
Abstract
“Medicare and uninsured patients were more likely to report good SDC compared to patients with private insurance.”
Background
Education and guidance provided by hospital staff to patients at discharge can guide stroke patients to properly manage their health through important lifestyle and behavioral modifications and reduce the occurrence of adverse post-stroke health outcomes and subsequent readmissions.1-3 Discharge education is a short educational intervention provided before the patient’s discharge from the hospital. 1 Discharge education/communication aims to guide and facilitate post-hospital transitions and reduce early (<=30-day) readmissions. Discharge education can improve patient knowledge4-6 and promote healthy lifestyle and behavioral changes.1,4,6 Recommended behavioral changes, such as diet modification,7-9 weekly exercise,10-12 medication adherence,13-15 substance use cessation,16,17 use of prescribed therapy,18-20 and attendance of a medical follow-up visit21,22 can help to reduce readmission rates. The patient’s perception of the information provided during discharge education can have a further positive impact on the patient’s perceived readiness for discharge (i.e., readiness for the transition from hospital to home)23-25 and post-discharge coping,24,25 and can reduce readmissions.23,25
At pre-discharge, hospital staff such as nurses, physicians, social workers, and other care coordinators are required to provide discharge education consisting of all or a combination of the following information and resources to the patient: reasons for admission, current disease state, identification or risk factors, instructions for self-care, health maintenance for home/post-discharge location, prescribed medications, and follow-up appointment scheduling. 26 The discharge process can be overwhelming for patients and resource-intensive for healthcare providers.26-28 While most hospitals report consistent delivery of discharge education through disseminated written materials,29,30 there is a lack of standardized mechanisms for assessing the depth and quality of education received and how well the patient understood or received the education materials. 29 Additionally, retention of discharge education material can be challenging for stroke patients, 29 possibly due to the overwhelming psychological impact of a stroke on both patients and their family members. 29
Many studies examine the effect of discharge education on various health outcomes, yet studies specifically concerning education for patients after stroke are needed. Further, identifying potential racial/ethnic disparities in the receipt of patient-reported discharge education and its effects on post-discharge healthy lifestyle and behavioral changes remains unexplored. This study aims to determine the association of sufficient discharge communication with lifestyle and behavioral modifications within 30 days post-stroke and secondarily evaluate racial/ethnic differences in the relationship between SDC and ATOC.
Methods
The Transitions of Care Stroke Disparities Study (TCSD-S) is a multi-center observational study investigating drivers and disparities surrounding a successful transition from hospital to home among stroke survivors. Our sample consisted of individuals post-stroke from a subset of 10 comprehensive stroke centers (see supplemental table 1) within the Florida Stroke Registry (a registry of stroke survivors from 180 hospitals within the state of Florida). Eligible participants are ages 18 years of age and above, with a diagnosis of acute ischemic