
Abstract
Introduction:
Obesity is a worldwide pandemic that has many contributing factors. There is very scarce data available on this issue for the population in Syria. We aim to evaluate the body mass index and related obesity rates of medical students as they are the role model for the general population. We aim to explore the breadth of potential associated factors including psychological, physical activity, dietary, and a broad array of lifestyle and socio-demographic factors.
Methods:
This is a cross-sectional study that was conducted at a major university in Damascus. Paper-based questionnaires were distributed that included the International Physical Activity Questionnaire short version and the Depression, Anxiety and Stress Scale.
Results:
The mean body mass index was 23.5 (±4.2) kg/m2 with 540 participants enrolled in this study. Males had significantly higher body mass index than females by 2.5 kg/m2 (p < 0.001, χ2 = 47.9, V = 0.3). In our sample, 304 (60.68%) had normal body mass index (18.5–24.99), 40 (7.98%) were considered underweight (body mass index ⩽ 18.5), 120 (23.95%) were considered overweight (body mass index = 25–29.99) and 37 (7.39%) were considered obese. While many factors were found to be significantly associated with body mass index and obesity, only physical activity, depression, having a first-degree family history with obesity and poor dietary habits were associated in regression analyses evaluating all predictors concurrently.
Conclusion:
The findings reflect an ongoing epidemic of obesity. Our findings can guide targeted intervention for this young population who will become doctors and health role models in the future. More studies should be conducted to find the best possible ways to tackle this issue in the future.
Keywords
Introduction
Obesity is a worldwide pandemic that has an increasing prevalence in the world. In 2005, it was estimated that more than 1200 million adults were either overweight or obese worldwide and these numbers will likely exceed 3000 million by 2030 which is more than half of the adult population. 1 In Syria, it was estimated that obesity prevalence was between 4.5% and 3.66% in people aged 2–20 years. 2 Not many studies involved medical students in the region; one in particular was conducted in the Kingdom of Saudi Arabia where overweight prevalence was 21.7% and obesity was 8.4%. 3
Many studies have demonstrated risk factors for the development of obesity such as diet, physical activity (PA), genetic predispositions, and physiological and behavioural factors. 4 Poor dietary behaviours such as a high number of meals and high-calorie food, associated with low PA, smoking and alcohol consumption have been found to subsequently lead to obesity.5–7
Unfortunately, although health personnel have a crucial role in health promotion and are considered role models of having a healthy lifestyle, many studies suggest that obesity is also a common issue among them.8–12 Moreover, medical students’ beliefs about obesity greatly affect their biases towards and ability to counsel patients with obesity. 13 Obesity was a major issue in Syria prior to the 2011 war, with a mean population body mass index (BMI) that corresponded with obesity. 14 However, there has been little if any further study of obesity in Syria since that time.
In terms of the risk factors identified in the literature as being associated with obesity, those of particular relevance in Syria, include smoking cigarettes and shisha14,15 and together with psychological factors, mainly depression.14–16 The rationale for the focus on medical students in this study is that this group represents the future doctors and frontline workers in primary care, which is highly burdened due to funding along with a potential high prevalence of obesity. Furthermore, obese medical students were found to report more implicit and explicit self-stigma which further contributes to worse well-being. 17 It was also found that taking care of stress and regular exercise among medical students would improve their health. 18
This study aims to evaluate the BMI among medical students and the factors associated with elevated BMI including psychological factors of depression, anxiety and stress, PA, including smoking, diet and eating habits with studying.
Material and methods
This cross-sectional study was conducted at Damascus University using paper-based questionnaires which were distributed to medical students after lectures. Damascus University is the largest university in all of Syria and has over 1000 medical graduates every year.
Sample
This is a cross-sectional study that included medical students from 2nd to 6th year from Damascus University who were recruited to fill out a printed questionnaire from October 2019 to December 2019, Syria. Any student with a physical medical condition that might affect the weight was excluded.
