
Abstract
The gut microbiome (gMicrobiome)—a dynamic ecosystem of microorganisms—is emerging as a correlate of healthy lifestyle. Patients may not be aware of this. General Internal Medicine patients completed surveys evaluating gMicrobiome knowledge, lifestyle knowledge, dietary intake, physical activity, sleep, and stress. Surveys were given pre-/post-education (n = 112) and at 1 month follow-up (n = 60). The educational-module comprised a video and handout describing how lifestyle enhances gMicrobiome and health outcomes. Post-educational-module, 9 of 19 (47%) statements showed favorable change in knowledge (P < 0.05). Two statements reached statistical significance at 1-month follow-up: “Exercise influences the types of bacteria present in the digestive system” [7 (12%) to 24 (41%), P = 0.004] and “An inactive lifestyle promotes the growth of healthy types of digestive system bacteria” [12 (20%) to 24 (41%), P = 0.035]. We observed a small but favorable change in knowledge but not behavior. Large lifestyle changes are challenging to adopt, and education alone is necessary but insufficient for change. Our results confirm that education is a viable first step to establish the importance of pursuing lifestyle changes, perhaps moving from pre-contemplation to contemplation. Baseline knowledge in our participants was higher than anticipated, indicating that this intervention may have been too introductory. Future interventions should investigate baseline knowledge.
“The majority of subjects knew that there are bacteria on and in their bodies and that certain bacteria are beneficial for human health.”
Introduction
Lifestyle medicine is an important and growing frontier in medicine that aims to help individuals achieve better health through 6 pillars: whole-food plant-predominant diet, physical activity, stress management, restorative sleep, positive social connection, and avoidance of harmful substances. 1 Numerous studies show that improved outcomes are obtained in various areas of health (metabolic,2-4 cardiovascular,5,6 gastrointestinal, 7 etc.) when people commit to some or all of these behaviors. Despite the abundant evidence for these benefits, it is often difficult for individuals to start making and subsequently maintain lifestyle changes. 8 A common strategy used to facilitate behavior change is educational interventions.
There is extensive literature describing behavioral and nutritional education interventions. Many studies utilize classes or other forums outside of the clinical setting to deliver the education component. Specifically in nutrition education studies long study duration (>5 months) and few, focused objectives are factors associated with success within these trials. 9 There are advantages to this design such as longitudinal educational experience and sustained educator support; however, for some patients it may be an impractical or difficult commitment. Thus, it is important for clinicians to provide succinct and effective educational materials to patients during their standard appointments. There are few educational interventions that provide information about the role of the gut microbiome (gMicrobiome) in health. A randomized controlled trial by Uemura et al evaluated the effect of an educational intervention centered on gMicrobiome education and after 8 weeks dietary fiber intake and frequency of vegetable consumption increased while body mass index (BMI) decreased 10 —both favorable outcomes. Given this result, education regarding the gMicrobiome's influence on health is likely a viable and promising method to affect lifestyle behaviors.
In addition to the positive results described above, a strategy that may increase individual interest in pursuing lifestyle changes is informing them about changes that will affect an aspect of health with which they are unfamiliar 11 —for example, the importance of the gut microbiota and gMicrobiome. The gMicrobiome ecosystem contains a diverse collection of microorganisms with varying degrees of functionality that influence the host in health and disease. 12 Although the mechanisms underlying how the gMicrobiome affects the host are still incompletely understood, we do know that individuals of similar health or disease statuses have similar microbial compositions or comparable trends in the relative abundance of species, and therefore, presumably, function.13,14 While we cannot currently define what a “healthy” gMicrobiome is, in part due to large interindividual variation, markers of an apparently healthy gut microbial community include species diversity, genomic abundance, and a stable central microbiota 15 ; in other words, a resilient gMicrobiome with both flexibility and redundancy in function. 16 An optimal lifestyle is correlated with states of positive health that, in turn, correspond with an optimal gMicrobiome. We hypothesized that informing individuals how to improve their gMicrobiome through lifestyle modification will result in increased motivation for pursuing healthy behaviors.
Methods
Objectives
In this study, we sought to assess the feasibility of an educational intervention that would accomplish the following objectives: (1) Evaluate patients’ baseline understanding of the gut microbiome and principles of a healthy lifestyle. (2) Create an effective educational-module to enhance patients’ knowledge about the function of the gut microbiome, its connection to health status, and how lifestyle modification may affect this. (3) Analyze the impact of the educational-module on patients’ knowledge of the principles of a healthy lifestyle and frequency of behaviors associated with good health. (4) Assess changes in knowledge in patients completing the educational-module. (5) Assess the persistence of changes in knowledge and behavior after 1 month compared to baseline.
Study Design
This study was designed pragmatically, to mimic what might occur in the primary care clinic given the time constrain and infrequent follow-up. We sought to evaluate the feasibility of a short, educational-module explaining the link between healthy lifestyle behaviors and optimal gMicrobiome function and to determine if this educational intervention would impact knowledge, mindset, and behaviors about healthy living, dietary intake, and physical activity. This study used a single-group pre-test/post-test, quasi-experimental design to address the research question and objectives.
Study Population and Recruitment
We prospectively recruited patients attending the George Washington University (GW) General Internal Medicine (GIM) Clinic. Patients were eligible if they were between the ages of 18-85 years, were able to read/understand English, and had access to a phone or computer with Internet capabilities.
From July to September 2022, patients in the GW GIM waiting room met with a researcher (BK or SN), who informed them about the details of the study, answered any questions, and enrolled them in the study if desired. Recruitment flyers containing information about the study were also placed in the waiting room for patients to explore on their own. All flyers contained a QR code that, when scanned by a smartphone, took patients to the enrollment screen.
Although most participants who enrolled in the study were patients of the GW GIM, we cannot exclude the possibility that some of the participants enrolled were accompanying a patient attending the GW GIM Clinic.
Study Procedures
Study Protocol. Timeline of Key Study Milestones.
