
Abstract
The increasing prevalence of reduced habitual sleep duration presents a significant public health challenge, impacting cardiovascular health, metabolic function and mental well-being. This umbrella review analyses findings from systematic reviews and meta-analyses to comprehensively evaluate the consequences of sleep deprivation (SD) on health. The databases searched included PubMed, Scopus, and Web of Science. Inclusion criteria focused on adult populations with SD and systematic reviews/meta-analyses. Twenty-nine articles were included in the final synthesis, encompassing a variety of health outcomes. Key findings highlight a U-shaped relationship between sleep duration and all-cause mortality, with both short (<7 h) sleep durations associated with increased risks. SD was a significant risk factor for cardiovascular diseases such as hypertension, stroke and coronary heart disease. Alongside heightened risks of metabolic disorders, like obesity and type 2 diabetes. Moreover, SD contributed to elevated anxiety levels, impaired emotional regulation. As well as increased susceptibility to stress and depressive symptoms. This synthesis underscores the critical importance of maintaining recommended sleep duration (typically 7-9 h for adults) to mitigate these health risks effectively. The findings support the need for robust public health interventions aimed at promoting healthy sleep habits to reduce the burden of associated health conditions and enhance overall well-being.
“Short sleep duration has been identified as a contributing factor to the development of atrial fibrillation (AF), a major risk factor for stroke.”
Introduction
The prevalence of habitual sleep loss has become a major concern today due to night shifts and other work. The consequences of lack of sleep may not have an immediate impact on health, but chronic sleep loss seems to have adverse effects on a person’s well-being.1,2 Several studies have recorded the impact of reduced sleep time on the cardiovascular system, the metabolic system, and even depression and anxiety levels.3,4 The recommended amount of sleep for adults (18-65 years) should ideally be 7-9 h per day, while older adults (65+ years) should aim for 7-8 h of sleep per day. The amount of sleep required varies with age, with children and adolescents needing more sleep than adults, usually over 8 h per day.5-7 Adults and the elderly, who often sleep less than 7 h, are at increased risk of health issues 8 ; however, both sleeping too little (less than 6 h) or too much (more than 9-10 h) appears to negatively influence well-being to varying degrees.9,10
Sleep duration and its association with various health-related outcomes have become a major topic of interest and concern, evidenced by 18 systematic reviews conducted in the last decade. Adverse health effects are a by-product of inadequate sleep duration, with reduced sleep time reported to increase the risk of all-cause mortality among both male and female.8,11 Chronic sleep deprivation (SD) has been linked to the development of co-morbidities such as hypertension, diabetes, and obesity.12,13 The elderly population is more affected than adults, mainly due to pre-existing health conditions. Sex differences also play a role, with male being at a significantly higher risk of all-cause mortality due to short sleep. In both male and female, the risk of all-cause mortality increases with sleeping more than recommended duration.11,14
Recent studies indicate a U-shaped relationship between sleep time and co-morbidities such as hypertension, cardiovascular diseases (including atherosclerosis, stroke, and coronary artery disease), diabetes mellitus and obesity.15,16 Short sleep duration can lead to an increase in overall body weight and influence glucose metabolism. Insufficient sleep also affects homeostasis, leading to food cravings, reduced insulin sensitivity, and altered levels of leptin and ghrelin.17,18 Due to these reasons, inadequate sleep is linked to metabolic syndrome. 19
The hypertensive effects of SD have also been studied in the past, showing a positive correlation between SD and hypertension, but results vary based on the population, due to factors such as sex, age etc.16,20,21 The elderly population (65+ years) is at a higher risk for hypertension compared to younger adults (under 65 years).16,20
The sweet spot in the curve representing the relationship between sleep duration and the development of negative health outcomes, typically falls between 7 to 9 h of sleep per night. 22 This duration is generally associated with the least risk for adverse health conditions, compared to both shorter and longer sleep durations. Lack of sleep is associated with obesity, as indicated by the U-shaped relationship between sleep duration and health outcomes. While factors such as overall dietary intake and circulating hormone levels (leptin, ghrelin, and thyroid hormones) influence body mass, the correlation between sleep and obesity is significant. Zhou and colleagues reported a reverse J-shaped relationship between sleep duration and obesity, with the lowest risk associated with 7-8 h of sleep daily.18,23
Emotional instability combined with elevated cortisol levels is also correlated with lack of sleep. 24 SD appears to be a major cause of increased anxiety levels, emotional stability, aggression, mood and depressive states.4,25-29 It has been shown to predict a range of behavioral and psychological changes, including heightened irritability, reduced attention span, impaired emotional regulation, and increased interpersonal conflicts, such as those within marital relationships.26-29 Anxiety is usually considered a secondary outcome of SD, with primary physiological processes including increased sympathetic activity, heart rate and blood pressure. 30
Currently, various systematic reviews individually examine the specific physical and mental health effects of SD. However, a comprehensive review providing a complete overview is lacking. Such a review is important to identify patterns, relationships, and potential mechanisms associated with SD and various health issues. The growing body of research in this area can be overwhelming for health care providers, researchers, and policymakers to synthesize and interpret. Comparing findings from different reviews that may have used varied methods is essential to understand the discrepancies in conclusions. Moreover, examining the degree of overlap in the primary studies included in these reviews helps to clarify the consistency of evidence. By synthesizing the highest quality evidence, practice guidelines can be developed to offer informed recommendations. Ultimately, answering a broader question through this synthesis can advance the field by providing a more holistic understanding of the overall effects of SD on health. To achieve this, we conducted an umbrella review to gather information from existing systematic reviews and meta-analyses, highlighting the combined physical and mental impacts of SD on health. The purpose of this umbrella review is to synthesize evidence from diverse settings, provide guidelines for clinical practice, and underline the importance of having a public health intervention.
Methods
Guidelines
This umbrella review followed three specific steps to ensure a comprehensive synthesis of existing evidence.31,32 First, we developed a systematic search strategy tailored to capture a wide range of reviews on SD and its health effects. Second, we applied rigorous inclusion and exclusion criteria to delineate the boundaries of the review, to enhance methodological quality and reliability, and utility of the data. Third, we extracted key data points from the selected studies using a standardized form, including information on study design, population characteristics, sleep measures, health outcomes, and key findings. By following these detailed steps, the umbrella review method allowed us to map out the broad landscape of existing research on SD and its health effects, offering a holistic and nuanced understanding that bridges gaps in knowledge and provides an evidence base for practical applications, clinical guidelines and future research.
Search Strategy and Information Sources
A search strategy including keywords relevant to SD and health outcomes was developed and used to identify relevant articles in published in three databases (PubMed, Scopus, Web of Science). The search included Boolean operators as follows: (“sleep loss” OR “sleep deprivation”| OR “sleep restriction”) AND (“health” OR “depression” OR “anxiety” OR “public health” OR “cardiovascular disease” OR “ischemic heart disease” OR “cancer” OR “respiratory disease” OR “stroke” OR “cerebrovascular disease” OR “metabolic syndrome” OR “morbidity”) AND (“Systematic review” OR “meta-analysis” OR “meta-analyses”). A comprehensive literature search was conducted from database 2008 to 2024.
