
Abstract
The expression lifestyle describes a frame of expressed behaviors, usually in the form of patterns of consumption, that defines how an individual or social group fits into society. It presents as a focus of interest by researchers in this field, who classically favor the study of alcohol consumption, tobacco, eating habits, and physical activity. The aim of this study was to identify the relationship between physical activity and healthy lifestyles, especially in terms of eating habits, tobacco, alcohol consumption, resting habits, and resting heart rate (RHR) in Health Sciences first-year students. A total of 177 students of both genders participated, of whom 31 (17.5%) were male and 146 (82.5%) were female, with a mean age of 20.20 years, from 18 to 30 years. The data collection instrument used was the Healthy Lifestyle Questionnaire (EVS), using SPSS 21.0 for descriptive statistics and the Cronbach α to evaluate the internal consistency of the questionnaires. A level of significance was adopted with a margin of error of 5% for a probability of at least 95% using the Kolmogorov-Smirnov technique and Mann-Whitney test for comparisons between practitioners’ students and genders. The results obtained demonstrate more favorable results in all variables in students practicing physical activity with significant differences in eating habits and RHR. In terms of gender, there were significant differences in all variables except for eating habits. We conclude that students practicing physical activity present more favorable results in terms of lifestyles combined with lower RHR values, considered as positive factors in terms of quality of life.
‘ . . . we noticed that active individuals had better levels of cardiorespiratory and muscular fitness, better body composition and bone mineral density, and fewer symptoms of anxiety and depression.’
Introduction
The practice of physical activity is not only important, but also necessary for healthy growth and human development, regardless of the type of activity or the sport dimension chosen. It can also be considered an important element of culture, with relevance in educational programs, but also as an element of comparison, selection, and competitiveness, which may lead, in certain circumstances, to excess. 1 According to some authors, 2 the increase in sedentary behaviors, as well as the invasion of tasks that can make physical effort unfeasible, represent one of the greatest problems that characterize today’s societies, because there is a lot of evidence that highlights the impact active lifestyles have on health. However, the importance of physical activity practice in our society goes beyond the benefits related to the physical health of humans, insofar as it allows individuals to value their ego, because it is possible to perceive the development of socioaffective relations, communication, and socialization, making individuals adjust to the environment in which they live. 1
The expression lifestyle describes a set of expressed behaviors, usually in the form of patterns of consumption, that characterize the way an individual or social group fits into society. This was an expression that originated in research on noninfectious diseases, especially in developed countries. 3 Although with advances in science and the facilitation of human tasks there is a reduction in mortality from infectious diseases and an increase in longevity, the appearance of chronic degenerative diseases negatively affects the quality of life. The conception of lifestyle has been evolving, accompanying, in a certain way, the evolution of society, expressed in the change of the focus of interest by investigators in this field, where classically, they privileged the study of alcohol and tobacco, eating habits, and physical activity. 4
According to the relationships between physical activity, resting heart rate (RHR), and overall health, RHR is commonly assessed as an indicator of wellness and well-being. RHR is increasingly known to have valuable predictive utility in the assessment of a variety of cardiac diseases.5-7 In the literature, there is much evidence to show that regular participation in physical activity is an important factor for quality of life 8 as well as for health promotion, both social and mental, in the entire population. In fact, when we compared active with inactive individuals, we noticed that active individuals had better levels of cardiorespiratory and muscular fitness, better body composition and bone mineral density, and fewer symptoms of anxiety and depression. 9 Thus, it is essential to promote physical activity among the youngest, because in some studies, 10 it has been shown that young adults are not very active and it is proven that physical inactivity in this age group carries the risk of chronic diseases as well as reduces life expectancy because it is closely related to morbidity and mortality. The World Health Organization recommends that all individuals should perform physical activity for the benefits that come from it. 3
