
Abstract
Introduction
Complementary health (CH) modalities can be used as part of a Lifestyle Medicine (LM) approach to preventing and managing chronic conditions.
Methods
This cross-sectional study used data for respondents to the 2020 (N = 6,715) and 2014/2015 (N = 11,112) cycles of a Northern California health plan member survey to estimate use in 2020 of five CH modalities relevant to LM: vegetarian/vegan diet, mind/body stress management techniques (MBSM), yoga/Pilates, massage therapy, and prayer/spiritual practice. Use was estimated by sex and racial/ethnic group (White, Black, Latino, Asian/PI)) for ages 35-64 and 65-79 years and for adults 35-79 years with diabetes, hypertension, heart disease, fair/poor sleep quality, and chronic stress. CH use in 2020 was compared to 2014/2015.
Results
In 2020, 53% of adults used ≥1 of these CH modalities, including 8.4% vegetarian/vegan diet, 25.8% MBSM, 23.7% prayer/spiritual practice, 16.5% yoga/Pilates, and 17.7% massage. Sex, age group, and racial/ethnic differences were seen in use of most CH modalities, and CH modality use varied by health condition. Significant increases from 2014/2015 to 2020 were seen in use of MBSM and yoga/Pilates, vegetarian/vegan diet, and prayer/spiritual practice.
Conclusion
There is substantial opportunity to increase use of CH modalities within a LM approach to preventing and managing chronic health conditions.
Keywords
“Our study is among the first contemporary studies to estimate the use of CH modalities across different chronic health conditions.”
Introduction
There is growing interest among healthcare providers and patients in “whole person” health, defined by the National Center for Complementary and Integrative Health as “helping individuals, families, communities, and populations improve and restore their health in multiple interconnected domains—biological, behavioral, social, environmental—rather than just treating disease.” 1 The whole person approach to healthcare aligns with the growing specialty field of Lifestyle Medicine, which the American College of Lifestyle Medicine describes as the use of lifestyle interventions such as whole food, plant-predominant dietary lifestyle, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connections as the primary therapeutic modalities for prevention, treatment, and reversal of chronic health conditions. 2 The older but continually evolving field of complementary and integrative health (CH), which uses conventional Western medicine (e.g., medication, surgery, physical rehabilitation, and psychotherapy) together with non-mainstream therapies (e.g., special diets, mindfulness meditation, acupuncture, massage therapy, and yoga) in a coordinated way, also aligns with a whole person approach to treat and prevent disease, 1 also aligns with a whole person approach to healthcare. Many CH modalities can effectively be used to address one or more of the six pillars of Lifestyle Medicine, and successful use of individual CH modalities may also serve as a bridge to future adoption of the lifestyle changes recommended by the American College of Lifestyle Medicine. It has now been more than two decades since the 2012 National Ambulatory Medical Care Survey (NAMCS PII) found that more than half of office-based physicians had recommended at least one CH approach to their patients within a 12-month period. 3 However, the extent to which contemporary populations utilize these modalities is less clear.
Complementary Health Modalities Relevant to Lifestyle Medicine Pillars.
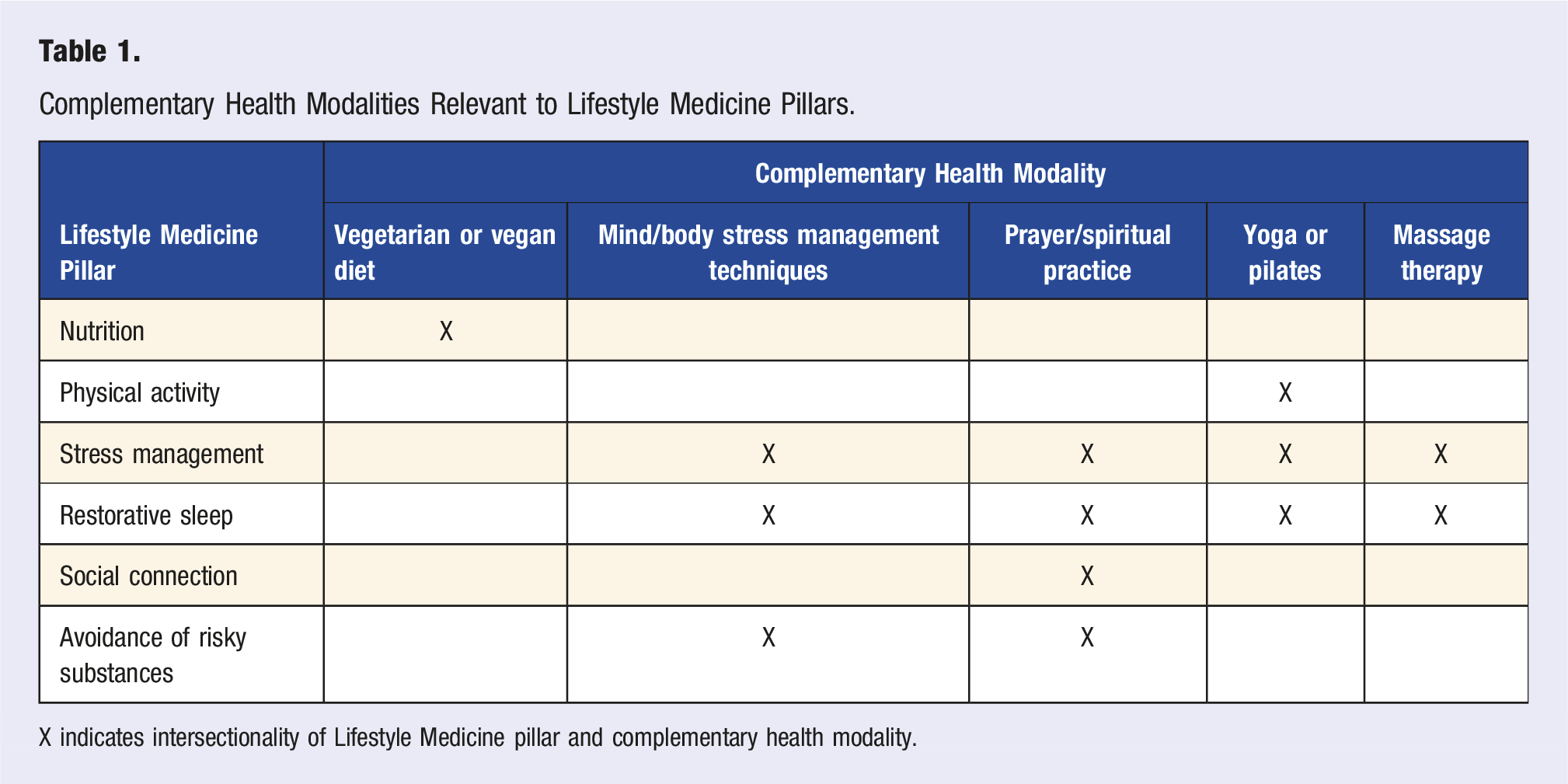
X indicates intersectionality of Lifestyle Medicine pillar and complementary health modality.
