
Abstract
“Following the simulation students reported increased confidence partnering with patients to build an individualized LM plan.”
Background
At a private university school of nursing (SON), faculty members within the family nurse practitioner (FNP) program recognized the need to enhance the FNP students’ ability to more effectively assess and address health behaviors when working with patients experiencing or at risk for chronic disease. At this SON, FNP students progress through 3 seminar courses during their final 3 semesters. FNP students traditionally have received training on the pathophysiology of chronic diseases, the pharmacology of medications used to address these diseases, and lab and diagnostic management of disease. Before this pilot, students were introduced to the importance of healthy behaviors in many acute and chronic disease lectures. However, there was a gap in how to more effectively assess and address the needs for health behavior change. FNP students were often able to verbalize that healthy diet, regular exercise and avoiding risky substance use is important for slowing disease progression when discussing treatment plans. Students were often less knowledgeable about the role of stress reduction, restorative sleep, and social connectedness in relation to health outcomes. Students often lacked knowledge and skill on how to partner with patients to make healthy lifestyle changes in the areas of diet, exercise, sleep, avoiding risky substances, meaningful relationships, and managing stress. This lack of knowledge and skill was observed by multiple FNP faculty members while grading narrative assignments, during class discussions, and during simulations.
The importance of appropriately counseling patients in prevention and treatment of chronic diseases cannot be overstated. Six out of every ten American adults is diagnosed with a chronic, noncommunicable medical condition and four out of ten is diagnosed with two or more chronic diseases. 1 It is estimated that approximately 90% of the $3.5 trillion spent annually on healthcare costs in the US goes towards treating chronic medical and mental health diagnoses. 1
Given the vast and growing burden of chronic disease in the US, it is essential to examine how to more effectively prevent and treat chronic conditions and to ensure that student clinicians are trained to meet this need. The link between health behaviors and chronic disease is well established. Katz et al 2 found that 8 health risk behaviors, contribute to 15 chronic conditions that account for 80% of the total cost of chronic care worldwide including poor diet, physical inactivity, smoking, lack of health screenings, poor stress management, poor standard of care, insufficient sleep, and excess alcohol consumption. When examining actual causes of death, the 3 leading causes are tobacco use (18%), poor diet and physical inactivity (15.2%), and alcohol consumption (3.5%). 3
Despite the strong link between lifestyle and health outcomes there is limited time allocated to assessing and counseling patients regarding health behaviors in clinical practice. Healthy People 2030 reports that that only 19% of visits for obesity in 2019 included behavior change counseling about diet and exercise. 4 In response to this, Health People 2030 Goals include increasing the proportion of medical office visits that include counseling or education related to nutrition or weight and increasing the proportion of health care office visits that include counseling or education related to physical activity. 4 Similar goals were included in Health People 2020 however limited improvement was observed between 2010 and 2020. 4
In response to these goals, there is an ongoing need to train clinicians and health professional students in lifestyle medicine (LM) and health behavior strategies.5-8 There has been a growing response to this need in the past decade.5,6,9,10 In 2017, the American Medical Association House of Delegates released a resolution in support of LM inclusion in medical education. 9 This resolution called for the inclusion of LM education and social determinants of health in undergraduate, graduate and continuing medical education. 9 In recent years, professional organizations and health professional schools across the US have intensified their efforts to incorporate LM education into their curriculum.5,6,8,9,11-13 Despite these efforts, LM experts continue to identify gaps in health care provider (HCP) training and urge health professional educators to champion full integration of LM education into their programs.6,8
Extensive work has been done to develop resources and to identify strategies to include LM in HCP training. 8 Frates et al 13 published The Lifestyle Medicine Handbook in collaboration with the American College of Lifestyle Medicine (ACLM) as a comprehensive introduction to LM and the 6 Pillars. Frates et al 14 also developed the LM 101 curriculum available through the ACLM. The LM 101 curriculum includes an instructor manual and thirteen comprehensive slide decks that align with the chapters of the Lifestyle Medicine Handbook.13,14 The Lifestyle Medicine Education website (LMed), created by members of the Lifestyle Medicine Collaborative, was developed to provide open access to evidence-based curriculum recourses and to support training HCP learners and practitioners. 15 LMed resources include slide decks, case studies, videos, and webinars to support training of future and current clinicians in LM. 15 In addition, the ACLM has created opportunities to support programs at nearly every level including Lifestyle Medicine Interest Groups (LMIG), the Undergraduate Medical Education Task Force, pathways for health professionals to become LM certified, both the Full Academic Pathway and Partial Academic Pathway for health professional students, and the Lifestyle Medicine Residency curriculum.6,8,16,27
This work, along with a wide body of scholarly literature, supports the inclusion of motivational interviewing (MI) and behavior change training in HCP student training.17-21 This pilot project follows the example of educational programs that have highlighted the importance of training learners in behavior change strategies.13,14,21 In a systematic review, Kaltman and Tankersley 17 reviewed 16 studies and concluded that teaching MI skills early in the medical school curriculum is feasible and that students can gain basic proficiency in MI. A comprehensive review of the literature by Almansour et al 7 examines the role of MI within the field of LM and highlights the importance of training health care professionals about the essential role of MI in LM clinical practice. Lundahl et al 21 found that MI was an effective strategy for most areas of behavior change across health care locations and patient populations emphasizing the value of the content in health professional student training.