Although these benefits are well established, there are some factors associated with exercise practice that can affect individuals life quality, such as stress, which is characteristic of the sport environment and can have negative consequences on overall performance and well-being, as well as social, economic, and nutritional factors; inadequate rest and monotony of practice can lead to a fall in quality of life.11,12 Healthy lifestyles are not shaped by denial or avoiding certain permissive habits; they are best structured from a set of behaviors that create interest in the individual and that prevail over other less healthy behaviors. There are others concepts associated with lifestyle that help better understand how physical activity and exercise fit the current model of health, and it is important to understand certain specific terms and concepts such as health, physical activity, and physical fitness. There is convincing evidence that regular physical activity protects the body against sedentary habits. The literature has demonstrated that individuals who exercise regularly at a moderate intensity show gains both in terms of health and quality of life. 13 It should also be emphasized that healthy behaviors refer to the conscious effort of individuals to preserve their own health and what it offers. Healthy food is fundamental for good general health because energy and nutritional recommendations point to the importance of complying with a nutritional balance between energy intake and energy expenditure. 14 Also participating in regular physical activity can be very enjoyable and an important factor in improving the quality of life because the physical form maintained throughout life seems to be essential for the body to function in a healthy way. Thus, we can conclude that even small changes in lifestyle can have significantly positive long-term health effects if they are maintained. 15 The characterization of lifestyles is fundamental because inadequate habits can be reflected in health problems; hence, preventive and constructive education coming from both the family environment and the sports environment is important. Sport and physical activity are basic pillars of education and health promotion as well as healthy lifestyles. 16 In terms of healthy lifestyles, we can use synonyms such as healthy lifestyles and health-related lifestyle, encompassing both behaviors that enhance health (physical activity practice, nutrition, and resting habits) as well as those that are harmful such as tobacco and alcohol. 17 Considering that behavioral patterns acquired in the early stages of life are likely to be maintained during adulthood, 18 adolescents and young adults who hold an educational pattern integrating healthy lifestyles will tend to be adults with a lower probability of exposure to risk factors. Lifestyles are determined by 4 dimensions, which correspond to eating habits, subdivided into balanced diet, tobacco, and alcohol consumption; resting habits; respect for meal times; and adequate energy and nutritional values. 19
However, considering the evidence regarding the negative health effects associated with elevated RHR in adolescents and young adults,20,21 the RHR is a relevant health-related physical fitness component. It is important to verify the relationship between healthy lifestyle components and RHR because it is possible to identify modifiable factors in the adolescent and young adult population by means of low-cost, easily administered instruments and to propose strategies with the objective of preventing health problems associated with high RHR. 22 A higher RHR is directly associated with indicators of cardiovascular diseases, such as increased blood pressure levels, elevated blood glucose, higher total cholesterol concentrations, and elevated triglycerides.20-22
A study 13 that analyzed the RHR in young adults as a lifestyle predictor concluded that exercise was a significant aspect of their lifestyles, with 90% of participants reporting regular weekly exercise. Students who exercised (n = 407) had lower RHRs (72.3 ± 10.5 bpm) than students who reported no regular exercise (n = 46, 79.0 ± 11.0 bpm).
Most of the findings related to RHR come from investigations aimed to establish a relationship between RHR and risk factors for cardiovascular diseases, such as blood pressure and inflammatory markers. The literature has reported that adolescents and young adults with better performance in physical fitness tests have lower odds of high blood pressure, hypercholesterolemia, and cardiovascular dysfunction as well as lower RHR.23,24 Health-related issues lead to positive changes in RHR. In addition, excess body fat is associated with higher blood pressure, which increases RHR. 25
Materials and Methods
The methodology used in the execution of this research was selected from the determination of the objectives of the study, using the quantitative method, which is characterized by the use of quantification, both in the collection and in the treatment of information, where we will use statistical techniques, aiming at results that avoid possible distortions of analysis and interpretation as well as providing a higher safety margin. 26 Regarding the participants, we used a random sampling technique—that is, a procedure to be used in choosing the elements that make up the sample. 27 This type of sample can be used successfully in situations where it is more important to grasp general ideas to identify critical aspects than scientific objectivity itself.
Participants
The participants were 177 students enrolled in the first year of health sciences courses who volunteered to participate in this study. They were between 18 and 30 years old, with a mean age of 20.20 ± 3.04 years; 146 (87.5%) were female and 31 (17.5%) were male students.
Inclusion and Exclusion Criteria
Participants who were included in the study were in the first year of health sciences degrees, with ages between 18 and 30 years old. Participants who were in the second, third, or fourth years of bachelor’s degrees were excluded as well as those who were in the first year but younger than 18 years of age or older than 30 years.
