
Abstract
Purpose: The study was to evaluate the physical condition and mental health of Chinese college student COVID-19 survivors, and to perform severity clustering of physical symptoms. Participants: The study finally included 1912 Chinese college students. Methods: A total of 33 symptoms including general physical symptoms, cardiopulmonary system, digestive system, neurological system, mental health and other symptoms were investigated three months after recovery from COVID-19, and these symptoms are identified using latent class analysis. Results: Three clusters were identified through latent class analysis: 13.2% with severe impairment (cluster 1), 27.2% with mild physical symptoms (cluster 2), and 59.5% with no or mild symptoms (cluster 3). The students who smoked, drank alcohol, did not exercise, or had a history of underlying medical conditions were more likely to have moderate to severe symptoms. Conclusions: Young COVID-19 survivors with a history of underlying diseases and unhealthy habits are more likely to have moderate to severe COVID-19 sequelae. Varying degrees of symptoms should be treated with different rehabilitation plans.
“The findings indicate that survivors in three different clusters require distinct and targeted prevention and management strategies.”
Introduction
As of January 2024, the coronavirus disease 2019 (COVID-19) pandemic has resulted in over 700 million confirmed cases worldwide, spanning more than 200 countries, with a mortality toll exceeding 7 million. 1 Since January 8, 2023, China has officially lifted the Class A infectious disease prevention and control measures against SARS-CoV-2. This action coincided with a rapid increase in SARS-CoV-2 infections, particularly among college students, leading to a pronounced trend of cluster infections in China. Moreover, a significant proportion of college students contracted COVID-19 approximately one month following the cessation of these control measures. The following symptoms and different degrees of COVID-19 sequelae appeared successively. Most patients have recovered from varying degrees of mild to moderate symptoms, but epidemiological and clinical studies found that persistent symptoms after COVID-19, continue to affect public health. These symptoms are described by a series of terms, such as long-COVID-19, post-COVID-19 condition, post-acute COVID-19 syndrome or COVID-19 sequelae,2,3 which defined as “condition that occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis” by the World Health Organization (WHO). 4
Numerous studies have shown that SARS-CoV-2 infection has prolonged damage to different organ systems, encompassing the pulmonary, cardiovascular, neurological, digestive, and integumentary systems.5–11 Based on a meta-analysis of COVID-19 persistent symptoms, the proportion of patients with COVID-19 sequelae may be between 10% and 30% of people with SARS-CoV-2 infection, 10 the most common subsequent symptoms are fatigue, dyspnea, cough, 12 anxiety and depression,13,14 nearly half of patients are limited in daily activities, 15 and the understanding of such impacts is constantly evolving. A systematic review of persistent symptoms in hospitalized patients with COVID-19 found that 72.5% of patients developed at least one symptom after 60 days or six months after COVID-19 diagnosis, with the longest-lasting reported persistent symptoms being fatigue and shortness of breath. 16 Furthermore, the emergence of subsequent COVID-19 symptoms correlates closely with persistent impairments in daily functioning, potentially precipitating inevitable psychiatric manifestations, including brain fog, cognitive decline, anxiety, depression, and sleep disturbances, among survivors.13,17
A survey conducted in the United States indicated that young adults accounted for approximately 5% of patients hospitalized for COVID-19. The rate of adverse outcomes among hospitalized young individuals is high, with obesity, hypertension, and diabetes being associated with increased risks. 18 Given that college students are typically between the ages of 18 and 25, the immune system, nervous system and endocrine system continue to develop and improve. Understanding the long-term effects of COVID-19 on college students can reveal the specific effects of the SARS-CoV-2 on body systems. In addition, college students are facing academic pressure, social relationship building and self-cognition challenges. The COVID-19 pandemic may aggravate their psychological problems, such as anxiety and depression, research on this group can understand the physical and mental health of college students in the post-epidemic era. Following the COVID-19 lockdowns, significant disruptions to students’ daily routines have contributed to mental health challenges, including increased anxiety and depression.19–21 Much of the literature indicates that students in social isolation during the pandemic experienced significant emotional challenges, including loneliness, stress, and low mood, which contributed to psychological issues such as anxiety and depression. 22 SARS-CoV-2 does not typically invade the brain in most cases; instead, neurological complications may arise from indirect effects of immune activation. 23 Psychological stress and adverse social factors following COVID-19 may alter neural and endocrine pathways, ultimately impacting gene regulation in immune cells.24–26 In addition, college students are the backbone of the future society, and their health status is directly related to the future health level of society and economic development. Ensuring their health recovery after COVID-19 infection can help increase the resilience of society as a whole.
Therefore, it is necessary to explore the general characteristics and long-term consequences of young COVID-19 survivors, to classify their symptoms accurately, and to effectively prevent illness and pain among this demographic. So we conducted an epidemical study of college students in Anhui, China, and use latent class analysis to classify the phenotype of persistent symptoms and predict cluster-associated factors, which will provide evidence to guide the development of COVID-19 sequelae recovery interventions in young people.