Medical education and medical residencies have led the way in incorporating LM in HCP training and publishing work in this area.5,6,8,12,22 Nurse Practitioner (NP) and Physician Assistant (PA) training programs are in earlier stages of incorporating LM into their curricula but have made progress in recent years. PA leaders in LM have identified the importance of training PAs by incorporating LM into PA curriculum.10,23 PA programs that have successfully incorporated LM in the curriculum serve as models for other advanced practice provider educational programs.10,24-26
While not as well documented in academic literature, efforts to integrate LM content into nursing and NP education programs have grown significantly in recent years. An increasing number of schools and colleges of nursing have received the ACLM designation of Partial Academic Pathway, a program that supports student clinicians in attaining ACLM certification 27 and at least 2 schools have pioneered full integration of LM by offering a LM specialty focus within their Doctor of Nursing Practice (DNP) programs.28,29 Currently, there are 8 DNP programs and 3 NP masters level programs that are part of the ACLM Partial Academic Pathway program. 27 As a part of the Lifestyle Medicine Series, Lifestyle Nursing is a comprehensive textbook by Merlo and Berry that introduces learners to LM. 30 It serves as a valuable resource and guide to educate nurses on how to incorporate LM in their clinical practice and personal lives. 30 Downes & Tryon, 31 published a textbook entitled, Health Promotion and Disease Prevention for Advanced Practice: Integrating Evidence-based Lifestyle Concepts. Within this text, they demonstrate the alignment between LM Core Competencies and NP Role Core Competencies supporting the natural fit of LM into NP training. 31
Importance for Family Nurse Practitioner Students
NP education incorporates nursing models that enhance knowledge and skills for effectively partnering with patients and families to address health behaviors. LM concepts are integrated within NP competencies, 31 and it is important to provide NP students with the most current practice recommendations and to prepare them to be leaders in LM. Training the nursing workforce on effectively assessing and addressing health behaviors directly aligns with the 2021 American Association of Colleges of Nursing Essentials domains of Person-Centered Care, Population Health, and Quality and Safety. 32
NPs often practice in settings that reach underserved populations experiencing health disparities, such as Federally Qualified Health Centers (FQHCs), Nurse Managed Centers (NMCs) and School Based Health Centers (SBHCs). In these settings, the opportunity to build trust with patients is enhanced, as these settings are often close to where patients live, learn, work and play. NPs can partner with patients in both one-on-one visits as well as during group visits and focus on assessing and addressing each of the 6 LM pillars during frequent visits over an extended period of time. The proximity that many NPs have to their patients and the relationship of trust that NPs develop with patients in these settings place them in an ideal position to partner with patients on lifestyle modification, health promotion, behavior change, and ultimately disease prevention and management.
Objectives
This pilot served to integrate LM into the FNP program which incorporated the curricular threads of patient and family-centered care, evidence-based practice, basic science foundations and teamwork and collaboration. In addition, the objectives for this pilot were in line with course objectives that focus on health disparities, risk reduction, health promotion and chronic disease management.
The primary focus of this pilot was to introduce FNP students to the ACLM’s 6 pillars and how they affect patient overall health and well-being. The secondary focus was to improve student confidence and skill in their ability to partner with patients to assess and address areas for improvement in each of the 6 LM pillars.
Objectives
By the end of this pilot program FNP students will: • Build a foundation of knowledge and understand the importance of LM for the prevention, treatment and reversal of chronic disease • Explain the application of LM into clinical practice settings • Demonstrate use of LM knowledge and skills in addressing each of the 6 pillars of LM during small group case studies • Examine the intersection of LM and Social Determinants of Health (SDOH) • Implement LM knowledge and skills in a simulation-based learning event (SBLE) to enhance confidence in the application of LM knowledge and skills
Methods
For this pilot program, the authors used content within the LM 101 curriculum.13,14 The authors used a scaffolding approach and employed various modalities that culminated with a SBLE to provide an opportunity for the application of LM knowledge and skills to a patient scenario. The FNP faculty used multiple modalities for the integration of the ACLM content into the FNP courses. These methods included (1) didactic lectures by FNP faculty (2) expert clinician lectures (3) small group case studies (4) a two-to-three-page narrative assignment and (5) an in-person SBLE. Multiple modalities were employed to help students build capacity to implement evidence-based LM practices in clinical settings. The authors used Bandura’s Social Learning Theory to guide the integration of multiple learning activities geared towards diverse learning styles including visual, auditory and kinesthetic learners. 33 As per Banduras learning model, observation, modeling and imitation are the most effective strategies for learning new behaviors 33 and Bahn 34 discussed how this can be successfully applied to nursing education.
