
Abstract
Health and wellness coaching (HWC) is an effective intervention for lifestyle disease such as obesity and type 2 diabetes. The evolving HWC profession needs recommendations to guide clinical practice, particularly the appropriate dose of coaching. The purpose of this paper was to systematically review and synthesize HWC literature to derive HWC programming recommendations. Of 102 papers retrieved, 88 were retained with data extracted determining HWC session number, frequency, duration, program length, and total coaching load. Differential analysis yielded no statistical difference in programming variables for randomized control trials and other designs, nor for studies with significant findings v. those not finding statistical significance, allowing these data to be pooled. The HWC intervention for obesity was slightly more intense (15 sessions over 7-8 mo) than the diabetes programming (12 sessions over 9-10 mo). On average, HWC programming applied in the peer-reviewed literature was 12-15 sessions of 35-40 min duration over 7-9 months. These recommendations for HWC programming variables are put forth as initial practice guidelines and should be examined with comparative effectiveness study for optimization. HWC best practice guidelines for other patient groups (e.g., heart disease, cancer, and chronic pain) should also be studied once an adequate literature data base is available.
“This study examines dosing parameters of health and wellness coaching, and moves toward designing recommendations for treating obesity and Type 2 diabetes mellitus”
Introduction
Obesity and type 2 diabetes (T2D) are highly related while being independent threats to our population-wide well-being. These diseases are life threatening and with advancing prevalence over the last two decades. Health and wellness coaching (HWC) is emerging as an effective intervention in the prevention and treatment of both obesity and T2D.1,2 With clinical efficacy supported, the American Medical Association’s decision to establish Current Procedural Terminology (CPT) codes (January 1, 2020) allows physicians to refer patients for coaching services. 3 This authorization will enable wider application of HWC services, particularly to people with obesity and T2D. An important next step for HWC is to establish programming recommendations, or dosing guidelines, to best initiate coaching interventions.
One reason that a pre-determined HWC dosing protocol is not always optimal is that the intervention is best described as patient-centric, and dosing is ideally determined in collaboration with patients to optimize services with needs. While this is a strength of HWC, it is not unique to this form of treatment. Practically all billable medical interventions rely on an acceptable initial dose for implementation but are ultimately mutable based on patient needs. For example, 8 sessions of physical therapy are often recommended for most patients, while 18 sessions of cardiac rehabilitation are a typical initial prescription. Similarly, medications typically have an initial starting dose (e.g., 10 mg of atorvastatin is common for starting hypercholesterolemia treatment). Physicians have latitude to prescribe different initial doses or can decide to amend or extend treatment when deemed necessary by patient needs. This is not unlike the individualized requirements of a HWC intervention, with patient and coach together determining the treatment needs. Determining dose for behavioral interventions, such as HWC, may be seen as difficult but even cognitive behavioral therapy (CBT) is shown to be effective for most patients in as little as eight sessions. 