Methods
Study Design and Recruitment
We recruited 2539 college students from various universities in Anhui Province, China, from 10 June to 30 August 2023. We collected a total of 2256 complete questionnaires, excluding 282 participants who did not complete the questionnaire. Then we excluded 273 participants who had not been infected with COVID-19 and 71 repeat questionnaires. The 71 repeated questionnaires were caused by the online system bugs during the data collection process and we excluded them. Finally, 1912 participants were included (Figure 1), with a response rate of 88.9% (n = 2256/2539) and a valid questionnaire rate of 96.4% (n = 1912/1983). All included participants had recovered from COVID-19 at least 3 months prior to the study. Participants were administered a questionnaire encompassing basic demographic information, lifestyle details, and post-COVID-19 symptoms. Due to the summer vacation period, a hybrid approach of online and offline questionnaires was employed. Most respondents were queried regarding post-COVID-19 symptoms. Informed consent was obtained from all study participants before all study procedures. Demographic characteristics of COVID-19 sequela include gender, age, education level, smoking and alcohol consumption habits, physical activity level, frequency of fruit and vegetable intake, use of health supplements, presence of underlying medical conditions, COVID-19 vaccination status, and body mass index (BMI). All participants were informed of the purpose of this study and signed an informed consent form. All completed questionnaires will be securely stored and meticulously reviewed for accuracy and completeness utilizing the questionnaire platform. Flow chart of the study.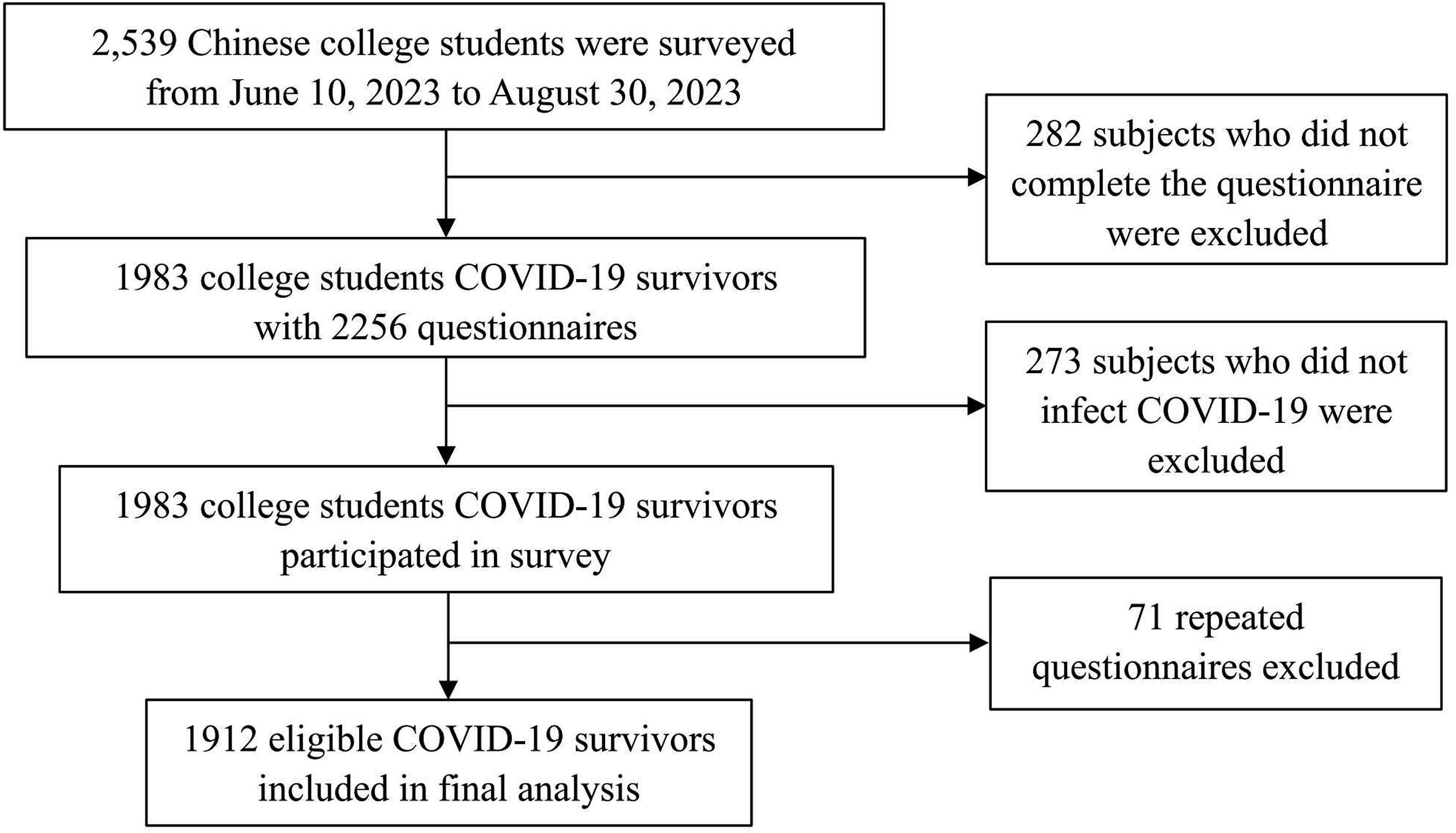
Ethical Considerations
This study was approved by the Ethics Committee of Anhui Medical University (Approval No. 83230329), and all participants were required to provide written informed consent for admission.