Scaffolding is a strategy by which educators support student learning over time using various methods.
35
Eventually learning supports are removed and students become more independent in their application of concepts, knowledge and skills. In an integrative review, Masava et al
36
reviewed 29 articles that included scaffolding in health science education programs and concluded that these methods enhance competency development. As illustrated in Figure 1, this pilot program incorporated scaffolding by beginning with didactic lectures to build the foundation of LM knowledge and to introduce FNP students to the extensive evidence supporting LM. Building on this knowledge, expert clinicians lectured on the application of LM practice in clinical settings. Students were then given the opportunity to demonstrate the use of the newly acquired LM knowledge by participating in small group case studies. The case studies included patient scenarios that required students to develop treatment plans assessing and addressing the LM pillar focused on by the expert. Students had the opportunity to examine the intersection of LM and SDOH by completing a required narrative assignment reflecting on this intersection in clinical settings. Finally, in order to practice implementing their newly acquired LM knowledge and skills, FNP students participated in a mandatory in-person SBLE with a live standardized patient. More information about each of these modalities as follows: Depiction of pilot program.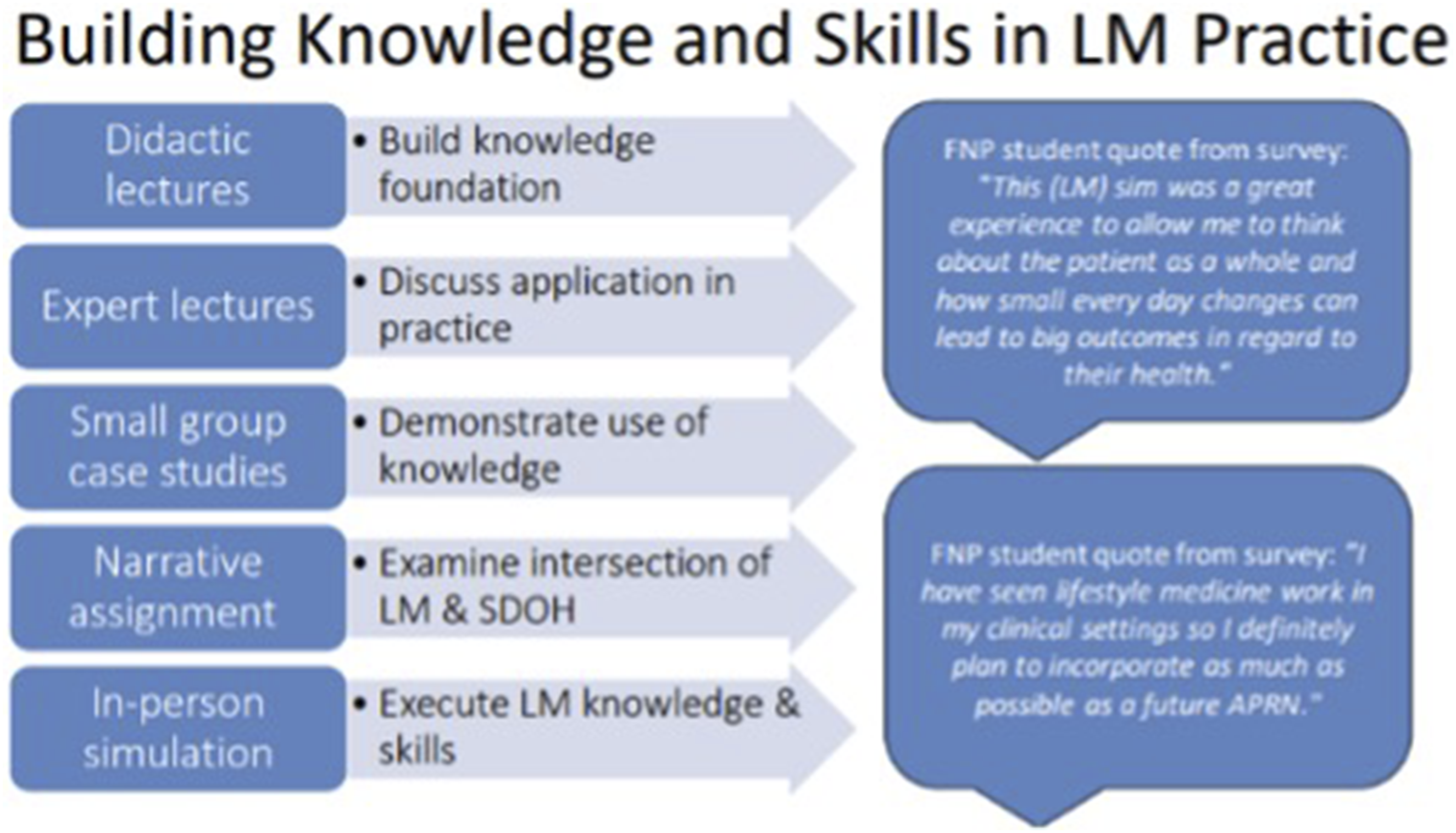
Didactic Lectures Given by Nursing Faculty
With the goal of helping students in building a foundation of knowledge about the evidence behind each of the 6 LM pillars, live didactic lectures were incorporated into class time using the LM 101 slide decks.13,14 Over the course of 2 semesters, FNP faculty lectured on each of the 6 LM pillars. LM lectures were synchronous one-hour presentations via Zoom for each topic. During the first semester, a FNP faculty member introduced LM to the FNP students by delivering the “Understanding Lifestyle Medicine” lecture. 14 This lecture defined LM and highlighted the expansive scholarly evidence supporting the critical impact LM has on health outcomes. 14 This first lecture also focused on the need for LM in clinical settings and for individuals, communities and health care systems. In addition to this introductory lecture, 2 of the 6 the ACLM pillars, stress management and physical activity, were introduced via one-hour synchronous Zoom lectures during the first semester. During the following semester, live synchronous lectures were provided to the FNP student on restorative sleep, nutrition, social connection, and avoidance of risky substance use, again using the LM 101 slide decks. 14
Expert Lectures
To enhance the students’ understanding of how LM is applied in practice, experts were invited to present on how they incorporate LM in their clinical setting. These lectures occurred 1 to 2 weeks after the didactic lecture on each of the 6 LM pillars and were one-hour synchronous classes via Zoom. Experts were intentionally selected from multidisciplinary fields to highlight the interdisciplinary nature of this work. For example, an ACLM certified psychologist provided a lecture that included strategies used to teach patients about the physiologic effects of stress and taught the students 3 specific techniques that can be used with patients. These techniques included (1) mindfulness meditation, (2) deep breathing, and (3) grounding techniques. She also guided students in developing their own SMART objectives for personal stress management. Another expert lecture was provided by a nationally renowned sleep expert who