Article Screening
Articles were independently screened for eligibility by title, abstract, and full text by two reviewers (ASS and MRP). Duplicate articles were recorded and removed. Any conflicts were solved by the third reviewer (TB). Furthermore, we performed forward reference searching by examining citations and authors to uncover potential subsequent reviews. The screening process is outlined in detail in Figure 1, using a flow diagram. PRISMA 2020 flow diagram for systematic reviews which included searches of databases. 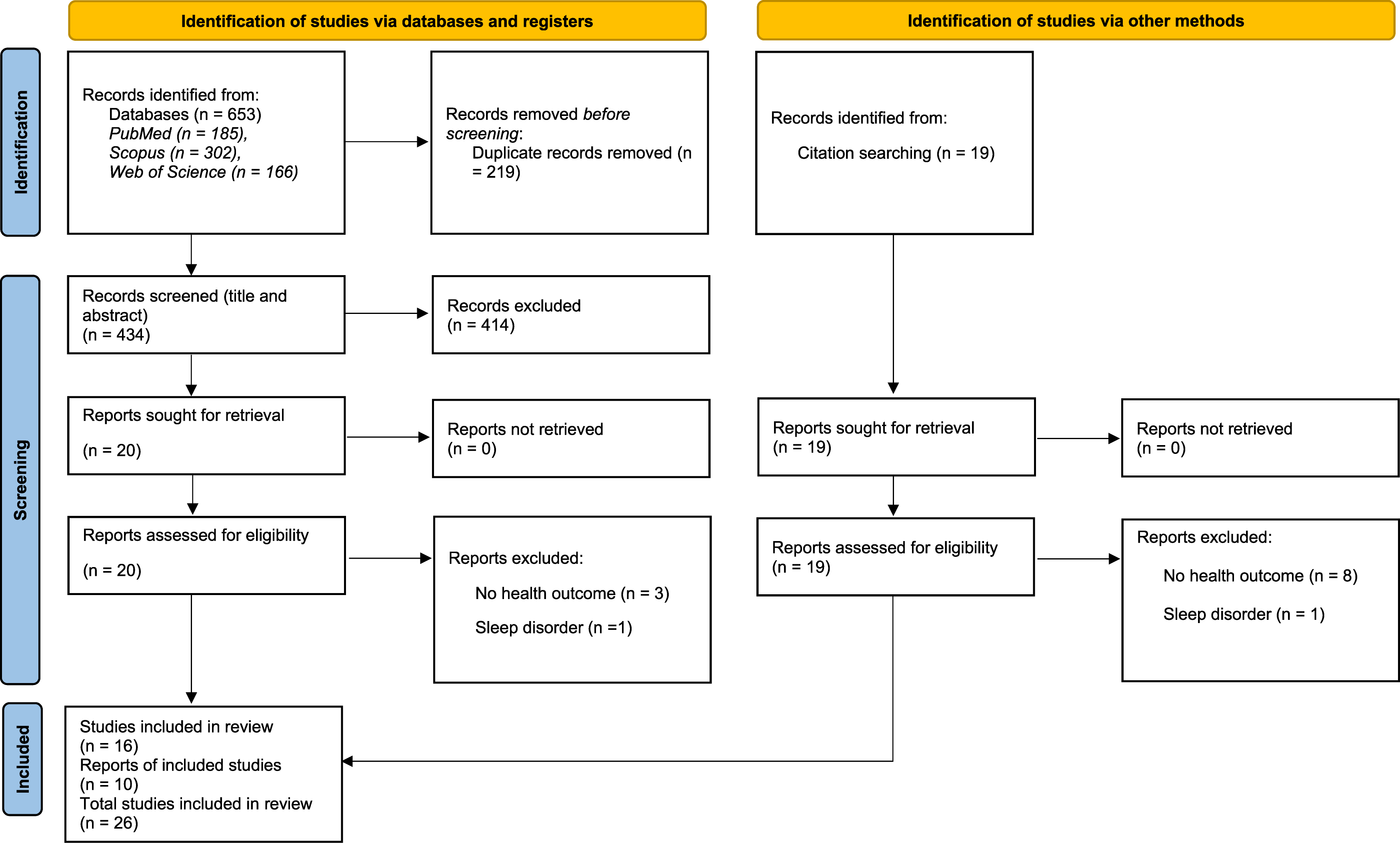
Eligibility Criteria
The inclusion and exclusion criteria were set and agreed upon by 3 reviewers (ASS, MRP and TB). The eligibility criteria for this umbrella review were developed based on Population, Intervention, Comparator, Outcome, Study Design (PICOS). The articles were accepted for screening if they met the following inclusion criteria: (P) examined adult male and/or female participants (≥18 years); (I) included participants identified to habitually experience sleep restriction or inadequate sleep (<7 h per night); (C) included participants identified to habitually obtain recommended amounts of sleep (7-9 h per night); (O) reported risk measures for overall mortality, cardiovascular disease, metabolic disease, stroke, cerebrovascular disease, respiratory disease, cancer, or mental illness; and (S) were published as a systematic review and/or meta-analysis.
Articles that dealt with animals, children and adolescents were excluded. Reviews that examined circadian disruption or diagnosed sleep disorders (e.g., insomnia) were also excluded. Literature reviews, narrative reviews, clinical trials/studies and case reports were also excluded.
Data Extraction
The data extraction process was carried out independently by two authors (ASS and MRP), with a third author (TB) responsible for conducting a thorough data check. The information extracted from the reviewed studies encompassed several key aspects: details about the study authors and publication date; sleep information categorized as short sleep (<7 h); risk measures including relative risk (RR), odds ratio (OR), hazard ratio (HR), standard mean difference (SMD), effect size (ES), or weighted mean difference (WMD); and the heterogeneity (I2 statistic) to assess the consistency of the study findings. Additionally, data were stratified based on age, with specific subsets for participants under 65 years and above 65 years, including their respective I2 statistics. Gender-based data were also extracted, with separate risk measures and heterogeneity statistics for males and females.
Quality Assessment
Quality Assessment of the Twenty-Six Included Studies, According to the Quality Assessment of Systematic Reviews and Meta-Analyses Tool Developed by the National Heart, Lung, and Blood Institute Tool.
