
Abstract
Objective. The aim of this study was to identify lifestyle habits that contribute to night sleep reduction in the Kuwaiti population. Methods. Children were 10 to 12 years old and were approximately equally distributed among 138 elementary schools representing the 6 governorates of Kuwait. In the first phase of the study, data were collected from 8317 children. The same data were collected 2 years later from 6316 of the children from the first phase of the study. Calibrated examiners conducted sleep evaluation, lifestyle habits interviews, and body weight measurements. A multilevel random intercept and slope model was conducted to determine the effect of screen-based activities on the daily night sleep hours at 3 levels: within schools, among children, and over time. The primary dependent variable was the number of daily sleep hours. Independent variables assessed were lifestyle habits including screen-based activity variables including TV and video game use. Results. Screen-based activities were significant factors that reduced daily sleep hours (P < .05). There were statistically significant variations between schools and children over time. Conclusion. Longitudinal analysis of Kuwaiti children revealed that TV and video game use were major risk behaviors contributing to decreased sleep duration with strong clustering effect of the observations within schools across time.
Keywords
‘Current evidence shows that children who sleep less at night have a significantly higher risk of becoming obese than children who sleep longer.’
It has been recently recognized that healthy sleep patterns play a fundamental role in improving overall health. Current evidence shows that children who sleep less at night have a significantly higher risk of becoming obese than children who sleep longer.1,2 Consistent delayed night sleep has been shown to increase the risk and the severity of infectious diseases, cancers, respiratory diseases, and depression. 3 Similarly, little and disrupted sleep is related to costly metabolic diseases.4-7 Metabolic diseases in Kuwaiti children is a growing problem, where, according to the International Diabetes Foundation, every fourth adult has type 2 diabetes 8 and by our data every fourth 10-year-old child is obese. Given the high prevalence of obesity in Kuwaiti children, there are serious health implications for these children as they reach adulthood, given the fact that overweight in children is a predictor of obesity in adulthood. 9 Kuwaiti children had a larger proportion of obese children than American children among the same age groups.10-13
The aim of the present analysis was to identify the risk behaviors related to delayed night sleep among a population having the highest prevalence of obesity in the world—the Kuwaiti population. 14 Previous work has determined a significant relationship between insufficient sleep and obesity among Kuwaiti children. 13 This study also demonstrated that screen-based activities (TV and video game use) are major risk factors contributing to diminish sleep time. 13 However, it is important to keep in mind that this previous analysis used a cross-sectional design, which has its inherent limitations. The prospective longitudinal design of this study allows us to evaluate the changes of behaviors over time, to determine the trend of the observations and their contribution to the outcome. In other words, cross-sectional studies based on one single observation are not appropriate to determine the effect of behavior on changing the outcome. It is essential to follow behavior over time using multiple observations to determine a causal relationship to the outcome. 15 Moreover, multilevel modeling accounts for the clustering effect between schools and the variation between children to provide a more precise and correct inference. 16
Materials and Methods
Study Approval
This prospective cohort study was approved by the Forsyth Institutional Review Board in Cambridge, MA, and the Dasman Institute Human Ethical Review Committee in Kuwait (RA/065/2011 and RA/005/2011). Informed consent forms in Arabic language were provided to parents (or guardians) and assent was required from the children. Assent was obtained on the day of the study visit before participation in the study. Written consent forms were collected and securely stored at the School Oral Health Program in Kuwait.
Study Population
In the first phase of the study, data were collected from 8317 children representing the 6 governorates in Kuwait between October 2011 and May 2012. The Kuwaiti participants were in the fourth and fifth grades, and their ages ranged between 8 and 11 years in 2012 (visit 1) for this initial screening. The final data collection occurred between October 2014 and May 2015, where the same data were collected from the same cohort of children (n = 6316) representing 138 public schools in Kuwait (visit 2). The response rate for the second round was high (95%). There were 2001 children from visit 1 who were unable to follow-up by the second examination visit due to the approaching end of the academic year. In the analysis for this article, we included only the 6316 subjects who had complete measurements at both visits. In this data set, the distribution of participants across the 6 governorates of Kuwait was approximately equal. Students enrolled in these schools represented all socioeconomic levels and ethnic groups among the Kuwaiti population, but did not include expatriate children. All volunteer participants were accepted but selection into the cohort was not randomized across the population.
Data Collection
Subject identification, sleep evaluation interviews, saliva samples, nutrition analysis interviews, and body weight analysis were collected by 2 calibrated teams. Information on these variables was recorded into a programmed iPad (Apple, Cupertino, CA) system for Internet transfer.
Outcome Measure
Sleep Duration
The primary outcome in the present analysis was daily sleep hours. Each child was asked the following: (1) During the past week, at what time did you go to sleep? (2) During the past week, at what time did you wake up? Based on the responses, the number of sleep hours per day was calculated for each child.
Independents Variables
These variables were assessed and obtained from “one-on-one” interviews with each child by calibrated interviewers. Tables 1 and 2 demonstrate the tested variables and their descriptions. Questions about sleep behavior and lifestyle habits were answered using ordinal responses (never, rarely, sometimes, often), or continuous variables (ranging from 0 to 7) in the multilevel modeling, and answers choices were the following: never, 1 day a week, 2 days a week, 3 days a week, 4 days a week, 5 days a week, 6 days a week, or every day.
Variables and Corresponding Sleep Quality Questions a .