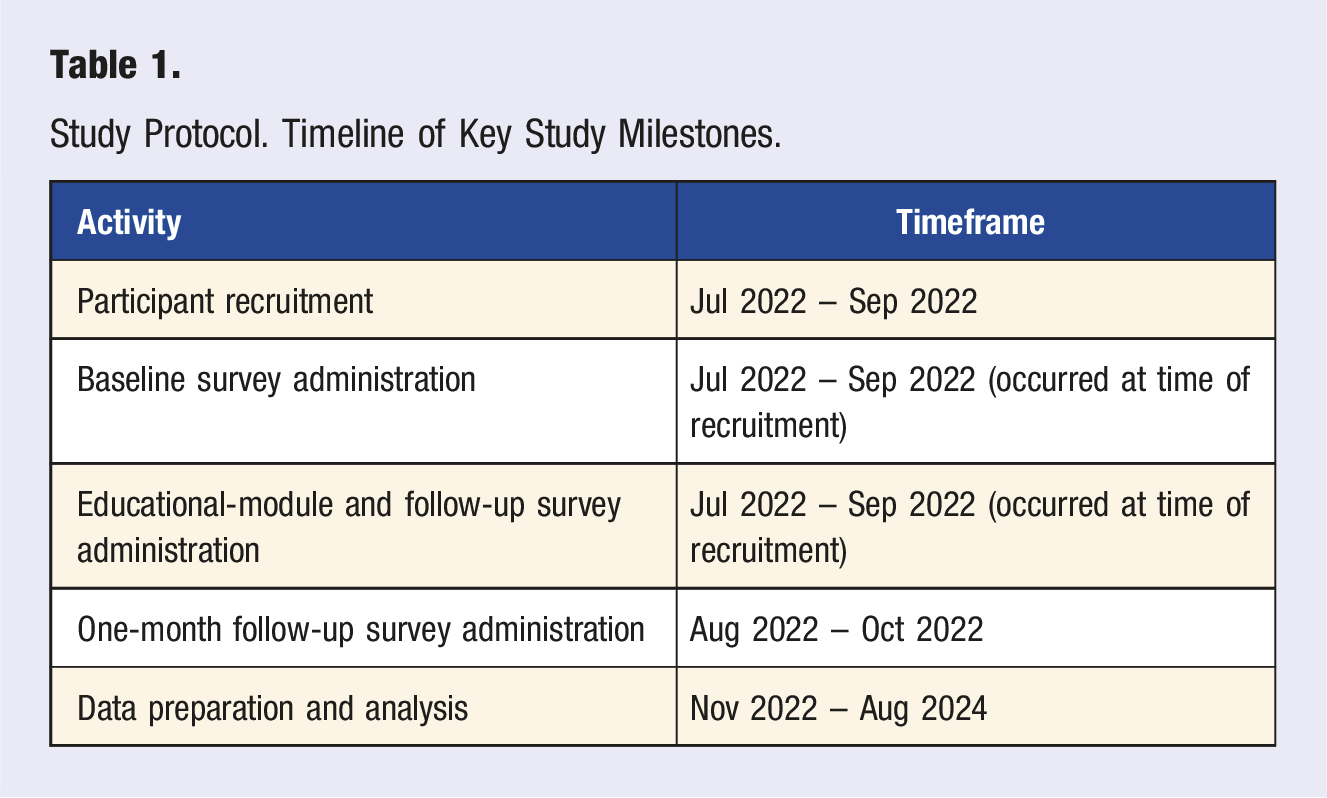
Potential participants were met by BK or SN in the GW GIM clinic. Most participants who agreed to enroll immediately completed the baseline survey, educational-module and initial follow-up survey on their smart phone. A minority of participants completed the baseline survey, educational-module, and initial follow-up survey at a separate time. Those participants accessed the survey materials on a laptop or smartphone via the QR code or URL that was located on the study handout. Per the study protocol, participants were not contacted prior to 1-month after enrolling into the study as the study was evaluating the impact of a 1 time educational-module without additional investigator support. At the 1-month time point post enrollment, participants were contacted via email, which contained the link to complete the 1-month follow-up survey. Three additional reminder emails containing the link to the 1-month follow-up survey were sent to participants who had not returned the survey during September – October 2022.
Part 1: Baseline Survey
Part 1 consisted of participants agreeing to participate through informed consent and completing a baseline survey via Qualtrics. When accessing the baseline survey, the informed consent appeared as the first observed screen. Participants were required to read the informed consent (no signature required) and accept it before proceeding to the survey. The baseline survey had 47 questions/statements and was designed to capture participant demographics, gMicrobiome knowledge, familiarity with lifestyle behaviors as well as general health concepts, and frequency of certain health behaviors associated with positive health outcomes including dietary intake and physical activity.
Part 2: Educational-Module and Initial Follow-up Survey
Part 2 involved patients viewing a five-minute video and a handout that provided information about the connection between lifestyle behaviors and gMicrobiome composition/function and the relationship between a “healthy” gMicrobiome and positive health outcomes. The video appeared at the end of the baseline survey. The handout and an additional copy of the video were sent to participants via email upon completion of the baseline survey. The video and handout (the educational-module) were designed by the investigators, who have expertise in the principles of adult learning and behavior change, in collaboration with instructional designers at our university.
Immediately after, participants were asked to complete a survey to evaluate the impact of the educational-module on their knowledge. This survey contained 19 questions/statements that were identical to those in the baseline survey (gMicrobiome, lifestyle, and general health concepts).
Part 3: One-month Follow-up Survey
Part 3 was a final follow-up survey with 41 questions/statements sent to participants via email 1 month after the baseline and initial follow-up surveys. The 1-month follow-up survey contained essentially the same questions/statements as the baseline survey for the purpose of identifying persistence of changes in knowledge and/or behavior from baseline.
Survey Design
This survey was adapted from several existing and validated surveys.17-19 The baseline and 1-month follow-up surveys were nearly identical and contained 7 sections described in detail in the subsequent sections (see the Supplement for the full baseline, initial follow-up, and 1-month follow-up surveys). The initial follow-up survey contained the following sections: knowledge of human-relevant bacteria, lifestyle behaviors and the gMicrobiome, and personal beliefs about health and motivation.
Demographics
The demographics section collected names, email addresses (for follow-up contact), gender identity, race/ethnicity, highest education attained, and highest science education attained. The follow-up survey did not contain an extensive demographics section and was assumed to be unchanged.
Health History
Health history was evaluated with 1 question, which asked participants to rank their health over the past year on a scale of poor, fair, good, or excellent.
Knowledge of Human-Relevant Bacteria
Knowledge about bacteria found in humans was assessed with 3 basic statements that participants responded to on a 4-point Likert scale—Strongly Disagree, Disagree, Agree, Strongly Agree: (1) There are bacteria on and in our body. (2) All bacteria are bad for human health. (3) Certain bacteria are beneficial for human health.
These were chosen because they assessed a basic understanding of the relationship and interactions between bacteria and humans and established a participant’s baseline knowledge of the human microbiome as a whole.
Nutritional and Gut Microbiome Knowledge
Knowledge of nutrition and the gMicrobiome was gauged with 4 questions/statements assessing whether participants felt comfortable implementing nutritional changes in their lives and if they were familiar with the gMicrobiome. In addition, we assessed if participants previously had discussions with their physician about dietary changes or the gMicrobiome: (1) I have an understanding of what nutrition is and how to implement it into my lifestyle. (4-point Likert scale) (2) Have you and your physician discussed making dietary changes to influence your health? (Yes/No) (3) Have you heard of the gut microbiome? (Yes/No) (4) My physician has discussed the gut microbiome with me. (4-point Likert scale)
Lifestyle Behaviors and the Gut Microbiome
Eight statements, all on the 4-point Likert scale, were used to evaluate whether participants were aware of the relationship between dietary pattern, sleep, exercise, and stress on gMicrobiome composition/function: (1) Diet influences the types of bacteria present in the digestive system. (2) Eating a predominantly plant-based diet promotes the growth of healthy types of digestive system bacteria. (3) Eating a standard American diet promotes the growth of healthy types of digestive system bacteria. (4) Sleep influences the types of bacteria present in the digestive system. (5) Exercise influences the types of bacteria present in the digestive system. (6) Stress influences the types of bacteria present in the digestive system. (7) An inactive lifestyle promotes the growth of healthy types of digestive system bacteria. (8) It is better to have more types of digestive system bacteria than less diversity of digestive system bacteria.
These domains are strongly linked to the gMicrobiome; they are also among the 6 Pillars of Lifestyle Medicine. These statements were key to assessing changes in knowledge and behavior.