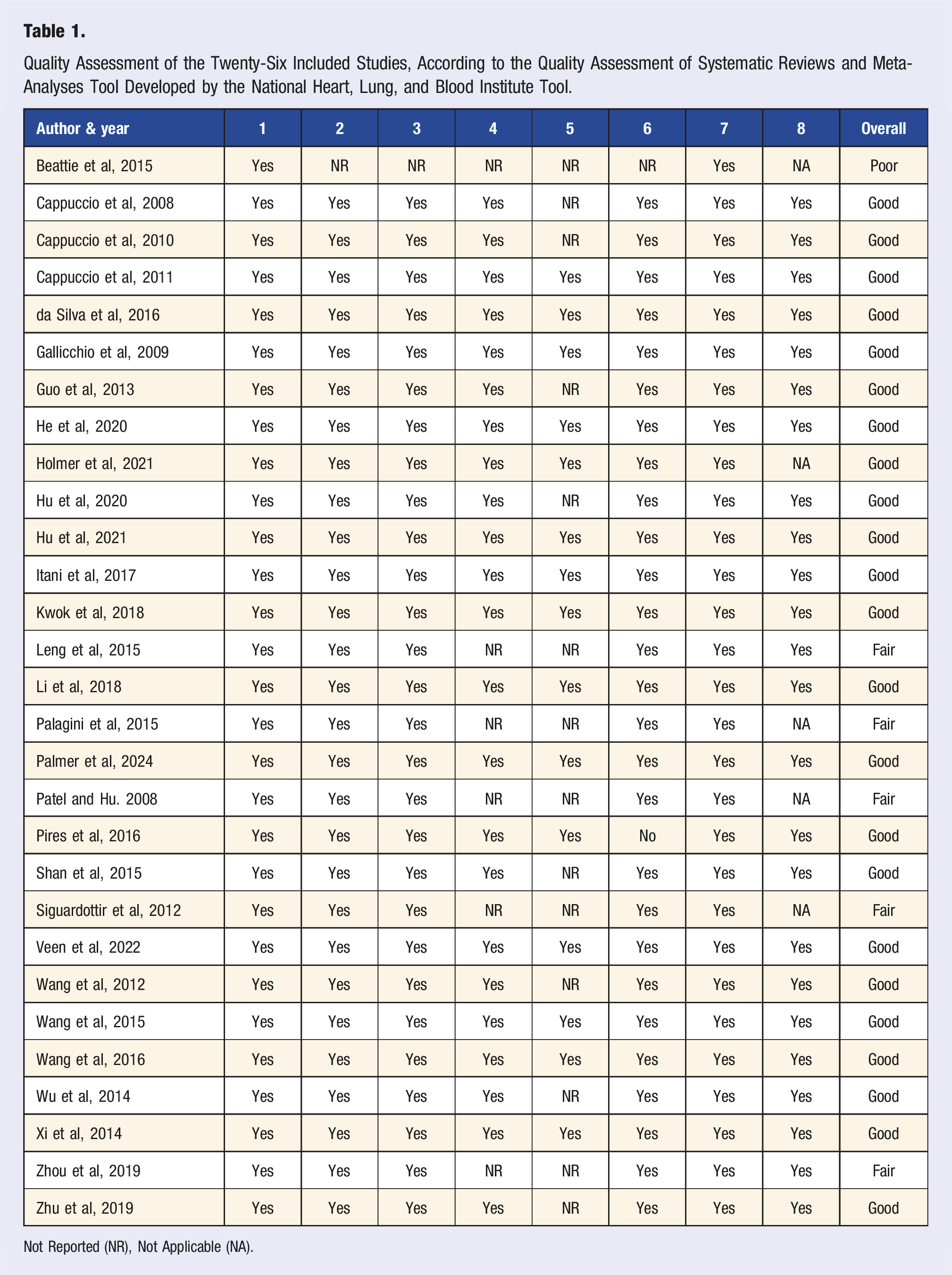
Not Reported (NR), Not Applicable (NA).
Research Questions
As research questions are an important factor for expressing the intent of an umbrella review, five research questions were defined for this umbrella review: 1. Research Question 1 (RQ1) - How many systematic reviews have been published that explored the topic of sleep and health? 2. Research Question 2 (RQ2) - What is the association between SD and all-cause mortality? 3. Research Question 3 (RQ3) - What is the relationship between SD and incidence of cardiovascular diseases (CVD)? 4. Research Question 4 (RQ4) - What is the association between SD and metabolic syndrome? 5. Research Question 5 (RQ5) - What are the effects of SD on mental health?
Results
(RQ1) - How Many Systematic Reviews And/Or Meta-Analyses Have Been Published that Explored the Subject of Sleep and Health?
Twenty-nine manuscripts met inclusion criteria, and these were published between the years 2008-2024. The twenty-nine reviews covered a wide range of health outcomes: seven articles investigated effects of SD on mortality, ten articles investigated effects of SD on CVD, five articles investigated effects of SD on mental health, 7 articles investigated effects of SD on metabolic diseases.
(RQ2) - What is the Association Between SD and All-Cause Mortality?
Impact of Sleep Deprivation on All-Cause Mortality and Other Related Mortality: Relative Risk (RR) and Confidence Intervals (CI), Subclassified by Age (18-65 years and 65+ Years), Gender (Male and Female), Heterogeneity (I2 Statistic) and * Indicates P < 0.05.