discussed assessment of sleep deficiencies, and which patients are most at risk for lack of restorative sleep, and the importance of referral to sleep disorders clinic when indicated. During the substance use module, a PA led a smoking cessation workshop. The workshop reviewed MI techniques, identification of the level of readiness to quit smoking, how to assist a patient in developing a quit plan, and medications and dosages that support smoking cessation. For each of the 6 pillars, the content was then applied to small group case studies and discussed with the larger group.
Small Group Case Studies
Following the lecture from an expert in the field, the group of 41 students were divided into groups of 6 or 7 students to work on 1 of 2 to 3 patient case studies. The student groups were moved into Zoom breakout rooms and were each given a patient case study focused on the LM pillar discussed by the expert. The case studies provided an opportunity for students to apply the knowledge received from the didactic and expert lectures. The groups were asked to discuss how they would assess and address the patient scenario. After 20 to 30 minutes students were brought back into the large group Zoom room to discuss each case. Students led the conversation, providing examples of how they would develop a treatment plan for their assigned case study patient, incorporating what they had learned from the ACLM didactic lecture and the expert lecture that day. Students received feedback from the nursing faculty, the expert lecturer and their peers.
Written Assignment: LM and SDOH
In addition to the lectures and application activities, students wrote a two-to-three-page paper that explored the intersection of LM and SDOH. Students first listened to the “Lifestyle Medicine Into Underserved Communities” Podcast interview between Dr Dexter Shurney and Corey Dion Lewis. 37 In the assignment guidelines, students were required to highlight content from the podcast that was most interesting or relevant to their current clinical setting or future desired work environment. In addition, students were required to cite at least 1 scholarly article about an intervention or program targeting 1 of the 6 LM pillars with an underserved population and discuss how this addressed a specific SDOH. If they were not able to identify a specific intervention that addressed 1 of the 6 LM pillars and SDOH concurrently, they were required to outline what could have been done to more effectively to address LM or SDOH within the intervention.
Simulation-Based Learning Experience (SBLE)
As a culminating experience, students participated in a required LM simulation. This provided students an opportunity to apply the knowledge and skills they learned from the lectures, case studies and narrative assignment in a live learning environment. This type of learning may be especially effective for kinesthetic learners. 38 In a systematic review of literature related to the NLN Jefferies simulation model a major finding was that simulation clearly contributes to improved performance. 39 The in-person simulation was designed to give each FNP student an opportunity to demonstrate their ability to assess and address LM during a simulated clinical encounter.
The authors developed a patient scenario in which students would independently interact with a trained standardized patient in a simulated clinical setting. The simulation was observed by faculty via live video monitoring and occurred at the end of the second semester of LM instruction. During the simulation, students were expected to demonstrate proficiency in assessing and addressing LM during a patient encounter. Forty-one students participated in the in-person LM Simulation.