Questionnaires were distributed at the end of mandatory lectures on several occasions during the previous period. Anonymity was guaranteed using Google Forms and not taking any personal data such as names or emails. Given population data, an estimation of the population number was 6000. With a 95% confidence interval, 5% margin of error and an overestimation of overweight being 35% among the population, we estimated the sample size to be 331.
In total, 540 Damascus University medical students agreed to participate, with 501 participants included for data analysis, while the other 39 questionnaires were excluded due to having diarrhea in the last 2 days, chronic diseases, diabetes mellitus I or II, endocrine and metabolic disorders that might affect body weight in addition to uncompleted questionnaires.
The average time to complete the questionnaire was 15–20 min and the response rate was 92.8%.
Measures
The questionnaire contained information on demographic data such as name, age, gender, academic year, marital and living status, college score and socioeconomic status (SES).
We could not use a valid tool to determine the SES of participants as there was not a valid tool that could be used in the Syrian community because of the economic differences between Syria and other countries, where the majority of tools were developed, and because it is socially inappropriate to ask about the income or salaries. 19 Therefore, SES was assessed by family income by asking participants to grade their income as good (having a luxurious life), average (having basic needs and some luxury) and poor (providing only basic needs).
The university academic performance average was assessed according to university rankings and was divided depending on their average grades during university.
Body weight and standing height were measured by the researchers and were rounded to the nearest kg and cm, respectively. BMI was measured by dividing weight in kg by height in meters square. Height was measured without shoes and was approximated to the nearest 0.5 cm when standing erect against a wall, heels together and touching the wall. Weight was measured with minimal clothes, no footwear and using a standardized weighing machine. BMI was used to decide students body status and was divided into four categories: underweight (<18.5), normal (18.5–24.9), overweight (25–29.9) and obesity (⩾30). 20
We asked whether the participant regularly smoked or not, how many daily cigarettes, weekly shisha smoking and drinking alcohol (yes, no or occasionally) in addition to living status (with family, alone or other).
We also asked about having a history of first-degree familial obesity (father or mother).
Questions regarding diet and studying were directly asked to the participants. Diet was assessed by asking about the average quantity of meals every day and the average quantity of meat, vegetables and fatty food weekly. This was assessed by directly asking the participant to estimate how much they had consumed in the previous week. These questions were not taken from a validated questionnaire. The daily number of hours spent on studying and eating during studying was also asked.
Demographic questions, diet and SES are all provided in Supplemental Material 1.
PA was assessed using the official Arabic version of the International PA Questionnaire (IPAQ) short version for the last 7 days (IPAQ-S7S 2014). We categorized the PA into low, moderate and high following the instructions provided by the IPAQ scoring protocol. 21 IPAQ questionaries include an estimation of the activities the participant usually does, including high-level activity and how much they walk and therefore an estimation of their activity level. We have included an English copy of the questionnaire as a supplement (Supplemental Material 2) and an Arabic version in Supplemental Material 1.22,23 According to the IPAQ scoring system, 152 out of 501 students were removed from the analysis. We used the Arabic form of the short form of IPAQ which has good validity and reliability with Cronbach’s alpha of 0.769–1.00. 23
A psychometrically validated Arabic short version of the Depression, Anxiety and Stress Scale (DASS 21) 24 was used to assess the psychological health of the students to know its effect on body weight. Each one of depression, anxiety and stress were labelled into five severities (normal, mild, moderate, severe and extremely severe). Then, we combined mild with moderate categories into moderate and severe with extremely severe into severe. Therefore, DASS-21 was categorized into three categories in our study normal, moderate and severe. DASS 21 is validated to be used in Arabic. 24 English version of DASS-21 is in Supplemental Material 3 and the Arabic version is in Supplemental Material 1. 25 The paper is registered under UIN: researchregistry8994. This work has been reported in line with the Strengthening the report of cohort studies in surgery (STROCSS) criteria. 26 This study was approved by Damascus University’s ethical committee and supervised by one of its professors. The approval number is 2839آت. Written informed consent was taken from participants for using and publishing data anonymously.