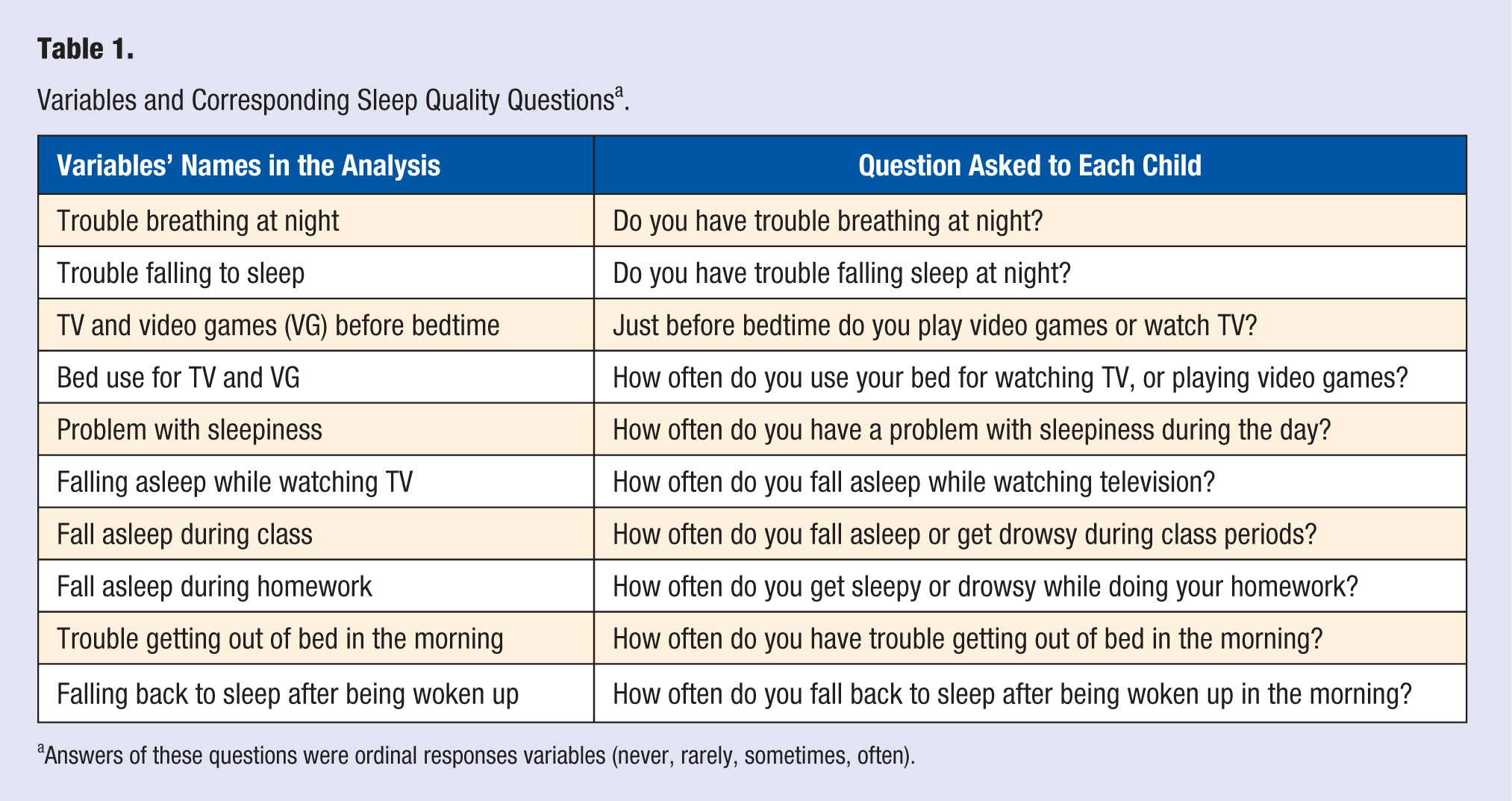
Answers of these questions were ordinal responses variables (never, rarely, sometimes, often).
Variables and Corresponding Questions of Lifestyle Behaviors.