Each of these five CH modalities have been shown to positively impact chronic conditions. For example, vegetarian and vegan diets have been linked to significantly lower incidence of cancer, 16 and plant-predominant diets may play a major role in stabilizing or even reversing type 2 diabetes and cardiovascular disease.17,18 MBSM interventions have been shown to reduce blood pressure. 19 The practice of yoga has been studied as an effective adjunctive therapy for hypertension 20 and diabetes, 21 and use of Pilates-based exercise protocols has been shown to reduce glycated hemoglobin in patients with type 2 diabetes. 22 Furthermore, a combination of yoga, vegetarian diet, and meditative practices has been shown to significantly improve various parameters associated with metabolic syndrome, including waist circumference, blood pressure, hemoglobin A1c, and lipid markers. 23 Massage therapy, used in combination with antihypertensive medications, has been shown to reduce systolic blood pressure significantly more than medication alone. 24 However, it is important to note that while these CH modalities can be used to address many pillars of Lifestyle Medicine, the American College of Lifestyle Medicine views the practice of Lifestyle Medicine as the foundation of a whole person healthcare delivery system to be utilized as a primary, not complementary, approach to preventing, treating and reversing disease.
While several U.S. studies have estimated the use of CH modalities (previously called complementary and alternative medicine or CAM) among adults in the late 1990s and early 2000s, information about the use of CH modalities in contemporary community-dwelling U.S. adult populations remains limited,25-27 particularly in healthcare settings. The aims of our study were: to estimate prevalence of use of these five CH modalities in a community-dwelling adult health plan population in 2020, including those with select chronic health conditions; to examine variation in CH modality usage by demographic group; and to learn whether use of CH modalities has increased over time, given the growing interest in holistic health and therapeutic lifestyle interventions.
Methods
Setting and Study Population
Kaiser Permanente in Northern California (KPNC) is an integrated healthcare delivery system that provides primary and specialty health care to a sociodemographically diverse health plan membership that includes over three million adults who mostly reside in the Greater San Francisco Bay, Sacramento, Silicon Valley, and Central Valley areas of Northern California. The KPNC adult membership is similar to the non-Medicaid insured adult population of Northern California with regards to sociodemographic and health characteristics. 28
Data Source
We used data for KPNC members aged 35-79 years who responded to the 2014/2015 (N = 11,112) or 2020 (N = 6,715) cycles of the KPNC Member Health Survey (MHS). The MHS is a self-administered survey conducted with an age-sex stratified random sample of adults aged 25-90 who were health plan members during at least the fourth quarter of the preceding year. The 2020 survey cycle used a sample half as large as the 2014/2015 cycle. The MHS, which is conducted in English only, collects self-reported information about sociodemographic and health-related characteristics. More information about the MHS can be found in an earlier publication. 29
Study Variables
Complementary Health Modalities
The MHS included a checklist question which asked whether during the past 12 months the respondent had used any of the following methods to help prevent or manage their own health problems. In this study, we focused on the following five CH modalities: vegetarian or vegan diet; deep breathing, mindfulness meditation, or other mind-body stress management (MBSM) techniques; prayer or spiritual practice done by the individual; massage therapy (massage); and yoga or Pilates. Because many MBSM techniques were derived from prayer and spiritual practice, especially meditation, we also created a composite variable to capture use of MBSM and/or prayer/spiritual practice (MBSM/PSP).