4 Similarly, obesity counseling is prescribed for up to 22 sessions in the first year 5 and the Diabetes Prevention Program (DPP) includes weekly lifestyle counseling for the first 16 weeks. 6 If HWC is to be easily and well-integrated into the existing healthcare system, it is optimal to establish a recommended initial dosing protocol.
One previous attempt to codify HWC interventional approaches determined the existing literature was too diverse and lacked report detail, making it impossible to provide consistent practice recommendations. 7 This study was limited to randomized and controlled trials (RCTs) and included only 16 papers. The HWC coaching literature has expanded greatly since then and is well organized in a published compendium. The Compendium of Health and Wellness Coaching literature provides a systematic review of research and presents all related HWC peer-reviewed studies published in the last 20 years.8,9 There are over 200 peer-reviewed research papers meeting a criteria-based HWC definition, and more than 100 RCTs are included. An “intervention synthesis” can be described as the missing link between research and practice. 10 With the availability of an organized compendium, and given an abundance of data, there is now an opportunity to address the question of appropriate HWC programming and dosing.
Reviewing methodology and deriving recommendations for clinical practice requires systematic review followed by mining and synthesizing existing meta data.
11
Furthermore, a critical mass of focused data is valuable for making consensus recommendations. The most studied patient domains in the extant HWC literature are obesity and T2D. Therefore, we focus the current study on extracting relevant HWC dosing data from the Compendium for these patient populations. Accordingly, the purpose of this paper is to carefully examine the HWC literature and determine effective HWC doses. Programming variables used to define a HWC dose or prescription (e.g., session frequency and duration) are depicted in Figure 1. It is hoped this analysis will help establish, or at least support a discussion of best practices for, initial dosing of a HWC intervention. Health and wellness coaching programming variables.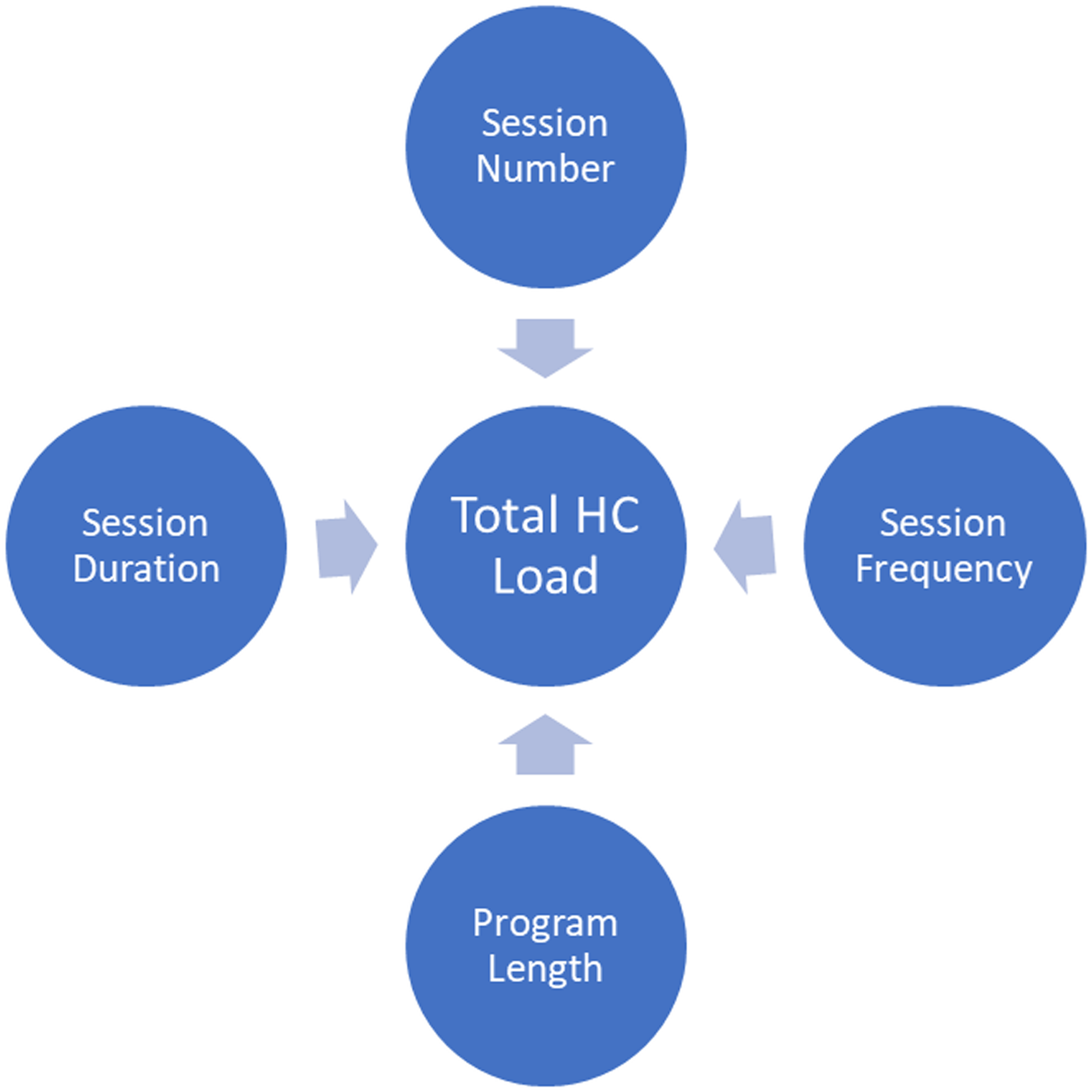
Methodology
The process used in this synthesis of findings report is data mining and extraction from a systematic review. Data was drawn for this analysis from the two Compendium databases.
8
These databases included HWC-related literature published between 2000-2019 in eight categories including cancer, cholesterol, diabetes, heart disease, hypertension, obesity, wellness, and a miscellaneous section. All data-based studies examining diabetes or obesity (N = 102) across the two Compendium databases were extracted, compiled, and examined. All included studies had to (1) meet a criteria-based definition of HWC as previously described,
8