Ethical Procedures
All students participated freely in the study, giving their consent by signing an informed consent form. Before starting to collect data, students were informed of the scope and objectives of our study as well as the confidentiality of individual data and the results of the tests performed. Data collection was carried out by the researcher himself for the application of the instrument and clarification of doubts. The students were approached in classrooms at the end of teaching, with the authorization of the teacher, as a way of inviting them to participate in this research. They were properly informed of the purpose of the study and that the collaboration was voluntary and anonymous. Students were asked their opinion about what was being questioned, and reminded that it would be important for them to be as sincere as possible. The questionnaires were self-filled in our presence and returned at the same time, making them reach us when they were completely filled, in an envelope, guaranteeing total anonymity. After the questionnaires were processed, they were destroyed. The study was approved by the Ethics Commission of the University Fernando Pessoa (Oporto, Portugal).
Statistical Procedures
All variables of the questionnaire in this study were treated statistically using the SPSS for Windows (version 21.0). This statistical treatment consists of a descriptive analysis, and the Cronbach α was calculated to evaluate the internal consistency of the questionnaires. A level of significance was adopted with a margin of error of 5% for a probability of at least 95% using the Kolmogorov-Smirnov technique and Mann-Whitney test for comparisons between practitioners and nonpractitioners’ students as well as genders regarding their eating habits, tobacco and alcohol consumption, resting habits, and RHR.
Instruments and Data Collection
To collect data in accordance with what we intended to evaluate, we used the Healthy Lifestyles Questionnaires (EVS) 28 to characterize the habits and lifestyles of the students, translated and validated for the Portuguese language. 29 The original questionnaire consists of 30 items; however, after the necessary adaptations, only 20 items were used, with questions that refer to different factors, such as balanced diet, respect for meal times, tobacco consumption, and resting habits. In terms of reliability, the indices of internal consistency were considered acceptable. For heart rate measurement, a digital cardiofrequencimeter (Polar Flow) was used according to the following protocol: the students were asked to lie down on their back, relaxed, in a private classroom, after a 30 minute period of rest. Then, they put on the soft strap with the heart rate sensor; after about 1 minute, they breathed calmly and were asked not to look at the monitor. The investigator registered the value of the lowest heart rate. RHR varies from person to person, but according to the Seattle Criteria 30 the average RHR ranges from 60 to 90 beats per minute (bpm). In the case of a heart rate <50 bpm, the participant repeated the ECG after mild aerobic activity.