Chronic Health Conditions
Using combined responses from two checklist questions, respondents were identified as having diabetes (other than only during pregnancy), hypertension, and/or heart disease (e.g., heart attack, angina, blocked artery, atrial fibrillation, congestive heart failure) if in the past 12 months they reported having that condition or using medication or a special diet for that condition. Separate questions were used to identify people with fair or poor sleep quality (response of fair, poor, or very poor to “How would you rate the usual quality of your sleep?”) and chronic stress or tension (response of “much of the time” or “most of the time” to “During the past 12 months, how often have you felt very stressed, tense or anxious?”).
Sociodemographic Characteristics
Sociodemographic characteristics derived from the self-reported survey data included sex (male/female); age at time of the survey; racial/ethnic group (non-Hispanic White (White), African American/Black (Black), Latino, Asian or Native Hawaiian/Pacific Islander (Asian/PI), or other); and educational attainment (≤ high school diploma, some college or associate degree, or ≥ bachelor’s degree).
Statistical Analysis
For both survey cycles, respondents were assigned post-stratification weighting factors so that the analytic sample, after weighting, would reflect the age-sex-racial/ethnic (White, Black, Latino, Asian/PI, other) composition of the 2019 KPNC membership aged 35-79 years with English as their written language preference. We used SAS Proc Surveyfreq to estimate prevalence and 95% confidence intervals (CI) for each of the five CH modalities (vegetarian or vegan diet; MBSM techniques; prayer/spiritual practice; yoga or Pilates; and massage) and MBSM/PSP among four age-sex groups overall and by race/ethnicity. Modified log-Poisson regression models were conducted to examine differences in prevalence of CH modality use by age (65-79 vs 35-64 years), sex (female vs male), and racial/ethnic (Black, Latino, Asian/PI vs White) groups after adjusting for demographic covariates.
To compare prevalence of the five CH modalities in 2014/2015 to 2020, we created normalized weights for the 2014/2015 survey that weighted respondent data to the same age-sex-racial/ethnic distribution as the 2020 weighted sample. We then produced prevalence estimates for the CH modalities in 2014/2015. To evaluate whether significant changes had occurred between 2014/2015 and 2020, for each survey cycle, we produced estimated counts of adults who used and who did not use each of the five CH modalities for each age-sex group using weighted