(2) employ quantitative or mixed methods designs, (3) study T2D or obesity as an outcome, and (4) assess the impact of HWC on physiological (e.g., glycosylated hemoglobin and body mass) and/or psychological/behavioral change outcomes (e.g., self-efficacy, quality of life, health risks, and stage of change). Exclusion criteria for the current examination included case studies, meta-analyses, qualitative analyses, and studies without either physiological or psychological/behavior change outcomes. As depicted in Figure 2, 88 studies were retained with physiological and/or psychological outcomes reported. PRISMA flowchart of study inclusion.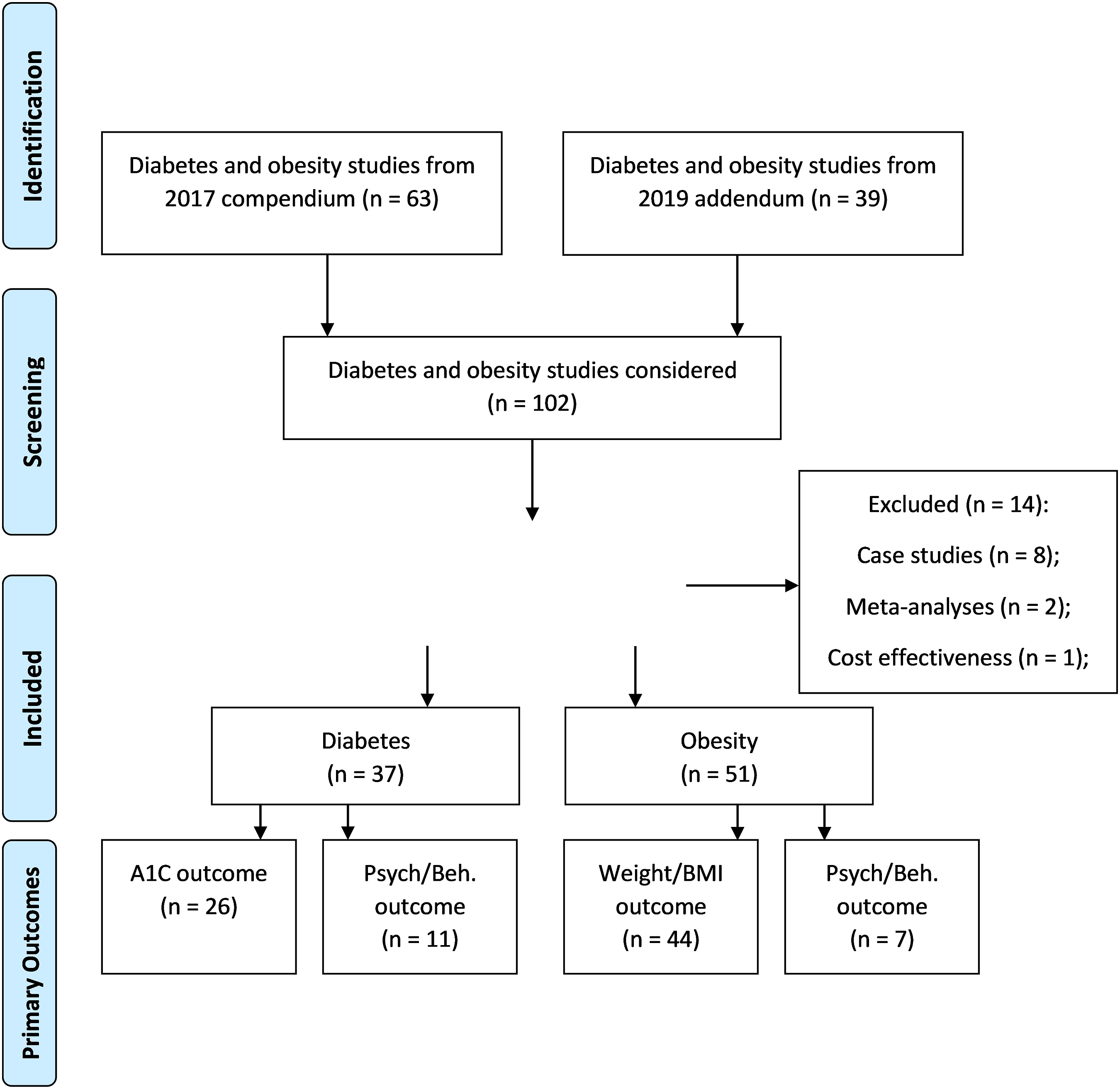
Authors (MK and AF) worked independently to review data published in the Compendium8,9 for the identified studies as well as extract additional HWC programming information from each article such as HWC session duration and program length. Each reviewer’s work was verified by at least one of the other reviewers. The ultimate goal of this exercise was to derive initial dosing recommendations for clinical practice of HWC. Accordingly, we examined several HWC intervention programming variables: (1) program length (months of coaching), (2) total session number, (3) session frequency (sessions/mo), (4) session duration (min/session), and (5) program load (total hours of coaching). Additional descriptive variables were extracted from Compendium data including sample size, study design, and study length. Following extraction, data from these studies were assembled, described, and analyzed (Figure 3). Initial health and wellness coaching programming guidelines.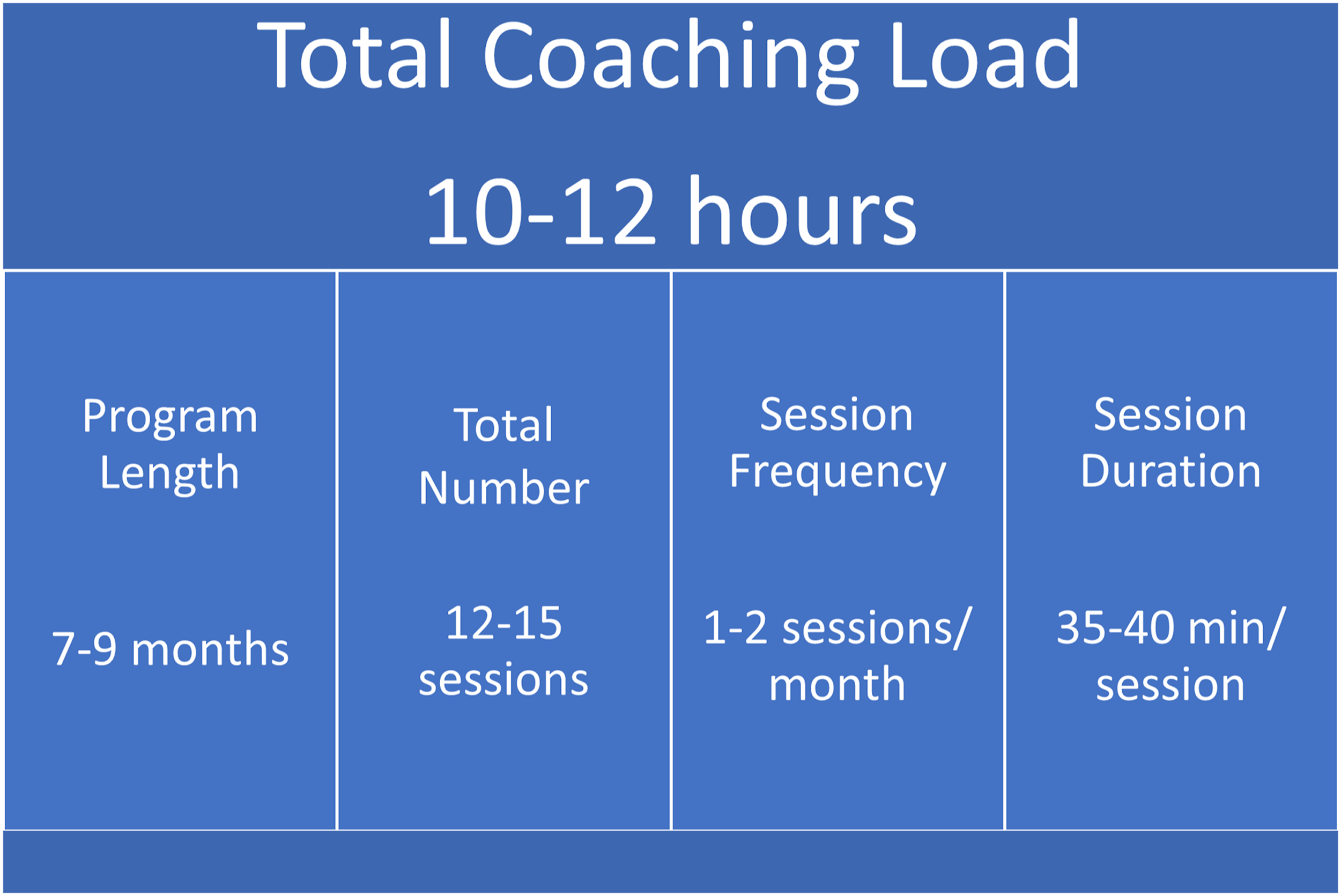
Data Analyses
Descriptive information regarding study characteristics were reported (i.e., sample size, study length, and study design) to provide an overview of included studies. Descriptive information and correlations for HWC programming variables (i.e., program length, total coaching sessions, session frequency, session duration, and program load) were compiled across studies as well as within types of study design, the population studied, and the outcomes examined. Next, four series of comparisons were examined. First, examining all 88 studies, programming variables from randomized control trials (RCTs) were compared to studies with other designs to determine if expected study quality impacted the applied coaching prescription using independent sample t-tests with Bonferroni corrections applied (P = .007). Second, comparisons in HWC programming between diabetes studies with significant and non-significant findings were examined using independent sample t-tests with Bonferroni corrections applied (P = .01). In other words, HWC programming variables in studies effectively reducing A1C or enhancing psychological/behavioral outcomes were compared to those that did not produce a statistically significant finding. Third, comparisons between HWC programming variables between obesity studies with significant and non-significant findings were examined using independent sample t-tests with Bonferroni corrections applied (P = .01). Finally, HWC programming variables for obesity and diabetes studies were compared using independent sample t-tests with Bonferroni corrections applied (P = .01) to determine if unique recommendations were needed for each condition.