Results
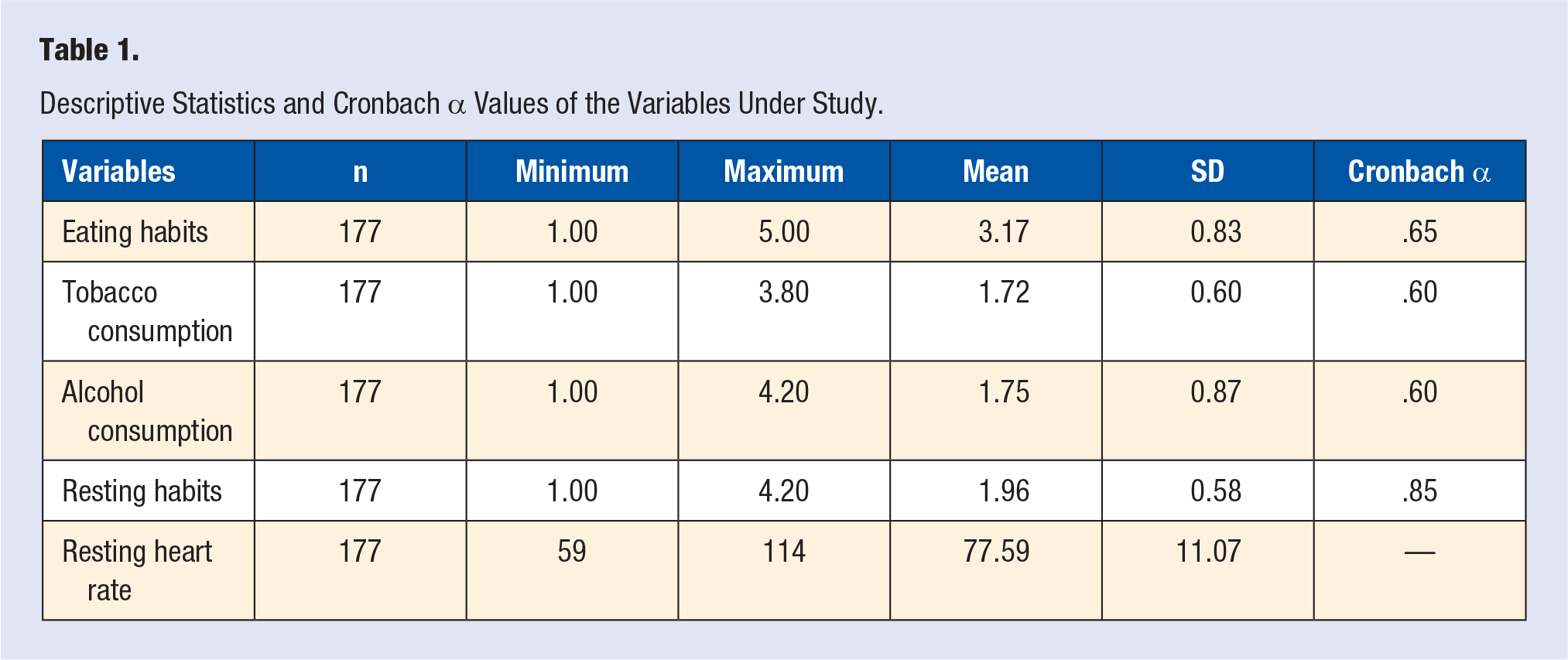
In this section, we present descriptive statistics with measures of central tendency and specific tests (Table 1).
Descriptive Statistics and Cronbach α Values of the Variables Under Study.
We started the description of our sample with reference to the descriptive values of each variable, and considered the practice of habits of healthy lifestyles according to the gender of the students. It can be seen from Table 2 that the male students present higher values (X = 3.19 ± [σ = ]0.65) for resting habits (X = 2.17 ± [σ = ]0.85) and RHR (X = 72.7) in relation to the female students, who in turn present higher values (X = 1.67 ± 0.60) for alcohol consumption (X = 1.68 ± [σ = ]0.60). There are significant differences in all variables except for eating habits.
Mean Values and SDs of the Variables Analyzed in All Students According to Gender.
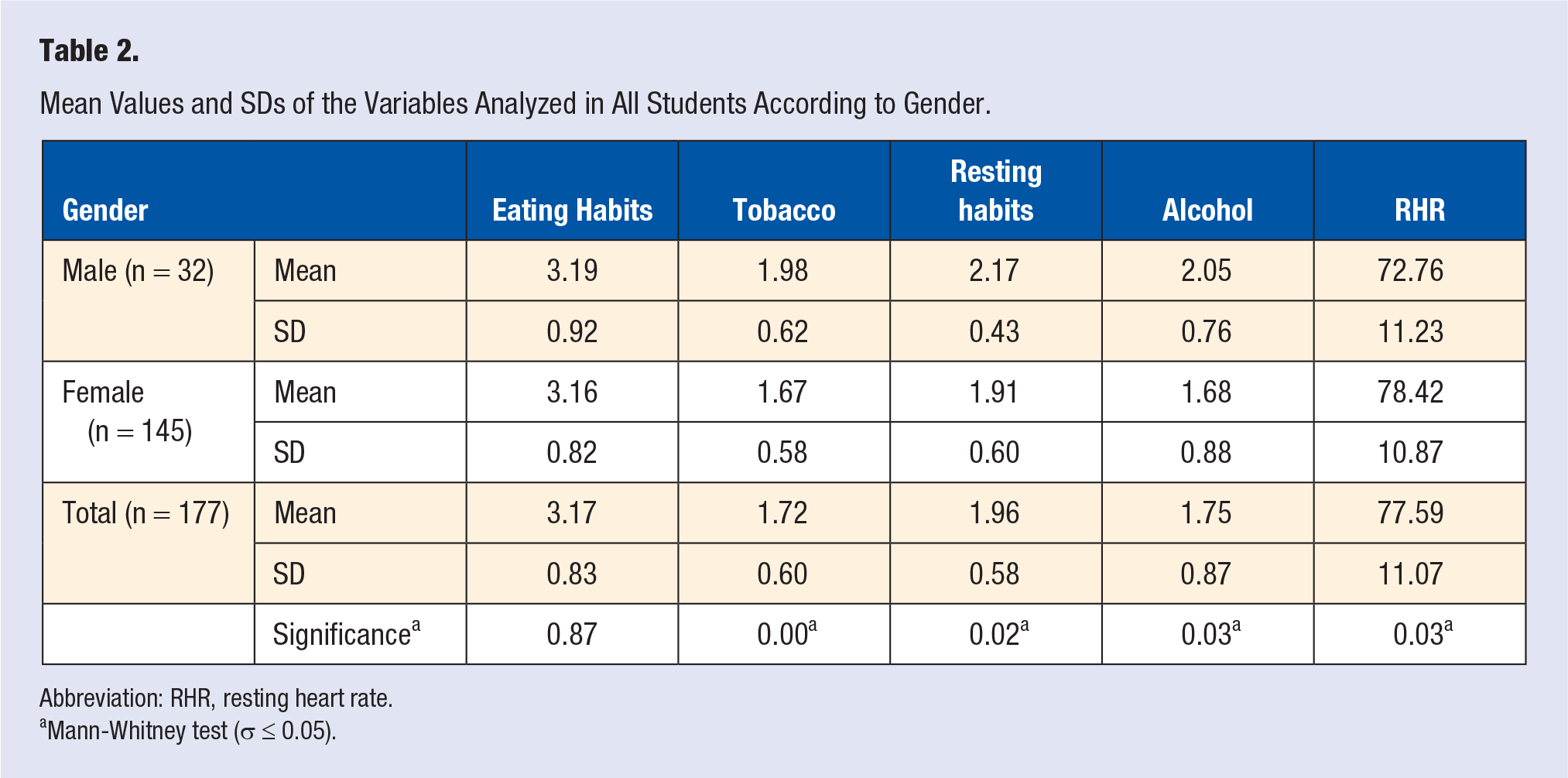
Abbreviation: RHR, resting heart rate.
Mann-Whitney test (σ ≤ 0.05).
According to Table 3, all variables are more favorable in the group of students practicing physical activity. There is more concern about eating habits (mean = 3.33), with significant differences between groups; lower tobacco consumption (mean = 1.70), more resting periods (mean = 2.00), lower consumption of alcohol (mean = 1.67), and lower RHRs were also seen, with significant differences between exercise practitioners and nonpractitioners.
Means, SDs, and Significance Values of Healthy Lifestyle Variables for Students With and Without Physical Activity.