data. Chi-square tests (using the VassarStats website statistical calculator (https://vassarstats.net/index.html) were then conducted to compare findings for each CH modality between MHS survey years.
All results reported are based on weighted survey data, and all differences mentioned in the results are significant at P < 0.05 unless otherwise noted.
Results
Characteristics of the Study Population.
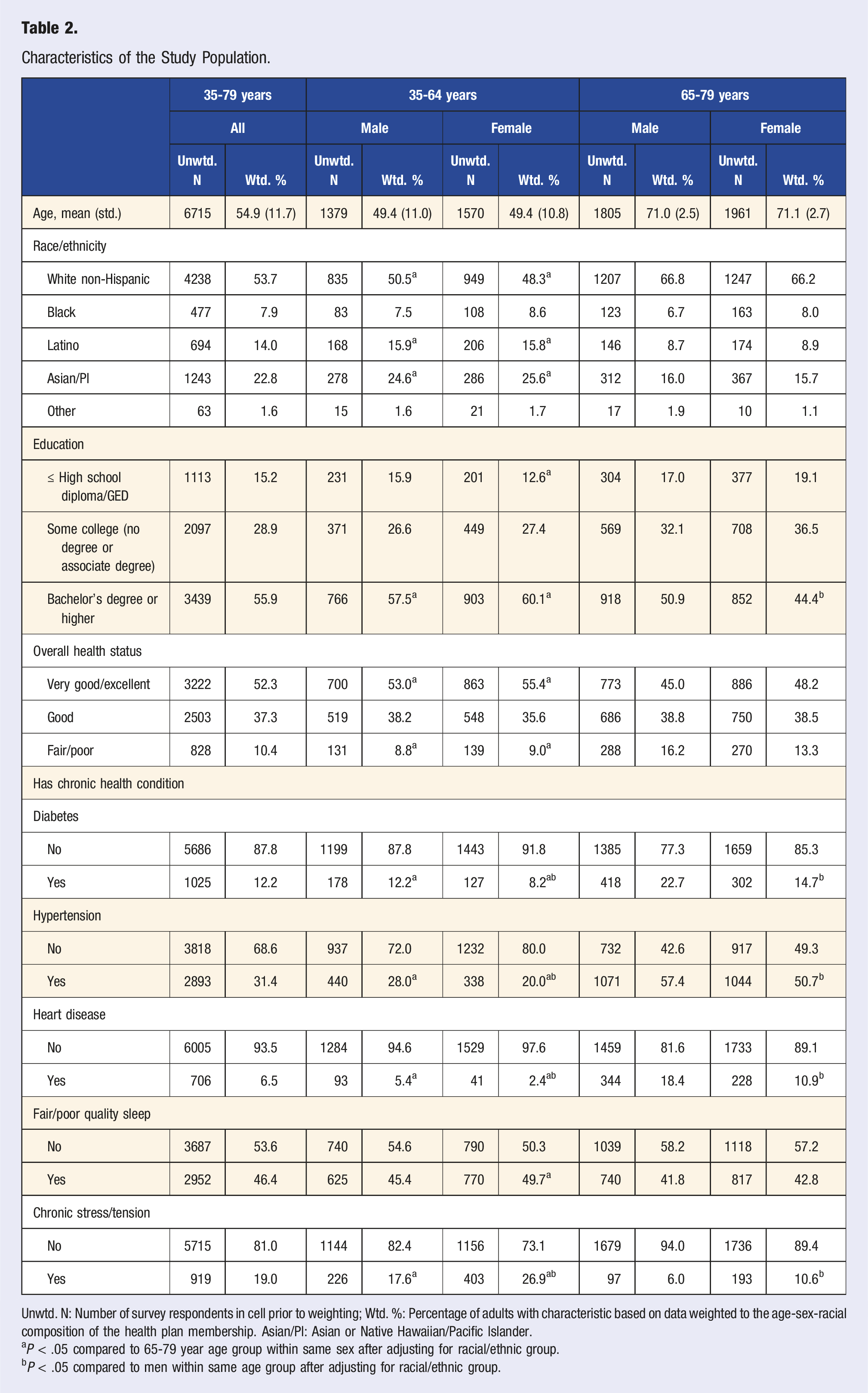
Unwtd. N: Number of survey respondents in cell prior to weighting; Wtd. %: Percentage of adults with characteristic based on data weighted to the age-sex-racial composition of the health plan membership. Asian/PI: Asian or Native Hawaiian/Pacific Islander.
aP < .05 compared to 65-79 year age group within same sex after adjusting for racial/ethnic group.
bP < .05 compared to men within same age group after adjusting for racial/ethnic group.
Use of Complementary Health Modalities in 2020
Prevalence of Use of Five Complementary Health Modalities Among Adults Ages 35-79, by Age Group and Sex, 2020.
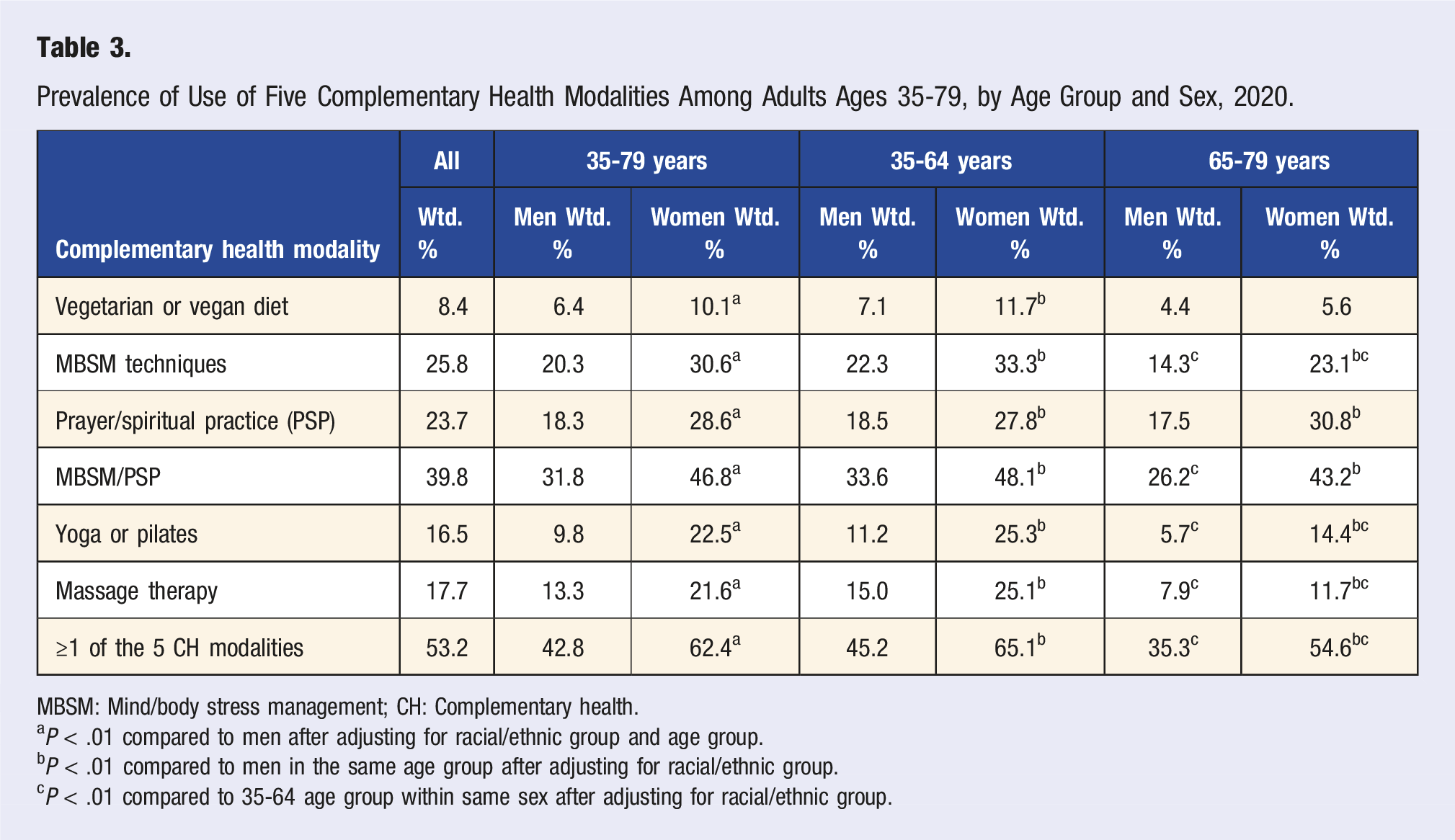
MBSM: Mind/body stress management; CH: Complementary health.
aP < .01 compared to men after adjusting for racial/ethnic group and age group.
bP < .01 compared to men in the same age group after adjusting for racial/ethnic group.
