
Abstract
Biases and stigma related to health, diabetes, and obesity are an obstacle to providing respectful, empathetic, holistic care. Recognizing explicit and implicit biases and understanding the detrimental consequences is key to the stigma that exists, and the impact that it has on patient care is key. Health care professionals have a responsibility to communicate with patients with respect, empathy, and honesty, ensuring the person is at the center of care. There are a multitude of ways to positively change the landscape in which biases exist.
Keywords
“The overlap of stereotypes between diabetes and obesity worsens the stigma and may interfere with effective management of the chronic conditions.”
Introduction
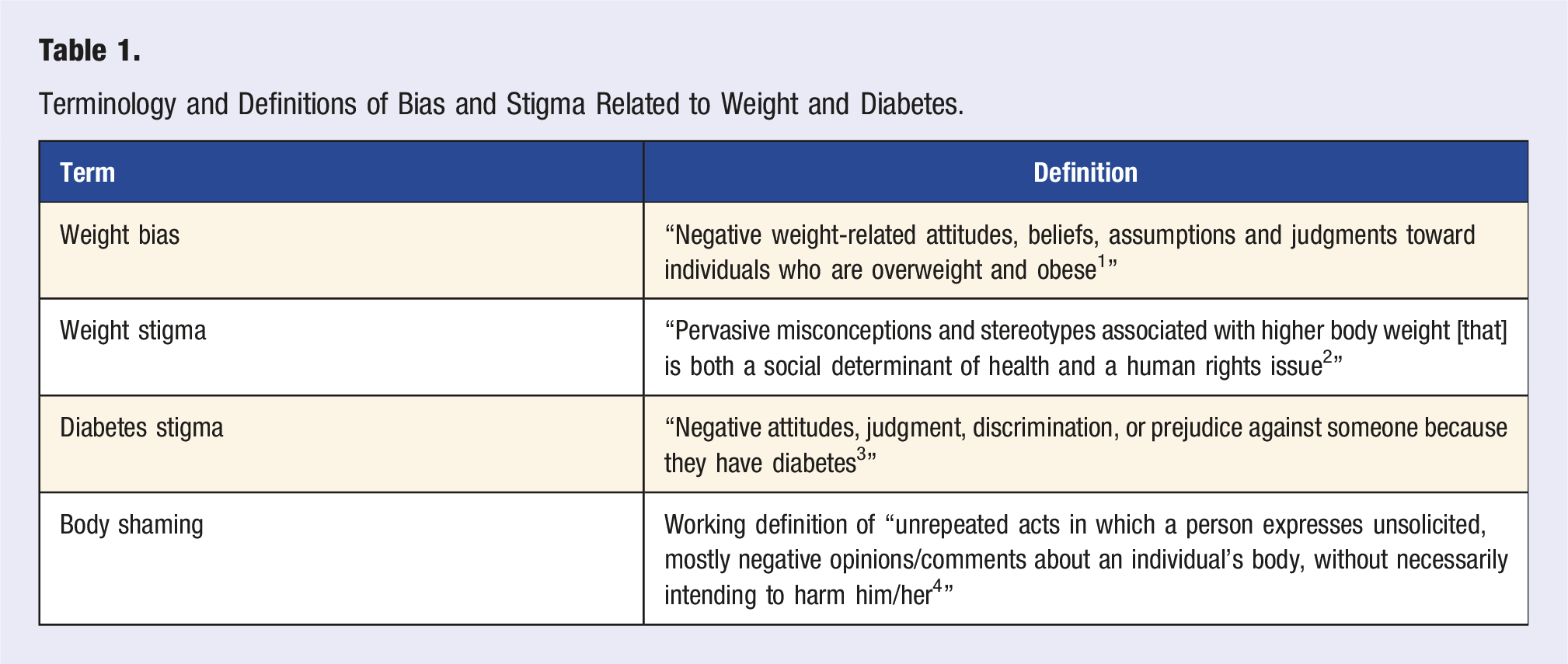
Terminology and Definitions of Bias and Stigma Related to Weight and Diabetes.
A Glimpse Into the Issues
While bias, stigma, and shaming may occur in school, by family or friends, in social media or mass media, unfortunately, people also experience it at health care facilities and by health care professionals. Various studies have been conducted measuring weight and diabetes bias in health care professionals and health care profession students. 5 These biases may result in health care providers believing people with diabetes or obesity are lazy, lacking motivation, non-compliant with treatment, lack self-control or willpower, and are deserving of derogatory humor.5,6 The overlap of stereotypes between diabetes and obesity worsens the stigma and may interfere with effective management of the chronic conditions. Guidelines also emphasize weight loss, which can contribute to the stigma even if it’s not in an explicit way.