Dietary Intake
Dietary intake was assessed by asking participants to identify the number of servings of vegetables, fruit, beans, minimally processed whole grains, nuts and/or seeds, meat, seafood, and processed snacks, treats, and fast food consumed in a typical day. These questions were adapted from a validated 15-item food frequency questionnaire measuring dietary quality. 17 Additionally, participants were asked to identify the number of fermented foods consumed in 1 month and the number of different minimally processed plant foods consumed in 1 week, the latter of which can be compared to the American Gut Projects’ finding that at least 30 plants/week are associated with gMicrobiome diversity. 20 Minimally processed plant foods a.k.a. whole plant foods are more likely to contain fiber and an intact food matrix, which supports a “healthy” gMicrobiome.21-23 Fermented foods act similarly to whole foods in that the food matrix and fiber are typically intact; however, they also contain live active cultures (probiotics) and/or beneficial microbial metabolites (postbiotics).24–28
Physical and Mental Status
Physical and mental health were evaluated by asking about perceived stress (sliding, 0-10 scale), hours of sleep per night (sliding 0-15 scale), feeling rested upon waking (4-point Likert scale), sedentary hours per day (sliding, 0-16 scale), and frequency of moderate and vigorous physical activity, both per week (0-30, 30-60, 60-90, 90-120, 120-150, 150+ minutes). These questions were adapted from Centers for Disease Control and Prevention (CDC) recommendations for physical activity. 29
Personal Beliefs About Health and Motivation
Personal beliefs about health and motivation were evaluated (4-point Likert scale) by asking participants to gauge how personal actions, lifestyle, diet, genetics, and the gMicrobiome affect health outcomes. We also asked directly if participants make lifestyle and dietary decisions with the intention of impacting their health. Finally, we evaluated if participants were influenced by recommendations by their physician to make dietary or lifestyle changes. These are the specific statements used: (1) My actions and decisions influence my health. (2) Genetics is the strongest determinant of physical and mental health. (3) Lifestyle is the strongest determinant of physical and mental health. (4) Lifestyle choices influence the activity of my genes. (5) The bacteria in my digestive system influence my health. (6) My diet influences my physical and mental health. (7) I make dietary and/or lifestyle decisions with the intention of influencing my health. (8) I am likely to implement a dietary or other lifestyle change if my physician recommends it.
Information on Survey Completion
Additional parameters were also recorded by Qualtrics, including duration of time to complete the survey, date of initiation and completion, and percent progress through the survey.
Educational-Module Design
In collaboration with the GW Instructional Media for Programming, Collaboration and Teaching (IMPACT) Initiative, an educational-module was developed to quickly deliver the key points relating to the gMicrobiome, its role in health and disease, and how lifestyle affects this. Using principles of adult learning and best practices, an outline for a short educational video was developed. The video audio was recorded by LF and then animated by the GW IMPACT Initiative team. All content was reviewed by multiple content area experts as well as those outside of the field to optimize accuracy and understandability; all feedback was incorporated prior to implementation.
Video
The five-minute educational video covered the following key points: • The gut microbiome is an ecosystem of microbes living inside humans that functions to digest food, produce nutrients, influence the immune system, and impact overall health • A “healthy” gut microbiome supports better immunity and reduced risk of digestive tract diseases • Dietary changes impact the composition and health of the gut microbiome • Microbiome health is a function of diversity, which is achieved by eating numerous different whole plant foods • How to eat to support gut microbiome health ○ Eat minimally processed foods ○ Eat the rainbow—consume different colored plant foods • Other ways to support gut microbiome health through lifestyle ○ Move throughout the day as much as possible—high intensity is not a requirement ○ Get restorative sleep to allow the body to rest and heal ○ Practice stress management—yoga, meditation, walk in nature, deep breathing This video is publicly available on the GW Health Sciences YouTube Channel at https://www.youtube.com/watch?v=a3DIjt09q4Q.
Handout
The handout covered similar concepts as the educational video, reinforcing the learning from the video, a key element in the principles of adult learning. This also provided the material in a different format and made it easy to reference back to the key ideas, unlike a video, even a short one. The handout also included a whole food, plant-based meal plan, to provide examples of what is discussed in the video and give them tools to, potentially, implement changes in their own lives. The meal plan offered dietary suggestions for breakfast, lunch, dinner, snacks, and beverages and included a variety to appeal to a broad population. The handout also included resources to learn more about whole foods, plant-based eating through evidence-informed websites, books, and videos
Survey Curation and Data Management
For all 3 surveys (baseline, initial follow-up, 1-month follow-up) responses were excluded if both name and email address were missing, as it would not be possible to link the baseline and follow-up survey data. In addition, baseline surveys with less than 58% completion and initial follow-up surveys with less than 100% completion were eliminated from our primary analysis.
Two separate bins of baseline surveys were developed. Bin one included all baseline surveys that were not previously excluded—this was used for our primary analysis. Bin two included all baseline surveys that had a companion 1-month follow-up survey, which was used for our secondary analysis and to assess potential for bias in bin one. Name and email were used to pair the baseline surveys to the 1-month follow-up surveys. If surveys could not be adequately paired, the 1-month follow-up survey was excluded. For example, if the baseline survey contained a name without an email address and the follow-up survey contained an email address without a name, the baseline survey could not be accurately paired with the follow-up survey and thus was censored.
Initial follow-up surveys did not require the pairing process because the responses were collected with the baseline survey; thus, they were already linked to the participant
All surveys were designed and disseminated in Qualtrics (Seattle, WA). Qualtrics maintained all data submitted by participants on a secure web server using encryption. Data from Qualtrics was downloaded to a CSV or Excel document for data analysis.
Statistical/Data Analysis
Statistical analysis was conducted using IBM SPSS v28 (Chicago, IL). Descriptive statistics were calculated for estimates of the mean (continuous data) and frequencies (nominal data). For each question, we calculated the number of responses of each answer choice as a percentage for the baseline, initial follow-up and 1-month follow-up surveys.
Inferential statistics were conducted in SPSS. The McNemar statistical test was applied to the knowledge-based questions/statements to determine if the proportion of the selected answer choices per question were significantly different between the baseline and 1-month follow-up surveys. The McNemar test was also used to evaluate change in dietary and exercise patterns in the baseline and 1-month follow-up surveys. An alpha of 0.5 was used as a cut-off for statistical significance.
To determine the type of change in responses, we analyzed the direction and magnitude of the response change between the baseline and 1-month follow-up surveys. For Likert scale responses, we calculated the percentage of participants whose response either stayed the same or changed. For each question, either Strongly Agree or Strongly Disagree was considered the favorable response depending on the wording of the question. If a change in response occurred in the direction of the favorable response, it was considered positive. A change in response away from the favorable response was considered negative.
For the nutrition and physical activity questions, the same process was applied. However, for questions about vegetable, fruit, bean, whole grain, and nut/seed intake as well as physical activity, responses that changed in the direction of higher servings consumed or more time spent doing physical activity were considered positive. For the question about fast food / processed snacks, responses that changed in the direction of lower servings consumed were considered positive. For the 2 questions about meat and seafood, we calculated the percentage of participants with either the same or changed response, but the direction of change was not considered favorable or unfavorable because moderate amounts of meat/seafood can be part of a healthy diet.