or intracerebral hemorrhage stroke and discharged from the hospital to either a rehabilitation facility or directly home. Hospital care coordinators interview eligible participants at discharge with questions regarding social determinants of health, including difficulty paying for necessities and social support network size. At 30 days and 90 days after discharge, coordinators follow up via structured telephone interviews either directly with the patient or the patient’s caretakers to acquire information regarding any readmissions or emergency room visits that occur within the 30-day and 90-day span after discharge. Specifically at 30 days, coordinators also record responses regarding receipt and evaluation of specific eligible discharge education and the patient’s participation in healthy lifestyles and behavioral modifications such as diet improvement and/or physical activities.
Data from TCSD-S was linked to the American Heart Association Get with the Guidelines-Stroke Database to include details on patient race-ethnicity, sex, age, insurance status, stroke severity, discharge location, and pre-stroke health conditions. Discharge and follow-up data included the TCSD-S questionnaires completed at hospital discharge and at 30 days and/or 90 days after discharge. The dataset used for analysis included participants who met TCSD-S inclusion criteria and self-identified as Hispanic, non-Hispanic Black, or non-Hispanic White. Further, participants who did not complete 30- and/or 90-day follow-ups were excluded from the study. The thirteen patients that died within 30 days post-discharge were excluded due to the lack of availability of 30-day TCSD-S data. Patients with a post-discharge disposition to hospice care, acute care facilities, skilled nursing facilities, intermediate care facilities or leaving against medical advice (n = 70) were also excluded from the dataset used for analysis. Figure 1 displays the cohort diagram for this analysis. The flow diagram for the transitions of care stroke disparities study (TCSD-S) cohort.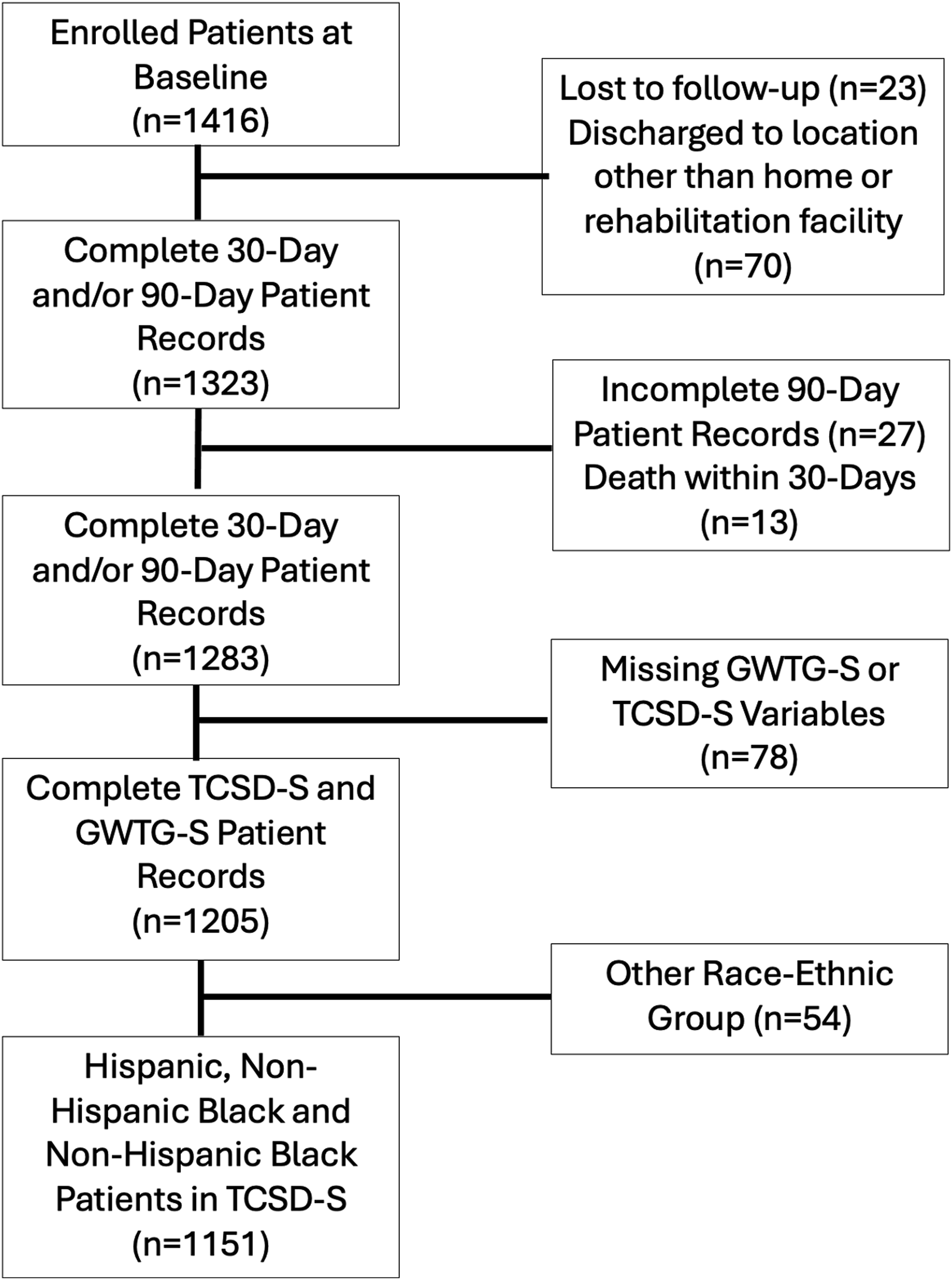
Sufficient Discharge Communication
Our main exposure of interest is patient perception of sufficient discharge communication (SDC), referenced as sufficient discharge education and guidance in prior work. 31 SDC is a composite score that evaluates a patient’s perception of the quality and adequacy of resources provided at discharge. This score comprises of patient-reported answers to three 30-day questions in the TCSD-S questionnaire (Supplemental Table 2). Using these three questions, the SDC score incorporates 3 components: (1) perception of whether the patient received sufficient dietary improvement education; (2) perception of whether the patient received sufficient substance use cessation education (if the patient has a reported history of excessive alcohol, tobacco, or illicit drug use); and (3) whether the patient was scheduled for a follow-up medical appointment at discharge. A patient has sufficient discharge communication if they have reported receiving all applicable forms of education and guidance for which they are eligible at discharge. That is: (1) diet education and medical follow-up scheduling for patients without a reported history of excessive alcohol, tobacco, or illicit drug use; or (2) diet education, substance use cessation education, and a medical follow-up scheduling for patients with the reported history of substance use. SDC is a binary variable, with 1 indicating receipt of a sufficient discharge communication and 0 indicating no receipt.