When people experience stigma related to diabetes or weight, they may experience lower self-esteem, increased risk of depression, anxiety, stress, social isolation, eating disorders, and substance use, all of which may make them more likely to avoid, delay, or stop medical care. 7 Additionally, weight stigma may contribute to behaviors that increase weight gain, including binge-eating behaviors, maladaptive weight control, disordered eating patterns, increased calorie intake, avoidance of exercise, and lower motivation for physical activity.
A Glimpse Into Ways to Implement Change
A Glimpse Into Starting Education About Biases and Stigma Early—Teaching Health Care Professional Students
Studies have also been published on the ways that schools, colleges, and institutions are intervening to understand body diversity and address weight bias. 12 Best practices for teaching health professional students have evolved to encompass the inclusion of complexities and biologic processes involved in obesity; recognition and mitigation of personal biases; and describing ways in which bias and stigma impact health and well-being. One example of an educational intervention is a 15-minute interactive web-based e-module on obesity bias created by an interprofessional group of health care students and expert faculty. The results showed that residents taking the module appreciated having a patient’s perspective and that there is a need for more strategies to mitigate obesity bias in patient encounter. 13 Schools are also involved in including this education through didactic, simulation, and other experiences—however, there is a need to have more consistent education throughout all the health care curricula.
A Glimpse Into Conversations About Weight, Diabetes, and Medications
The Endocrine Society, American Heart Association, American Gastroenterological Association, American Diabetes Association, and the American Academy of Pediatrics are some of the organizations that have released guidelines about the preferred treatment approach and role of medications in treating patients who are overweight and obese patients in a holistic and cardiometabolic way. Patients may hear about medications from their health care providers, but also from social and mass media. The information from all of these sources sometimes contributes to the stigma. People taking medications for obesity may hear “medication is the easy way out” or “you’ll just gain the weight back” or “it’s just a quick fix”—these message are either explicitly said or implied through various outlets including media, social media, friends/family, and sometimes health care providers. Another interesting thought is how medications used to treat obesity are often called “anti-obesity” medications—this may be contributing to weight stigma and misconceptions about the role of medication in optimizing health. 14 These messages add to the stigma and do not represent the complexity of the pathophysiology of obesity and the complications that may arise from obesity. Understanding the relationship between the pathophysiology of the condition, the interconnectedness of the body, and the person at the center allows the health care practitioner to optimize health in an individualized way.
Summary: Eight Ways Health Care Providers Can Acknowledge, Address, and Avoid Worsening Weight Stigma
(1) Embrace evaluating, confronting, and addressing one’s own implicit biases. (2) Communicating in ways that are truly person centric. This includes using person-first language—avoid “diabetic” or “obese person,” and instead say “person with diabetes” or “person with obesity.” (3) Provide excellent, comprehensive patient education when prescribing and dispensing medications used to treat obesity. Ways to reduce stigma associated with weight loss medications include focusing on the holistic indications for the weight loss medication beyond the scale, highlighting the cardiometabolic benefits. Additionally, issues with coverage or high cost may make patients feel as though the medication is not “medically necessary.” Oftentimes, that is the implication behind the lack of coverage. Pharmacists and health care providers can use language that addresses that implication by focusing on the role the medications may play in cardiometabolic management; advocating for easier access to medication with appropriate use; and communicating this information to patients without bias. (4) Understand body diversity and health data beyond body mass index or weight. Focus on the person beyond the scale which may include health promotion that is weight-neutral. For example, eating plant-based whole foods, engaging in physical activity, addressing stress in a healthy way, and having healthy relationships are evidence-based ways to optimize health that do not always take weight into account.
2
(5) Create an environment that is welcoming for all people. This may include tangible items such as having seating and blood pressure cuffs for every size as well as patient education material that features people of diverse backgrounds and sizes. It also encompasses training the entire team of people including but not limited to the front desk staff, medical assistants and care coordinators, and health care providers on sensitivity training including weight bias and stigma.
15
(6) Addressing all of the patient’s needs and health concerns rather than focusing solely on weight management. Most people want to be seen for who they truly are, not just how others see them externally. Health care providers may focus on weight management in people who are overweight or obese, neglecting seeing and treating the whole person. When discussing weight, seek consent from the patient—one way would be to say, “I would like to talk about your weight today, if that’s okay. Is it something you’d feel comfortable talking about?”
16
(7) Initiate didactic and contact-based education about biases and stigma in the health care professional curricula. Studies have shown that implementing intentional educational opportunities can reduce stigma.
17
(8) Lead with empathy. Even if the health care provider does not exhibit explicit or implicit biases, a recognition that we do not know all about a patient’s past experiences can be instrumental in building a foundation of trust and respect with the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.