar cross-sectional surveys. All P-values were two-tailed. Alpha level for significance was P < 0.05. IBM SPSS Statistics Version 30 was used for all the analyses (IBM Corporation, Armonk, NY, 2024).
Results
Sample Characteristics Among Those With and Without Infertility.
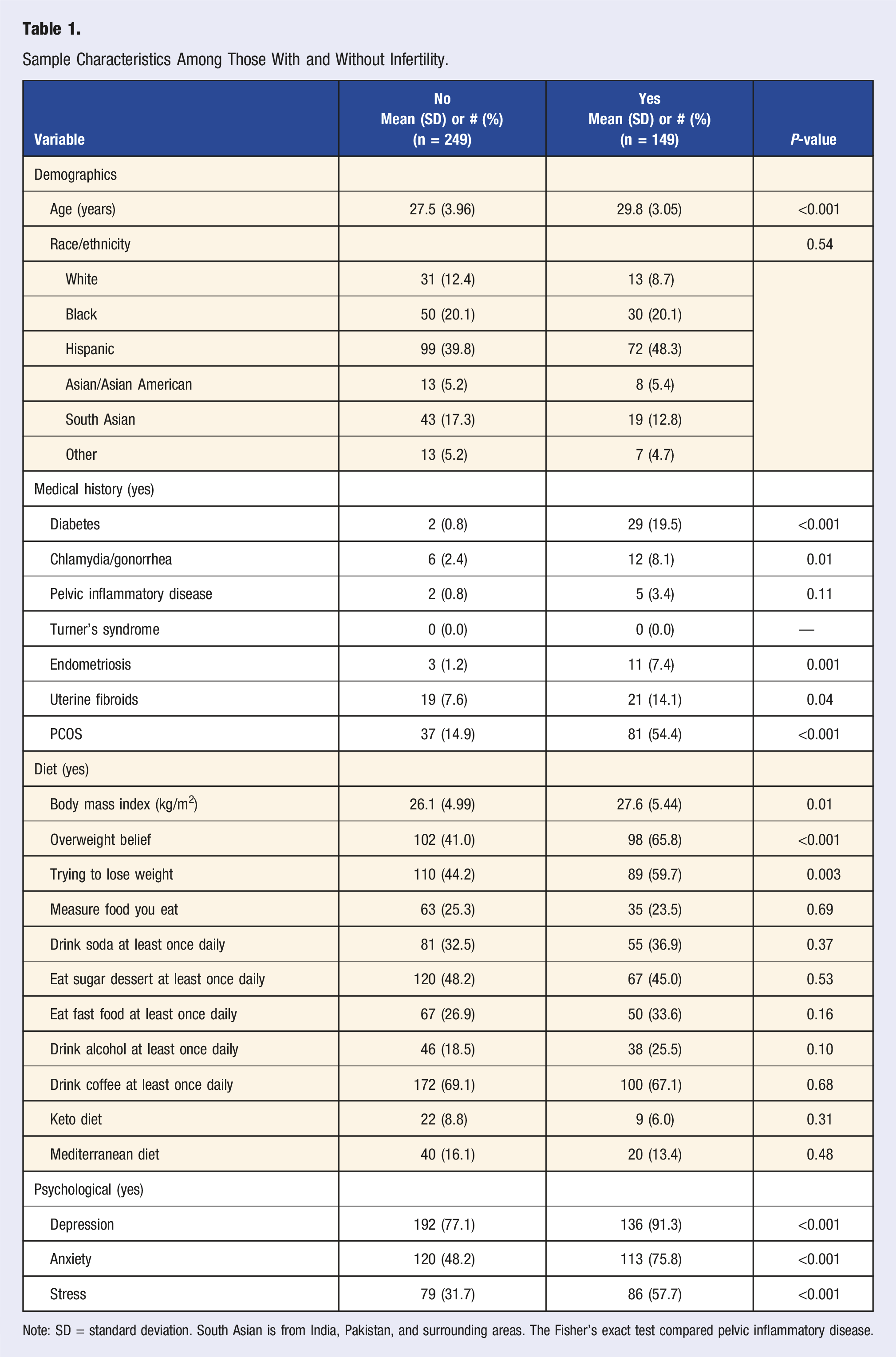
Note: SD = standard deviation. South Asian is from India, Pakistan, and surrounding areas. The Fisher’s exact test compared pelvic inflammatory disease.