Results
Baseline and One-Month Follow-Up Survey Results
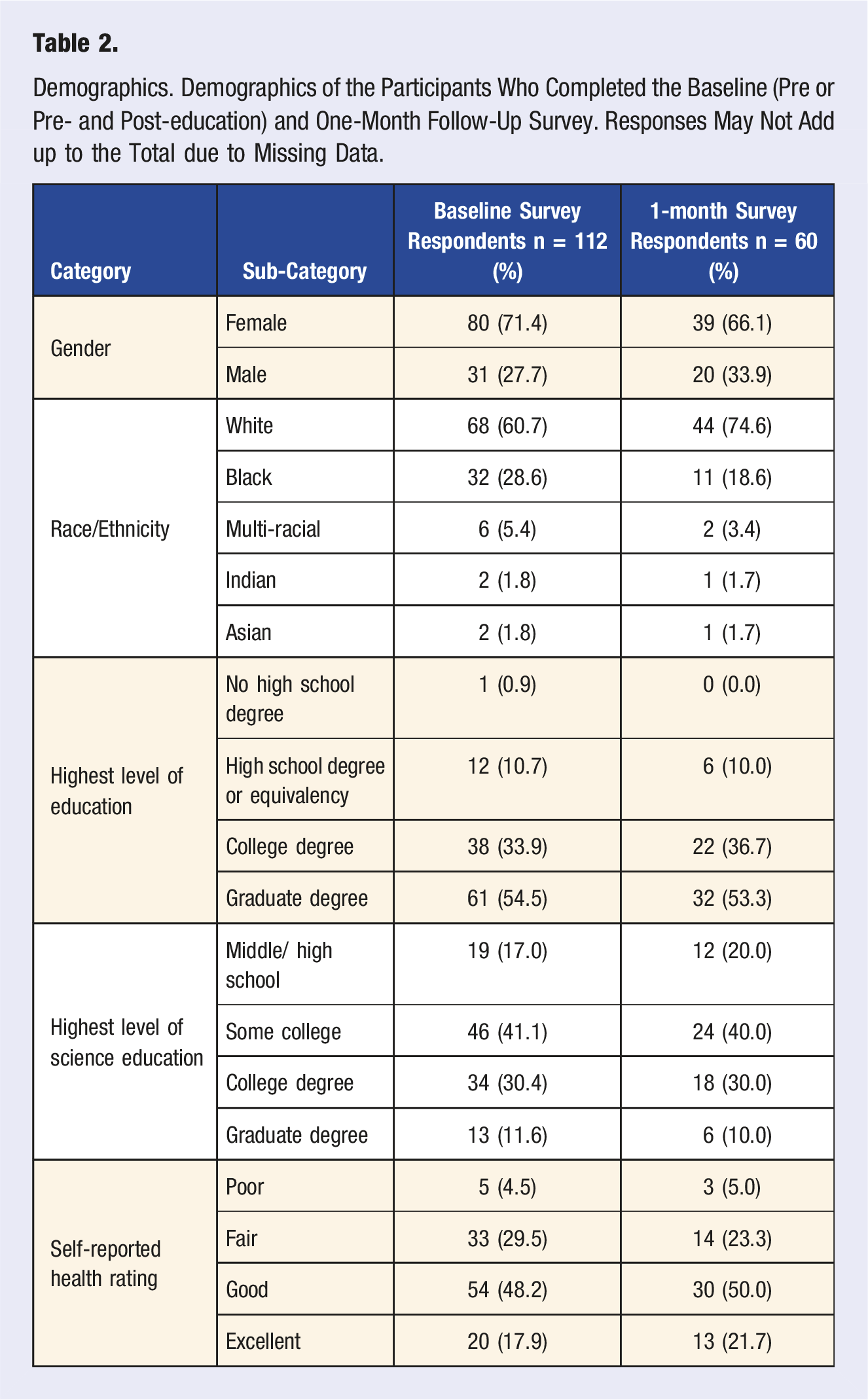
A total of 157 baseline (pre- and post-education) and 65 1-month follow-up surveys were received. After excluding surveys that were either unidentifiable or less than 58% complete, 112 baseline surveys remained. Of the 65 1-month surveys completed, 5 were excluded because they could not be matched to their companion baseline survey. This left 60 linked baseline and 1-month surveys for analysis.
Demographics. Demographics of the Participants Who Completed the Baseline (Pre or Pre- and Post-education) and One-Month Follow-Up Survey. Responses May Not Add up to the Total due to Missing Data.
At baseline, 80 participants (71%) had previously heard of the gMicrobiome, but 99 (88%) either disagreed or strongly disagreed with the statement, “My physician has discussed the gMicrobiome with me.” Furthermore, 72 (64%) participants answered yes to “Have you and your physician discussed making dietary changes to influence your health.” Finally, 105 (94%) participants agreed or strongly agreed with the statement, “I am likely to implement a dietary or other lifestyle change if my physician recommends it.”
Survey Responses for Knowledge-Based Statements. Baseline and One-Month Responses for Knowledge-Based Statements. Baseline Survey Responses are Only From Participants Who Also Completed the One-Month Survey. Responses May