Simulation Objectives
The simulation’s goal was to provide an opportunity for FNP students to apply the knowledge and tools learned about LM over 2 semesters. By the end of the simulation, participants were expected to be able to: 1. Demonstrate the ability to perform a thorough health history and physical examination 2. Assess the patient’s level of readiness for change, based on the Stages of Change Model
40
3. Provide support and encouragement using MI techniques 4. Determine the patient’s willingness and barriers to change 5. Set SMART goals that are congruent with patient’s readiness to change 6. Identify diagnosis of prediabetes and provide appropriate education and plan for this, ideally with 1 SMART goal for healthier dietary choices and possibly 1 FITT goal for increased physical activity
Pre-Briefing
Prior to participating in the SBLE, students were advised that during the simulation they would be required to address appropriate elements of the history of the present illness, past medical history, social history, medications, allergies, and family history in addition to a focused physical exam within a 30-minute visit. They were also advised that they should identify the patient’s readiness to change and use MI to partner with their patient to develop a SMART goal or FITT prescriptions that would address at least 1 of the 6 LM pillars and develop a plan for follow-up with the patient.
Simulation Case Scenario
The simulation setting was a primary care outpatient visit. The simulation patient, between 45 and 60 years old, was diagnosed with prediabetes 3 years ago and was now here for a follow-up visit for lab results. Lab results from the week prior had revealed that the hemoglobin A1C result had increased from 5.9 to 6.1 over the past year. The patient’s father had passed away from poorly controlled diabetes after a foot amputation. The patient was very interested in avoiding a diagnosis of diabetes but felt that his/her stressful work as a high school teacher was making it difficult for him/her to make healthier dietary choices. The patient and his/her spouse enjoyed eating out at restaurants many times each week. In addition, the patient felt that long workdays made it difficult to find time to include physical activity in the week. When asked, the patient reported that they slept for 7 or 8 hours each night, consumed 1 or 2 glasses of wine each week and did not use any tobacco products, vape or recreational drugs.
Debriefing
After completing the individual live simulation, students received individualized feedback from the standardized patient about communication style and how well they partnered with the patient during the visit. Following this, students were provided individualized feedback from a NP faculty member who evaluated their history taking skills, physical examination techniques, diagnosis and plan of care with a focus on incorporating appropriate health behavior education and prescriptions including a follow-up plan. The final portion of the simulation experience included a small group debrief with 5 or 6 students. This small group met with NP faculty to further discuss what went well, challenges encountered and overall learning that could be applied to the clinical setting.
Results
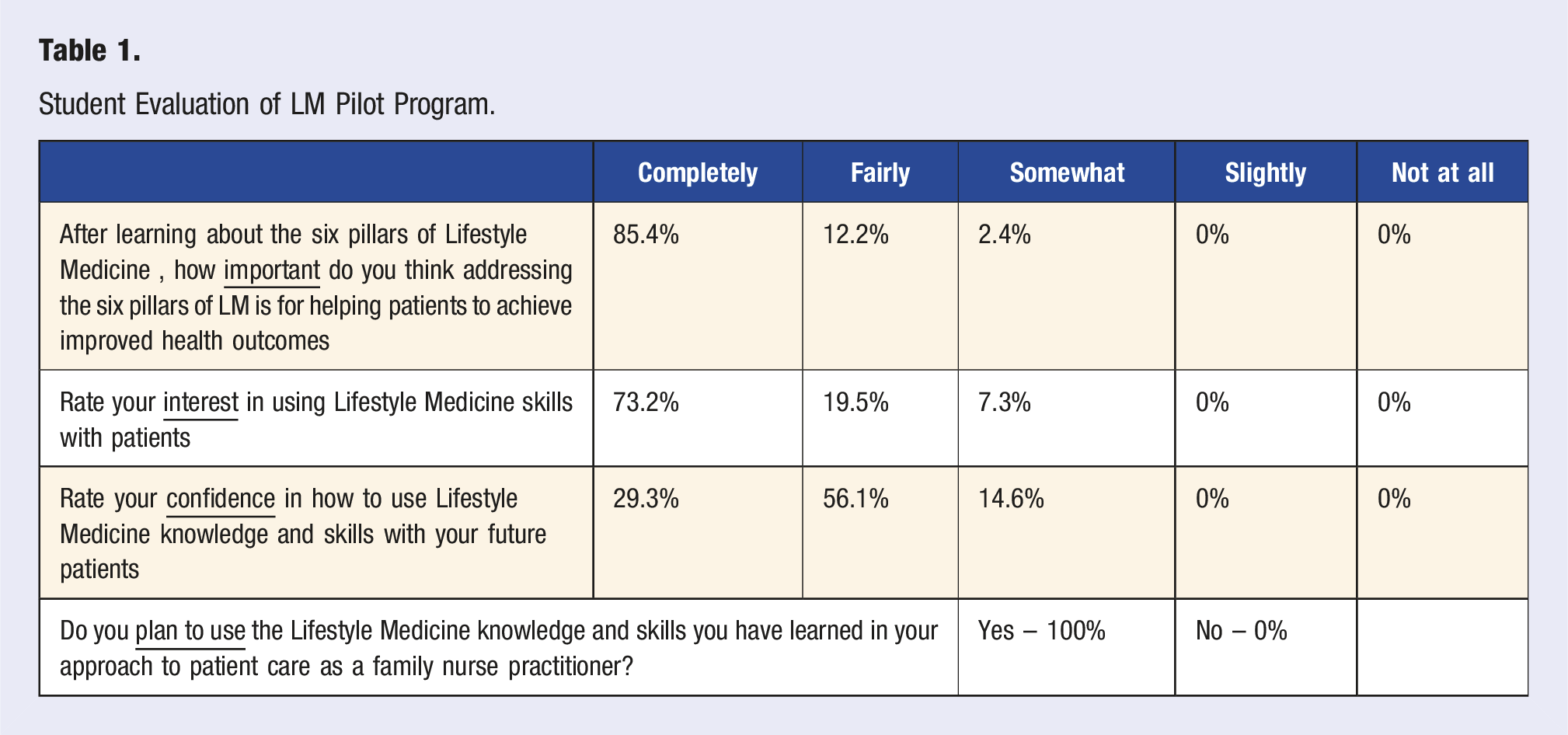
Student Evaluation of LM Pilot Program.