Results
The combined results for all studies (N = 88) are presented here before describing HWC programming variables separately for diabetes and obesity studies. As seen in Figure 3, across all examined studies (i.e., diabetes and obesity) the average HWC program length was approximately 8 months (M = 8.324; SD = 5.951) with 12 coaching sessions over the course of this time (M = 12.200; SD = 13.162). Also highlighted in Figure 3, HWC frequency approached twice monthly (M = 1.993; SD = 1.530), session duration averaged nearly 40 minutes (M = 38.46; SD = 21.802) and total coaching program load over the program length was about 11 hours (M = 11.324; SD = 20.394). Studies with longer program length had more coaching sessions (r(84) = .346, P = .001) but lower frequency (r(84) = −.467, P < .001) suggesting HWC sessions were spread over a greater period of time. Frequency was also related to session length, suggesting studies with more frequent coaching sessions also incorporated longer sessions, r(52) = .348, P =.013. HWC programming variability, as indicated by range, was extremely large with HWC program length between 2–24 months and number of sessions ranging from 2 to 96. Similarly, session frequency (ranging from .17 to 7.00 sessions/mo) and session duration (i.e., ranging from 5 to 105 min) were applied in a large variety of ways across this wide range of HWC studies.
Health Coaching Programming Variables and Descriptive Information: All Retained Studies Comparing RCT to Other Designs.
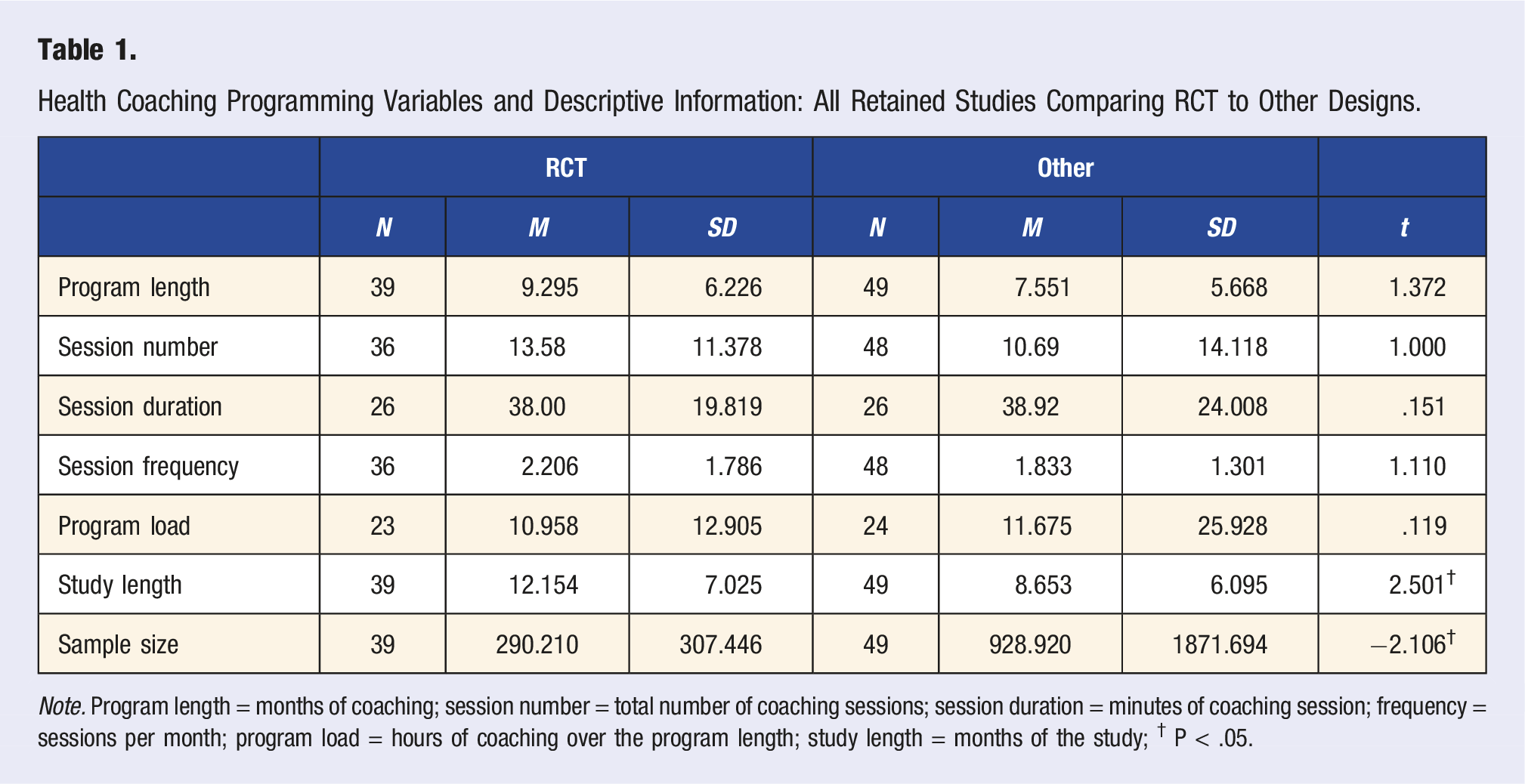
Note. Program length = months of coaching; session number = total number of coaching sessions; session duration = minutes of coaching session; frequency = sessions per month; program load = hours of coaching over the program length; study length = months of the study; † P < .05.