Not Add up to 60 for Each Question if There was Missing Data; Missing Data Were Not Interpolated. *P < 0.05 Indicates a Statistically Significant Change in the Responses From Baseline to the One-Month Survey. IND = Indeterminate.
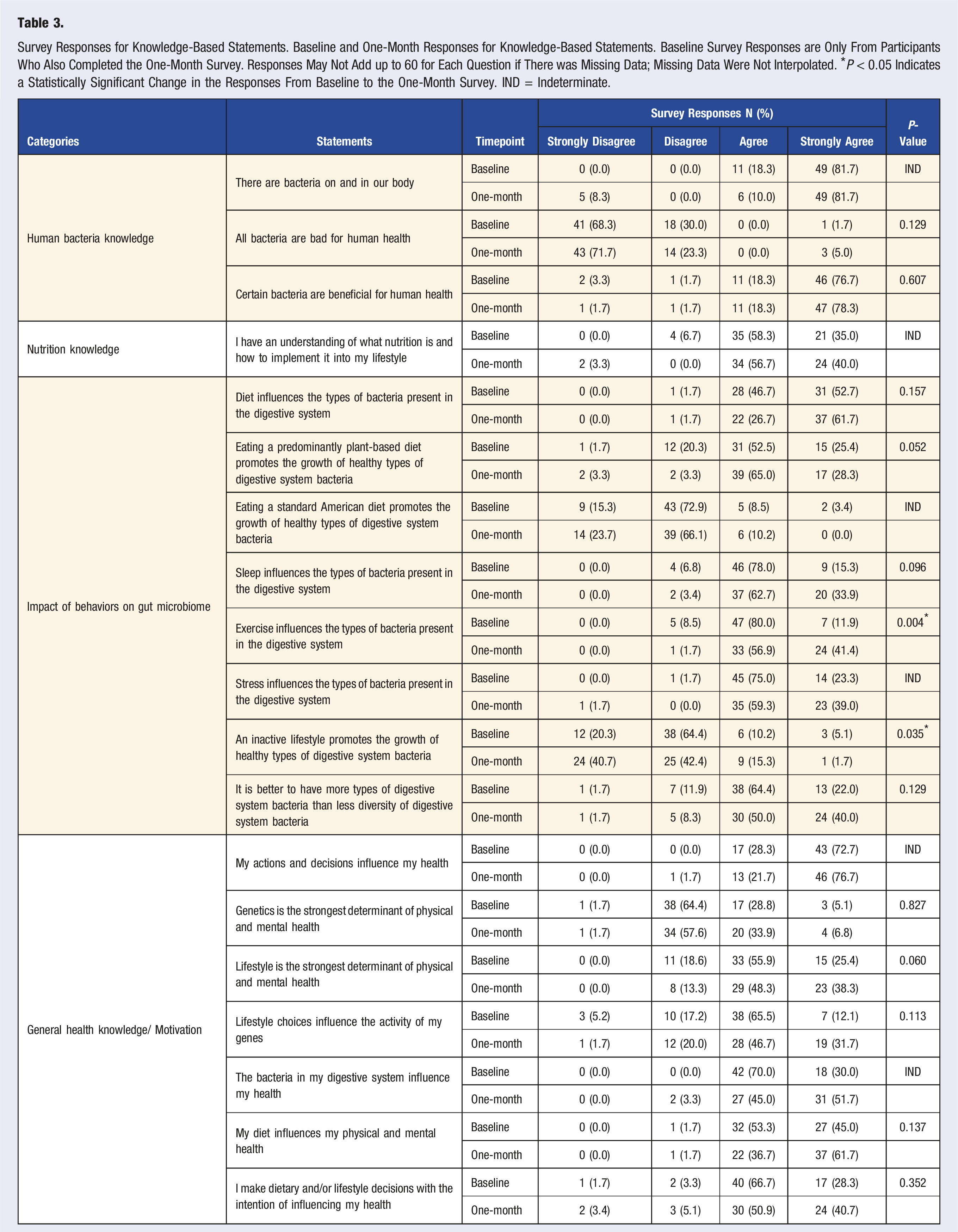
Two responses reached statistical significance (Figure 1 and Table 3). The number of people who chose Strongly Agree for “Exercise influences the types of bacteria present in the digestive system” increased from 7 (12%) to 24 (41%), P = 0.004. While those who chose Strongly Disagree for “An inactive lifestyle promotes the growth of healthy types of digestive system bacteria” increased from 12 (20%) to 24 (41%), P = 0.035. Statistically significant knowledge-based responses at one-month. (Top) Responses for the statement, “Exercise influences the types of bacteria present in the digestive system.” (Bottom) Responses for the statement, “An inactive lifestyle promotes the growth of healthy types of digestive system bacteria.”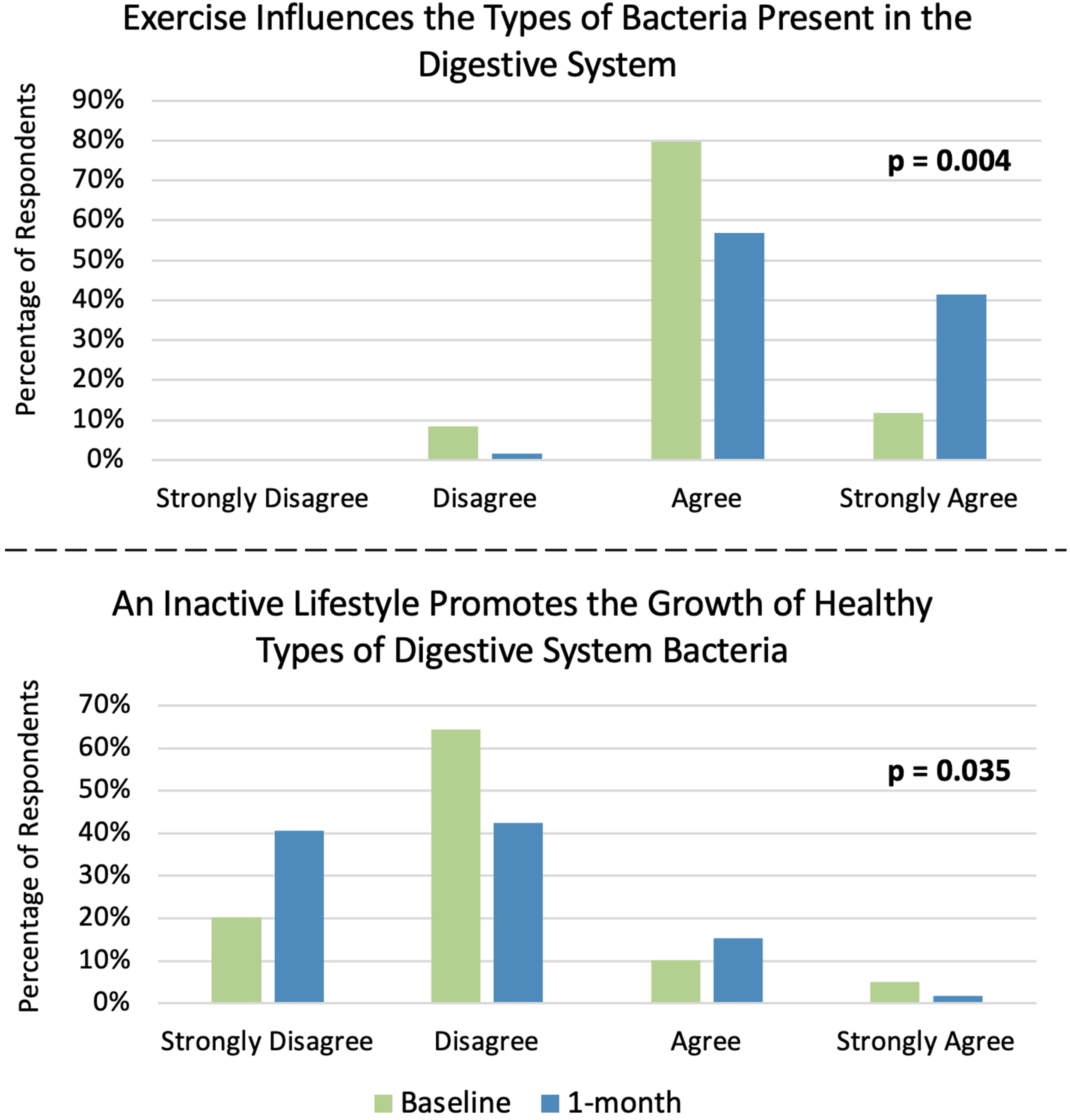
Dietary and Physical Activity Responses. Baseline and One-Month Responses for Dietary Intake and Physical Activity (Only for Matched Baseline and Follow-Up Surveys). Responses May Not Add up to 60 for Each Question Because of Missing Data; Missing Data Were Not Interpolated. *P < 0.05 Indicates a Statistically Significant Change in the Responses From Baseline. IND = Indeterminate.