Baseline Characteristics
The study collected data on 33 follow-up symptoms from participants, encompassing five organ systems: systemic, cardiopulmonary, mental, neurological, digestive, visual, auditory, and reproductive systems (Supplemental Table S1). Among these, 32 symptoms were asked through self-created questions, while the anxiety symptom was assessed using a validated scale. The anxiety symptoms measured in the appendix (Supplemental Table S1) were assessed by the Self-Rating Anxiety Scale (SAS), which consists of 10 items: (1) I was plagued by fatigue; (2) I get tired quickly; (3) I don’t do much during the day; (4) I don’t have enough energy in my daily life; (5) (Physically) I feel exhausted; (6) I have trouble getting things started; (7) I don’t think clearly; (8) I have no desire to do anything; (9) (Mentally) I feel exhausted; (10) I am not able to concentrate very well when doing things. Participants rated each item on a scale of 1 to 5 (1, never; 2, sometimes; 3, usually; 4, often; 5 always), with the total score of the ten items multiplied by 1.25 to derive the anxiety total score. A total anxiety score below 50 indicates normalcy; scores ranging from 50 to 59 signify mild anxiety, while scores between 60 and 69 indicate moderate anxiety, and scores of 69 or higher denote severe anxiety. A SAS score exceeding 50 indicated the presence of at least mild anxiety symptoms. In latent class analysis, SAS items were recoded as dichotomous variables.
Statistical Analysis
Continuous variables are expressed as the mean and standard deviation (SD) or median and interquartile range (IQR). Binary and categorical variables are presented as counts and percentages. The basic characteristics of the participants were stratified based on the presence or absence of sequelae symptoms. The chi-square test is used to identify differences in proportions among multiple categories. One-way analysis of variance (ANOVA) was utilized to test for differences between classes for normally distributed continuous data, and the Kruskal-Wallis test was used for non-normally distributed data.
To identify subsequent symptom cluster in COVID-19 survivors, we performed unsupervised clustering of self-reported general physical symptoms as well as cardiopulmonary function, digestive system, neurological system, mental health, audiovisual and reproductive symptoms using latent class analysis (LCA). The final number of categories is determined based on conceptual implications, the minimum estimated class proportion, and statistical model fitting indices, such as Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), Adjusted BIC (aBIC), and Entropy. 27 The Lo-Mendell-Rubin (LMR) test is also used to determine the number of classes in a latent class analysis. 28 This is obtained by running a k-class while performing a k-1 class analysis and using the derivative of the model to calculate the P-value. A low P-value rejects the K-1 model in favor of the K-1 model. To explore the predictors of subsequent symptoms, we employed multiple logistic regression for subsequent symptom clusters derived from latent class analysis. We adjusted for gender, age, physical comorbidities, COVID-19 vaccination status, and anxiety. All tests were two-tailed, and a P-value of less than 0.05 was considered statistically significant. Latent class analysis was performed using Mplus version 8.3 and other analyses were conducted using SPSS 23.0.
Results
Demographic Information
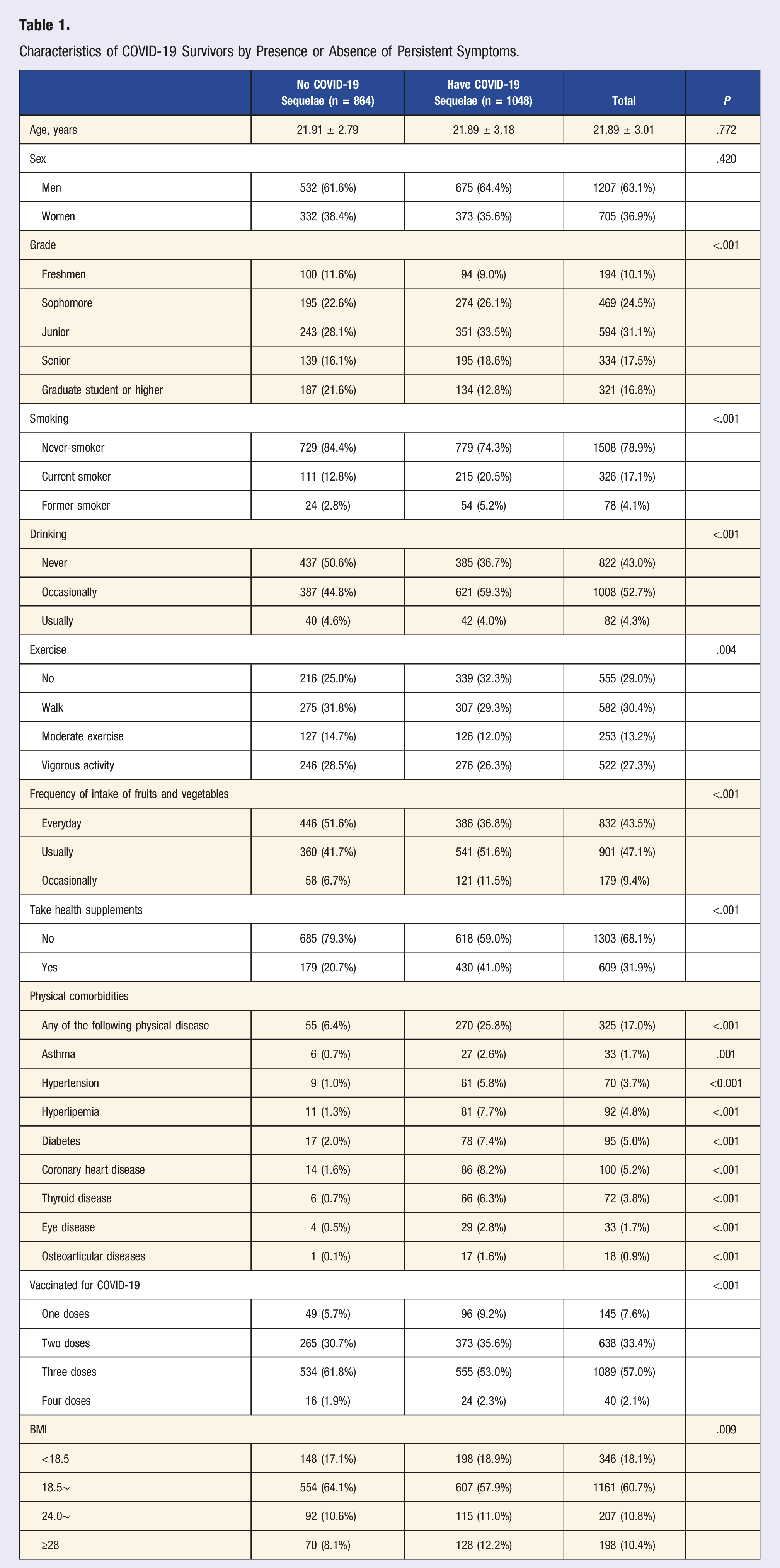
Characteristics of COVID-19 Survivors by Presence or Absence of Persistent Symptoms.