Data analysis
Data were processed using IBM SPSS software version 26 for Windows (SPSS Inc., IL, USA). Chi-square and one-way analysis of variance (ANOVA) were used to determine statistical significance. Bonferroni correction was used to reduce type 1 error and is calculated using the equation p = α\m given that α is 0.05 and m is the number of hypotheses. 27
Cramer’s V was used to calculate the effect size of the Chi-square. A weak relationship is present if either the Cramer’s V is less than plus or minus 0.10. A moderate relationship is present if either Cramer’s V is between plus or minus 0.10 and 0.25. A strong relationship is present if Cramer’s V is greater than plus or minus 0.25.
We used the Levene test for homogeneity in one-way ANOVA. If the p-value for the Levene test is greater than 0.05, then the homogeneity assumption of the variance is met. If the p-value for Levene’s test is less than 0.05, then there is a significant difference between the variances. In this study, the Levene test was based on the median as it provides good robustness against many types of non-normal data while retaining good power.
Cronbach’s alpha was used for internal reliability. Binary regression is used to assess the statistical significance of multiple variables.
Paper registration and preprint
This paper has a preprint on: https://www.researchsquare.com/article/rs-926816/v1. Our paper is registered under UIN: researchregistry8994.
Results
Of 540 students who completed the questionnaire, 39 were excluded from the analysis due to exclusion criteria. In the sample, 271 were females and 230 were males.
Body mass index
The mean BMI in our sample was 23.5 ± 4.2 kg/m2 and the mean age was 21.3 ± 1.6 years.
The mean height of females was 162.28 ± 6.15 cm, the mean weight was 58.86 ± 10.24 kg and the mean BMI was 22.32 ± 3.53 kg/m2, while the mean height of males was 176.26 ± 6.43 cm, the mean weight was 77.30 ± 15.26 kg and the mean BMI was 24.83 ± 4.45 kg/m2. Furthermore, 304 (60.68%) had normal BMI (BMI = 18.5–24.99), 40 students (7.98%) were considered underweight (BMI ⩽ 18.5), 120 students (23.95%) were considered overweight (BMI = 25–29.99) and 37 students (7.39%) were considered obese (Table 1). Table 2 demonstrates eating patterns, studying methods, PA, and DASS 21 results in our sample categorized by their BMI.
The characteristics of the sample according to each BMI category.

NS: Not significant. Chi-square was used. p Value was considered significant when it was p ⩽ 0.006.
df: Degrees of freedom; V: Cramer’s V; χ2: Chi-square.
Eating patterns, studying methods, PA and DASS 21 results in our sample categorized by their BMI.

NS: Not significant. Chi-square was used in this table. p Value was considered significant when it was p ⩽ 0.0038.
df: Degrees of freedom; V: Cramer’s V; χ2: Chi-square.
Table 3 shows mean age, university year, cigarette and shisha quantity, and number of daily meals categorized according to their BMI. Only testing for anxiety was not homogeneous.
Mean age, university year, cigarette and shisha quantity, and number of daily meals are categorized according to their BMI.