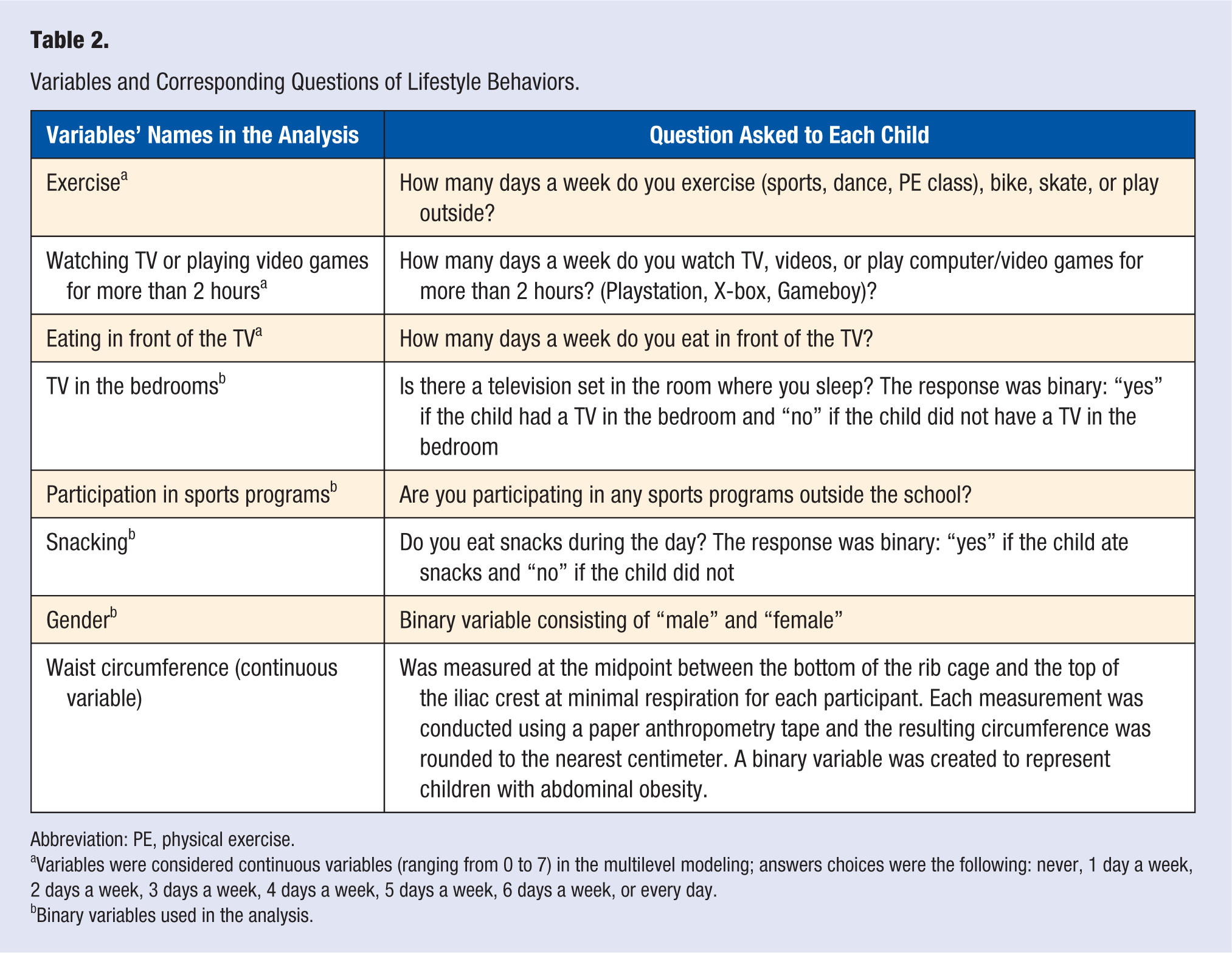
Abbreviation: PE, physical exercise.
Variables were considered continuous variables (ranging from 0 to 7) in the multilevel modeling; answers choices were the following: never, 1 day a week, 2 days a week, 3 days a week, 4 days a week, 5 days a week, 6 days a week, or every day.
Binary variables used in the analysis.
Information on these variables was recorded into a programmed iPad (Apple, Cupertino, CA) system for Internet transfer.
Statistical Analysis
Our data had a hierarchical structure composed of time (first level), nested within children (second level), and nested within the schools (third level; Figure 1). Level 3 represented the contextual effect of the school environment on the outcome. We fit the data using multilevel longitudinal linear regression model to determine the linear relationship between sleep duration and the individual-level variables to verify which individual factors were associated with the outcome over a period of 2 years.
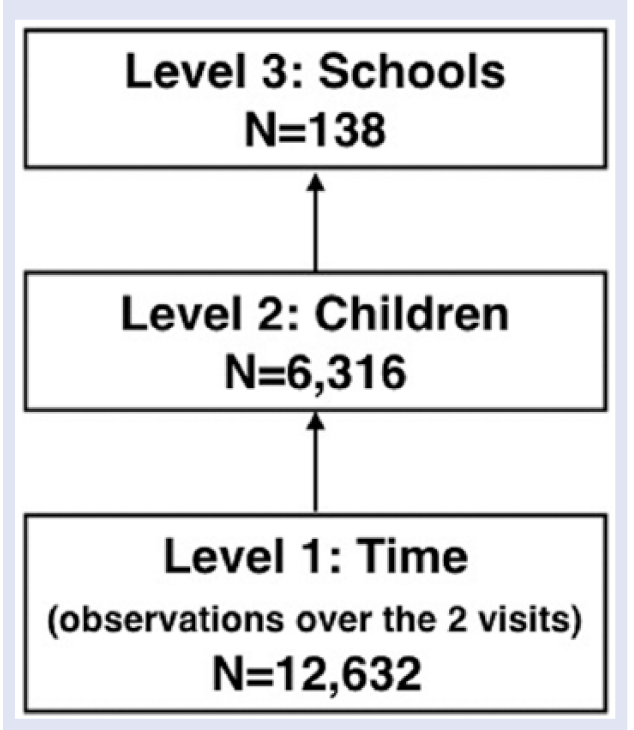
Schematic representation of the 3-level hierarchical structure of the final analytic sample.