LCAs and the Symptoms Analysis
We performed LCAs ranging from 1 to 6 class and listed various model fit indices for each. The results showed that as the number of classes increased, AIC, BIC, and aBIC all decreased. The 1-class model exhibited the highest AIC, BIC, and aBIC values, suggesting that it deviates the most from the data compared to other models. Although the entropy of the two types of models was the highest, the LMR test results were not significant. After specifying the 3-level model, AIC, BIC, and aBIC stabilized somewhat. Both the 2-class and 3-class models yielded significant LMR and BLRT values (P < .0001), yet the 3-class model exhibited lower AIC, BIC, and aBIC values, suggesting superior model fit compared to the 2-class model. Given the more balanced sample proportions and the aforementioned metrics, we selected the 3-class model due to its greater parsimony and improved classification ability (Table S2).
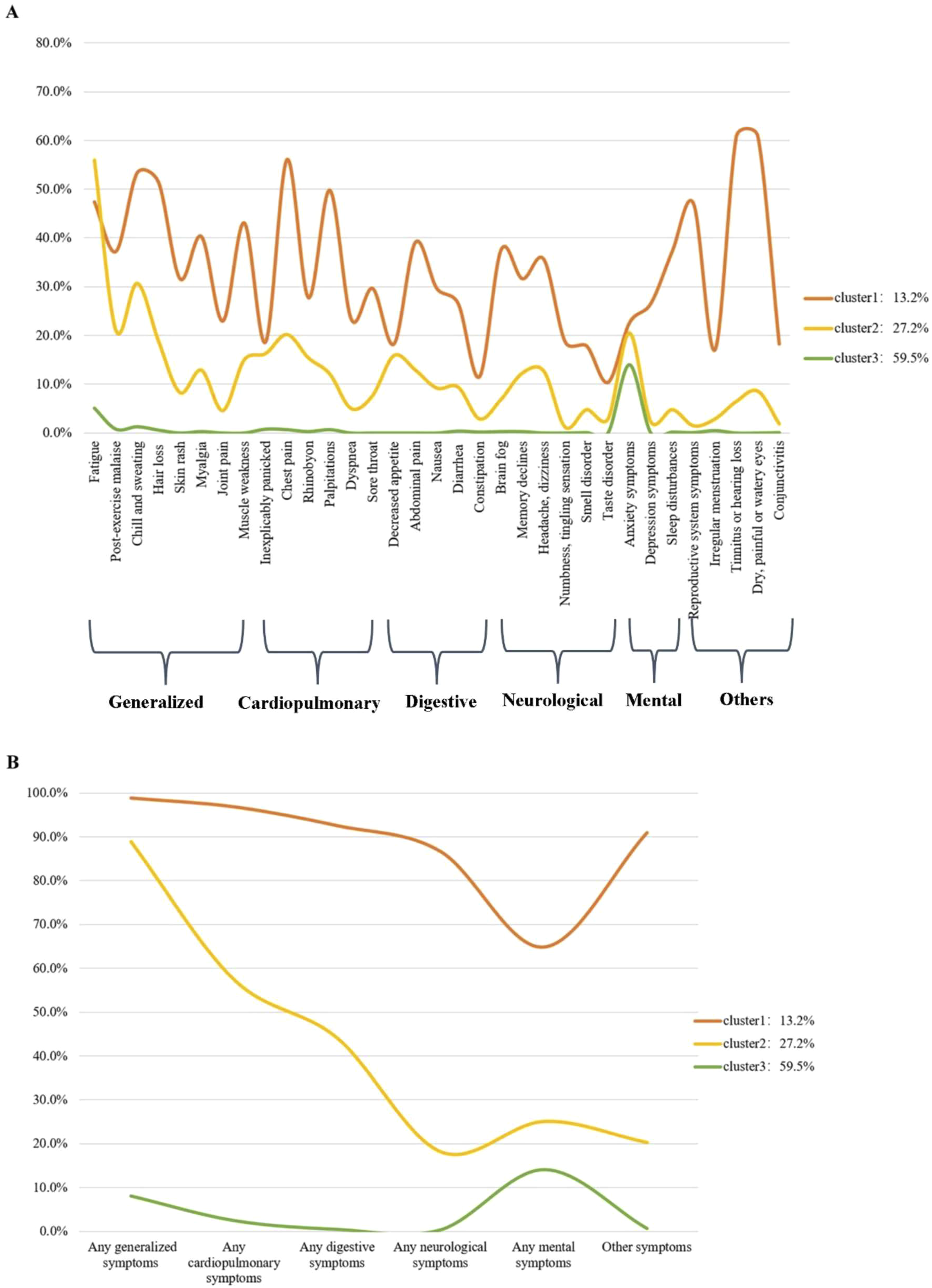
We utilized latent class analysis to classify multiple sequelae phenotypes in 1912 participants, considering 33 symptoms across various systems. We finally identified three COVID-19 sequelae clusters. The first cluster has a higher scoring probability, indicating that this cluster of college students