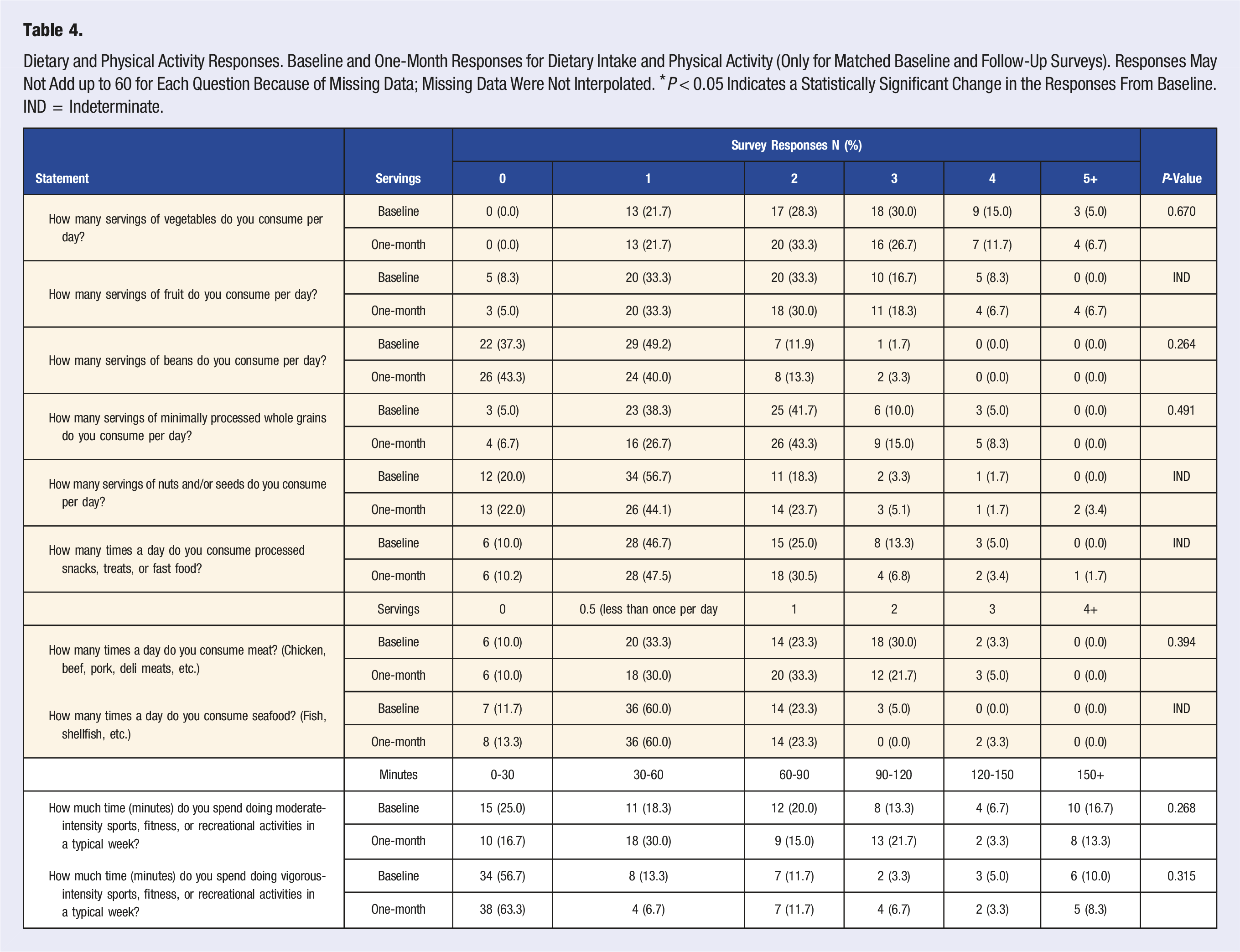
For dietary intake, participants reported eating on average 8.3 ± 5.1 and 8.6 ± 6.2 different types of minimally processed plant foods per week at baseline and 1-month follow-up, respectively. Both well below the 30 plants supported by the American Gut Project findings. Furthermore, the median number of vegetables consumed per day was 2.5 and 2 at baseline and 1-month follow-up respectively. The median daily servings of fruit (2), beans (1), whole grains (2), nuts/ seeds (1) or the frequency per day meat (1), seafood (0.5 (less than once per day)), or processed snacks/treats (1) consumed was the same at baseline and 1-month. See Table 4 for a detailed breakdown of specific responses.
Stress (scale of 0-10 with 10 being maximum stress) was similar at baseline (5.4) and 1-month follow-up (5.4). Hours slept per night was also similar at baseline (6.9) and 1-month (6.7); both below the recommended 7-9 hours. There was no significant difference between the number of waking hours spent sitting or lying from baseline (7.7) to 1-month follow-up (7.2). In both the baseline and 1-month surveys roughly 60% of participants Agreed or Strongly Agreed to the statement “I feel well rested when I wake.”
The median of moderate-intensity exercise per week was 60-90 minutes at baseline and 1-month follow-up. Additionally, the median of vigorous-intensity exercise per week was 0-30 minutes at baseline and 1-month. It is unlikely but possible that these combine to meet the CDC recommendation of 150 minutes of moderate-intensity activity or 75 minutes of vigorous-intensity activity. Table 4 details the physical activity responses.
When analyzing for a directional change in the response from baseline to 1-month, most answers were unchanged across all survey statements/responses (Figure 2). For gMicrobiome knowledge, in 10/11 statements, there was a greater percentage of participants with a more favorable score as opposed to a less favorable score at 1-month vs baseline (Figure 2(A)). For health literacy/motivation, 7/8 statements had a higher percentage of participants with a more favorable score at 1-month follow-up vs baseline (Figure 2(B)). The categories of fruit, whole grains, and nuts/seeds had a higher percentage of participants with a more favorable score at 1-month follow-up; however, the vegetable and bean category did not. (Figure 2(C)). Table S3 details the magnitude and direction of response changes for each statement. Change in survey scores from baseline to one-month follow-up. Change in gut microbiome knowledge (A), health literacy/motivation (B), and dietary consumption (C) scores. For meat and seafood, more consumption was not labeled as less favorable and vice versa. *P < 0.05 indicates a statistically significant change in the responses from baseline.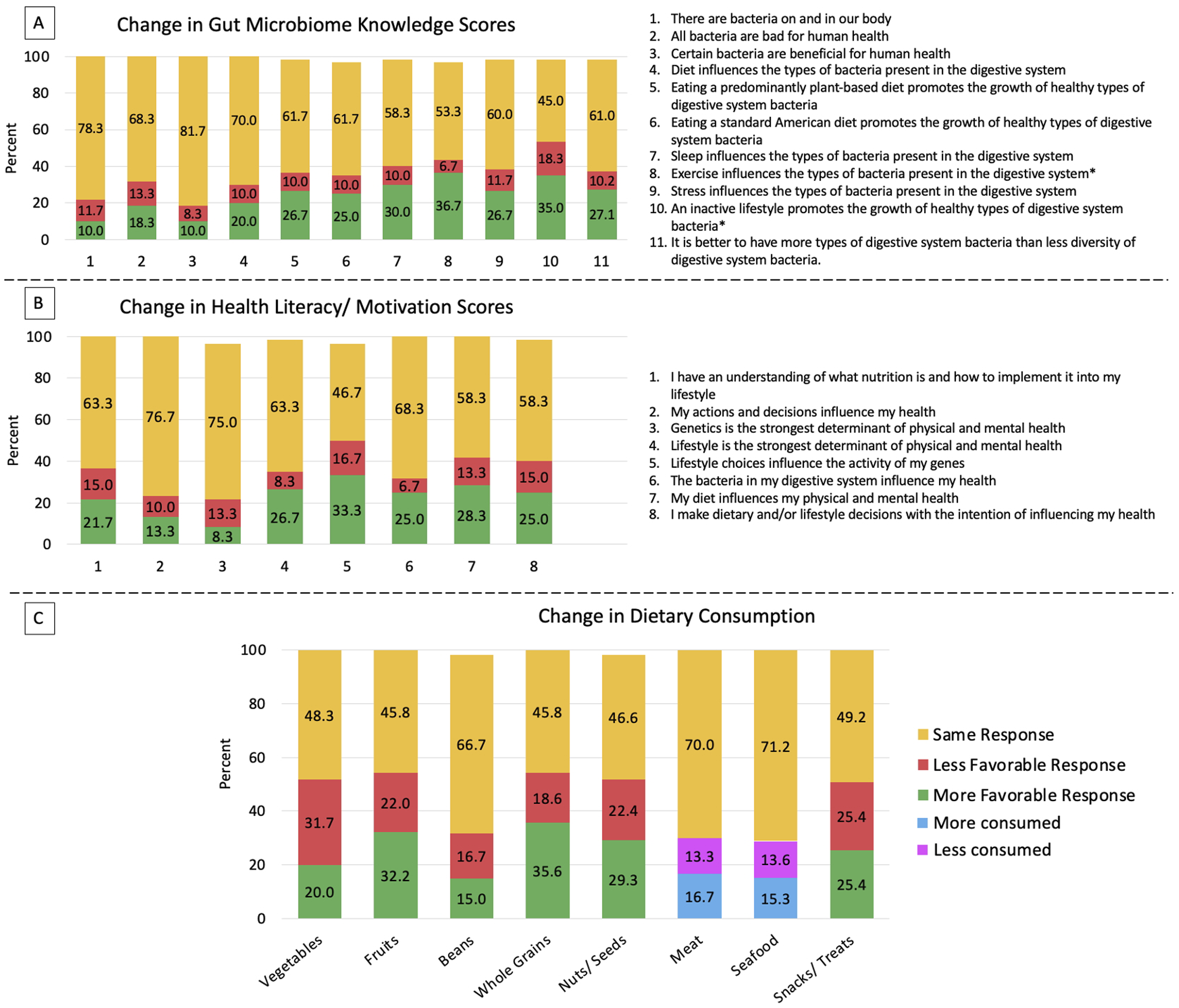