Student Assessment of Effectiveness of Each Teaching Strategy.
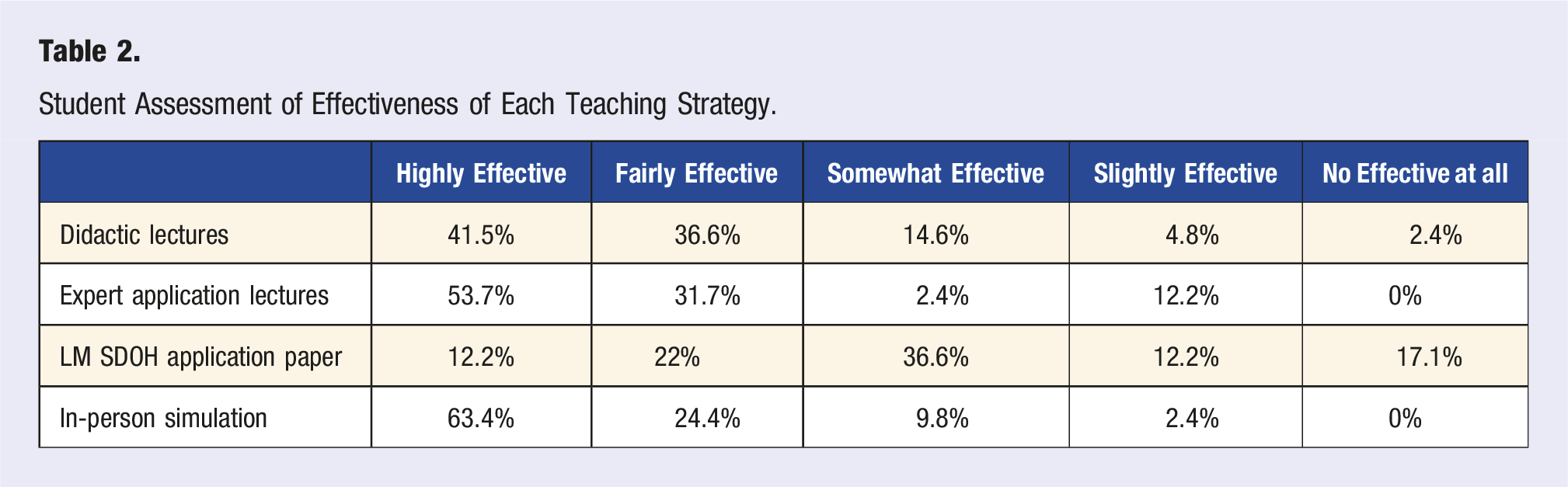
When asked what was the least effective or least interesting part of the LM content covered over the 2 semesters the following themes were reported; the application paper (6), didactic lectures (4), not enough opportunities to practice were provided (3), too much redundancy (3), simulation (1), breakout groups (1), and sleep lecture (1).
One quote that represents many of the student comments was that: [there was a] lack of interaction/practice. I feel I understand the information that was presented very well, but I struggle more with how to practice explaining and educating with the information.
When asked what was the most effective or interesting part of the LM content covered in the 2 semesters the following themes were reported; the simulation/being able to practice (17), expert application lectures (6), smoking and substance use content (5), nutrition content (3), everything (3), sleep content (2), social connectedness content (2), physical activity content (1), didactic lectures (1).
One quote that captured the sentiments of many students highlighted the value of addressing all 6 pillars; “social connection! also we always tell our patients about diet and exercise but it’s SO useful to also talk about sleep, wellness, and substance use as well. I have so many new tools in my toolbox and I plan on incorporating lifestyle medicine whenever I can with a patient.”
A second quote highlighted the importance of time for application and simulation: “The in-person simulation this semester was very helpful with honing MI techniques and having the opportunity to practice the skills we've been learning over the last 2 semesters. I enjoyed the application lecture days because it helped solidify any topics covered the week prior. It was very effective and informational to have the course structured that way. It helped cater to different learning styles.”
Student Evaluation of the Simulation Activity Based on Adapted SET-M Survey.