has more follow-up symptoms after the epidemic, so it is labeled as a “severe cluster.” This cluster comprised the smallest number of college students (n = 253; 13.2%), predominantly experiencing general symptoms (n = 250; 98.8%), cardiopulmonary symptoms (n = 245; 96.8%), digestive system symptoms (n = 234; 92.5%), and symptoms related to the visual, auditory, and reproductive systems (n = 230; 90.9%). The second cluster (n = 521; 27.2%) was defined as a “moderate cluster” because it scored a moderate probability of depression and anxiety, lower than the first cluster and higher than the third cluster. These college students primarily experienced moderate physical impairments following the COVID-19 infection, including general symptoms (n = 463; 88.9%), cardiopulmonary symptoms (n = 299; 57.4%), digestive symptoms (n = 230; 44.1%), and psychological symptoms (n = 95; 25.1%). The third cluster of college students (n = 1138; 59.5%) primarily consisted of psychological disorders such as anxiety and sleep disorders (n = 160; 14.1%), along with general physical symptoms (n = 92; 8.1%). The probability scores for various symptoms were low, hence labeled as the “mild cluster” (Figures 2 and 3). In Figure 3, the Y-axis represents the probability that the cluster will have subsequent symptoms, the X-axis represents the type of symptoms, and the three lines show the symptom patterns of the three subsequent symptoms of COVID-19 infection. College students with physical illnesses were more prone to experiencing multisystem follow-up symptoms, encompassing general symptoms, cardiopulmonary symptoms, digestive symptoms, neurological symptoms, psychological disorders, as well as symptoms related to the visual, auditory, and reproductive systems (P < .05). Persistent symptoms stratified by sex, age, physical diseases and symptom clusters. “*” indicated P < .05. The rate of sequelae symptoms by three sequelae clusters. (A) The rate of sequelae symptoms by three sequelae clusters. (B) The rate of organ systems by sequelae clusters. Cluster 1: Severe group (mostly generalized, cardiopulmonary, digestives and other symptoms) (13.2%). Cluster 2: Moderate group (mainly physical impairment, cardiopulmonary symptoms and digestive symptoms) (27.2%). Cluster 3: No or mild group (no or mild physical and mental health impairment) (59.5%).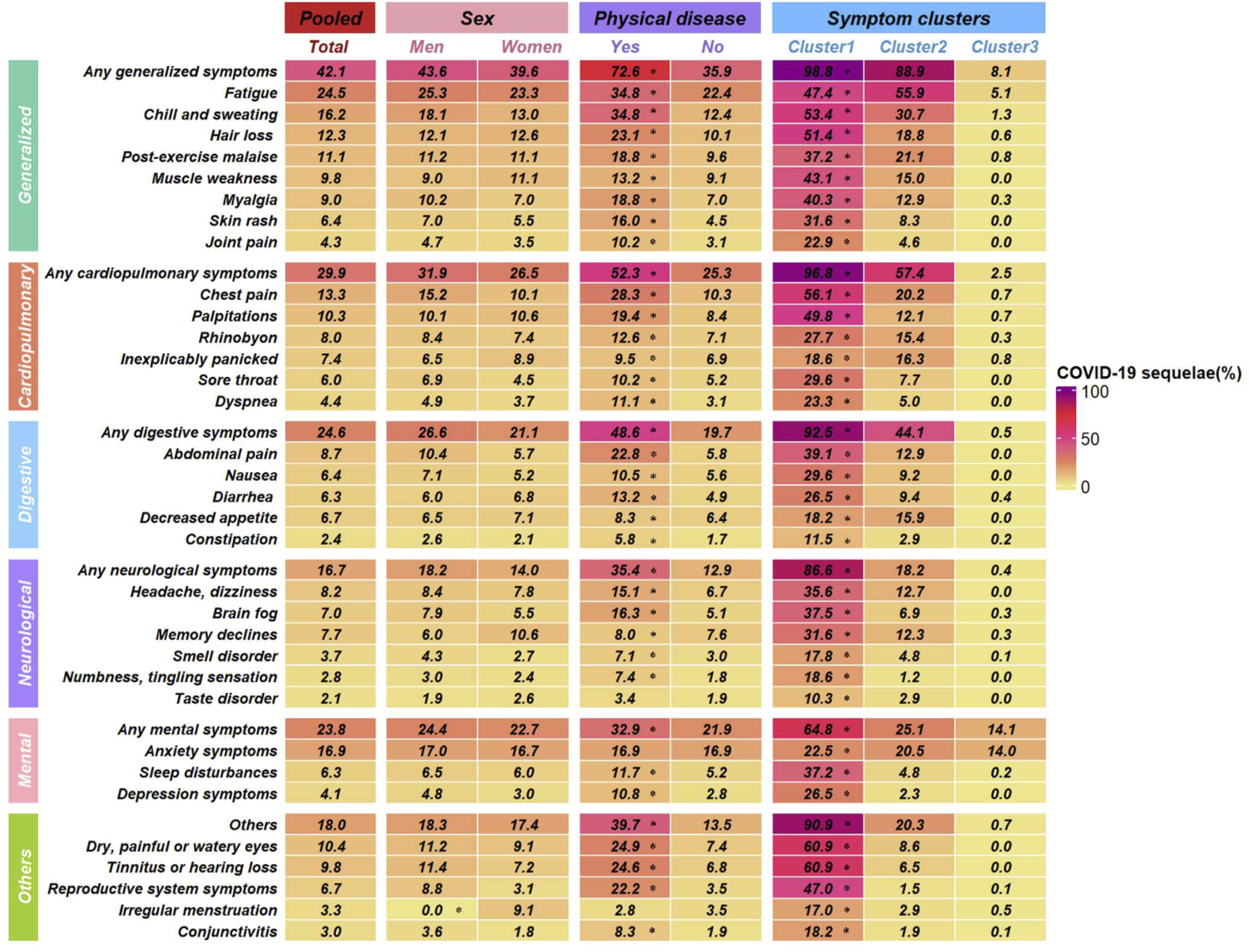
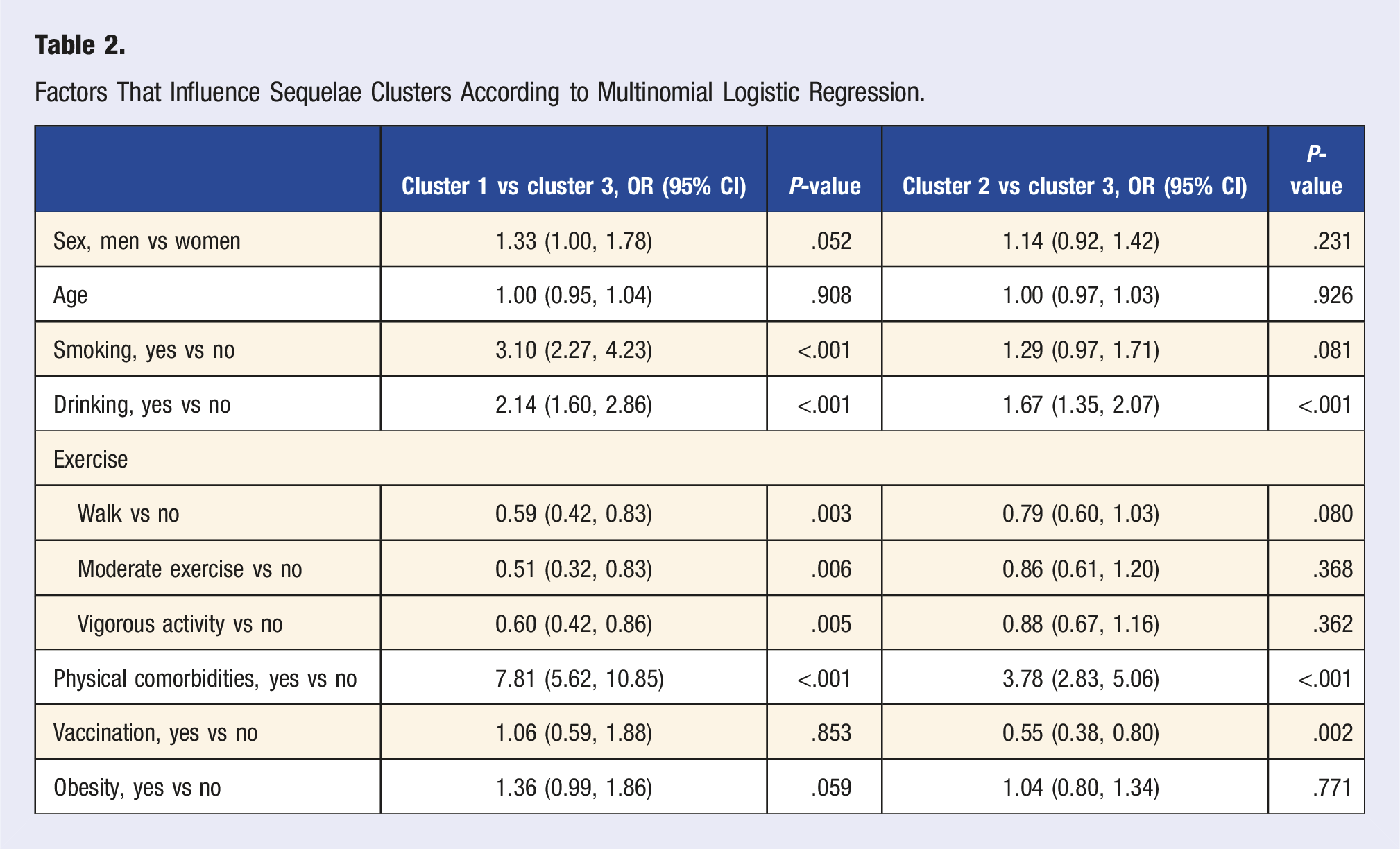
The Risk Factors of Three Clusters
Factors That Influence Sequelae Clusters According to Multinomial Logistic Regression.