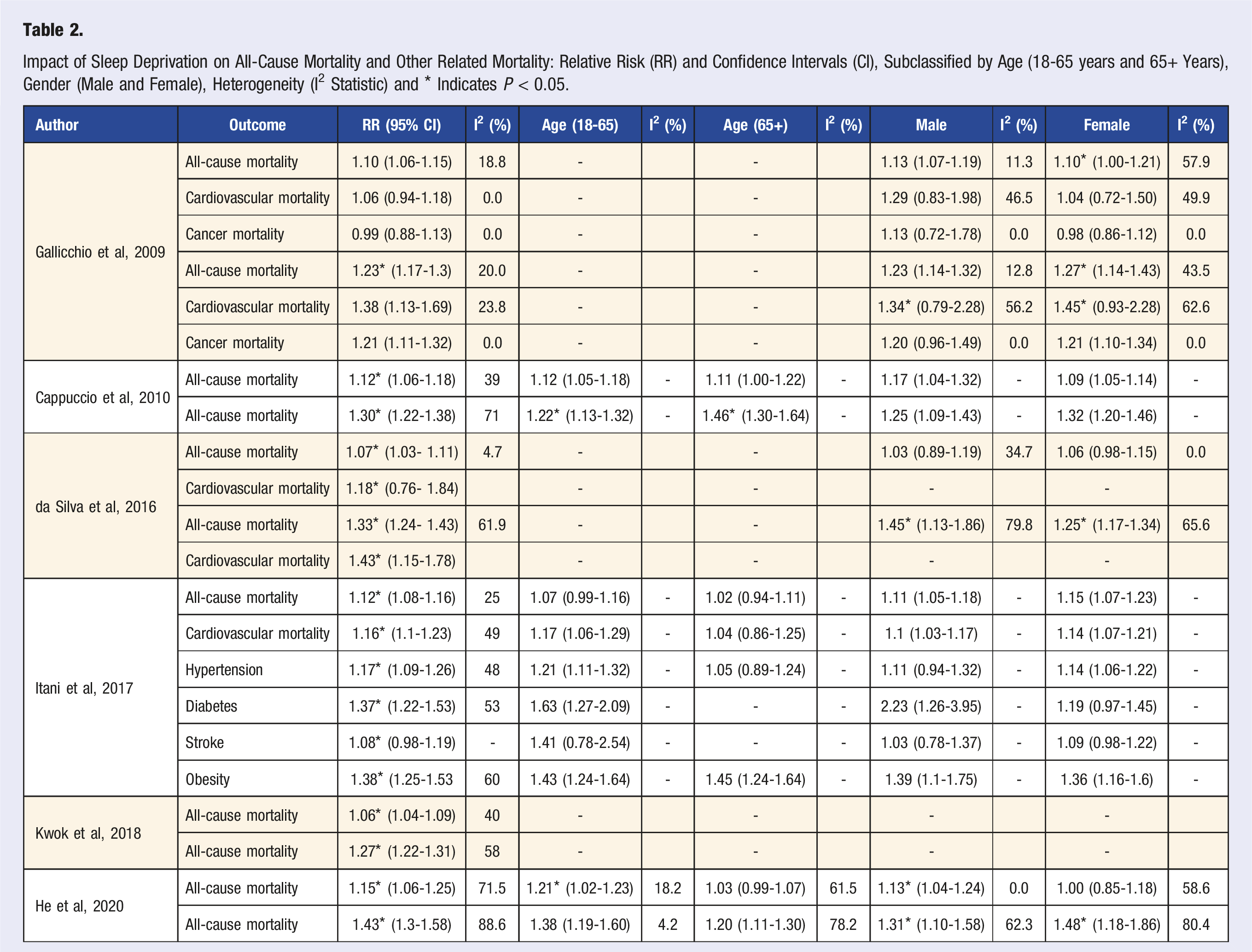
Health outcomes include cancer, diabetes mellitus and cardiovascular diseases like coronary heart disease. There was an increased risk of prostate cancer if sleep was reduced below 6 h per day. Reduced melatonin secretion and circadian rhythm disruption lead to an increased cancer of risk. 34 Short sleep presented increased mortality risk in both the sexes, but the effect of short sleep on diabetes mellitus showed a significant increase in males. 35 Also, males were at a higher risk of all-cause mortality than female when short sleep was reviewed. 14
(RQ3) - Does SD Increase Incidence of Cardiovascular Diseases?
Impact of Sleep Deprivation (SD), Coronary Heart Disease (CHD), Cardiovascular Disease (CVD) and Hypertension (HTN): Relative Risk (RR), Odds Ratio (OR), Weighted Mean Difference (WMD) and Hazard Ratio (HR) and Confidence Intervals (CI), Subclassified by Age (18-65 years and 65+ Years), Gender (Male and Female), Heterogeneity (I2 Statistic) and * Indicates P < 0.05.
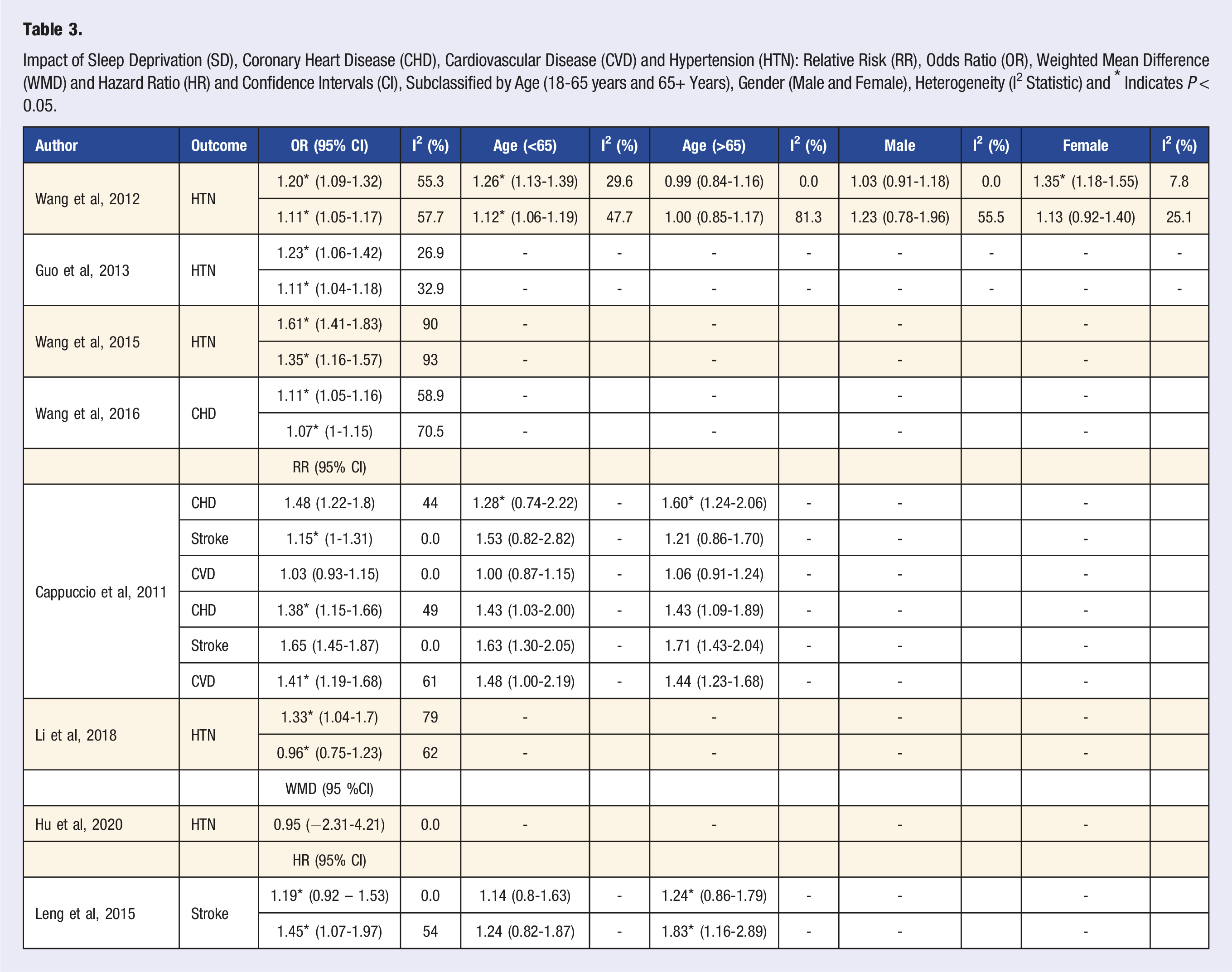
Research has extensively focused on hypertension as a primary cardiovascular outcome influenced by SD. The reviews consistently show that individuals experiencing insufficient sleep are 1.2 to 1.61 times more likely to develop hypertension compared to those who get sufficient sleep.20,37-39,41-43 The impact of SD on hypertension varies based on factors such as age, gender and lesser duration of sleep. 17 Individuals under 65 years old face a 1.26 times higher risk of developing hypertension with chronic SD, while females are at a 1.35 times higher risk. 20
Endothelial function is not a variable that was studied by many articles. 45 SD appears to impair both micro and macro-vascular endothelial function. The exact association between the two and degree of impairment is not clear.