Variable selection was based on clinical relevance and potential confounding. We used the stepwise model building strategy. We kept the significant variables in the final model. Beta coefficients for the linear model and their 95% confidence intervals were estimated at a predetermined significance level of α = .05. As is often done with multilevel models, we computed the intraclass correlations (ICCs) at each level. ICCs represent the amount of variability in the outcome attributed to each level, after accounting for other variables in the regression models. The statistical analysis modeling was conducted in MlwiN. MLwiN is a statistical software package for fitting multilevel models (Centre for Multilevel Modeling, University of Bristol). Using the prospective longitudinal multilevel design in this study increases the analysis precision by accounting for the clustering within schools, and clustering of the observations between the 2 time points. 16
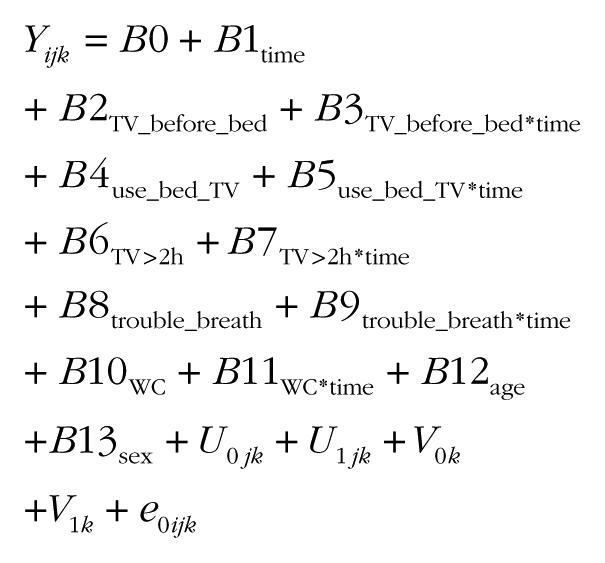
The final model is shown below:
Results
There were more girls (61.4%) in the study than boys (38.5%). The age of children was tightly clustered around 10 ± 0.008 years in visit 1 and around 12 ± 0.008 years in visit 2. On average, both boys and girls slept 8.8 hours/day, with an average bedtime occurring at 10:00
The population’s descriptive statistics for the lifestyle habits are summarized in Table 3. We noticed a considerable increase in the use of screen-based activities over time in this population. A total of 43.4% of Kuwaiti children in this study have a TV in their bedrooms, with boys more likely to have a TV (56.2%) than girls (35.3%). Most Kuwaiti children (86.7%) watch TV and play video games just before bedtime; once again, this is more commonly found to be a habit of boys (88.7%) than girls (85.5%). Most children (59.5%) watch TV and play video games for more than 2 hours a day (4 days a week or more), more commonly for boys (62.2%) than girls (59.6%). Most children (58.4%) eat in front of the TV (4 days a week or more), with more girls exhibiting this behavior (63.2%) than boys (57.7%). The use of the bed for watching TV and playing video games was reported by 50% of the children, with girls (53.5%) more likely to do so than boys (46.3%). Only 30% of Kuwaiti children reported that they practice exercises 4 days a week or more, with the higher proportion among boys (37%) than girls (24.6%). A small percentage of the children reported having trouble breathing at night (12.4%), which was more common in boys (13.6%) than in girls (12.4%).
Summary Descriptions of Lifestyle Habits Stratified by Sex and Visit.
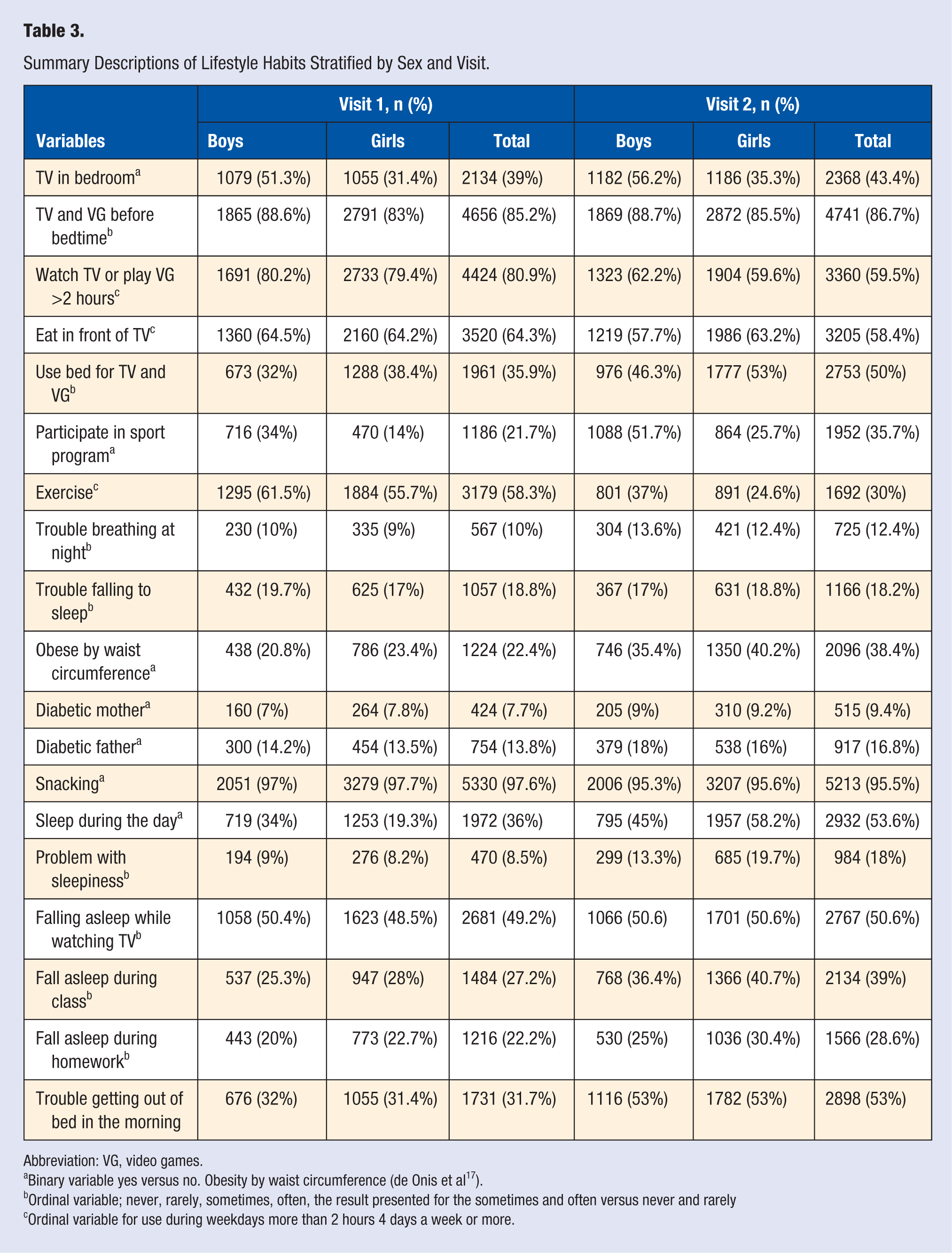
Abbreviation: VG, video games.