Discussion
This study reports the phenotypic population of COVID-19 sequelae in 1912 college student survivors who recovered 3 months after recovery from COVID-19, including multiple organ systems. We identified three distinct clusters: 59.5% participants exhibited either no or mild symptoms, 27.2% experienced moderate symptoms, primarily general, cardiopulmonary, digestive and psychological impairments; and 13.2% survivors suffered from severe symptoms, mainly general, cardiopulmonary and digestive. Vaccination status and pre-existing medical conditions prior to COVID-19 infection are likely associated with the classification of survivors into severe or moderate symptom clusters. The findings indicate that survivors in three different clusters require distinct and targeted prevention and management strategies. We propose a framework to map numerous subsequent symptoms into a precise classification of COVID-19 sequelae phenotypes and offer guidelines for physical recovery and preventive care for college students in the post-pandemic era.
Multisystem Symptoms and Psychological Health
We used a method of LCA to classify 33 post-COVID-19 sequelae based on the severity. Over half of the college student survivors exhibited either no or mild symptoms, a finding consistent with the prevalence rates of asymptomatic or mildly symptomatic clusters reported in a Chinese study. 3 Our results show that a certain percentage of survivors had moderate impairment, mainly general physical, cardiopulmonary, and digestive symptoms. A potential association exists between SARS-CoV-2 infection and subsequent physical dysfunction, including weakened cardiopulmonary function, corroborating findings from studies on varying degrees of cardiopulmonary impairment post-COVID-19. 29 SARS-CoV-2 infection has direct and indirect effects on the myocardial and cardiovascular systems, potentially due to the presence of viral particles in myocardial tissues accompanied by inflammatory cell infiltration.30,31 Concurrent gastrointestinal and respiratory diseases are common, with gut microbiota potentially influencing a spectrum of conditions via the gut-lung axis. This aligns with observed digestive symptoms such as nausea, abdominal pain, and diarrhea among COVID-19 survivors in our study. 32 Gastrointestinal manifestations could stem from direct viral damage to endothelial cells and persistent inflammation, with intestinal microbiota disturbances potentially arising months post-SARS-CoV-2 infection.33–35 Gastrointestinal symptoms may also influence mental health through the gut-brain axis, potentially contributing to anxiety and depression. 36 Six months post-infection, our study observed diverse neurological symptoms among college student survivors, including fatigue, headache, brain fog, and memory loss, largely attributable to immune-mediated autonomic nervous system impairments.37,38 These potential symptoms may affect college students’ learning progress and life satisfaction. Various mechanisms underlie the effects of SARS-CoV-2 on the nervous system, such as virus-induced neurotropism triggering an immune response, pulmonary and multi-organ dysfunction impairing nerve cell function, and responses to multiple neuroinflammatory processes. 8
SARS-CoV-2 has had a profoundly negative impact on the mental health of survivors, and the psychological disorders we studied were assessed by measuring anxiety, depression, and sleep disturbances. Social isolation and quarantine during the pandemic have significantly impacted sleep disorders. Substantial evidence indicates that many individuals experience poor sleep quality and mental health issues following the COVID-19 pandemic, and these conditions often persist after its conclusion. This may be due to the lockdown affecting people’s social activities, as well as their eating and exercise habits, which in turn lead to changes in biological rhythms. 39 Our study showed that the mild cluster may also experience psychological symptoms of anxiety, featuring a higher proportion of anxiety symptoms and a lower incidence of depression compared to the other two studies, potentially attributable to the different scales used to assess anxiety.3,40 In addition, our study found that symptoms such as hair loss, dry eyes, tinnitus and hearing loss are more common in college student COVID-19 survivors, and that viral infections may cause direct or indirect damage to the eye, potentially leading to conditions such as retinopathy or ocular inflammation.31,41
Several studies have discovered that women COVID-19 survivors are more likely to develop COVID-19 sequelae of different systems than men.13,42,43 The reason our results differ from those of previous studies may be that our study subjects were college students rather than a broader age range, and more research is needed to focus on gender differences in COVID-19 sequelae among young adults. Gender differences in COVID-19 sequelae may be related to differences in the function of the immune system between women and men, and infectious and immune diseases manifest differently in men and women. Gender differences in immunity stem from genetic, hormonal and behavioral factors.44–46 The larger rate of memory decline in women in our findings is consistent with an increased risk of persistent neurological symptoms in women in another study. 47 Compared to other studies, our study was predominantly college students with COVID-19 survivors. A higher proportion of follow-up symptoms in our study may be due to young people with long-COVID-19 symptoms being more willing to be evaluated and more sensitive to physical symptoms, contributing to selective bias and a higher observed proportion of COVID-19 sequelae in young adults. 37 In our study, a positive correlation was observed between physical comorbidities and post-COVID-19 symptoms. Physical comorbidities such as hyperlipidemia, diabetes, coronary heart disease, and thyroid disease may exacerbate COVID-19 sequelae 48 and are more likely to be classified as severe clusters.