The risk of both fatal and non-fatal stroke tends to increase by 15-19 % with SD compared to sufficient sleep. Additionally, SD was associated with an elevated risk of ischemic stroke.
(RQ4) - How is SD Linked to Metabolic Syndrome
Impact of Sleep Deprivation on Metabolic Syndrome, Obesity and Diabetes: Relative Risk (RR), Odds Ratio (OR) and Confidence Intervals (CI), Gender (Male and Female), Heterogeneity (I2 Statistic) and * Indicates P < 0.05.
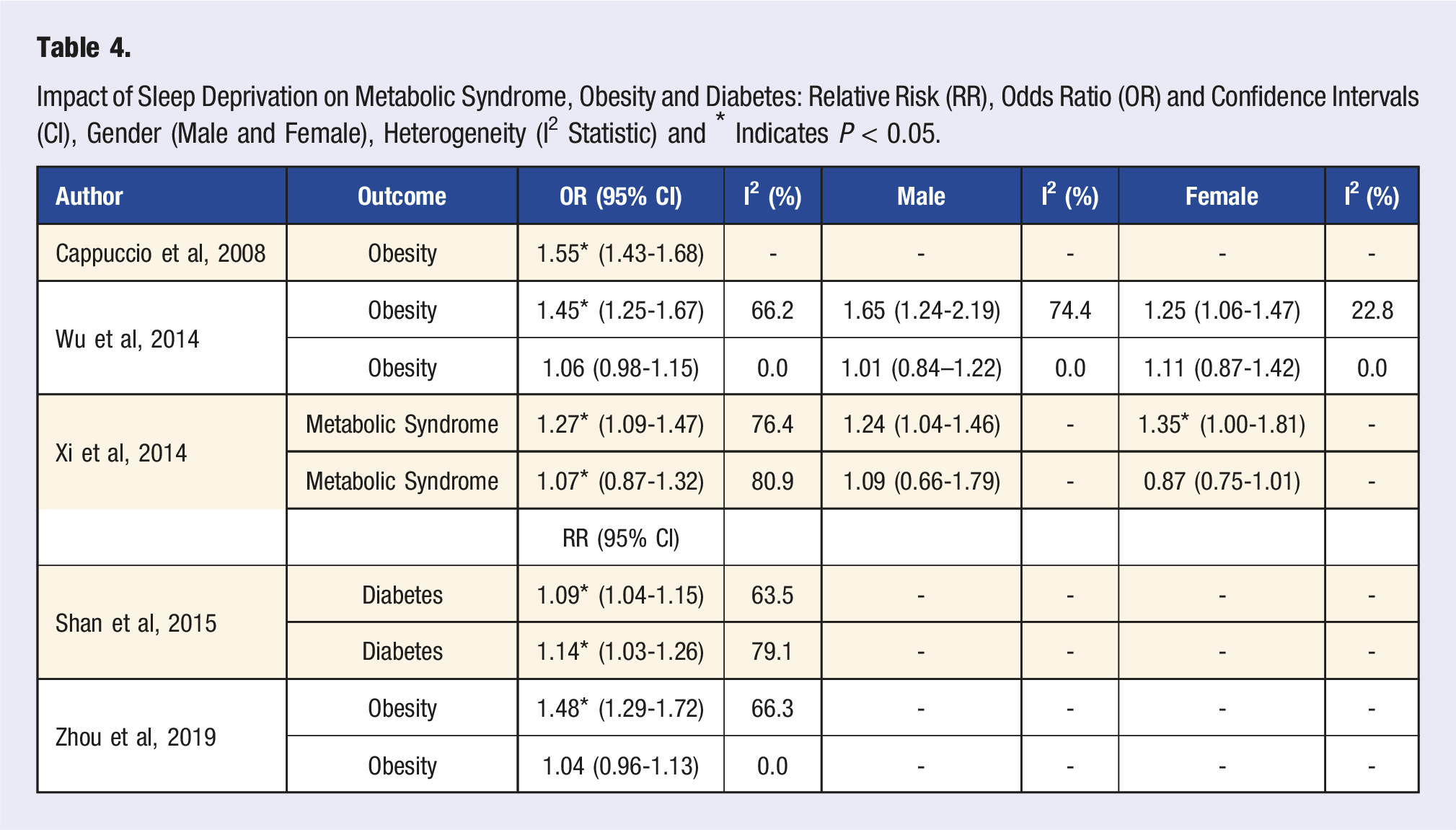
Two reviews identified a U-shaped relationship between sleep duration and the risks of obesity and type 2 diabetes.47,48 Conversely, Zhou et al. (2019) observed a reverse J-shaped curvilinear relationship between sleep duration and obesity risk. 23 They found that shorter sleep durations both increased the risk of obesity compared to normal sleep patterns. 23 Specifically, individuals experiencing SD were 1.45 to 1.55 times more likely to be obese than those with normal sleep patterns.17,46 Moreover, chronic SD was associated with a 9 % higher risk of developing diabetes compared to individuals with normal sleep patterns. 48
Apart from the parameters mentioned above, it was pointed out that SD was associated with suppressed leptin and elevated ghrelin levels. 47 SD was associated with an increased hunger level, caloric intake (especially carbohydrates), increased neuronal activity in the brain to food-related stimuli, reduced insulin sensitivity, and increased insulin resistance. 23
(RQ5) - What are the Effects of SD on Mental Health?
Impact of Sleep Deprivation (SD), and Sleep Restriction (SR) on Anxiety, Aggression, Depression: Effect Size (ES), Odds Ratio (OR), Standard Mean Difference (SMD), Confidence Intervals (CI), Heterogeneity (I2 Statistic) and * Indicates P < 0.05.