Diabetes
There were 37 HC studies evaluating HWC in pre-diabetic or diabetic participants, with 16 utilizing a RCT design. Overall, HWC program length averaged about nine months (M = 9.19; SD = 5.89) ranging from 2 12 to 24 months.13,14 HWC session frequency was between 1 and 2 per month (M = 1.66; SD = 1.10) ranging from a low of .167 14 to a high of 4.5 sessions per month. 15 The coaching visit schedule was not always static, and sessions might vary based on participant needs and goals.16,17 Often studies decreased HWC frequency over time13,18-22 or followed an initial schedule of coaching sessions with a follow-up booster. 23
Twenty diabetes studies reported HWC session duration averaging 35-40 minutes (M = 36.40; SD = 14.77) and ranging from 1015 to 60 minutes.16,24,25 Session duration could vary throughout the study. For example, a longer session duration might have been utilized initially with shorter sessions following. Program load, or the total time of coaching in these diabetes studies, averaged a little over 5 hours (M = 5.27; SD = 2.98), ranging from a low of 1.33 26 to 12 h 16 over the course of the study.
Diabetes: Health and Wellness Coaching Programming Variables for Studies Examining A1C and Psychological/Behavior Outcomes.
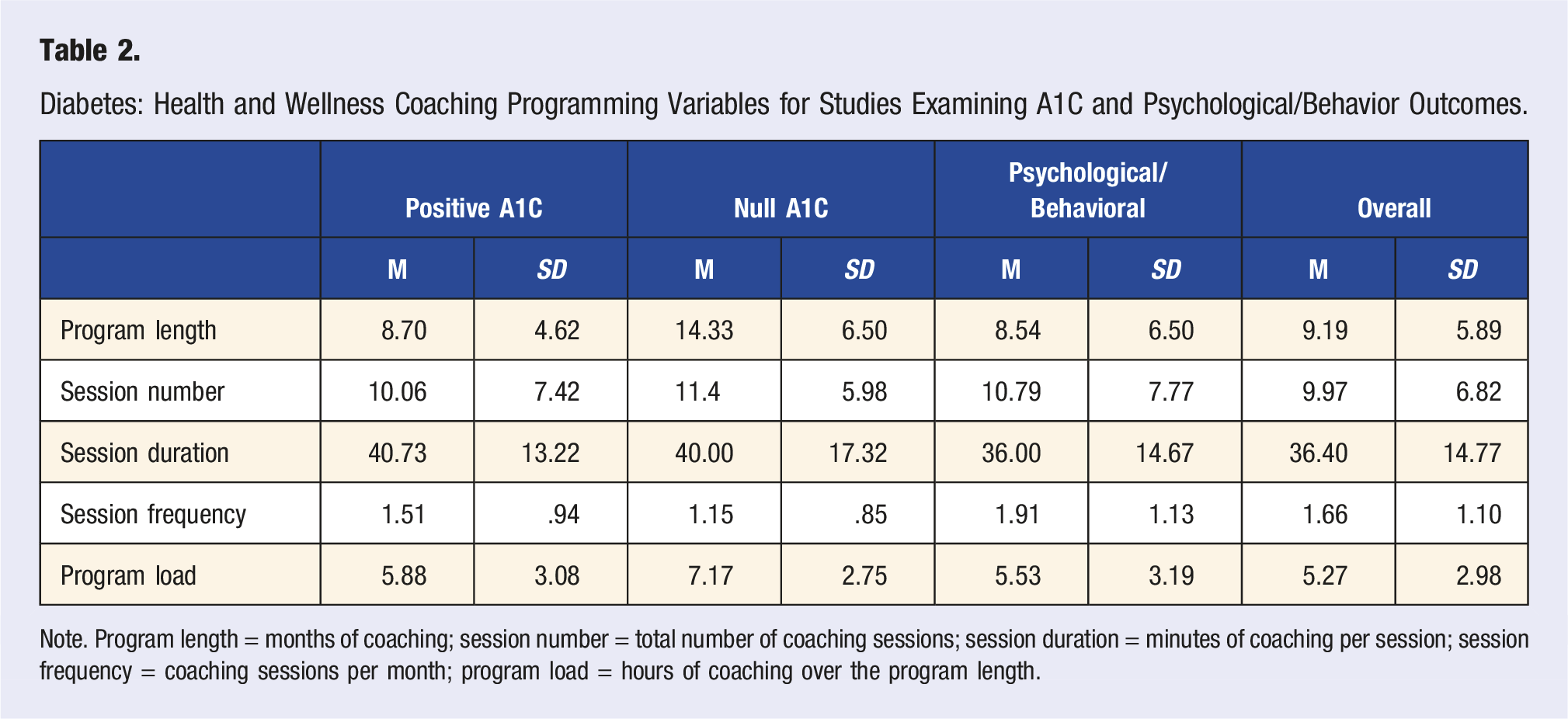
Note. Program length = months of coaching; session number = total number of coaching sessions; session duration = minutes of coaching per session; session frequency = coaching sessions per month; program load = hours of coaching over the program length.
Thirty-seven studies examined psychological or behavioral outcomes. These 37 included 16 studies which also examined A1C (i.e., examined psychological or behavioral outcomes and A1C) and 11 diabetes studies which did not assess A1C. In other words, these 11 studies examined HWC in a diabetic population, assessing only psychological or behavioral outcomes. All but one 27 had positive psychological or behavioral change results attributed to coaching. Coaching programming variables for these 37 studies are detailed in Table 2. Considering the 11 studies that did not assess A1C (i.e., assessed only psychological/behavioral outcomes), coaching frequency ranged from 4 sessions over 24 months 14 to 27 sessions over 6 months. 15 Session duration was as low as weekly 10-minute sessions 15 to four sessions totaling 3 hours (45 min average). 12 As for total HWC program load, Adams et al 26 utilized four 20-min sessions over 12 months (totaling 80 min of coaching) while Schneider et al 29 employed eleven 40-min sessions over 12 months (totaling 7.33 h of coaching). Both ends of the spectrum of total coaching hours over 12 months were reported to help in reaching health goals.