Binary variable yes versus no. Obesity by waist circumference (de Onis et al 17 ).
Ordinal variable; never, rarely, sometimes, often, the result presented for the sometimes and often versus never and rarely
Ordinal variable for use during weekdays more than 2 hours 4 days a week or more.
At visit 1, 7.7% of the children reported that they had a diabetic mother, and 13.8% reported having a diabetic father. At visit 2, the same children reported that 9.4% had a diabetic mother and 16.8% had a diabetic father. This indicated a 4.7% increase in the prevalence of diabetes in parents over the 2 years. These findings confirm the estimated 24% of diabetic adults in Kuwait reported by the International Diabetes Federation. 8 Almost all children (95.5%) acknowledged snacking during the day (Table 3). A big increase in the incidence of childhood obesity over time was observed (obesity by waist circumference in visit 1 = 22.4% and in visit 2 = 38.4%, according the World Health Organization guidelines 17 ).
Results from the multilevel longitudinal linear model showed that the main factors predicting short night sleep duration in children were screen-based activities (Table 4): watching TV or playing video games before bedtime reduced daily sleep hours, with statistically significant change over time (P < .05). Moreover, using the bed for watching TV and playing video games predicted shorter sleep duration over time (P < .05; Table 4). Playing video games or watching TV more than 2 hours a day also reduced daily sleep hours, with statistically significant rate of reduction over time (P < .05; Table 4). Children with bigger waist circumference had less daily sleep hours over time (P < .05), adjusted for age and gender.
Multilevel Longitudinal Linear Regression Model With Daily Sleep Hours as the Outcome Variable.
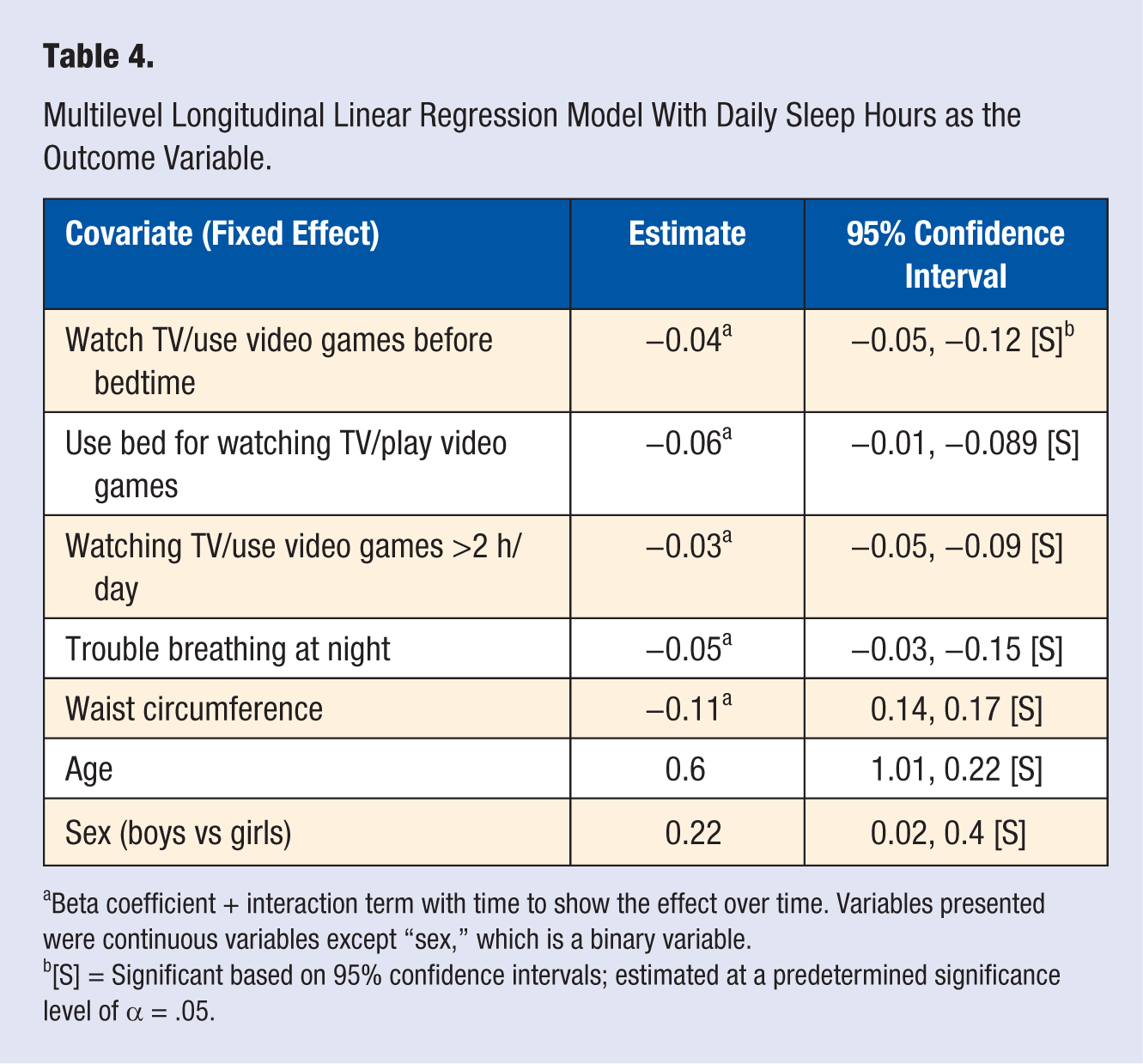
Beta coefficient + interaction term with time to show the effect over time. Variables presented were continuous variables except “sex,” which is a binary variable.