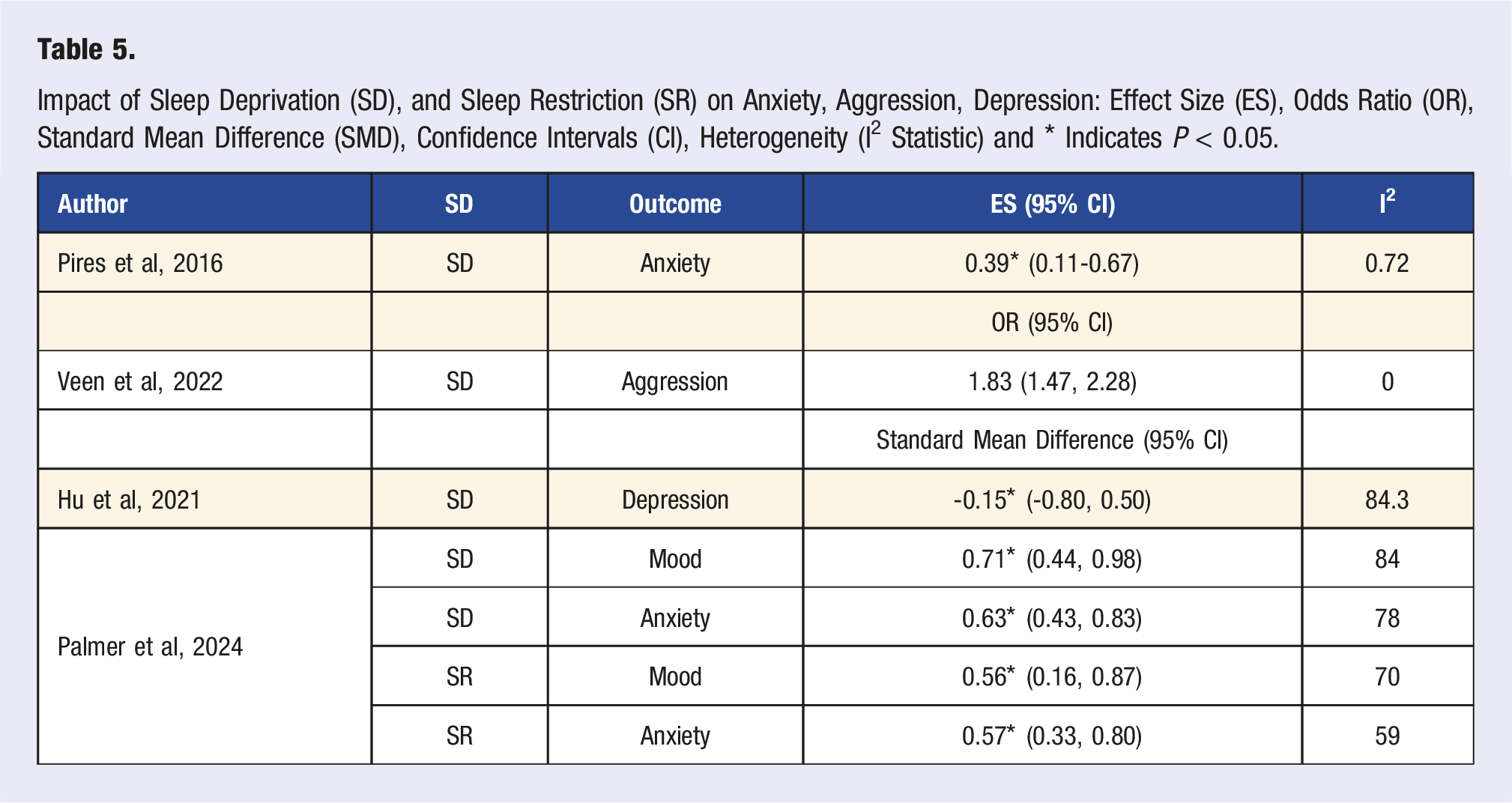
Studies reviewed the effect of SD on emotional stability and found that it led to significant changes in emotional instability and dysregulation.9,27-29 SD significantly impacted individuals' ability to process and respond to emotional stimuli. 27
Quality Assessment
Twenty-nine articles underwent independent quality assessment and were graded good, average, or poor (Table 1). Out of total 232 items, there was conflict in 26 items (11.2 %), which was subsequently resolved by the third reviewer (TB). The quality assessment of various systematic reviews and meta-analyses on sleep and health reveals that the majority (23 out of 29) are of “Good” quality, demonstrating high methodological rigor and reliability. Five reviews received a “Fair” rating, indicating they met most criteria but failed to report whether two independent reviewers carried out screening and quality assessment. Only one study was rated as “Poor,” as it failed to report the methodological process and quality assessment showing significant shortcomings. 9 Overall, the assessment indicates that most research in this area is robust and reliable. However, a few reviews could improve in specific methodological aspects, particularly in detailing the independent screening process and the risk of bias. One article was found to not have an adequately described research question. 9 This was due to lack of reporting of quality assessment and failure to elaborate on reviewing methods.
Discussion
In this umbrella review of twenty-nine reviews, a consistent negative trend was observed when the effects of SD were observed on physical and mental health. These health outcomes were primarily categorized into four types—all-cause mortality, cardiovascular disease (including hypertension, stroke and coronary heart disease), mental disorders (anxiety, emotional dysregulation), and metabolic syndrome (diabetes mellitus and obesity) (Figure 2). Deviation from the recommended sleep hours poses a health risk depending on age. However, SD was more detrimental in almost all the health outcomes included in this review, except for the risk of stroke. Potential mechanisms influenced by sleep deprivation (CVD, Cardiovascular Disease; CHD, Coronary Heart Disease; HTH, Hypertension).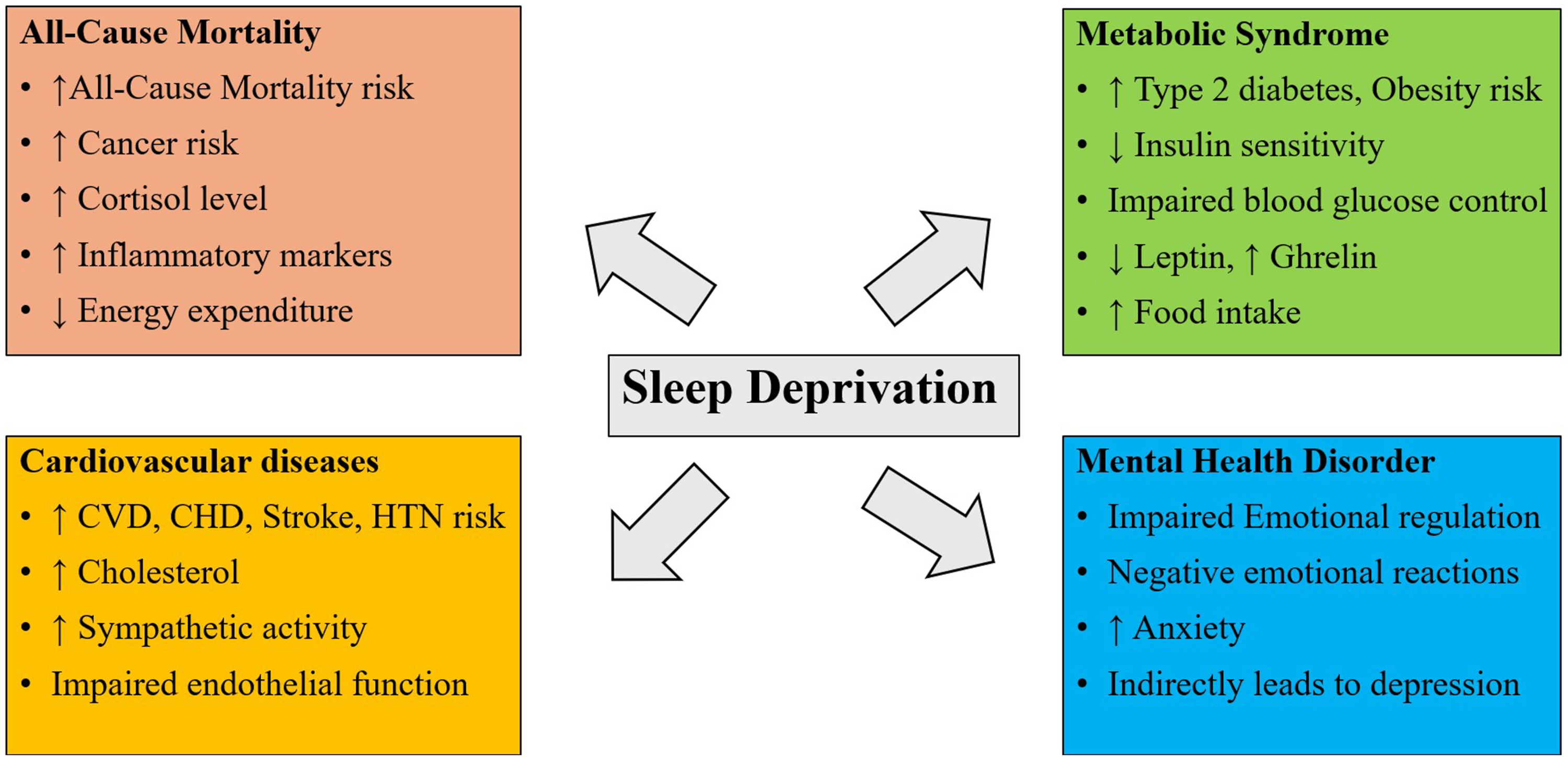
Results for the relationship between all-cause mortality and SD showed that short sleeping populations are at risk compared to individuals with an average amount of sleep. 13 Although the definition of regular sleep hours varied in the studies and age, the hours seemed to lie in the same spectrum (7-9 h).12,14 Sleeping less than 5 h per night had a 12 % higher risk of all-cause mortality. 12 Most reviews had a U-shaped curvilinear correlation between sleep duration and all-cause mortality. However, Kwok et al, 36 observed a J-shaped relationship in their study. This pattern may be attributed to the elderly population they studied, where the prevalence of shift work and extended work hours is low.49,50 SD leads to increments in the all-cause mortality related parameters, which included—37 % in type 2 diabetes, 17 % for hypertension, 16 % for CVD, 26 % for coronary heart disease and 38% for obesity. 35 These conditions put an individual at an increased risk of SD. Although they may not directly impact the outcome of all-cause mortality, their possible influence on the quantity of sleep cannot be discounted. The mechanisms leading to the rise in all-cause mortality are—increased cortisol levels, increased sympathetic nervous system activity and low-grade inflammation linked to CVD and cancer.12,14 One study focused primarily on cancer risk and reported circadian and melatonin disruption to be a leading cause of prostate cancer in males and breast cancer. 34 Socio-economic status also can impact the incidence of mortality as people have to work multiple shifts and working longer hours can significantly reduce sleep duration. 51