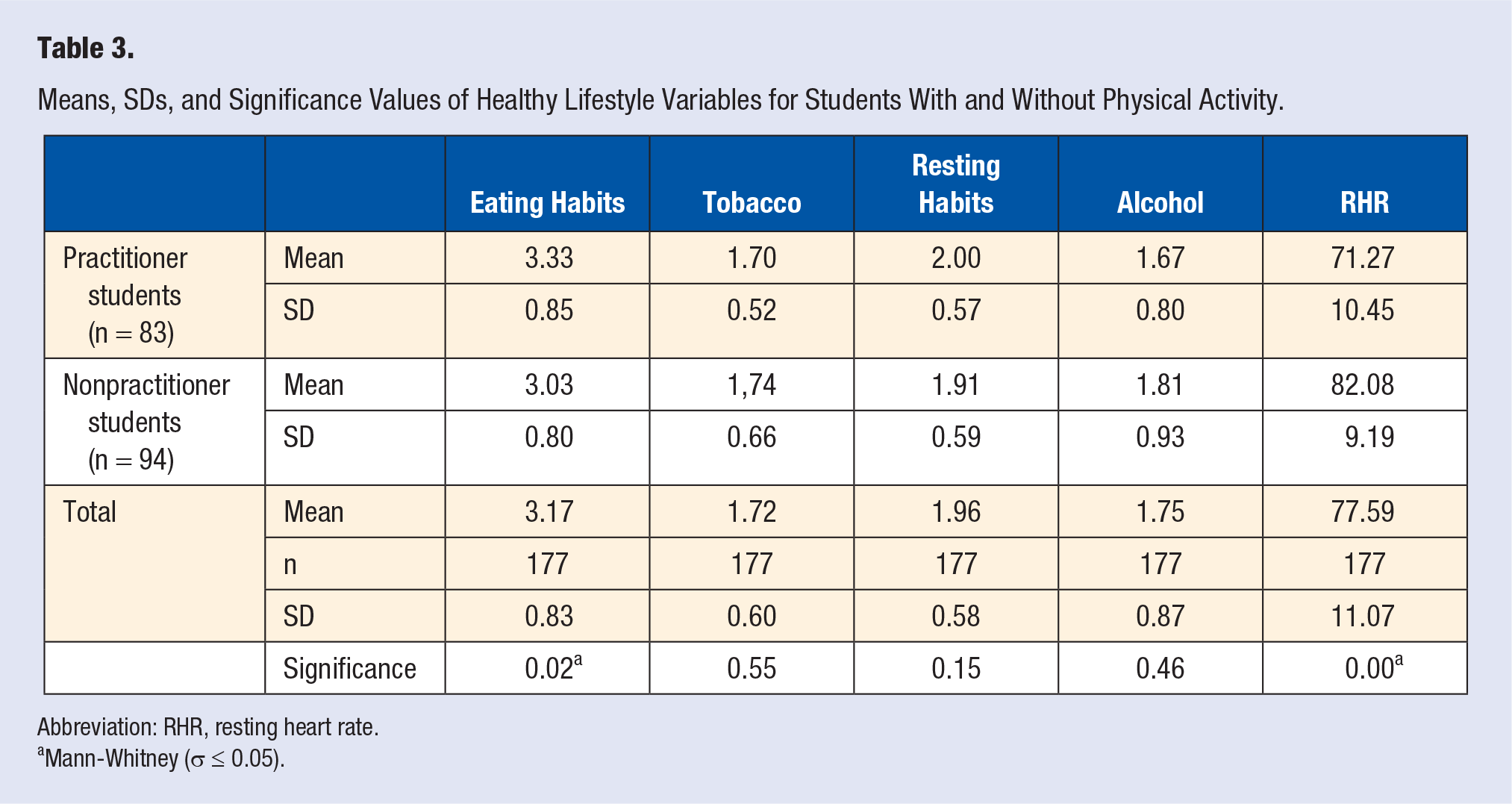
Abbreviation: RHR, resting heart rate.
Mann-Whitney (σ ≤ 0.05).
Table 4 shows that in the comparison between the male group, the students with physical activity have more favorable values in all variables (except in rest habits with an equal value), with significant differences in alcohol consumption (P = .006) and RHR (P = .007). The same aspect is also observable in the comparison between the female group, with significant differences in eating habits (P = .05) and RHR (P = .00) as well. It means that the students with physical activity have more healthy lifestyles and also a lower RHR, considered adequate according to the Seattle criteria. Between male and female students with physical activity, the only significant differences are in tobacco consumption, with a higher incidence among male students. In eating habits, both genders have similar values, with higher values for resting habits in male students, as well as lower RHRs; but they consumes more alcohol than female students. These results agree with those of Table 3, showing that physically active students take greater care, have more favorable lifestyles, and have RHR values that are considered favorable predictors for lower probability of having cardiovascular diseases. In these young adults, the students who exercised had lower RHR; according to some studies,31,32 exercise and lower RHRs are useful indicators of overall cardiovascular health.
Mean Values and SDs of the Variables Analyzed for Male and Female Students.