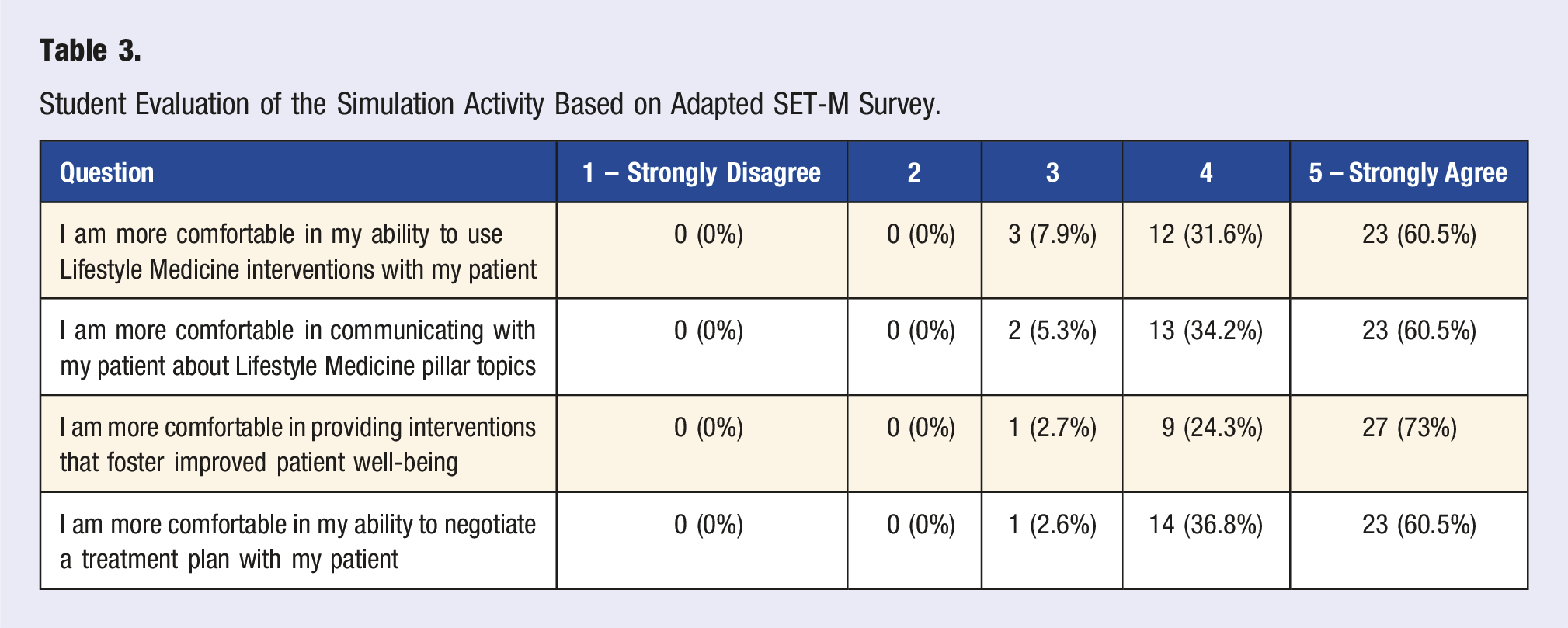
Overall students responded favorably to the simulation which was consistent with the larger evaluation of the LM pilot program. Students reported that they felt more comfortable communicating with patients about topics of LM and developing a LM treatment plan with patients after the simulation. Students responded that the debrief with the standardized patient and the faculty was valuable.
When asked “What did you like best in todays simulated clinical experience?” the following themes were reported: Feedback during debrief with standardized patient and/or faculty (14), the opportunity to apply health behavior change principles that have been taught (10), the opportunity to practice MI and have this dialogue with the patient (9), and the realistic scenario (4).
Three quotes that provide a representation of the students’ comments include: “I liked the collaboration felt between myself and the patient. It didn't feel as though I was preaching a point, but rather working alongside the patient to discover a SMART goal to improve the patient's lifestyle as they saw fit.” “The realness and prevalence of the topic discussed with the patients and how to motivate someone who does not know a lot about exercise and healthy nutrition.” “I liked that today really tested my ability to perform motivational interviewing. My SP and [faculty] were super helpful in their feedback in ways to phrase questions.”
When asked “How did this simulation help you apply Lifestyle Medicine content to a clinical scenario?” the following themes were reported: it provided an opportunity to practice LM and behavior change rather than only pharmacological treatment plan (20), it allowed opportunity to practice MI and goal setting with the patient (15), it allowed time to practice discussing all or many of the six pillars of LM (8), and the chance to think about and plan appropriate follow-up (2).
Three quotes that provide a representation of student comments include: “Making a plan revolving around LM in the context of a treatment plan made me more confident in my knowledge of these subjects and how important they are to implement in chronic diseases.” “I think it was great to have this simulation as I have not had the opportunity to provide in-depth lifestyle change education to my patients in clinical. It was a good simulation because there are many patients who are pre-diabetic and diabetic and this gave me a safe environment to learn.” “This scenario helped me to be able to consider lifestyle modifications instead of solely pharmacological options to be able to provide treatment for my patient. It also allowed me to incorporate motivational interviewing to determine the best treatment options.”