Adequate Transitions of Care
Our main outcome of interest is adequate transitions of care (ATOC). 32 As described in other TCSD-S publications, ATOC is a composite score that calculates a patient’s level of participation in healthy behaviors and activities within 30 days post-discharge. A participant would accomplish ATOC by having reported completion of at least 75% of applicable behaviors and activities. During the 30-day structured telephone interview, coordinators ask each participant about engagement in the following 6 behaviors and activities since their stroke discharge: (1) diet modification, (2) medical follow-up appointment visit, (3) medication adherence, (4) weekly exercise, (5) utilization or completion of prescribed therapy, and (6) toxic habit cessation (Supplemental Table 3). In the composite ATOC score, each applicable behavior and activity category is a binary question for each eligible participant, with 1 indicating accomplishment and 0 indicating no accomplishment.
When interviewed by coordinators, participants report whether they modified their diet following their stroke. An affirmative answer indicates that the participant was able to make dietary changes. Participants accomplished the medical follow-up appointment visit if they reported being seen in a clinic or doctor’s office since their hospital discharge. Medication adherence was accomplished if the participant reported taking their medications as prescribed since they left the hospital at least 75% of the time. Participants accomplished exercise as an activity if they answered affirmatively to weekly walking, treadmill use, or aerobic, stretching, or strengthening exercises outside of prescribed therapy. Prescribed therapy use, only applicable to participants prescribed therapy at discharge, is an accomplishment when the participant reports attending or completing therapy sessions within the 30-day post-discharge period. Toxic habit cessation is an accomplishment that is only applicable to participants with a self-reported history of using tobacco, marijuana, excessive alcohol, or illicit drugs within 1 year prior to stroke. Participants accomplished cessation if they reported reducing substance use by more than 50% of what was used before the stroke.
Statistical Analysis
Descriptive statistics [mean (SD), median (IQR), frequencies (percentages)] are used to summarize the participant characteristics of this dataset. SDC is the primary exposure, and accomplishment of ATOC is the outcome of interest. In a series of 4 models, the association between SDC and ATOC was examined and stratified by race-ethnicity. The 4 models reflect a sequential adjustment of categorized covariates in the following