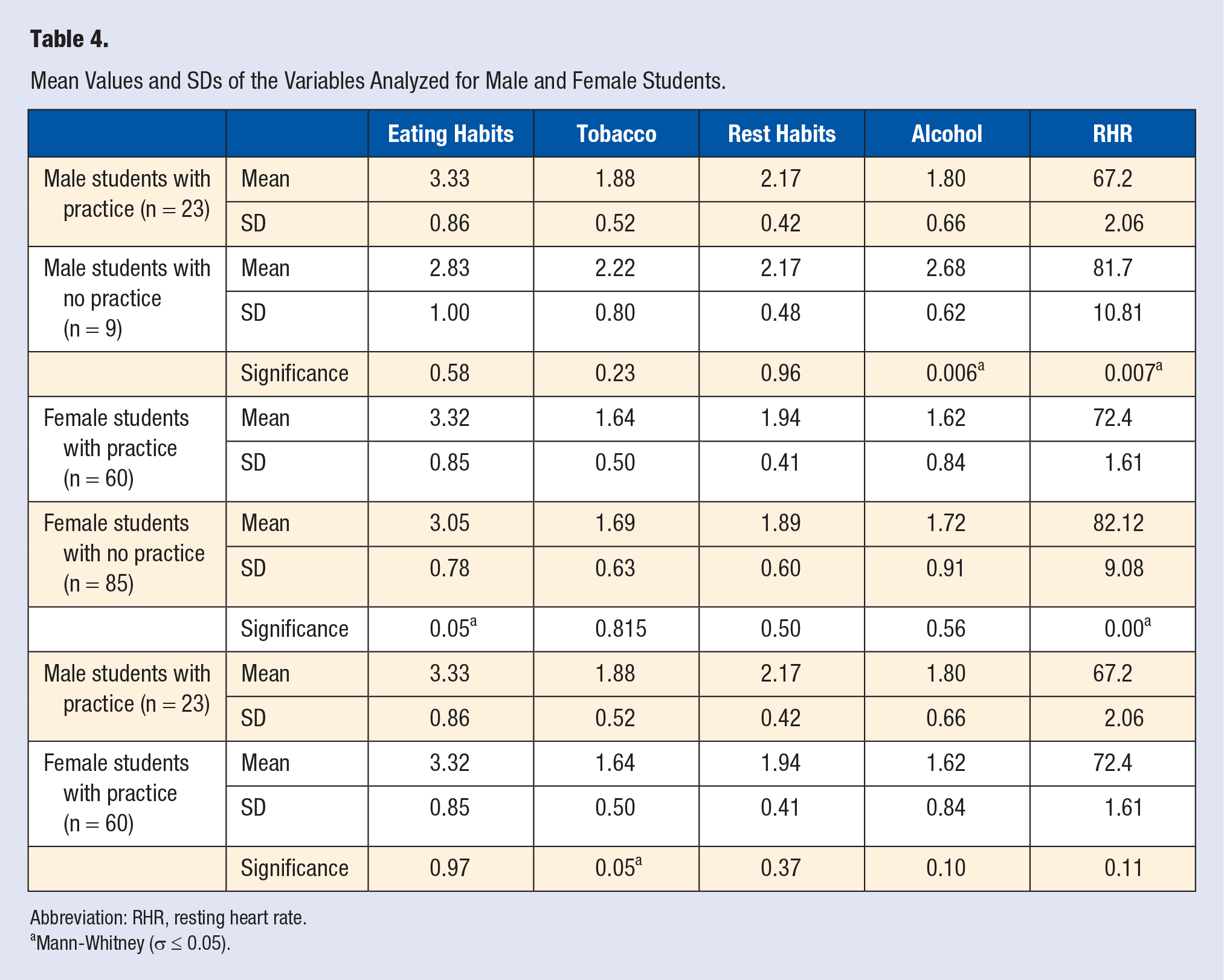
Abbreviation: RHR, resting heart rate.
Mann-Whitney (σ ≤ 0.05).
Discussion
The results of this research are presented through the comparison between practitioners and nonpractitioners of physical activity and students’ gender in relation to lifestyles. According to gender comparison, the male students had more favorable values for eating habits, resting habits, and RHR than female students. However, male students had higher values of alcohol and tobacco consumption with significant differences. In the comparison between physical activity practicing and nonpracticing students, those who practice physical activity present the best lifestyles with differences in eating habits and RHR. This result seems to suggest that male students give more importance to energy and nutritional consumption because it is essential for the maintenance of performance, body composition, and health. They use dietary restriction as a means of adjusting body weight and optimizing sports performance.19,33 Thus, we can say that the results obtained in this study do not resemble other results, 34 where women are seen to have a more balanced diet, consuming fruits and vegetables more often than men. However, men also consumed more tobacco, a situation that also occurs in this study.