Multivariate Logistic Regression Analysis for Infertility.
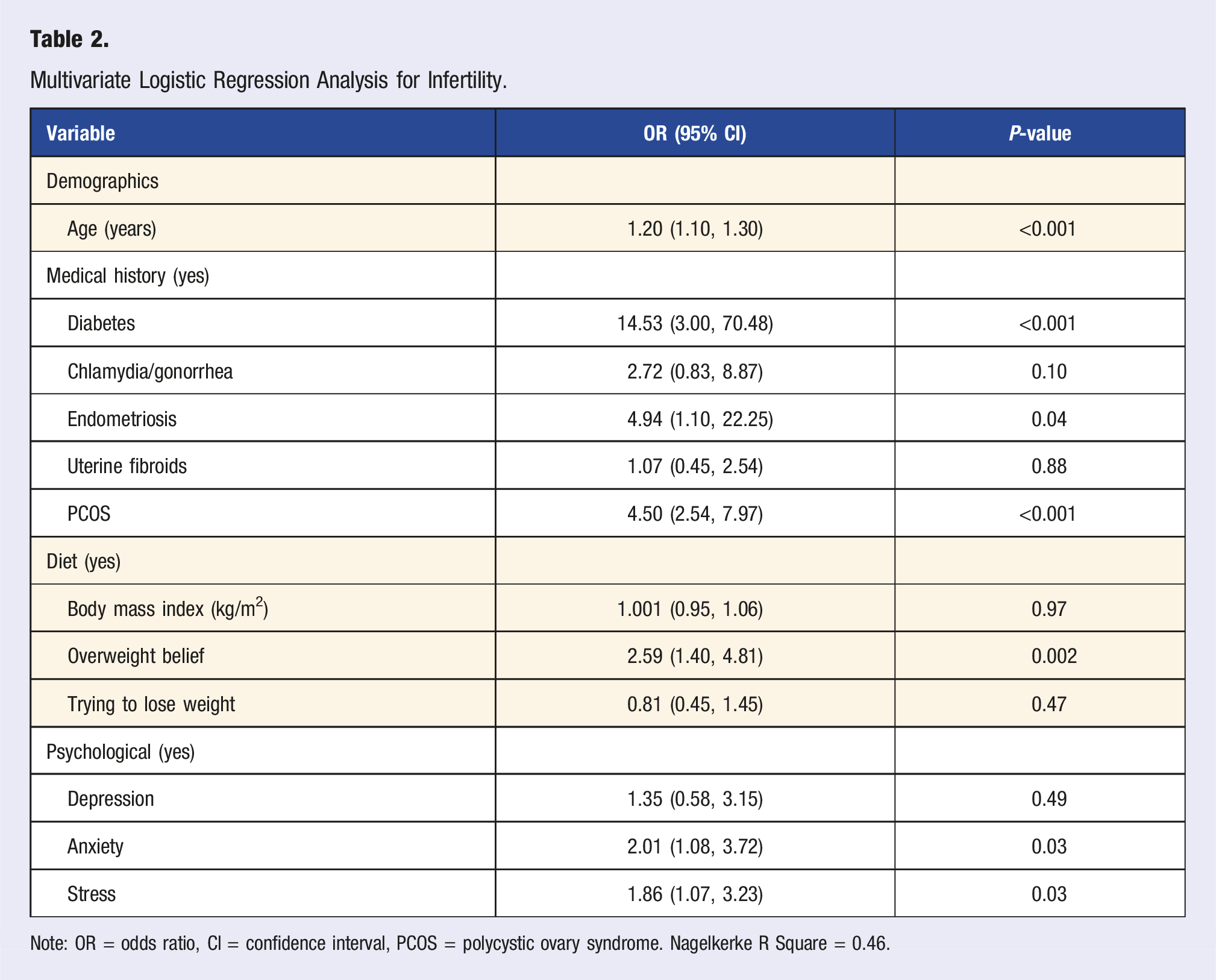
Note: OR = odds ratio, CI = confidence interval, PCOS = polycystic ovary syndrome. Nagelkerke R Square = 0.46.