cP < .01 compared to 35-64 age group within same sex after adjusting for racial/ethnic group.
Racial/Ethnic Differences in Use of Complementary Health Modalities
Racial/Ethnic Differences in Prevalence of Use of Five Complementary Health Modalities Within Four Age-Sex Groups, 2020.
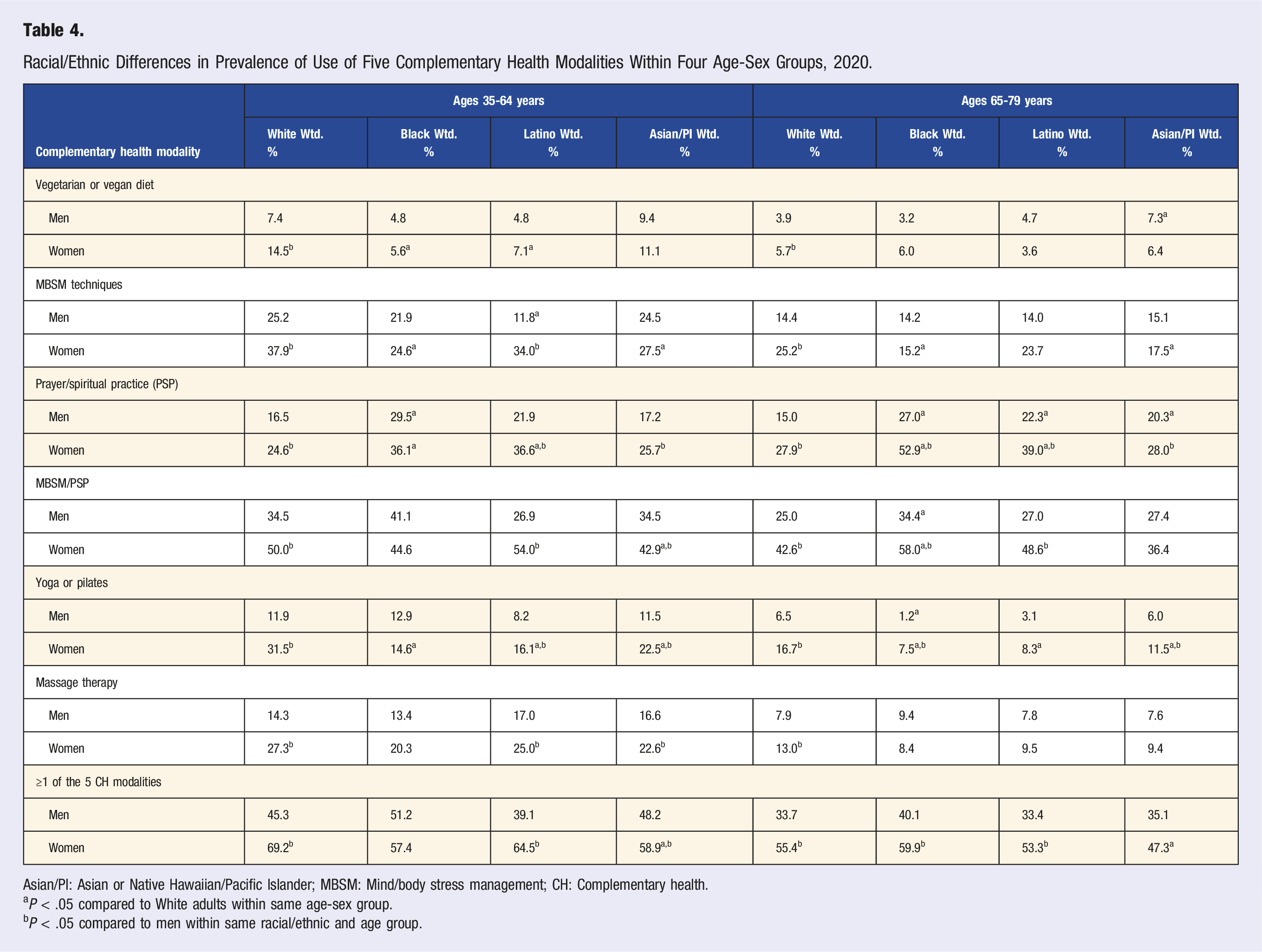
Asian/PI: Asian or Native Hawaiian/Pacific Islander; MBSM: Mind/body stress management; CH: Complementary health.
aP < .05 compared to White adults within same age-sex group.
bP < .05 compared to men within same racial/ethnic and age group.
Use of Complementary Health Modalities by Adults with Chronic Health Conditions
Prevalence of Use of Five Complementary Health Modalities in 2020 Among Adults With Selected Chronic Health Conditions.
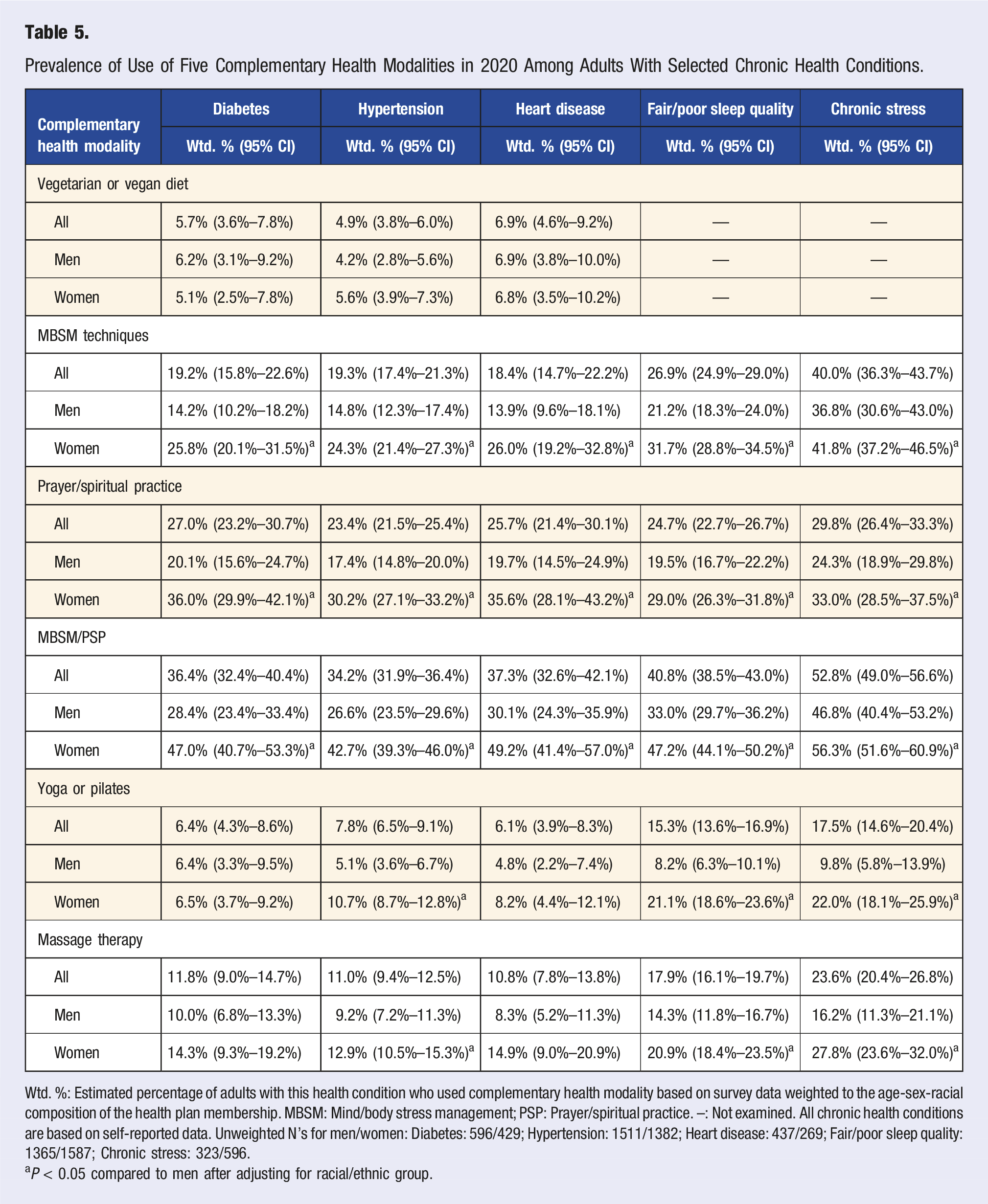
Wtd. %: Estimated percentage of adults with this health condition who used complementary health modality based on survey data weighted to the age-sex-racial composition of the health plan membership. MBSM: Mind/body stress management; PSP: Prayer/spiritual practice. –: Not examined. All chronic health conditions are based on self-reported data. Unweighted N’s for men/women: Diabetes: 596/429; Hypertension: 1511/1382; Heart disease: 437/269; Fair/poor sleep quality: 1365/1587; Chronic stress: 323/596.