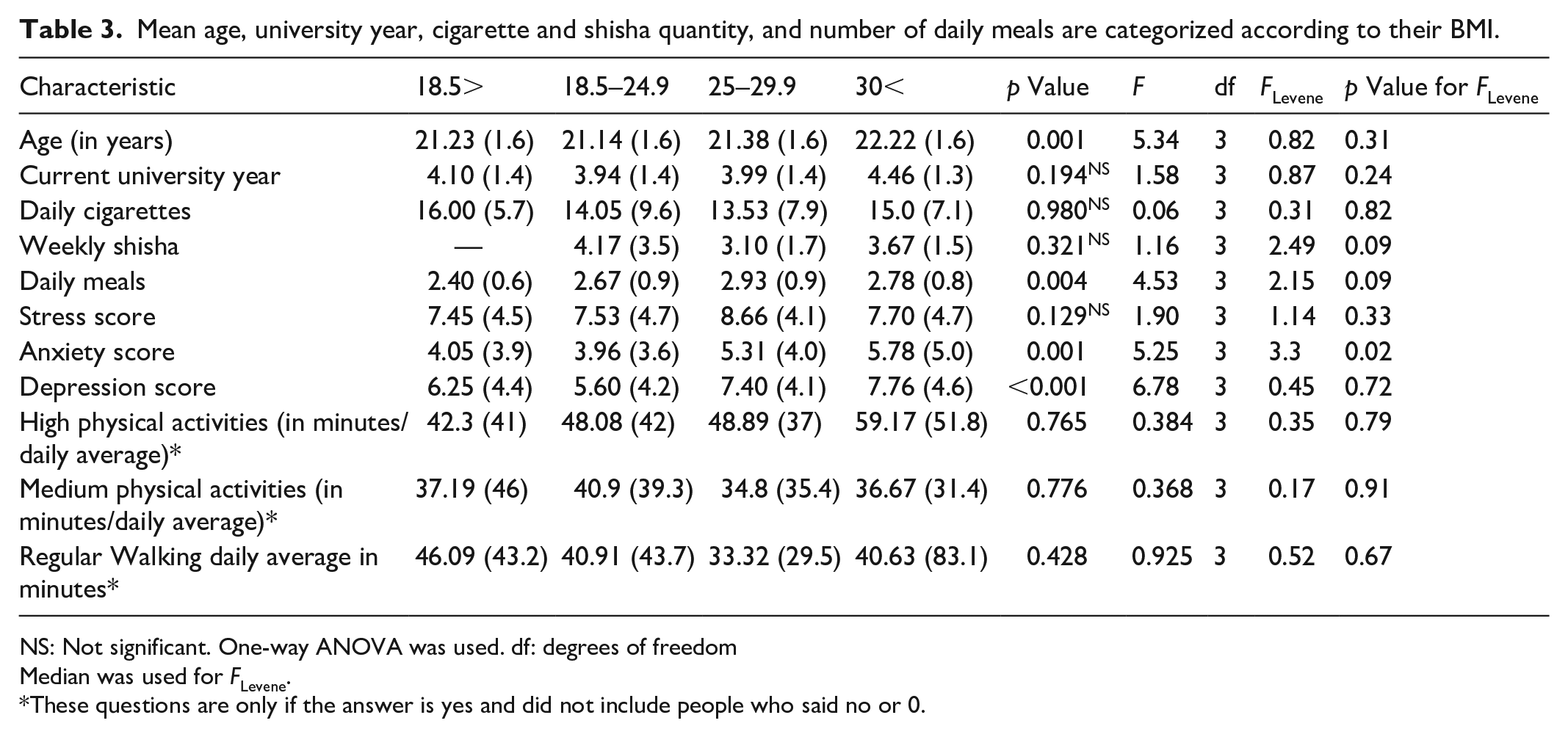
NS: Not significant. One-way ANOVA was used. df: degrees of freedom
Median was used for FLevene.
These questions are only if the answer is yes and did not include people who said no or 0.
We then categorized our sample into people who has a BMI of 25 and more and people with a BMI of 24.9 and less and used the two new categories in the binary regression. We combined occasional and regular alcohol drinking categories into one. When using binary regression on BMI (as shown in Table 4), we found factors associated with elevated BMI included being male (adjusted OR 5.90 (3.21–10.81)), having a first-degree family history of obesity (adjusted OR 2.66 (1.48–4.77)), low PA (adjusted OR for medium PA 0.250 (0.13–0.47)), and greater depression (adjusted OR for moderate depression 2.120 (1.08–4.16) and severe depression 2.87 (1.14–7.21)). Interestingly, although significant in the univariate analyses, no association was found between higher BMI, shisha smoking, alcohol use, anxiety or stress in the regression analyses which controlled for contributions across all predictor variables concurrently.