The impacts of SD on CVD are varied, but it is evident that SD has negative consequences on cardiovascular health.20,37-39,41,42,48 Research has shown that sleep duration of less than 7 h per night increases risk, one of them being coronary heart disease (CHD). The risk of CHD increases by 11 % for a decrease of one hour of sleep below the recommended range. This finding is consistent across both males and females. The exact mechanism behind this has not yet been clearly defined, but SD creates a host of cardiovascular risk factors—like elevated lipid profile, high-sensitivity c-reactive protein, tissue plasminogen activator and other, which are likely to lead to CHD.37,41,52 SD results in elevated ghrelin levels and reduced leptin levels. 18 Consequently, appetite increases and causes increased caloric intake, weight gain, decreased energy expenditure and the development of obesity. In the long term, it is common for blood glucose control to decrease and cholesterol levels to increase. As a result, the risk of calcification and atherosclerosis contributes heavily to the development of CHD. 52
Another consequence of SD that was studied was the risk of fatal and non-fatal stroke.37,40 SD, had a more statistically significant impact on the increase of stroke risk (18 %). SD was linked to an increase in risk of ischemic stroke through, and this was more pronounced in middle-aged populations. As mentioned above, the exact mechanisms are unclear, but impaired metabolism, increased dietary intake, increased cholesterol levels, sympathetic activity and increase in inflammatory markers might be behind the increase in stroke risk. 41
Another factor that contributes to CVD is endothelial dysfunction.45,53 SD was found to impair both microvascular and macrovascular endothelial function. There are several pathways through which this dysfunction occurs. Inflammation and oxidative stress were a significant driver change in endothelial function. 53 Due to the absence of normal dips in blood pressure that occurs during regular sleep, the endothelium is activated causing an increase in inflammatory markers, reactive oxygen species and coagulation factors. 16 This in turn restricted the effects of nitric oxide, an important vasodilator. Combined with chronobiological disruption and sympathetic nervous system stimulation, this leads to vascular aging and consequently endothelial dysfunction. 53
The effects of SD on blood pressure and incidence of hypertension is widely studied. SD is accompanied with an increased risk of hypertension.20,37-39,41-43,48 All the mechanisms previously listed above contribute to an overall increase in blood pressure.16,21 Interestingly, exercise has the potential to negate some of the ill-effects of SD on cardiovascular outcomes. Further research is needed to shed light on exercise being a useful intervention and mitigator to the effects of SD.
Short sleep duration has been identified as a contributing factor to the development of atrial fibrillation (AF), a major risk factor for stroke. Evidence suggests that insufficient sleep is associated with an increased duration and incidence of atrial fibrillation. 54 Moreover, short sleep duration exacerbates risk factors such as obesity, diabetes, and hypertension, all of which further contribute to atrial fibrillation development and, subsequently, stroke risk.