Initial Follow-up Survey Results: Post-education
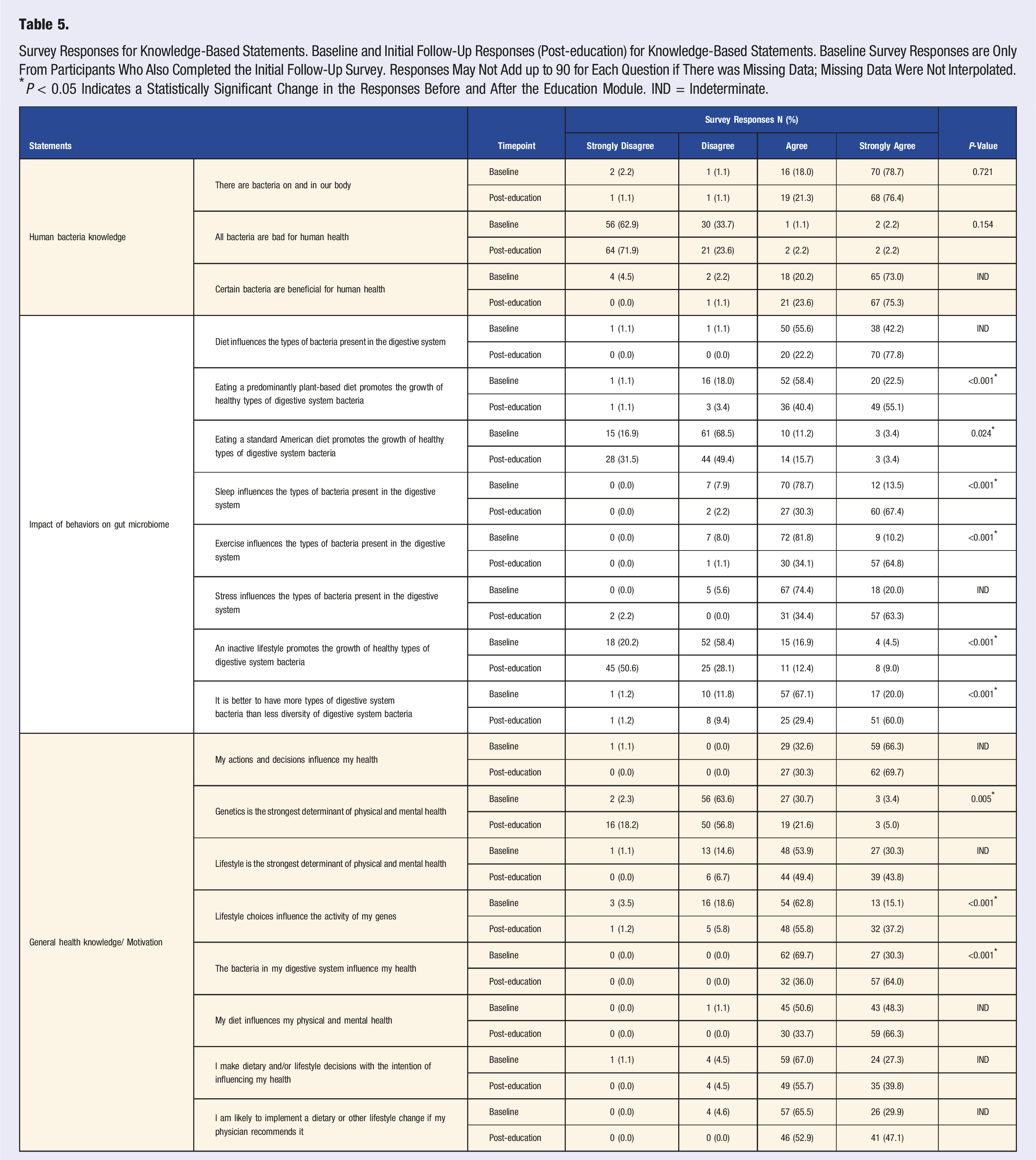
Survey Responses for Knowledge-Based Statements. Baseline and Initial Follow-Up Responses (Post-education) for Knowledge-Based Statements. Baseline Survey Responses are Only From Participants Who Also Completed the Initial Follow-Up Survey. Responses May Not Add up to 90 for Each Question if There was Missing Data; Missing Data Were Not Interpolated. *P < 0.05 Indicates a Statistically Significant Change in the Responses Before and After the Education Module. IND = Indeterminate.
Discussion
The first goal of this study was to evaluate baseline understanding of the gMicrobiome and principles of a healthy lifestyle. Our results demonstrated a higher than expected baseline knowledge. The majority of subjects knew that there are bacteria on and in their bodies and that certain bacteria are beneficial for human health. They understood that a connection exists between lifestyle choices and the type of bacteria in the gut with many understanding that diet has an effect and the vast majority understanding that sleep, physical activity, and stress play a role. At baseline, >95% of participants agreed that bacteria support our health, >75% agreed that lifestyle behaviors impact the gMicrobiome composition and function, and >65% answered favorably to statements about the influence of genes, lifestyle behaviors, and diet on health outcomes. While understanding the importance of diet, they were less clear on which dietary pattern was most favorable for microbiome health.
Because of participants unexpectedly high level of baseline knowledge in this area, the effect of the educational-module was limited. The initial follow-up survey (post-education) allowed us to evaluate the immediate impact on knowledge regarding the gMicrobiome and other health topics. Responses were statistically different from baseline in 9 of 19 (47%) statements (Table 5). In all cases, the change in response was in a more favorable direction. However, the majority of changes were from favorable to more favorable instead of undesirable to favorable, which suggests that the educational-module reinforced knowledge rather than provided new information.