Stress score, anxiety score, depression score, age, academic year, smoking cigarettes, smoking shisha and number of daily meals are categorized according to each IPAQ category.

NS: Not significant. One-way ANOVA was used. df: degrees of freedom.
Median was used for FLevene.
Physical activity
Examination of the relationship between PA and the DASS scale is shown in Table 5. Anxiety subscale scores decreased as the PA of individuals increased. In the low-PA group, the anxiety score was 5.12 ± 4.27, compared with 3.82 ± 3.866 (p = 0.026) in the high-PA group. No statistical association between the IPAQ score and each of the age, university year, number of daily cigarettes, number of weekly shisha heads and daily meals was found using the ANOVA test.
The characteristics of the sample and exercise level according to IPAQ.

NS: not significant. Chi-square was used in this table. p ⩽ 0.0038 was considered significant.
df: Degrees of freedom; V: Cramer’s V; χ2: Chi-square.
About three-quarters of the high PA group were males 41 (73.2%), which was significantly higher than the males who did low PA 44 (37.9%) (p < 0.001) as shown in Table 5. There were no statistically significant results between the PA and the economic status, mean grades, marital status, smoking, alcohol consumption, living status, heredity within the family, daily mean hours of study, or the scale of anxiety and stress.
When including all the samples, the average days of doing high-intensity workup was 1.3 (±1.8), medium-intensity workup was 2.4 (±2.2) and regular walking was 5.4 (±1.7). For those who were doing high-intensity workups, their average time spent per session of workup was 47.9 (±41.9) minutes. For those doing medium-intensity workup, their average time for workup session was 39.2 (±38.5). For those doing regular walking, their average time of walking on the day was 39.5 (±45.2) minutes.
We then examined factors associated with PA grouping combining those in medium and high PA into one and compared to those with low PA. We used these two categories in binary regression to regress gender, shisha smoking, cigarette smoking, first-degree obesity and drinking alcohol (Table 6). We found males (3.54 (2.29–5.45)), smoking shisha 3.76 (1.79–7.89) and having a first-degree relative with obesity-associated low PA.
Binary regression.

CI: confidence interval; df: degrees of freedom.
Depression, anxiety and stress
Using DASS-21, 208 (41.5%) scored normal for depression, 201 (40.1%) had moderate depression and 92 (18.4%) had severe depression; 250 (49.9%) scored normal for anxiety, 166 (33.1%) had moderate anxiety and 85 (17.0%) had severe anxiety; and 260 (51.9%) scored normal for stress, 166 (33.1%) had moderate stress and 75 (15.0%) had severe stress. Furthermore, according to IPAQ, 116 (23.2%) had low PA levels, 177 (35.3%) had moderate PA and 56 (11.2%) had high PA.
Significant differences on moderate and severe depression scales were found between students with low PA 53 (45.7%) and 23 (19.8%), respectively, compared with students with high PA 14 (25.0%) and 9 (16.1%) respectively (p = 0.040).
No significant association was found between IPAQ and stress and depression (p < 0.05).
Cronbach’s alpha for our study for anxiety was 0.786, depression was 0.803 and stress was 0.810.
We found no significant association between PA and depression, anxiety and stress and thus were not included when regressing on PA.
Discussion
This study found that of the medical students sampled, 23.95% were considered overweight and 7.98% met the criteria for obesity. While little comparative research exists, these results are reasonably consistent with the findings of studies of medical students from the Kingdom of Saudi Arabia (overweight: 21.7%; obesity: 8.4%). 3 Moreover, obesity was estimated to be between 1.5% and 7.8% in Oman in people aged 18–25 years. 28 Obesity prevalence in Palestine with participants aged 18–24 was 5.2% and in Jordan participants aged 20–25 years was 6.8. 28 Also, consistent with this emerging international research on medical students, our study found that males had higher BMI than females. Furthermore, we found levels of PA, mental health (depression specifically), family history of obesity and dietary habits were all significantly associated with higher BMI. Interestingly, no consistent association was found between BMI and shisha smoking, alcohol use, socio-economic or marital status when examined in regression analyses controlling for all predictor variables concurrently.