Metabolic syndrome also presented with similar results with short sleep (<5 h a day). Increased likelihood of obesity, hypertension and diabetes mellitus were primarily included under metabolic syndrome. A U-shaped relationship was presented between diabetes and sleep duration, with the lowest risk of diabetes at 7 to 9 h of sleep.16,48 One study showed a reverse J-shaped relationship between sleep duration and obesity. 23 Individuals sleeping fewer hours are likely to be more fatigued during the day and are less likely to participate in physical activity; this could be a leading cause of increased adiposity in such individuals. However, we cannot conclusively determine the extent to which sleep influences physical activity, as this specific relationship falls outside the scope of this review. Dietary habits also are to be kept in mind as short sleepers are prone to late-night snacking, which may further increase caloric intake for the day. Snacks generally are calorie-dense foods, that predisposes individuals to metabolic dysfunction. 47 The hormonal differences in individuals also play a role, especially in female. In middle-aged female, menopausal symptoms play a crucial role in the relationship between sleep and obesity. 17 The mechanisms that facilitate the increased incidence of diabetes mellitus are—reduced glucose tolerance and insulin sensitivity, increased sympathetic activity leading to reduced beta-cell responsiveness and reduced insulin secretion. 48 Human adipocytes can also become insulin resistant as a result of reduced sleep. An increase in serum ghrelin and reduction in leptin levels may lead to obesity in individuals. 18 SD caused an overall decrease in the brain regions responsible for decision making. 19 This could be one of the reasons behind late-night snacking and the choice of food that is consumed. There is an increase in cortisol levels by activating the hypothalamus-pituitary-adrenal axis. 23 This, in turn, results in increased food appetite and weight gain.
The negative effects of SD extend beyond physiological impairments to significantly impact mental health outcomes. SD has been found to have an anxiogenic effect, leading to increased anxiety levels in individuals. 30 This may be attributed to heightened amygdala activity, a key region involved in emotional processing, which has been observed in sleep-deprived individuals.55,56 Increased amygdala reactivity, combined with impaired connectivity with the prefrontal cortex, can lead to heightened emotional responses and reduced emotional regulation, further exacerbating anxiety symptoms. Beyond anxiety, SD impairs an individual’s ability to regulate emotions, often leading to difficulty in emotional recognition and response.9,57 Sleep-deprived individuals exhibit a reduced ability to accurately interpret emotions from facial expressions. 58 Additionally, SD affects emotional expression, making it more challenging for individuals to convey emotions through facial expressions and vocal descriptions. 58 These impairments in emotional perception and expression may contribute to increased irritability, impatience, and difficulties in social interactions.9,30 Moreover, SD is associated with heightened aggression and mood disturbances, reinforcing the broader impact of sleep loss on emotional stability. Individuals experiencing SD report increased impulsivity, frustration, and difficulty in controlling negative emotions, which may contribute to interpersonal conflicts.9,30 These behavioral changes may explain why SD has been linked to increased relationship difficulties, including heightened marital conflicts and negative social behaviors. 26 While SD has also been associated with the development of depression, the exact nature of this relationship remains unclear. Some evidence suggests that chronic SD may contribute to depressive symptoms through disruptions in neurotransmitter systems, such as serotonin and dopamine, which play crucial roles in mood regulation. 59 However, further research is needed to clarify the causal link between SD and depression and to determine whether SD acts as a precursor or an exacerbating factor for depressive disorders. The broad mental health consequences of SD emphasize the need for further research to explore its long-term effects, particularly on emotional regulation, aggression, and social interactions. Future studies should also investigate potential interventions to mitigate these negative outcomes and improve overall well-being in sleep-deprived individuals.
A constant limitation in all the reviews was that the data was gathered through subjective or self-reported questionnaires. These methods can be inaccurate as time spent in bed can be synonymous with time spent sleeping. Subjective methods can be inaccurate as individuals average their sleep duration throughout the week, especially for those who tend to have varying sleep duration on weekdays and weekends. 60 Failure to factor daytime naps can also influence the findings of the reviews. Also, sleep quality was not measured/monitored in all the reviews. Even if someone sleeps for what is considered an adequate duration, they may still wake up feeling unrested and fatigued because the actual time spent sleeping can differ from the total time spent in bed. 61 Moreover, the duration of Rapid Eye Movement and Non-Rapid Eye Movement phases can influence the overall quality of sleep, cognitive function, emotional regulation, and susceptibility to various health issues. Sleep journaling can be a beneficial subjective method, and it can be more accurate than self-reported timings that are not logged in a journal. Reviews also did not factor in physical activity and other lifestyle parameters which can influence sleep. 62 While this review focuses on sleep deprivation as a distinct entity, it does not specifically address sleep disorders such as sleep apnea and insomnia, which can contribute to sleep fragmentation and reduced sleep duration through different physiological mechanisms.
Conclusion
In this umbrella review of twenty-nine reviews, SD consistently demonstrated detrimental effects across various health outcomes, including all-cause mortality, cardiovascular diseases (including hypertension, stroke, and coronary heart disease), mental disorders (such as anxiety and emotional dysregulation), and metabolic syndrome (including diabetes mellitus and obesity). SD has more detrimental effects on most health outcomes. SD tends to have a more pronounced negative impact on health outcomes in male compared to female, particularly for conditions like obesity and hypertension. Additionally, younger individuals (under 65) are more adversely affected by SD compared to older adults, especially in terms of all-cause mortality and cardiovascular disease. This synthesis underlines the need for public health interventions and practice guidelines to mitigate the adverse effects of SD and promote optimal sleep health.
Implications for Health care Practitioners, Policymakers, and Public Health Interventionists
The findings underscore the critical role of sleep in health outcomes, providing health care practitioners with evidence to advocate for adequate sleep practices. Clinicians can use this information to educate patients about the risks associated with insufficient sleep and promote sleep hygiene measures. Policymakers can develop public health policies that prioritize sleep education and address societal factors contributing to SD, such as work hours and lifestyle. Public health interventionists can implement targeted programs to raise awareness about the importance of sleep and its impact on overall health. By synthesizing high-quality evidence, stakeholders can formulate guidelines and interventions that support healthy sleep patterns and mitigate the adverse effects of SD. This comprehensive approach aims to improve population health by addressing SD related risks and promoting well-being through informed health care practices and public policy initiatives.
Abbreviations
Sleep deprivation
Cardiovascular disease
Coronary heart disease
Footnotes
Author Contribution
Arambh Sanjay Shah: Writing—original draft, Methodology, Mitresh Raj Pant: Writing—original draft, Methodology. Tulasiram Bommasamudram: Writing—review & editing, Methodology, Supervision, Data curation, Conceptualization. Kirtana Raghurama Nayak: Writing—review & editing. Spencer S.H. Roberts: Writing—review & editing. Chloe Gallagher: Writing—review & editing, Methodology. K. Vaishali: Writing—review & editing. Ben J. Edwards: Writing—review & editing. David Tod: Writing—review & editing. Fiddy Davis: Writing—review & editing. Samuel A. Pullinger: Writing—review & editing, Methodology, Supervision, Conceptualization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.