Obesity
There were 51 HWC studies of obesity recovered, retained, and examined with 23 utilizing a RCT design. Overall, program length averaged just over seven months (M = 7.370; SD = 5.559) while ranging from 1 30 to 24 months of coaching.31-34 HWC session frequency averaged over two sessions per month (M = 2.25; SD = 1.706) with a range35-38 from .17 39 to 740,41 sessions per month. As seen with diabetes, the obesity studies’ coaching schedule was not static, and sessions could vary based on participant preferences or goals.33,35,39 Some decreased in frequency over time,31,41-46 or had the initial coaching program followed by boosters or maintenance,40,41,47-49 or provided unlimited access to coaches. 37
Session duration was reported in 32 studies with average of nearly 45 min (M = 43.50; SD = 31.91) and sessions ranging from 5-10 min 46 to up to 120 min. 50 Session duration varied based on the session order in six studies with a longer initial session (up to 120 min) followed by shorter coaching sessions on a regular frequency.39,46,51-53 HWC program load (M = 15.048; SD = 25.310) ranged from as low as 1.67 h 32 to 131.2 h 33 over the course of the study. Three studies had a programming load significantly above the rest.33,54,55
Obesity: Health and Wellness Coaching Programming Variables for Studies Examining Weight/BMI and Psychological/Behavior Outcomes.
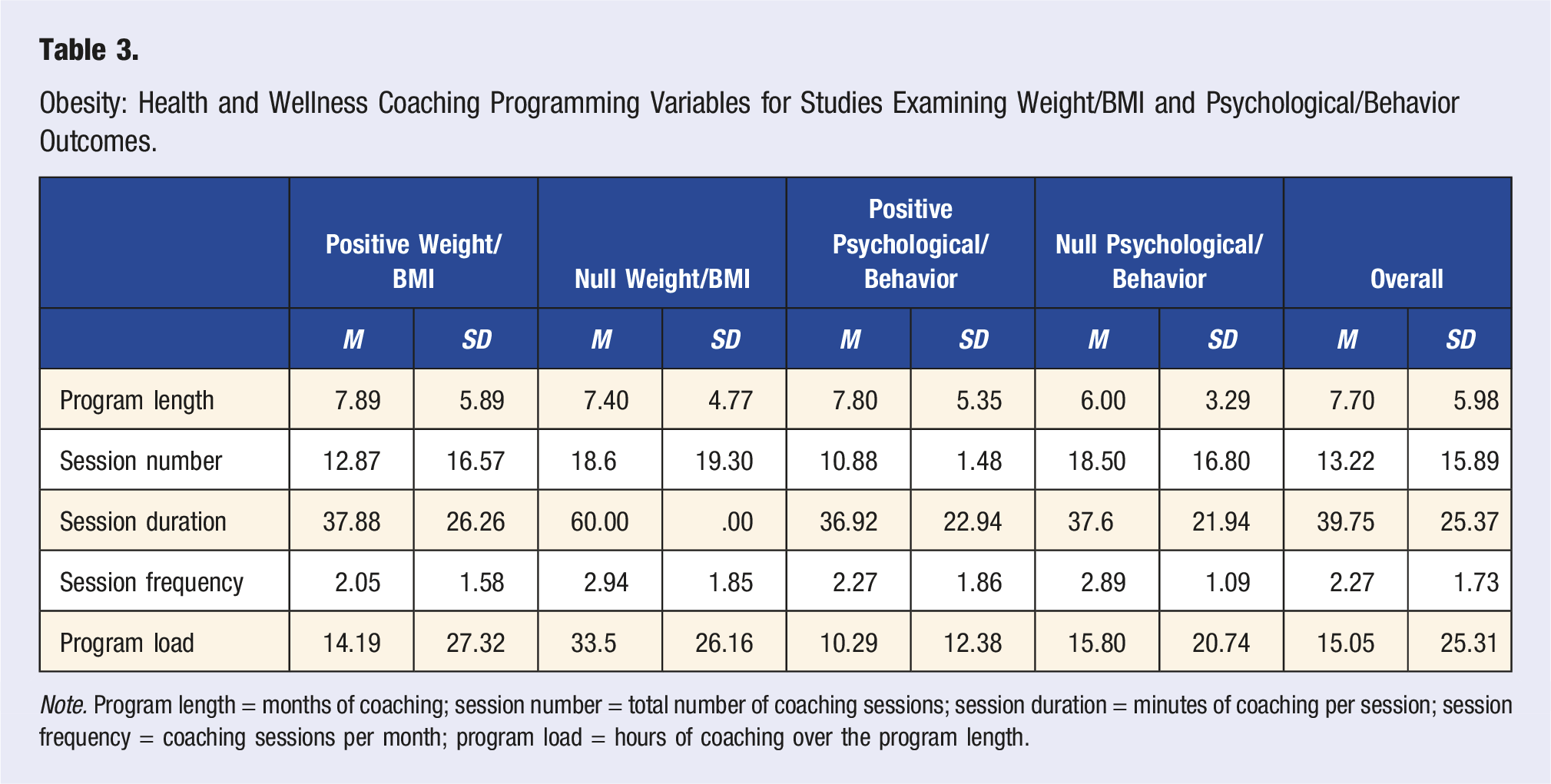
Note. Program length = months of coaching; session number = total number of coaching sessions; session duration = minutes of coaching per session; session frequency = coaching sessions per month; program load = hours of coaching over the program length.