order: (1) demographic variables of race-ethnicity [non-Hispanic Black, Hispanic, non-Hispanic White (reference)], sex [male and female (reference)], age at discharge (in years), stroke severity (National Institutes of Health Stroke Severity Scale), and insurance status [private insurance (reference), Medicare, Medicaid, or Self-insured/uninsured]; (2) social determinants of health (difficulty paying for necessities, education level, and support size); (3) binary stroke risk factor variables prior to stroke hospitalization (prior stroke, pre-stroke smoking, pre-stroke heart failure diagnosis, pre-stroke coronary artery disease, pre-stroke diabetes, pre-stroke hypertension, and pre-stroke chronic renal insufficiency); and (4) acute care variables, or variables that may be indicative to the patient’s discharge experience beyond the discharge communication [modified Rankin scale at discharge, stroke type [acute ischemic stroke (reference), intracerebral hemorrhage], and discharge location [home (reference), rehabilitation facility]. Odds ratios (OR) with Wald confidence intervals calculate the likelihood of accomplishing ATOC. For all models, the significance threshold was set at alpha = .05.
To further assess which ATOC components contribute to the overall association, post-hoc logistic regression analyses examine the association between SDC and the 6 behaviors and activities comprising ATOC separately, controlling for demographic variables, social determinants of health, stroke risk factors, and acute care variables. All analyses were conducted using SAS version 9.4.
Results
Characteristics of TCSD-S Analytical Sample by Sufficient Discharge Communication.
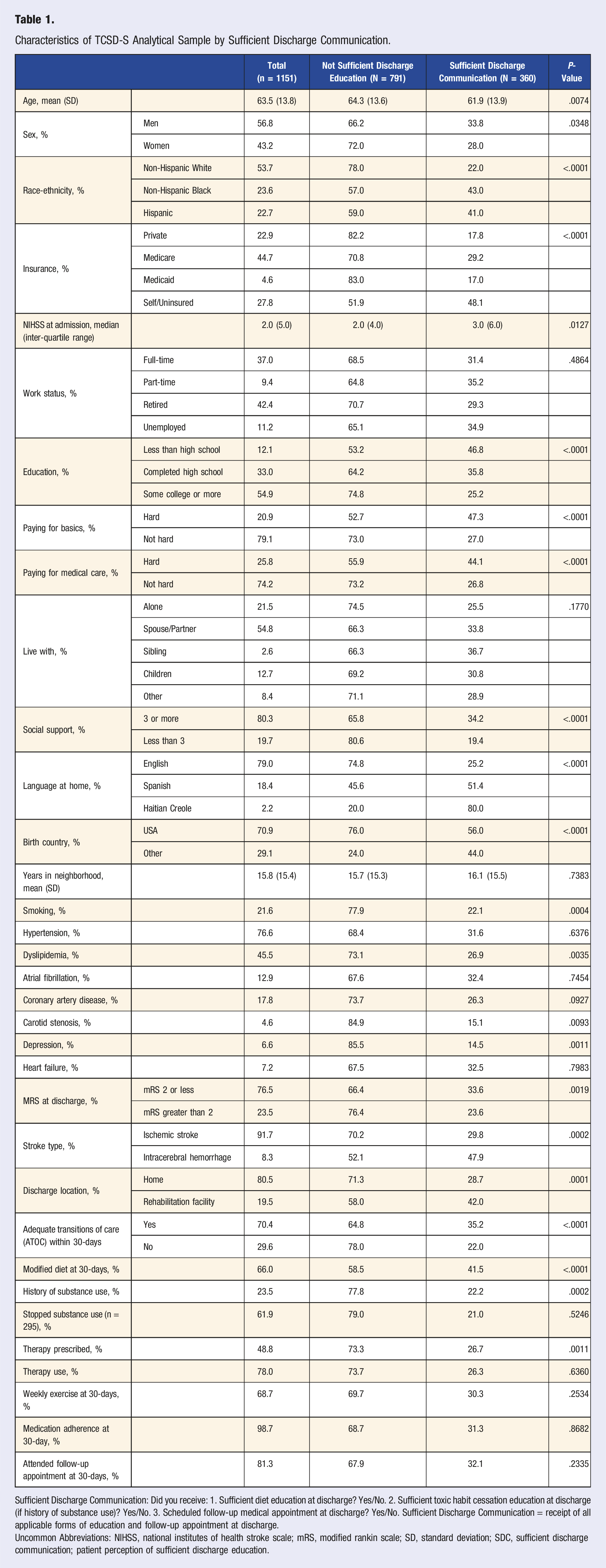
Sufficient Discharge Communication: Did you receive: 1. Sufficient diet education at discharge? Yes/No. 2. Sufficient toxic habit cessation education at discharge (if history of substance use)? Yes/No. 3. Scheduled follow-up medical appointment at discharge? Yes/No. Sufficient Discharge Communication = receipt of all applicable forms of education and follow-up appointment at discharge.
Uncommon Abbreviations: NIHSS, national institutes of health stroke scale; mRS, modified rankin scale; SD, standard deviation; SDC, sufficient discharge communication; patient perception of sufficient discharge education.
The Association Between Reporting Sufficient Discharge Communication and Achievement of Adequate Transitions of Care Within 30-Days Post-Discharge in the Transitions of Care Stroke Disparities Study (TCSD-S) 2018-23.
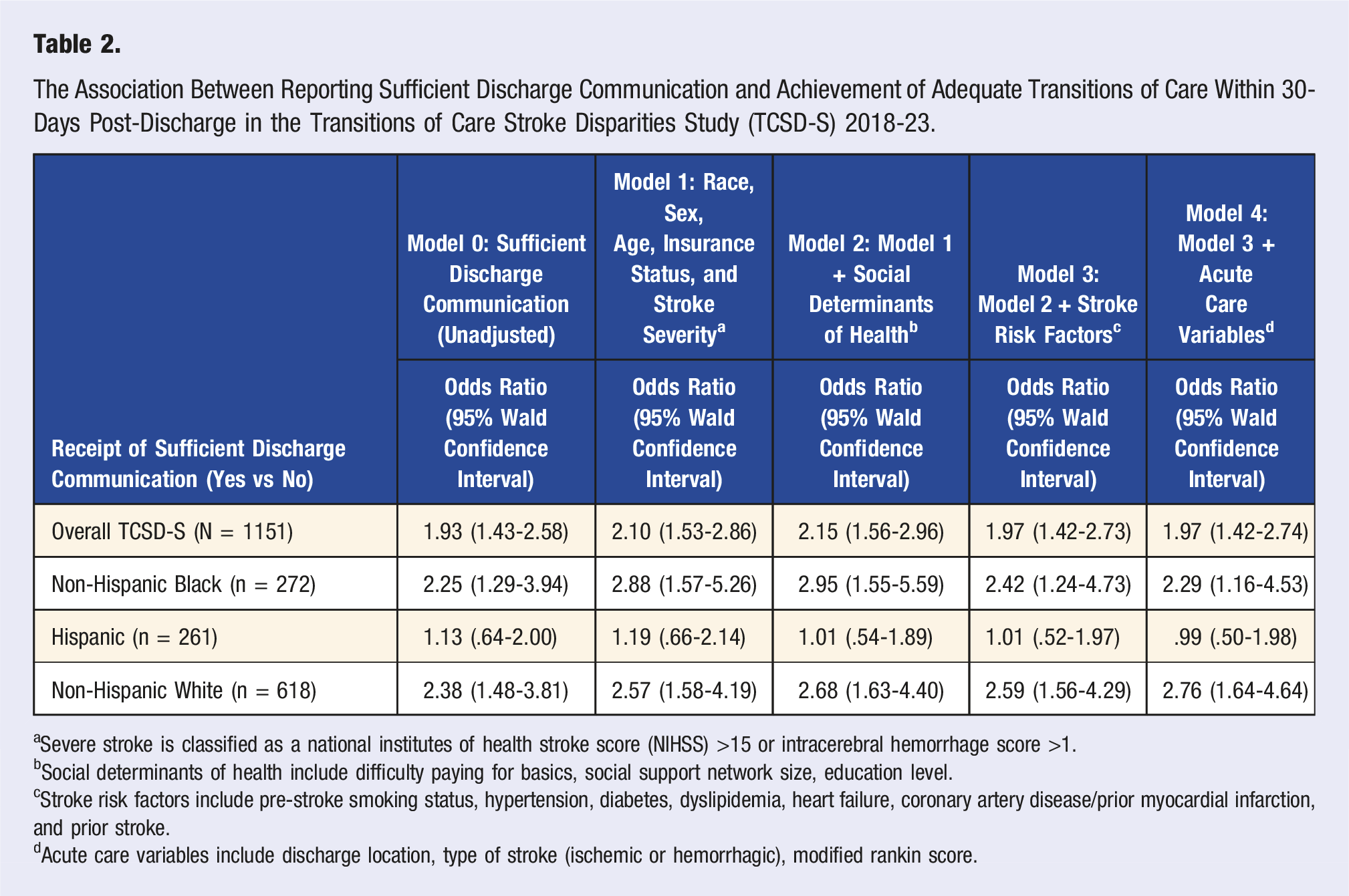
aSevere stroke is classified as a national institutes of health stroke score (NIHSS) >15 or intracerebral hemorrhage score >1.