[S] = Significant based on 95% confidence intervals; estimated at a predetermined significance level of α = .05.
For this model, there were statistically significant time variations for both school and children levels, found also in the rate of change in sleep duration across children and schools (Table 5). In the secondary analysis demonstrated in Table 6, we showed that there was a strong clustering effect within schools in the observations of the sleep duration and screen-based activities.
Between School and Children Variation: Random Effect Estimates of the Linear Regression Multilevel Model in Table 4.
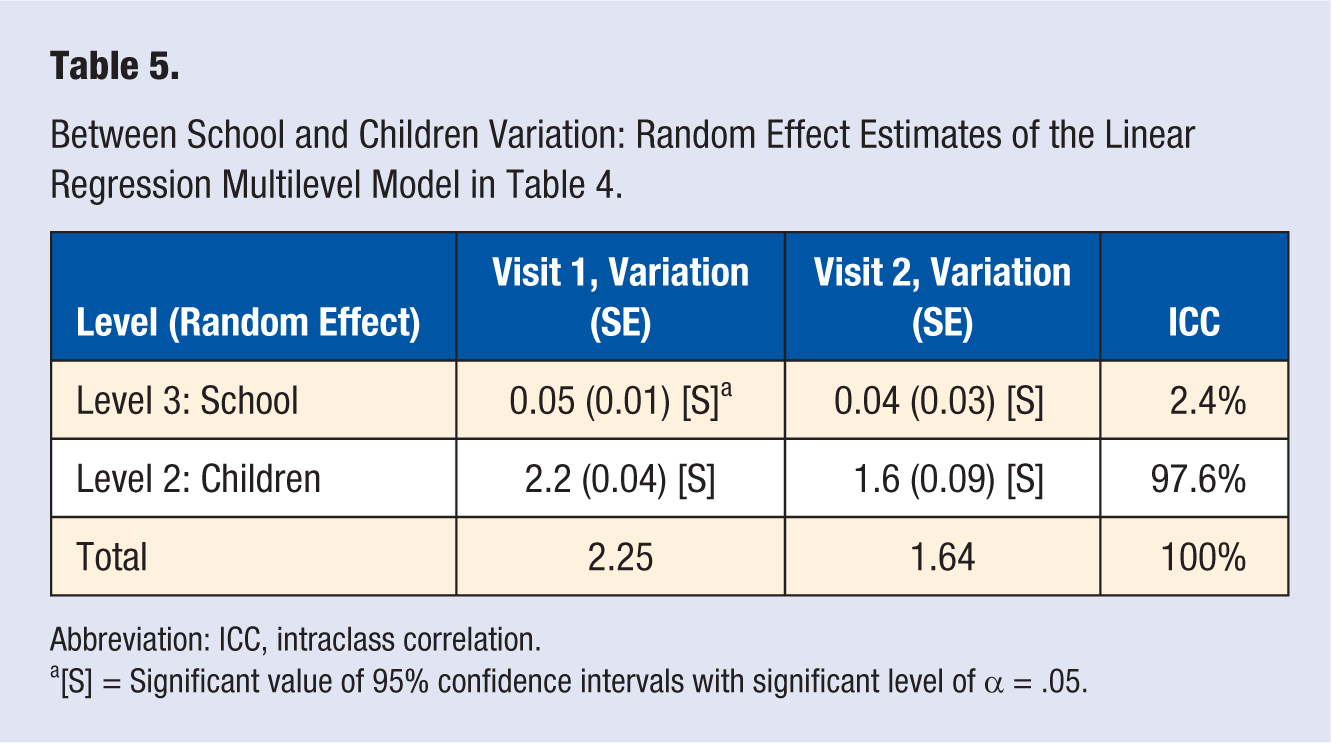
Abbreviation: ICC, intraclass correlation.