There is unfortunately a scarcity of studies regarding BMI in Syria. One study that included ages between 2 and 20 years in Syria demonstrated that obesity prevalence was 4.5% and 3.66% while overweight was 20.1% and 19.54% in boys and girls, respectively. 2 Finally, in Lebanon, one study found that among university students (mean age 20 ± 1.9 years), overweight prevalence was 24% and obesity was 7.2%. 29
While these rates of elevated BMI in the medical students in Syria are unremarkable in comparison with rates of obesity across the world population, they are of concern given the particular role these medical students are likely to have in the future as advocates and role models for health in their patient populations. The findings of our study also provide a clearer discrimination of key factors associated with elevated BMI, which allows for a more targeted remediation of this issue.
Consistent with international literature, this study also highlights the critical issue of PA in the prediction of obesity. The World Health Organization recommends at least 150 min of moderate-intensity aerobic PA throughout the week, or do at least 75 min of vigorous-intensity aerobic PA every week. 30 More than a third of our sample did not meet this criterion.
Low PA is considered one of the established risk factors for many medical conditions such as cardiovascular disease, cancer and diabetes. 31 Furthermore, it is associated with worse mental health and quality of life. One large study that included 358 population-based surveys found the prevalence of insufficient PA to be around 27.5% with age-standardizing. 32 Another systemic study that included studies from 20 countries declared that low PA varied from 9% to 43% and was slightly higher in males. 31 Finally, levels of inadequate PA were twice as much in high-income countries (31.6%) when compared to low-income countries (16.2%). 32 With these numbers, we find that 23.2% who had low PA is considered moderate when compared to other countries. This can be particularly significant at this time as low PA is associated with a higher risk of having severe coronavirus disease 19 (COVID-19) and meeting PA guidelines strongly decreases the risk of severe COVID-19. 33 This finding therefore provides some concrete guidance for recommendations to medical students endorsing elevated BMIs to engage in advised levels of PA to better manage their health and weight.
Our findings also have relevance for eating and drinking habits as factors associated with obesity. In our study, we asked participants to estimate the number of meals they had, such as fatty food or meat-containing food. Unfortunately, this method might not be very accurate as biased might interfere with the replies.
Alcohol consumption and certain foods, such as food that was fatty or contained oil, were linked with obesity in our study and the previous study as well. 14 However, we did not find an association with snacks and vegetables. Ha et al. 6 reported that overweight school students eat snacks less frequently than normal weight which is somewhat similar to our findings.
It was noted that among obese and pre-obese Pakistani medical students, 55% of them rarely had breakfast, 47.9% took four meals or more daily, 39.3% had fast-food meals at least three times a week and 58.1% drank soft drinks or juices almost every day. Moreover, obesity was associated with a decreased consumption of red meat. 34
Finally, our study also identified mental health factors as relevant as an association with obesity Depression was associated with increased BMI in the previous study in Syria, 14 similar to our study. Anxiety was also associated with increased BMI, but stress was not.
In a Pakistani study, 56.9% of the medical students, who declared that they tended to binge eat when stressed, were obese. 34 Furthermore, another study found that reducing precipitating factors of stress among medical students would improve medical students’ health. 18 Another study found that obesity-related anxiety is prevalent among college students and might improve with a restricted diet. 35
Many studies found contradictory data regarding depression and obesity. However, the most up-to-date ones demonstrate an association, the most consistent of these being with depression. 16 This provides us with clearer guidance also in relation to attention to encouragement of monitoring (particularly self-monitoring) of mental health and depression for medical students.