bSocial determinants of health include difficulty paying for basics, social support network size, education level.
cStroke risk factors include pre-stroke smoking status, hypertension, diabetes, dyslipidemia, heart failure, coronary artery disease/prior myocardial infarction, and prior stroke.
dAcute care variables include discharge location, type of stroke (ischemic or hemorrhagic), modified rankin score.
Association Between Sufficient Discharge Communication and Each ATOC Component in the Transitions of Care Stroke Disparities Study (TCSD-S) 2018-2023.
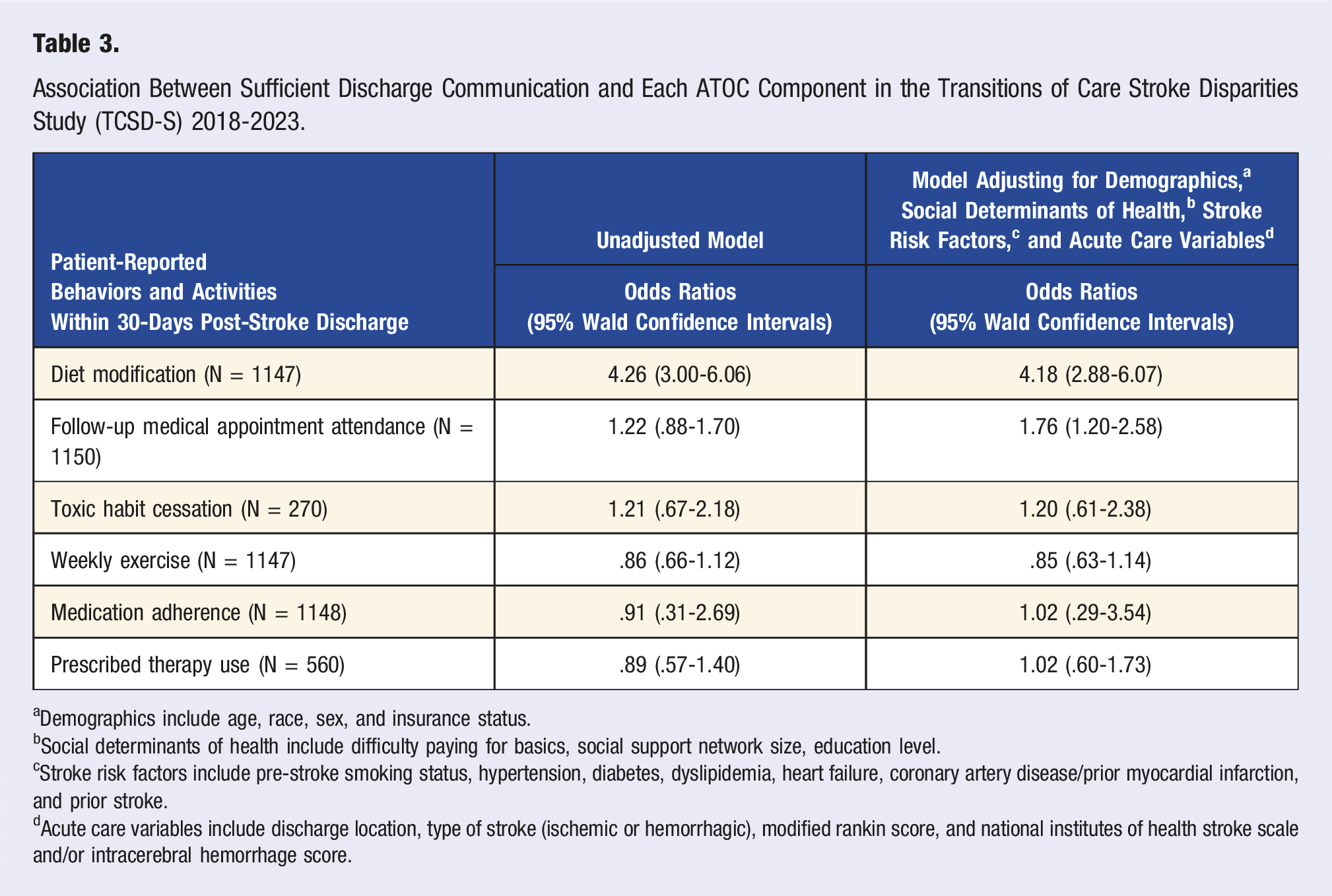
aDemographics include age, race, sex, and insurance status.