At 1-month follow-up, we observed a trend toward more favorable responses for knowledge statements. Participants either maintained their baseline response or selected 1 that was more favorable in most cases (Figure 2). Information in the module connecting physical activity and gMicrobiome health seemed to impact subjects more than other points. There was a statistically significant improvement in subjects supporting the idea that exercise influences the types of bacteria present in the digestive system and that an inactive lifestyle promotes the growth of unhealthy bacteria. Perhaps, patients perceived the link between physical activity and the gMicrobiome as more novel, making it more influential. In contrast, the role of diet on the gMicrobiome has been discussed in the media and other lay sources of health information and may be less novel/penetrating. Lifestyle behaviors such as diet, physical activity, stress, and sleep were largely unchanged at 1-month vs baseline with no statistically significant results.
Although we hoped that participants would pursue healthy lifestyle changes in response to the educational-module, the results we obtained were, in retrospect, not surprising. In order to make meaningful lifestyle changes, patients need the knowledge of what change to make, motivation to change, and an understanding of the practical steps needed to incorporate the changes into their life. Our subjects had a high baseline knowledge, which may have precluded a large effect from the module on that aspect of behavior change; 61 (55%) and 38 (34%) participants had a graduate or college degree, respectively. Unintentionally, the study population was skewed toward those with high educational attainment, and many were likely already aware of the lifestyle behaviors associated with positive health outcomes. The study population was generally healthy, as 74 (66%) participants rated their health “Good” or better. Thus, they may not have had reason or motivation to make behavioral changes. The message of our educational-module may have resonated stronger in a population of those with lower health status at baseline. Our intervention was short and did not provide participants with longitudinal support when making lifestyle changes; thus, it was unlikely to see a large shift in the responses. This population may have benefited more from a program focused on providing resources and tools to successfully integrate these behaviors into their lives rather than on education about the importance of these behaviors. A similar intervention incorporating these best practices of behavior change may show improved results.
Interestingly, the study population, drawn from an urban academic medical practice, was primarily comprised of well educated, white women. While their baseline knowledge of the gMicrobiome and its relation to health was unexpectedly high, it was notable that the vast majority (88%) had never discussed this important issue with their physician. Despite most (94%) participants reporting that they were likely to implement dietary changes if their physician recommended it, only 64% reported having discussions with their physician about making dietary changes to improve their health. This represents a gap in provider education/abilities that could improve patient outcomes.
Strengths and Limitations
Our study has at least 2 strengths. To our knowledge, this study was the first to inform individuals about lifestyle changes though their impact on the gMicrobiome at a GIM clinic. With this approach, we established feasibility and showed that education about how lifestyle changes impact the gMicrobiome and subsequently health can impact knowledge. Additionally, our study design allowed for face-to-face interaction between study recruiters and potential participants. Recruiters were able to answer questions and help participants successfully complete the survey and educational-module. The conversations started in the waiting room of the GW GIM Clinic and were informative of the lived conditions that these patients experience and the barriers they encounter in accessing health care and attaining a healthy lifestyle. This information can serve as the foundation for future interventions and resources.
There are at least 6 weaknesses. The 1-month follow-up survey response rate was roughly 50%, which is less than ideal, despite minimal detectable differences between those lost to follow-up and completers. Although we are confident in the surveys we received, the remaining 50% would have increased the power and the internal validity of the study of the study. Thus, ongoing and future research can be strengthened by implementing methods to improve the follow-up rate, which may include frequent engagement with participants. Additionally, the validity and reliability of the questionnaires were not established prior to implementation. The questionnaires were developed from existing validated surveys; however, the addition, removal, or modification of questions/statements could have impacted the validity. Future research can target the questionnaire and evaluate reliability and validity, which will ultimately improve confidence in the instrument. Furthermore, the educational-module provided a brief introduction to the gMicrobiome and the lifestyle changes that are associated with good health. We did not provide extensive details about strategies to begin pursuing the behavioral changes or how to maintain them, by design. The information we provided may not have been elaborate or comprehensive enough for some individuals to make lifestyle changes, which are very challenging to adopt, especially given the high baseline knowledge in this group. In addition, the survey was only accessible via the Internet; thus, the study population was restricted to participants with Internet access. Moreover, we limited our recruitment to 1 location and a single type of clinic—internal medicine. Thus, it may be erroneous to generalize the results to different settings with different patient populations. Finally, the 1-month follow-up survey was distributed via email with no incentive for participants to complete it other than the educational video and handout. These factors may have contributed to a lower yield than anticipated.
Conclusion
We designed and delivered a short educational-module about the connection between the gMicrobiome, lifestyle behaviors, and health outcomes. We measured how the educational-module affected knowledge and lifestyle behaviors via pre-/post-education surveys and at 1-month in participants recruited in an internal medicine clinic. Overall, we observed a small but favorable change in knowledge. Participants may now be more aware of how lifestyle behaviors affect gMicrobiome composition and function, but we did not observe a measurable change in diet, physical activity, or other behaviors. Lifestyle changes are difficult to adopt, and education alone may be insufficient to facilitate change. However, we show that education is a viable first step to establish the importance of pursuing lifestyle changes, perhaps moving from the pre-contemplation to contemplation stage of change. Moreover, our study showed that patients are likely to implement dietary changes if their physicians recommend it, but many physicians are missing the opportunity to discuss the gMicrobiome and recommend dietary change.
Further, the baseline knowledge in our participants was higher than anticipated, indicating that (1) the study population had some prior knowledge of the interplay between bacteria, lifestyle, and health and (2) this intervention may have been too introductory for this population. Future research may benefit from a greater understanding of baseline knowledge when designing appropriate educational interventions.
Supplemental Material
Supplemental Material - Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic
Supplemental Material for Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic by Benjamin Knudsen, Sasha Narain, Brad B. Moore, Patrick G. Corr, and Leigh A. Frame
Supplemental Material
Supplemental Material - Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic
Supplemental Material for Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic by Benjamin Knudsen, Sasha Narain, Brad B. Moore, Patrick G. Corr, and Leigh A. Frame
Supplemental Material
Supplemental Material - Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic
Supplemental Material for Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic by Benjamin Knudsen, Sasha Narain, Brad B. Moore, Patrick G. Corr, and Leigh A. Frame
Supplemental Material
Supplemental Material - Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic
Supplemental Material for Information About the Gut Microbiome’s Connection to Health and Disease can Impact Knowledge: Feasibility of an Education-Based Intervention in a General Internal Medicine Clinic by Benjamin Knudsen, Sasha Narain, Brad B. Moore, Patrick G. Corr, and Leigh A. Frame
Footnotes
Acknowledgment
For her assistance in developing the educational-module, we would like to acknowledge the contributions of Linda Cotton, Senior Instructional Technologist at the George Washington University School of Medicine and Health Sciences’ Instructional Media for Programming, Collaboration and Teaching (IMPACT) Initiative. For her contributions to statistical analysis, extending beyond her duties as a formal educator, we would like to acknowledge the work of Karen Schlumpf, Instructor, Department of Clinical Research and Leadership, The George Washington University School of Medicine and Health Sciences, Washington, DC, USA.
Author Contributions
BK, SN, BM, and LF conceptualized the design; BK, SN, BM, and LF designed the education module; BK and SN recruited patients; BK, SN, PC, and LF performed the data analysis and statistical analysis.; BK and SN wrote the first draft of the manuscript; BK, SN, BM, PC, and LF reviewed and revised subsequent drafts. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.