[S] = Significant value of 95% confidence intervals with significant level of α = .05.
School-Level Random Effect of Sleep Behavior and Screen Activities Variables a .
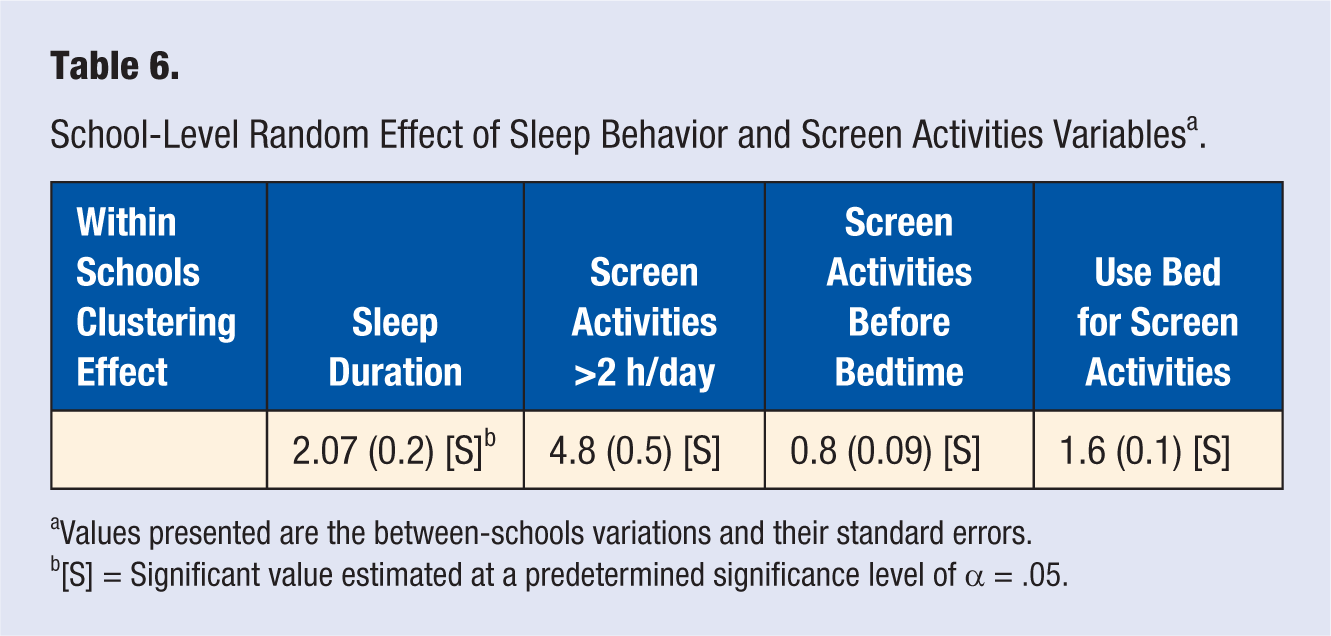
Values presented are the between-schools variations and their standard errors.
[S] = Significant value estimated at a predetermined significance level of α = .05.
Discussion
Our data showed that the mean sleep duration among Kuwaiti children (8.8 hours/day) was less than the minimum required hours for this age group. According to the Centers of Disease Control and Prevention and the pediatric clinical guide for sleep, 18 10 to 11 hours of sleep are considered a healthy average sleep duration for 8- to 12-year-old children. This indicates that there is an issue prevalent in Kuwaiti children in terms of short sleep duration. In addition, a recent meta-analysis showed that sleep duration among Kuwaiti children was comparable to the sleep duration in children of other countries. 19
In the present analysis, we showed that children who frequently watch TV or play video games just before bedtime sleep significantly less than children who rarely or never watch TV or play video games before bedtime, with a significant dose-response relationship over time (P < .05; Table 4). Similarly, children who mostly use their beds for watching TV and playing video games sleep significantly less than children who rarely or never used their beds for these screen-based activities, with a significant dose-response relationship over time (P < .05). We also found that children who watch TV or play video games for more than 2 hours most weekdays tend to sleep less during the weekdays than children who spend less time on screen-based activities, with a significant dose-response relationship over time (P < .05; Table 4). There is a strong body of evidence showing that screen-based activities have significantly contributed to decrease night sleep time. Most important, using the prospective longitudinal design in this analysis, we can infer the causal relationship between screen-based activities and little night sleep among those children. In addition, using this longitudinal multilevel modeling increases the precision of the analysis by accounting for the unmeasured confounders as well as accounting for the clustering within schools, and clustering of the observations between the 2 time points. 16 These findings from the present prospective cohorts ascertain that TV and video games use may be a short sleep duration risk factor that is prevalent in the child population of Kuwait.