bSocial determinants of health include difficulty paying for basics, social support network size, education level.
cStroke risk factors include pre-stroke smoking status, hypertension, diabetes, dyslipidemia, heart failure, coronary artery disease/prior myocardial infarction, and prior stroke.
dAcute care variables include discharge location, type of stroke (ischemic or hemorrhagic), modified rankin score, and national institutes of health stroke scale and/or intracerebral hemorrhage score.
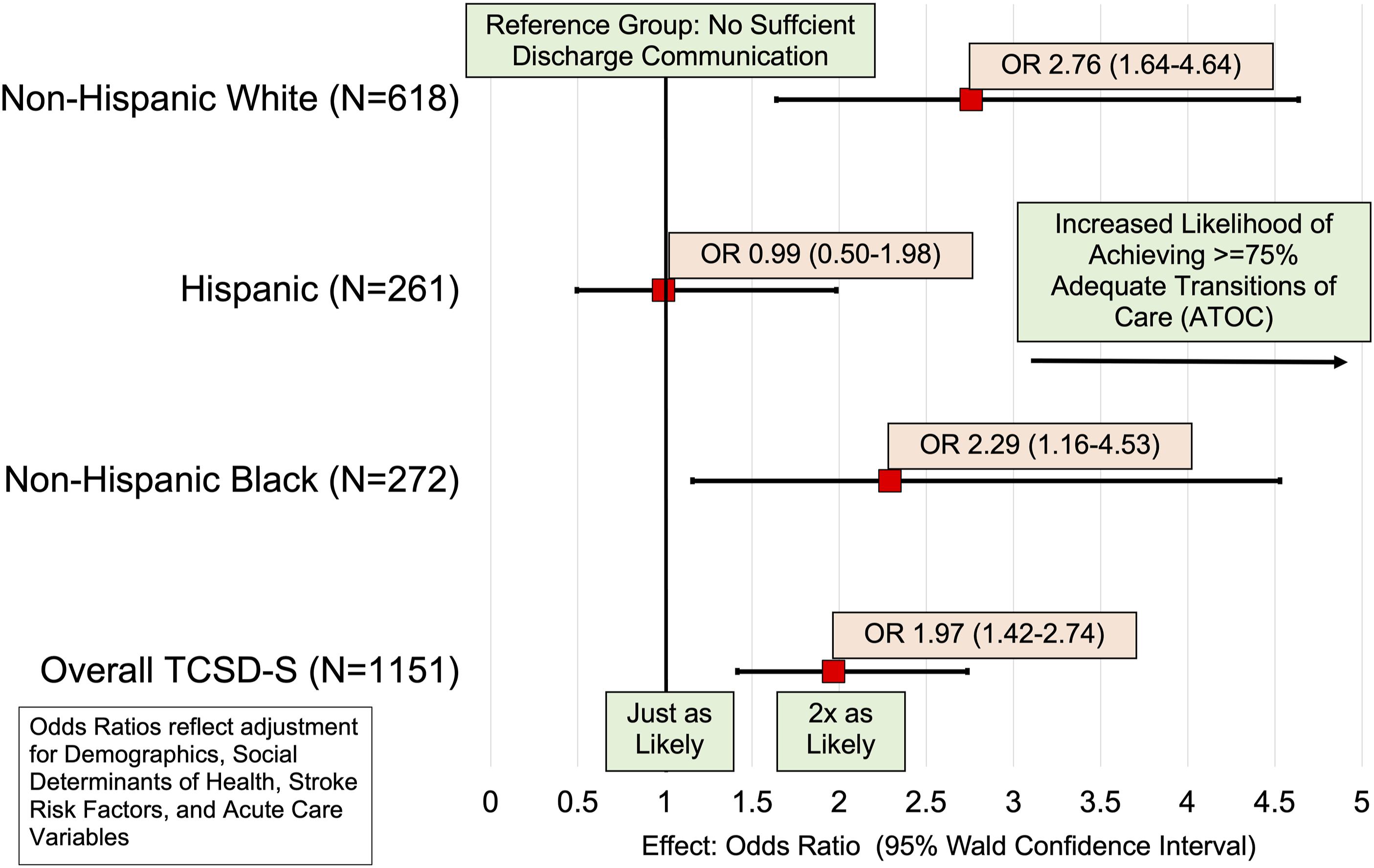
A forest plot showing the association between sufficient discharge communication (SDC) (i.e., patient receipt of sufficient diet education, sufficient toxic habit cessation education, if applicable, and scheduled medical follow-up appointment) and ATOC within 30 days post-discharge overall and by race/ethnicity [non-Hispanic white (NHW), non-Hispanic black (NHB), and Hispanic] in the transitions of care stroke disparities study (TCSD-S) (2018-2023).