In addition to the structured survey evaluation findings outlined above, the faculty evaluated the success of the LM curriculum based on student performance and through dialogue in the simulation debrief sessions. Anecdotally, faculty reported that FNP students exposed to this pilot project were able to discuss the role of LM in improving patient health outcomes and demonstrate skills to assess and address the 6 LM pillars with patients. In comparison, previous cohorts that did not receive the LM pilot program, limited health behavior recommendations to simply listing diet and exercise as important to the plan of care. Students in this pilot program demonstrated the use of MI interviewing techniques with patients, discussed the benefits of engaging patients in goal setting, and the development of SMART goals and FITT prescriptions in the care plan. A final metric of success was that all students passed the simulation with a grade of 80% or above demonstrating proficiency in meeting the objectives of the SBLE.
Discussion
Based on the evaluations, student feedback, faculty grading, and faculty observation this LM pilot program pilot was successful at meeting the objectives for the overall project and the LM simulation. After the program, FNP students understood the importance of LM and how it integrates into clinical practice. FNP students became more confident in their ability to assess the individual patient LM gaps and to develop treatment plans including counseling and lifestyle prescriptions. This project adds to the growing body of literature as an additional example of how educators of student clinicians from a wide range of disciplines, including NPs, can integrate LM into their curriculum.
Consistent with Bandura’s Social Learning Theory new behaviors are best learned through observation, modeling and imitation. 33 This project’s success is largely due to the purposeful scaffolding of content and application of the Social Learning Theory. As illustrated above in Figure 1, students initially had lectures to build a knowledge foundation. This was followed by expert lectures and case studies to discuss and demonstrate the application of knowledge. Finally, the simulation allowed students the opportunity to apply the knowledge and skills in practice. Consistent with NLN Jefferies simulation model that demonstrates how simulation contributes to improved performance 39 feedback from students and faculty observation of performance indicated that the simulation was most effective at increasing student confidence. Following the simulation students reported increased confidence partnering with patients to build an individualized LM plan.
Based on faculty observation comparing student performance in simulations prior to this LM education program and after completion of the program, students who participated in this pilot project performed significantly better in the objectives outlined above. It is notable that the foundational didactic lectures, discussions with content experts about application and use of case studies were crucial in their role to set students up for success in the simulation and ultimately the clinical setting. While the simulation was generally reported as the most effective portion of the program it is unlikely that it would have been as successful without the foundational LM knowledge and skills taught over the course of the two-semester program.
Based on student feedback, some of the adjustments made in the second year were to provide focused didactic lecture from LM 101 slides and use the second portion of class to allow an expert to discuss application to reduce redundancy and increase emphasis on application. In addition, the application paper was removed, however the importance of integrating SDOH and LM was still integrated into the lecture content, discussions with experts and the simulation.
Limitations
While the overall program and simulation evaluation survey provided positive and consistent findings, there is no baseline measure for comparison. Due to this, it is unclear how much of the LM knowledge and skill improved over the two-semester program. While students reported evaluating how much they learned or gained from the program and each individual component, this may not be separated from learning from other courses or clinical rotations they were completing simultaneously.
This program provided a strong introduction to LM with 12 hours of classroom content. However, it is recognized that this is merely an introduction to a vast and growing field of LM. Hopefully, this will provide a base of knowledge for all learners regardless of where they practice and that they will consider application of LM into their clinical practice. This program was also designed to introduce LM to students that may be inspired to pursue LM certification and clinical practice with a LM focus.
Conclusion
This pilot program and these findings are significant given the urgent need to better equip the US health care workforce with skills for more effectively preventing and treating chronic diseases and the burden they impose on our health care systems, economy, communities and individuals. To reach the goal of having clinicians ready to partner with patients to successfully assess and address health behaviors it is imperative that clinician educators advance their knowledge and skills for how to best train future clinicians. This program adds to the growing body of work in this area. It also supports the concept that educators cannot simply provide content in lectures, readings or even case studies but that clinician learners need opportunities to implement LM best practices in simulated and real-world clinical settings. NPs trained in the nursing model and focus on whole person care are in an ideal position to take an active and leading role in increasing LM best practices in clinical settings. Rigorous educational programs that incorporate LM content and simulation opportunities into NP training must be replicated. This pilot and other LM education programs can serve as examples for future work in this area.
Important next steps include further analysis of student feedback data and continued revision of program modalities with the goal of reducing redundancy, identifying opportunities for additional application activities, and continuing to update content as the field of LM advances. Additional next steps include the development of a LM elective course for NP students so that students with an interest in LM can experience a more extensive exploration of the evidence behind LM and experience clinical practicum hours in LM clinical settings. This would provide a trajectory for LM certification and enhanced incorporation of LM in clinical practice after graduation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.