Other factors
A published study among university students in Mexico City 36 showed that waist circumference was associated with parents’ obesity, which is consistent with our study. A family history of obesity is necessary because it may be correlated with genetic propensity.37,38
Living with parents was also associated with higher nutritional status, 34 which is different from our study.
Strength
This study included over 500 medical students and it is estimated that this university has around 5000 medical students; therefore, this sample presents around 10% of the studied population. Moreover, the unified method used of paper forms, native language, and methods to measure weight, height and mental health status should make the findings representative of the targeted population. Also, using standard questionnaires that are valid in Arabic was one of the strong points of this study.
Limitation
This cross-sectional study used a paper-based questionnaire from a major university in Damascus. However, this required students to be at the university at the time of data collection and agree to participate. The nature of this study made it difficult to determine the response rate. We could not also determine whether the person was from rural or urban areas as people had to relocate to study in Damascus and due to war that might have caused displacement, which made it hard. While IPAQ and DASS-21 questions were validated in Arabic,21,24 SES and diet questions were not and we were not able to test these questions on pilot. However, this SES tool was used in previous studies on the Syrian population. 19
Conclusion
BMI among medical students in Damascus is probably lower than the general population in Syria. However, it is still an issue that needs to be addressed. The mean BMI in our sample was 23.5 ± 4.2 kg/m2. Males had significantly higher BMI than females by 2.5. Low PA, family history of obesity, poor mental health (depression) and poor dietary habits were all significantly associated with higher BMI, while a broad array of other socio-economic, demographic and lifestyle factors were not.
These findings demonstrate a crisis as overall obesity can reflect worse health outcomes, which, in turn, will reflect negatively on the community as these students will become medical doctors and be considered role models for the public. More awareness should be raised among the population that emphasizes healthier eating and lifestyles and be part of the curriculum both in schools and universities. These findings also provide us with a more refined view into which associative factors ought best to be targeted in medical students to reduce these obesity risks and increase the subsequent flow of impacts onto the patient population. We encourage future studies to explore this matter further.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121241267224 – Supplemental material for Obesity and its related factors among university medical students in Syria: A cross-sectional study
Supplemental material, sj-pdf-1-smo-10.1177_20503121241267224 for Obesity and its related factors among university medical students in Syria: A cross-sectional study by Ahmad Naeem, Yazen AlJaber, Ameer Kakaje, Amjad Ghareeb and Bayan Al Said in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121241267224 – Supplemental material for Obesity and its related factors among university medical students in Syria: A cross-sectional study
Supplemental material, sj-pdf-2-smo-10.1177_20503121241267224 for Obesity and its related factors among university medical students in Syria: A cross-sectional study by Ahmad Naeem, Yazen AlJaber, Ameer Kakaje, Amjad Ghareeb and Bayan Al Said in SAGE Open Medicine
Supplemental Material
sj-pdf-3-smo-10.1177_20503121241267224 – Supplemental material for Obesity and its related factors among university medical students in Syria: A cross-sectional study
Supplemental material, sj-pdf-3-smo-10.1177_20503121241267224 for Obesity and its related factors among university medical students in Syria: A cross-sectional study by Ahmad Naeem, Yazen AlJaber, Ameer Kakaje, Amjad Ghareeb and Bayan Al Said in SAGE Open Medicine
Footnotes
Acknowledgements
None.
Availability of data and materials
The data can be made available upon reasonable request.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Written informed consent was taken before proceeding with the survey for participating in the research, and for using and publishing the data. We assured to maintain confidentiality and asked no questions that might reveal the person’s identity. All subjects aged 18 or older. This study was approved by Damascus University’s ethical committee and supervised by one of its professors. The approval number is 2839آت. Written informed consent was taken from participants for using and publishing data anonymously.
Consent for publication
Written informed consent for using and publishing the data was taken before participating in the research.
Trial registration
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.