Thirty studies examined psychological or behavior change related outcomes, including seven studies which did not assess changes in weight or BMI and 23 studies examining both weight/BMI and psychological or behavioral outcomes. Coaching information for these 30 studies is detailed in Table 3. All seven studies examining only psychological or behavior change outcomes had positive results attributed to coaching. Six studies examining both psychological/behavior change and weight/BMI outcomes did not report any significant psychological/behavior findings with two studies not finding a HWC impact on either weight- or psychological-related outcomes.55,57 Coaching frequency and program length in the seven studies examining only psychological, or behavioral change outcomes, ranged from 2 sessions over 12 months35-39 to 24 sessions over 6 months.44,58 Session durations as short as 5 44 and up to 60 min 51 were reported. When examining HWC programming variables for studies finding beneficial (n = 24) v. no effect on psychological (or behavioral) outcomes (n = 6), there was no difference in any of these variables. In other words, these HWC studies of obesity, regardless of subsequent findings, used statistically similar doses of treatment.
Diabetes v. Obesity
Diabetes v. Obesity: Health and Wellness Coaching Programming Variables.
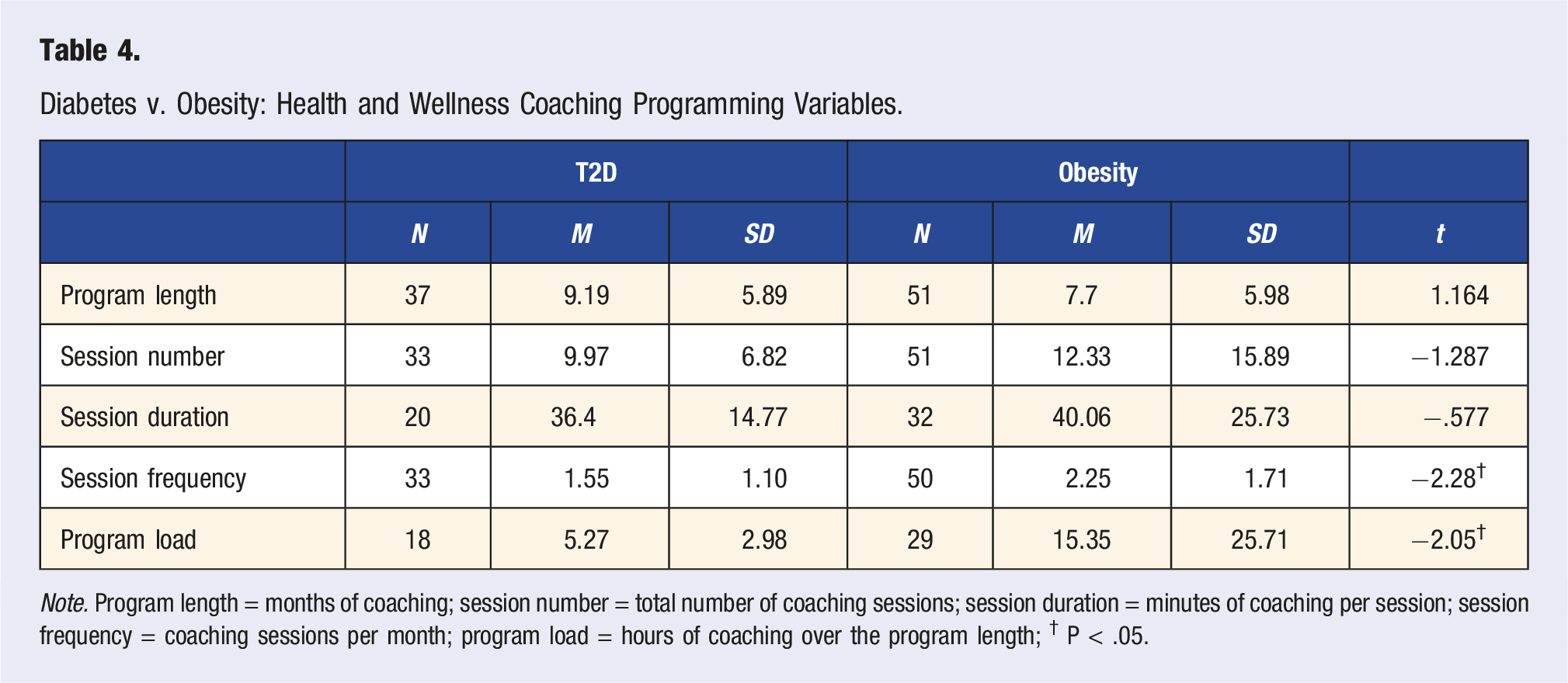
Note. Program length = months of coaching; session number = total number of coaching sessions; session duration = minutes of coaching per session; session frequency = coaching sessions per month; program load = hours of coaching over the program length; † P < .05.
Discussion
In this paper, we determined a general initial dosage, or prescription, for HWC programming of obese and T2D patients. Mindful that RCTs may have been higher quality than other research designs, we first compared HWC programming variables between study designs and found no difference. Similarly, no differences were found between HWC programming variables in studies finding significant and no statistically significant findings in primary outcomes. These results allowed us to combine all studies for a more powerful recommendation from a larger data base. Across all examined studies, including both T2D and obesity, initial HWC programming was determined to be 12 sessions of about 40-min duration provided over 7-8 months. Using similar HWC prescription, many studies have reported favorable findings in patients with diabetes16,22,59 and obesity.43,50 This is not to say our recommendation of 12 sessions is the minimum number for coaching effectiveness. In fact, significant drops in A1C 21 and reductions in weight 60 have been seen with fewer sessions. The same can be said of the session duration and program length variables, both shorter and longer sessions (i.e., min) and programs (i.e., months) can be effective. The initial programming recommendations for HWC provided here are a consensus average from those coaching interventions employed in the published literature. Essentially, these HWC recommendations are derived from expert input because they are based on the work of subject matter experts designing, conducting, and disseminating peer-reviewed studies.