Overall, diet modification (Adjusted OR 4.18 95% CI 2.88-6.07) and follow-up medical appointment attendance (Adjusted OR 1.76 95% CI 1.20-2.58) were significantly predicted by SDC, driving the association with the overall ATOC achievement. Supplemental Table 4 shows the relationship between SDC and each ATOC component separately.
Discussion
In this observational study of stroke survivors, patient perception of the information and resources provided by health care providers at discharge associates with the likelihood of engaging in healthy behaviors and activities within 30 days post-stroke discharge. An alarming finding from our study is that less than half of patients in our sample perceived having sufficient discharge education. The relatively low prevalence could reflect low overall satisfaction with their discharge care among our cohort. While the reasons are not entirely clear, satisfaction could also correlate with retention of knowledge. A 2018 series of pilot studies found that only 25% of stroke patients were able to fully retain information from in-depth verbal and written discharge education materials after 3 months post-stroke discharge. 29 Still, the STROKE Perception Report findings have shown that stroke patients and family members view discharge education as a valuable tool for helping them prepare for discharge.33,34 Future studies can investigate the patient perspectives on how discharge education and resources can be improved for the retention of vital knowledge and for better participation in post-stroke lifestyle and behavioral modifications.
Medicare and uninsured patients were more likely to report good SDC compared to patients with private insurance. A 2022 study found that uninsured Medical Expenditure Panel Survey participants were less likely to rate the healthcare from their providers with a high satisfaction rating when compared to privately insured participants. 35 This same study also found that Medicare-only and Medicare/privately insured patients were more likely to rate their healthcare with higher satisfaction than privately insured patients below the Medicare eligibility age of 65. The lower likelihood of private insurance recipients reporting sufficient discharge communication aligns with a recent study finding that Medicare recipients are more likely to report better access, greater satisfaction, and lower healthcare costs than privately insured patients. 36
Because race-ethnic differences in post-stroke health outcomes such as disability, death, or readmission are prevalent,37-40 our stratified analysis aimed to identify any race-ethnic disparities in the receipt and perception of discharge communication and the impacts of discharge communication on health behavior modifications. Currently, there is a lack of research that analyzes the patient perception of both discharge education quality and post-stroke health management among underrepresented race-ethnic groups. 41 A previous intervention implementing culturally tailored pre-discharge education sessions comprised of an interactive motivational video, PowerPoint presentation, and workbook for stroke patients found no significant effect of systolic blood pressure reduction after 12-days post-stroke when compared to usual care. 6 Our study, which does not highlight or describe a specific hospital-level intervention, found a significant benefit of reported/perceived SDC in accomplishing ATOC amongst both Non-Hispanic Black and Non-Hispanic White participants.
Despite Hispanic patients having the greatest prevalence of accomplishing ATOC than their non-Hispanic White counterparts, the benefit of SDC in ATOC accomplishment was not apparent among Hispanic participants. This finding justifies adjusting for social support as a relevant covariate in my analyses. It also reflects the fact that social support was a huge contributor to Hispanic patients’ likelihood of accomplishing post-stroke lifestyle and behavioral modifications. Social support is a protective factor against cardiovascular disease outcomes among middle-aged adults and can play a critical role in healthy decision-making for patients with vascular issues.42,43
Although prior studies have found minority patients with a higher likelihood of reporting discrimination and medical mistrust in the hospital setting,44-49 non-Hispanic Blacks and Hispanics reported a significantly higher prevalence of SDC than non-Hispanic Whites. The reasons behind our unexpected association between SDC and ATOC are not entirely clear. However, previous studies suggest that improved cultural competency efforts in hospitals, care by providers of similar race/ethnicity, and differences in expectations and social desirability influence self-reported discharge communication.50-54
The significant association between SDC and ATOC was largely driven by associations with diet modification and follow-up medical appointment attendance. Diet education at discharge, when coupled with information promoting and rationalizing other self-care behaviors such as exercise and medication adherence, can help improve patient self-efficacy and patient ability to improve their health through self-care measure adherence.2,55,56
This study has several limitations. Both SDC and ATOC are metrics derived from patient self-report. Because information on discharge communication and ATOC variables were collected from the patient in the same 30-day questionnaire, patient self-report of SDC may also be influenced by the outcome, representing a potential antecedent consequent bias. People who reported changing their behaviors may more likely say they received sufficient discharge communication. Social desirability bias is also a potential bias for the analyses of ATOC since achieving ATOC is an accomplishment signifying a successful post-hospital transition of stroke care, and this bias may also relate to the self-reporting of SDC.