aP < 0.05 compared to men after adjusting for racial/ethnic group.
We also examined whether, after adjusting for age and race and ethnicity, the same higher usage of CH modalities among women compared to men that was observed in the full population was seen in the subgroups of adults with different chronic health conditions. We found no statistically significant sex difference in use of vegetarian/vegan diet among adults with diabetes, hypertension, and/or heart disease, but the overall prevalence of use of vegetarian/vegan diet was relatively low in all of these subgroups. Women remained more likely than men to have used MBSM techniques, prayer/spiritual practice, and MBSM/PSP among adults with diabetes, hypertension, and/or heart disease, and more likely to have used prayer/spiritual practice among adults with fair/poor sleep quality and chronic stress. Women were also more likely than men with hypertension, heart disease, fair/poor sleep quality, and chronic stress to have used massage therapy, and were more likely than men with hypertension and fair/poor quality sleep to practice yoga/Pilates.
Comparing Complementary Health Modality use in 2014/2015 to 2020
We found statistically significant increases between 2014/2015 and 2020 in use of vegetarian or vegan diets (middle-aged men and women, P < 0.001), MBSM techniques (men and women in both age groups), prayer (middle-aged men and older-aged men and women), and yoga/Pilates (men and women in both age groups) (Figure 1). No significant difference was seen for massage. Use of ≥1 CH modality was significantly higher in 2020 for all age-sex groups: increasing from 57.8% (CI 56.2%–59.4%) to 64.8% (CI: 62.3-67.4) among middle-aged women, 37.2% (CI: 35.3%–39.1%) to 45.1% (CI: 42.2%–48.0%) among middle-aged men, 46.0% (CI: 43.7%–48.2%) to 53.9% (CI: 51.6%–56.2%) among older-aged women, and 28.1% (CI: 26.0%–30.2%) to 34.2% (CI: 31.9%–36.6%) among older-aged men. Comparison of complementary health modality use, 2014/15 vs 2020.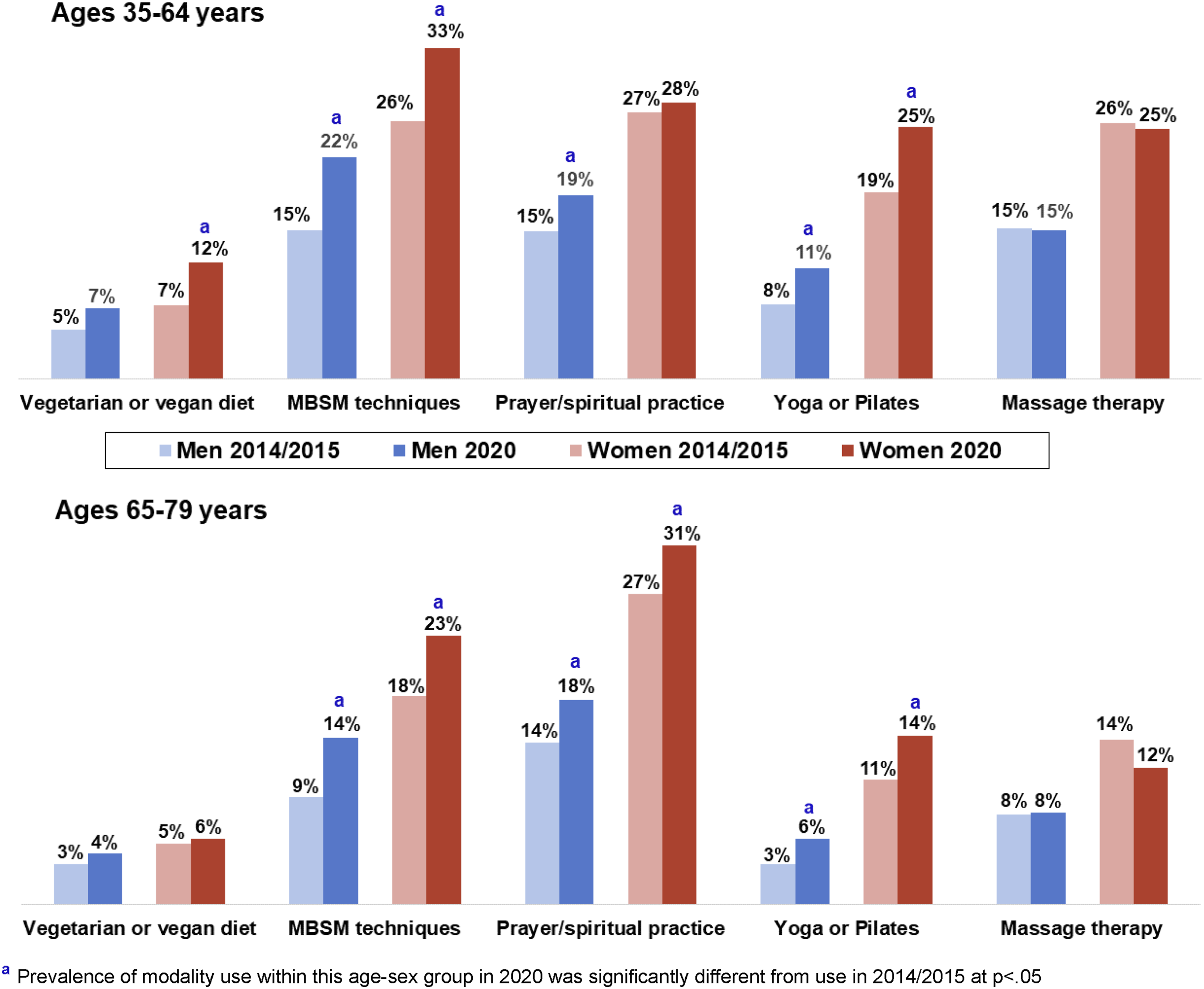
Discussion
In this study, we examined prevalence of use of five CH modalities (vegetarian/vegan diet, MBSM techniques, prayer/spiritual practice, MBSM and/or prayer/spiritual practice, yoga/Pilates, and massage therapy) and use of ≥1 of these modalities by middle-aged and older-aged adults in a community-dwelling Northern California health plan population, how usage varied by patient demographic characteristics and among adults with different chronic conditions, and how usage changed between 2014/2015 and 