According to another study, 35 it is the men who presented the most favorable values because this is directly related to eating habits; men also had more regular resting habits. In another study, 36 women had a lower mean of resting habits than men, not only because of hormonal factors, but also because of dating relationships and domestic and financial responsibilities. 37 Other studies38,39 report that the most frequent problems of insomnia are in fact related to poor sleep hygiene. Heavy stimulants may hinder the onset of sleep: B vitamins and calcium favor sleep, whereas alcohol, caffeine, and nicotine harm it. 40 Having said this, we can conclude that a good lifestyle also has advantages for the quality of sleep.
Considering other analyses, 41 we think that life habits tend to appear united or grouped, both in the case of habits related to healthy lifestyles and in the case of those that are considered risky. The authors found that in the comparison between practitioners and nonpractitioners of physical activity, the latter exhibited other health risk behaviors: physical inactivity, inadequate diet, consumption of other drugs, and so on. 42 It was verified that, according to this study, the individuals who practiced physical activity had better lifestyle indices related to a lower RHR.
Finally, and taking another approach, 43 where the same healthy lifestyles were studied between competitors and noncompetitors in surfing, the same trends were observed—that is, those practicing the sport present had better indices in all the studied variables. This study also studied the association of RHR. Several authors44,45 point out that the increase in stroke volume leads to a decrease in the number of beats required to maintain cardiac output, decreasing the metabolic load of the heart and contributing to lower RHR.44,45 Healthy lifestyles, such as those mentioned, are linked to physical activity and related to lower RHR, considered as an important factor for quality of life and lowering the chances of developing cardiovascular diseases. An explanation is that moderate to higher levels of physical activity decrease parasympathetic nervous system activity, which reduces the RHR. 46 Other authors found that improvement of cardiorespiratory fitness in adolescents and young adults leads to better cardiovascular health indicators, such as healthy blood pressure levels, favorable lipid profile, and lower risk of morbidity and mortality, in adult life.47,48 In this way, promoting the improvement of such healthy lifestyles will contribute to a healthier context throughout life.
Conclusions
Our study goals were to identify the differences between male and female students, and practitioners and nonpractitioners of physical activity, especially at the level of their lifestyles. Students practicing physical activity showed more favorable values in all variables, with significant differences in eating habits and RHR. In terms of gender comparison, men were more careful about diet and hours of resting, with lower values of RHR, although without significant differences; they had higher values only for tobacco and alcohol consumption. Although the literature shows that there are differences related to gender, among the variables we studied, it is curious to observe that men higher values, except for tobacco and alcohol consumption. However, there is no doubt that in the comparison between practitioners and nonpractitioners of physical activity, and between genders, there are better indices of lifestyles in the student practitioners, so the variable of physical activity is a determinant for a healthy life.
This study also demonstrated that RHR has a positive association with physical activity and the lifestyle variables under study. RHR values are a viable alternative for use in large health monitoring systems because they are easier to determine. It is important to practice these healthy lifestyles in early adulthood, especially in an educational context, so that these practices can be maintained through life and, as future health professionals, such behaviors can be taught to their students.
It is valid to state that low cardiovascular disease risk profile (no prior myocardial infarction and, simultaneously, no presence of untreated cholesterol and untreated blood pressure, no smoking, and no diabetes mellitus) in young adults has been demonstrated to be associated with lower mortality and morbidity rates, higher life expectancy, lower lifetime risk for cardiovascular disease, and furthermore, higher quality of life in older age. The practice of healthy lifestyle factors such as no smoking, vigorous or moderate physical activity, no excessive alcohol drinking, and a balanced diet during young adulthood are strongly associated with achievement of the low-risk profile in middle age. Our study indicates that the healthy lifestyle factors practiced are positively linked to a lower RHR. These data suggest that these students, and future professionals, should encourage their patients/students to adopt a healthy lifestyle starting at a young age or to improve their lifestyle as early as possible to maximize the benefits of the low cardiovascular risk profile in terms of healthy longevity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics Commission of the University Fernando Pessoa (Oporto, Portugal) approved the study.
Informed Consent
All participants provided informed written consent.
Trial Registration
Not applicable, because this article does not contain any clinical trials.