Discussion
We found support for the association of both dietary and psychological health factors with infertility. We found the belief of being overweight was significantly associated with infertility, while no other dietary variables of food behavior or practicing a ketogenic diet or Mediterranean diet were significantly associated. We found that adverse psychological health factors of elevated levels of anxiety and stress were each independently associated with infertility, while depression was not associated with infertility.
We found that only psychological aspects of diet of the belief in being overweight was significantly associated with infertility. We did not find any association between actual dietary behaviors or adherence to ketogenic or Mediterranean diets and infertility. Previous research reports that adherence to the Mediterranean diet is associated with improved ovulatory function and increased pregnancy rates. 13 Previous research reports that adherence to the ketogenic diet is associated with improved metabolic parameters linked to ovulatory dysfunction and increased pregnancy rates, particularly in patients with PCOS. 3 A number of studies report consumption of certain foods or beverages can influence pregnancy rates.4-6 Our findings contrast with this pattern, as specific diets or food items were not associated with infertility in our sample. Instead, the psychological belief of being overweight was significantly associated with infertility. One key distinction is that our study simultaneously adjusted for adverse psychological health of anxiety, stress, and depression. This discrepancy of our study with other studies may suggest that when psychological health and dietary patterns are assessed together, adverse psychological health may exert a more dominant impact on reproductive outcomes than diet alone. Our findings highlight the importance of considering the psychological components of dietary perception in infertility research and counseling.
We found that adverse psychological health factors of elevated anxiety and elevated stress were each associated with infertility while depression was not associated with infertility. Previous research reports elevated anxiety, stress, and depression as associated with infertility.9-11 Our findings for anxiety and stress are similar to this pattern. However, our finding for depression diverges from these prior studies. In our sample, there were greater percentage-point differences for anxiety and stress of approximately 25% between those with and without infertility while for depression this percentage-point difference was much lower at approximately 15%. We speculate that the markedly elevated levels of anxiety and stress overshadowed the potential importance of depression and its association with infertility.
We found that diabetes, endometriosis, and PCOS were significantly associated with infertility. However, we did not find any significant association of chlamydia/gonorrhea, pelvic inflammatory disease, or uterine fibroids with infertility. Previous research reports all these medical conditions/diseases as being associated with infertility.2,7,8 Our lack of statistical significance can occur for a few reasons. First, there was small sample size for some medical conditions/diseases. Second, there may have been a lack of screening or formal diagnosis for these medical conditions/diseases in our underserved sample with limited access to healthcare and those not reporting the condition/disease may have had the condition/disease. We did observe a significant association between increasing age and infertility, which is consistent with well-established reproductive patterns.1,7
A major strength of this study is including variables from both diet and psychological health. Additionally, our approach to dietary assessment was multifaceted, encompassing specific food intake, adherence to formal diet patterns, and psychological perceptions of weight. This study has several limitations. First, this was from a single center which may affect generalizability. Second, all diet and psychological health variables were self-reported introducing the potential for recall and reporting bias. This is especially relevant for variables of obesity from BMI, chlamydia/gonorrhea, and depression which are reported to be significantly associated with infertility in other studies which focus on more objective data. Our data does not undermine this association but may reflect patients’ perceptions rather than objective truth. Future studies should incorporate objective measures where feasible to replicate our findings. Third, perceptions of being overweight may be influenced by cultural norms, which were not assessed; future research should explore how cultural attitudes toward body image intersect with infertility.
In conclusion, we found that psychological health factors and only psychological aspects of diet but not actual diet behavior were associated with infertility. Given the multifactorial nature of infertility, we recommend that clinicians adopt a comprehensive approach to early infertility evaluation that includes not only formal screening for psychological health status, but also psychological aspects of diet. Such early identification and lifestyle interventions in these domains may improve reproductive outcomes and enhance patient care.
Footnotes
Author Contributions
Quyen Kelly: study design, data acquisition, data interpretation, manuscript drafting, approval of final version. Joshua Fogel: study design, data analysis, data interpretation, reviewing manuscript for critically important intellectual content, approval of final version. Shauna Harrison: data acquisition, data interpretation, reviewing manuscript for critically important intellectual content, approval of final version. Lennox Bryson: study design, data interpretation, reviewing manuscript for critically important intellectual content, approval of final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was received from the Nassau Health Care Corporation Institutional Review Board (IRB#23-458). Oral informed consent was obtained.
Data Availability Statement
Data are available from the corresponding author based upon a reasonable request.