When examining only diabetes HWC studies, we compared HWC papers finding a significant difference in A1C to those not reporting an A1C effect and found no difference in HWC programming variables employed. Keeping in mind that the number of studies not reporting improvement in A1C after HWC was modest (only 7 of 27), this finding simply allowed us to combine all studies to make a recommendation based on a larger view of the literature. Therefore, regarding session duration, frequency, and program length, we determined using 40-min sessions and having about 11 sessions over 9-10 mo is an effective HWC programming dose for T2D patients attempting to lower A1C. This prescription will likely also produce other related medical and psychological benefits.38,39 It should also be noted this recommendation is different from the DPP which makes use of group coaching over 22 sessions in the first year. The current analysis did not examine group coaching and future considerations should be made to optimize recommendations for this valuable form of coaching. While the HWC programming recommendations derived presently for T2D are essentially the same as the general HWC prescriptive recommendation, there were subtle and possibly clinically relevant differences when examining HWC programming variables for working with obese patients. As with T2D, we again compared papers with significant physiological findings to those reporting no change in weight (only 5 of 44) and saw no difference in HWC programming variables allowing us to combine results. Accordingly, the initial HWC programming recommendation for obese patients is 14 sessions of about 45-min duration over 7-8 months. While program length, session number, and duration did not prove to be statistically different between obese and T2D studies, the values for these variables led to a statistical trend in session frequency and total coaching program load. In other words, the number of sessions and session duration were both marginally greater when working with obese patients than seen with T2D resulting in a greater coaching load over a shorter program length. Specifically, studies with obese patients yielded over two sessions per month with about three times the total number of total hours of coaching than T2D. Therefore, the HWC intervention used for treating obese patients is determined to be slightly more intense, (i.e., more frequent sessions with more HC hours in a shorter programming period) than seen in T2D patients. This seems logical given the perceived urgency for weight loss at the start of an intervention compared to the expected life-long management of a condition like T2D. This recommendation of 14 sessions of 45-min duration stands in contrast to current obesity counseling recommendation of 22 sessions of 15 min. It is conceivable that longer duration sessions allow greater exploration of psychological enablers and barriers to changing behaviors. Future studies comparing these protocols need to be completed to make more definitive statements about optimal HWC programming recommendations for effectiveness in managing obesity.
These standardized HWC initial programming recommendations do not reduce the potential to vary or customize an HWC prescription for any given individual. A physician might immediately determine the initial dosage should be more or less. More likely, a patient working with a coach might agree more, or less, coaching than the initial recommendation is better suited to their needs. As with any other intervention, the option for extending or terminating treatment should always be considered according to what will best serve the patient. The recommendations offered here are meant to provide a reasonable initial programming dosage of coaching that should be effective in most circumstances.
Other examples of varying HWC dosage were employed in many of the studies reviewed.38,51,52 Frequently, the HWC program began with an initial session of greater duration than the visits that followed, as represented in the HWC CPT codes where the initial session is one hour and the subsequent sessions are 30 min. The first session should likely include intake questions, assessments, orientation, visioning, goal-setting, and other required initial meeting procedures. It seems appropriate that the first coaching session, as with many other effective interventions, should allow for a longer duration. Still other studies varied HWC frequency over the duration of the program. The use of greater initial HWC session frequency with a lower frequency employed after 6-12 months was a common strategy.31,42,43 Another manipulation of HWC dosing over time involved discontinuing the process after the initial period but then providing a booster HWC session several months later.47-49 These strategies align with clinical observations of patients extending benefits derived from HWC well after the first year of intervention. It is difficult to speculate on the effectiveness of these various practices for altering the coaching dose. As with any other evolving medical intervention, there is a real need for comparative effectiveness studies of various HWC protocols. Given our current data synthesis, we understand how to initially prescribe HWC, but have not fully elucidated the optimum and most cost-effective means for delivering HWC interventions. The presently recommended HWC prescription, however, is documented as valuable for improving the health status of obese and T2D patients.
Beyond obesity and T2D, there is good evidence to support HWC as a beneficial intervention for those suffering with cancer, hypertension, heart disease, MS, fibromyalgia, and a host of other conditions.8,9 The optimal initial HWC programming recommendations for these groups may be different than seen with obesity and T2D. Given the established impact of HWC on lifestyle-related diseases through behavior change, it is reasonable to speculate the coaching process may be most effective at improving prognosis of patients diagnosed with metabolic syndrome. This has been demonstrated in limited study. 61 Further research will have to better establish the scope of HWC intervention effectiveness, related programming recommendations for these patient populations, and ultimately ascertain if HWC treatment passes the test of cost: benefit analysis.
On the topic of HWC programming recommendations, it should be clear this paper provides only a beginning for the exploration. There is a definite need for future research to compare effectiveness of varying HWC intervention dosing on a variety of conditions, including obesity and diabetes. Most medical treatments change over the years with more specific and user-friendly medications developed as processes are refined. Examples of this also abound in the field of dietetics with recommendations on what to eat (or avoid eating) changing over time. 62 Recently, a basic tenet of exercise prescription was challenged and may result in a new paradigm for exercising recommendations. 63 We should expect a similar trajectory for HWC future as we learn more about the scope of use and specifics of application.
The HWC profession needs guidelines to help with the initial prescription for a HWC intervention. As with other interventions (e.g., physical therapy, cardiac rehabilitation), a patient is ideally given some idea of the nature and course of treatment. The arrival of CPT billing codes will prompt physicians to want to make HWC treatment recommendations to their patients. Accordingly, having programming guidelines available is important. For now, it is apparent that an initial HWC program with 12-15 sessions of about 40 min over eight months will be effective for helping treat obesity and T2D. Prescription for treating obesity might be made slightly more intense (e.g., 15 sessions over seven months) with a somewhat lighter schedule (eg, 12 sessions over 9-10 months) appropriate for T2D interventions. As comparative effectiveness data, and related programming results are made available, we can expect these recommendations to be refined and possibly expanded to include other patient domains.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
Supplemental Material - Dosing of Health and Wellness Coaching for Obesity and Type 2 Diabetes: Research Synthesis to Derive Recommendations
Supplementary Material for Dosing of Health and Wellness Coaching for Obesity and Type 2 Diabetes: Research Synthesis to Derive Recommendations by Gary A. Sforzo, Miranda P. Kaye, Aubrey Faber, and Margaret Moore in American Journal of Lifestyle Medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
GS is Research Advisor for Wellcoaches Corp; MK has no potential conflicts to report; AF has no potential conflicts to report; and MM is CEO and founder of Wellcoaches Corp
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.