Current evidence reported a remarkable decline in night sleep duration in several different populations, with a substantial parallel rise in the prevalence of metabolic diseases in these populations. 20
In this study, a substantial rise in the time spent on screen-based activities was observed over the 2 years. We show that 43.4% of the Kuwaiti children in the study have TVs in their bedrooms (Table 3), and 86.7% watch TV or play video games just before going to bed. In addition, 50% of the children are using their beds for watching TV and playing video games, while only 30% engage in physical exercise most of the weekdays (Table 3). These are alarming findings that may explain the general reduction in the sleep duration among these children. Using electronic devices for long periods can suppress melatonin secretion. 21 It has been suggested that short wavelength light released from electronic devices significantly inhibits melatonin secretion, resulting in both delayed sleep and a diminished quality of the night sleep. 22 A randomized study comparing a group of people who used electronic books with a group who used printed books before bedtime found that individuals who used electronic books sleep fewer night hours and have lower levels of melatonin secretion than the group who used the printed book before bedtime. 23 Melatonin plays an important role in carbohydrate metabolism and insulin regulation. 6 Moreover, it has been shown that short sleep duration and the use of electronic devices are associated with excess body weight. 22
In the present study, screen-based activities were the most significant factors contributing to reduced night sleep duration among Kuwaiti children. Screen-based activity has been considered a major public health issue, associated with unexpected health conditions such obesity. 24 We showed in our analysis that 65.6% of the children reported eating in front of the TV on most weekdays (Table 3). Independent of physical activity, adolescents who spend excessive time on screen-based activities are more prone to obesity.21,25 Strong associations have been consistently observed between the presence of the TV in the bedroom and weight gain, mediated by TV viewing time.21,26 It has been reported that screen-based activities have the ability to divert children’s attention away from the control of food intake, eventually distracting them from signals of satiety,27,28 suggesting that screen activities could mediate the relation between sleep and obesity. A previous cross-sectional study using the same data showed that Kuwaiti children of diabetic parents sleep significantly less than children who have nondiabetic parents. Giving the fact that short sleep duration is related to diabetes and metabolic diseases,22,26,29,30 this could be attributed to the family lifestyle factor: it is possible that parents who do not value sufficient night sleep may let their children stay up late, and these parents are more susceptible to be diabetic.
Our findings revealed that short sleep duration was significantly associated with increased waist circumference among Kuwaiti children. Short sleep duration plays an important role in the risk of abnormal weight gain and obesity by creating hormonal imbalance,6,31 potentially affecting appetite regulation and glucose metabolism, and eventually leading to the development of cardiometabolic diseases such as diabetes and cardiovascular disease. It has been reported that the association between sleep duration and weight gain is strongest between the ages of 2 and 18 years,5,20 suggesting that children and adolescents may be more vulnerable to the effects of inadequate sleep duration.
Another important findings presented in this study is that schools that children attend make a difference in the examined outcome, the sleep duration (Table 5). We also showed strong clustering effect within schools in reducing the sleep duration and increasing the use of screen-based activities over time (Table 6). This indicates that the school context has a substantial influence in shaping children’s behaviors and attitude in the Kuwaiti children population.
Children spend a considerable amount of their time at school. 32 Fifty percent of a child’s waking time is spent in schools; therefore, school is considered a unique social entity that could configure children’s health attitudes and behaviors that eventually shape their health outcomes.32,33 Studies show that health outcomes of children with high genetic susceptibility to certain health conditions could be improved if surrounded with a healthy protective environment. 34 Therefore, most common health intervention programs are school based, because the school can provide the social contextual framework that would support any selected intervention and enhance targeting risk factors for several health conditions. 32
It has been shown that modifying sleep behavior and improving the quality of sleep is efficient and has the potential to support immunity and relief symptoms of chronic diseases. 3 Therefore, school health intervention programs should consider behavioral sleep improvement by educating children and parents about the importance of sleep quality on overall health. Children’s behaviors may be more easily influenced than adults, resulting in a greater potential to accept and adopt new behaviors if they are exposed to healthy practices. Therefore, targeting children’s beliefs and attitudes is an essential step to building healthy behavior that can enhance overall health and prevent chronic diseases. A recent review explored school determinants for optimal health and included the World Health Organization and Centers of Disease Control and Prevention guidelines. This review reported that school health programs could predict children’s health outcomes.33,35-37 Strong evidence shows that school health programs can effectively change children’s health behaviors and decrease symptoms of chronic diseases. 32 Therefore, schools can act as an influential instrument to improve child health outcomes. Research in the United States and other developed countries has successfully identified primary school health determinants. 33 Based on this, school health policies and guidelines have been introduced and implemented to ameliorate chronic disease such as obesity. 38 This improvement has evolved from the substantial effort to integrate scientific research into practice.
Findings from our prospective longitudinal study might be the first step for future research and policy implementation to advance total health for Kuwaiti children and others who face similar health challenges. The following are recommendations for future work that evolved from our study: (1) introduce school health intervention and awareness programs to educate children and their families about the importance of sleep health and how to improve night sleep quality and limit screen-based activities and (2) promote public health research to identify healthy school determinants to help designing future cost-effective school intervention and prevention programs.
Study Limitation
The main problem with children responding to survey questions occurs when the questions are complex, ambiguous, or when information needs to be retrieved from memory. 39 In this study, we used direct forward questions with clear language. We pretested the questions in the pilot study. All the behavior questions were asked starting with “In the past week” to make it easier for children to remember over a shorter period of time. The study was conducted during the academic year, so the sleep behavior questions and other questions were consistent with the school season. The self-reported habitual sleep duration and other lifestyle habits might be susceptible to reporting bias. There were no contextual school-level variables measured in the analysis that might explain the big variation between schools.
Conclusion
This prospective cohort showed that screen-based activities are a major issue contributing to reduced sleep time, with a statistically significant dose-response relationship over time. Public health intervention programs should target schools and educate children and their families to focus on improving night sleep behavior as well as limit their screen time.
Footnotes
Acknowledgements
The present study was funded by Dasman Diabetes Institute in Kuwait (RA/065/2011 and RA/005/2011).