Although self-reporting is limited in that it doesn’t perfectly represent the level of education the patient received, documenting the patient’s perception of discharge stroke education experience can provide meaningful and reliable insight into the patient’s interpretation of available educational material provided at discharge. Future studies can explore both the patient perspective and perception (i.e., the perspective from patients and their representatives), like this study did, as well as clinical reporting of discharge education (i.e., nurse, physician, or care coordinator reporting) for external validation of the self-reports. The TCSD-S questionnaire is limited in that it assesses the patient perception of discharge communication only through their evaluation of sufficient diet and toxic habit cessation education and receipt of the follow-up appointment. Additionally, the mode of discharge communication delivery from the provider (i.e., verbal, written, hybrid) is not specified.
Additionally, this study did not factor in language barriers and other comprehension difficulties experienced by stroke patients. Stroke patients often experience serious cognitive impairments that negatively influence a patient’s retention of discharge education.29,57 Education and communication during the stroke discharge planning process should be simple for the patient to understand. For example, a one-page simplified information page with discharge guidance could provide a better alternative to more extended, tedious instructions that can make finding the essential details more difficult. 58 Also, evaluating a patient’s understanding by incorporating recommended strategies like the teach-back method could help healthcare professionals verify patients’ knowledge and understanding of health information. Previous studies have found that the teach-back method has demonstrated success in patient knowledge, self-efficacy, following instructions for post-discharge, reducing patient readmission, and satisfaction with discharge education.4,59,60
The Transitions of Care Stroke Disparities Study focused mainly on post-stroke behavior change and readmissions. It did not directly capture the patient’s level of understanding and comprehension of instructions at discharge, opening the possibility for potential over or under-reporting of receipt of sufficient discharge communication. Future studies should incorporate simplified language and the teach-back method to gauge patient understanding and perceived sufficiency of discharge communication. These factors could provide a more detailed and comprehensive knowledge of what makes a patient’s discharge communication more sufficient and explain whether the lack of adherence to behavior changes is tied to the lack of patient understanding of discharge instructions.
Our study sample size is limited to patients discharged from Florida hospitals to home or inpatient rehabilitation facilities, and the evaluation period is relatively short, 30 days, limiting the overall generalizability of our study results. It is essential to test this association further within a larger sample with a longer post-discharge follow-up, as 30 days is a short and challenging time for stroke patients to accomplish behaviors and activities.
Conclusion
Patient-reported, sufficient discharge communication is meaningful to examine the impact of patient perception of their stroke discharge experience on their accomplishment of transitions of care behaviors and activities, promoting lifestyle and behavioral modifications and improvements in post-stroke health and well-being, which can reduce readmissions. Findings from this study reinforce the idea that delivering quality education to stroke patients is critical for their post-stroke success. Stroke discharge guidelines should address and reflect each patient’s specific needs and concerns. Future analyses will examine the effect of SDC on readmissions amongst this cohort.
Supplemental Material
Supplemental Material - Discharge Communication and the Achievement of Lifestyle and Behavioral Changes Post-Stroke in the Transitions of Care Stroke Disparities Study
Supplemental Material for Discharge Communication and the Achievement of Lifestyle and Behavioral Changes Post-Stroke in the Transitions of Care Stroke Disparities Study by Karlon H. Johnson, Hannah Gardener, Carolina M. Gutierrez, Erika Marulanda, Iszet Campo-Bustillo, Gillian Gordon-Perue, Scott C. Brown, Hao Ying, Lili Zhou, Lauri Bishop, Emir Veledar, Farya Fakoori, Negar Asdaghi, Tulay Koru-Sengul, WayWay M. Hlaing, Jose G. Romano, Tatjana Rundek, and on behalf of the Transitions of Care Stroke Disparities Study (TCSD-S) Investigators in American Journal of Lifestyle Medicine.
Footnotes
Author’s Note
Preliminary work on this manuscript was presented at the American Public Health Association Annual Meeting and Expo in Atlanta, GA on November 17, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health/National Institute on Minority Health and Health Disparities, (1R01MD012467); PhRMA Foundation, (2023 PDVH 1059844). Dr Romano and Dr Gutierrez receive research support from National Institutes of Health (NIH) grants. Dr Romano, Dr Gardener, Dr Gordon Perue, and Dr Gutierrez receive research support from Florida Department of Health (FDOH) Grants. Dr Rundek is funded by grants from National Institutes of Health (R01 MD012467, R01 NS029993, R01 NS040807, U24 NS107267), the National Center for Advancing Translational Sciences (UL1 TR002736, KL2 TR002737), and the Florida Department of Health. Karlon Johnson is a recipient of the PhRMA Foundation Value Assessment and Health Outcomes Pre-Doctoral Fellowship Award (2023 PDVH 1059844).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.