At the same time, our study also observed that the occurrence of a variety of symptoms is associated with undesirable lifestyle habits, underscoring the need for health education and management of college students with moderate to severe sequelae through multidisciplinary rehabilitation programs. 49 Previous studies have focused on the mental health of students during the COVID-19 pandemic.50,51 The low proportion of depressive symptoms in our survey may be attributed to the strong psychological adaptability of most college students following the COVID-19 epidemic. However academic pressure after the epidemic may cause varying degrees of anxiety, including memory loss, sleep disturbances and distraction. The severe cluster experienced varying degrees of cardiopulmonary symptoms and digestive symptoms, which are believed to impact the academic process. These students require focused mental health interventions and the guidance and assistance of psychologists. In addition, our researches show that vaccination can also effectively protect college students from persistent symptom exacerbations after COVID-19 infection, especially from the mild cluster to the moderate cluster, which also indicates the need for COVID-19 vaccination for college students.52,53
Our study found that the majority of college students belonged to the mild cluster, experiencing primarily physical symptoms, among which fatigue was the most common. Consistent with other studies of COVID-19 sequelae, most of the chronic symptoms gradually recover six months after COVID infection, and may be similar to the pathogenic mechanism of many infectious diseases. 37 Nearly half of the survivors in the moderate cluster had cardiopulmonary sequelae, which was dominated by somatic, cardiopulmonary and digestive symptoms, with chest pain being the most common sequelae. These studies indicate the need to pay attention to the college students’ long-term cardiopulmonary function impairment after COVID-19, and to conduct objective evaluation of lung organs in the moderate to severe cluster during recovery, such as pulmonary function tests, cardiopulmonary exercise test, six-minute walk test (6MWT), respiratory muscle strength and endurance evaluation.
Our results suggest that precise interventions and management should be implemented for different COVID-19 sequelae phenotypes in college students. From the identified risk factors of different sequelae clusters, we can design specific management methods and rehabilitation measures for college student survivors according to their demographic characteristics and life habits. For college survivors with severe sequelae, multimodal care, including physiotherapy, rehabilitation, and psychotherapy, should be implemented following a comprehensive assessment. For the moderate cluster with predominantly physical impairments, cardiopulmonary function, and digestive symptoms, cardiopulmonary rehabilitation can be provided to help survivors improve cardiopulmonary function and digestive symptoms, and they are advised to improve their daily habits and reasonable exercise to promote recovery. The mild patients with predominantly psychological symptoms can receive psychotherapy and behavioral interventions, including measures to alleviate depression, anxiety, and insomnia disorders.
Advantages and Limitations
The advantages of our study include that we conducted a comprehensive assessment of physical, cardiorespiratory, digestive, neurological symptoms, and mental health outcomes in university students with COVID-19 following acute infection, and identified clusters of COVID-19 sequelae and investigated predictors of sequelae classification. However, the study has several limitations. First, we lack a control group with undiagnosed COVID-19 and a long-term follow-up survey to determine whether the sequelae symptoms are due to SARS-CoV-2 infection, it is difficult to compare symptom prevalence without an uninfected control group, and it is hard to estimate the relative risk of COVID-19 sequelae in young survivors due to the lack of validation from large cohort studies. Secondly, recall bias may occur when the questionnaire is conducted on study participants six months after the mass COVID-19 infection. Third, the patient-centered definition of recovery in this report is a subjective definition based on patient perception, which may be biased in reporting. Our study only used anxiety self-rating scales, and did not select other scales that may be used to assess mental health, such as depression self-rating scales or cognitive scales such as Montreal Cognitive Assessment (MoCA), and some pulmonary symptoms are also based on patient self-report and should be done more often such as CT. In this study, the physical symptoms, cardiopulmonary function, digestive symptoms, psychiatric symptoms, and psychological symptoms of some Chinese college students after COVID-19 were comprehensively evaluated through LCA, and three different rehabilitation phenotypes were identified. The three severity symptom clusters highlighted the possibility of classification of precision treatment for young people after COVID-19 recovery, extensively evaluated the survivors’ health status and promote post-COVID rehabilitation care.
Conclusion
We identified three clusters of post-COVID-19 sequelae based on the symptoms such as general physical dysfunction, cardiopulmonary, digestive, mental health, etc., and examined predictors associated with clusters. About three-fifths of Chinese college student survivors experienced varying degrees of sequelae symptoms three months after recovering from COVID-19 sequelae. Our results suggest that the long-COVID-19 symptoms of Chinese college students are related to their physical conditions before the outbreak of COVID-19. The prevention and intervention of college students’ sequelae should be carried out according to their physical conditions and living habits, which is conducive to more effective preventive measures, especially the rehabilitation of cardiopulmonary and digestive system function.
Supplemental Material
Supplemental Material - The Physical Condition and Mental Health of Chinese College Students 3 Months After COVID-19 Recovery
Supplemental Material for The Physical Condition and Mental Health of Chinese College Students 3 Months After COVID-19 Recovery by Yue-yang Wu, Na Wang, Qian Tang, Wen-bin Shen, Wei Xiao, Jian-wei Li, and Fen Huang in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Key Scientific Research Project in Higher Education Institutions in Anhui Province (2023AH050612).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.