2020. In the overall study population, approximately half of adults had used ≥1 of these five CH modalities, with MBSM techniques and prayer/spiritual practice being the most widely used and vegetarian/vegan diet the least widely practiced. Additionally, for all modalities studied except for massage therapy, we observed significant increases in use from 2014/15 to 2020. However, in 2020, only one-fourth of adults overall were using MBSM and prayer/spiritual practice modalities, about 17% using yoga/Pilates and massage therapy, and under 10% using vegetarian/vegan diets. Women were more likely than men to be using each of the five CH modalities, and within both sexes, middle-aged adults were more likely than older-aged adults to use each of the CH modalities except prayer/spiritual practice. Our findings of greater CH use among women and younger adults is consistent with prior research.26,27
Our study is among the first contemporary studies to estimate the use of CH modalities across different chronic health conditions. Notably, we found that well under 10% of patients with diabetes, hypertension, or heart disease were following a vegetarian diet, which has been repeatedly shown to improve outcomes in these conditions. 17 In addition, MBSM techniques were used by about 20% of adults with cardiovascular conditions, about one-fourth of adults with fair or poor sleep quality, and less than half (40%) of adults reporting chronic high levels of stress and tension. Approximately one-fourth of adults across all five conditions did use prayer or spiritual practices to help manage or prevent health problems, with more than one-third of adults with cardiovascular conditions or sleep issues and over half of adults with chronic stress using either MBSM, prayer, or spiritual practices. While we did not have sufficiently sized subgroups to explore racial/ethnic differences in use of MBSM techniques and prayer within these chronic conditions, we assume, based on findings from the full study population, that Black and Latino adults with these chronic conditions are less likely to be using MBSM techniques and more likely to be using prayer. Since both prayer and MBSM have similar positive effects on health, a culturally sensitive approach would be to encourage regular use of either modality, as well as potentially suggesting that some elements of MBSM, such as mindful breathing, could be beneficially incorporated into or between meditation or prayer sessions.
Overall, we found relatively low use of the five CH modalities we studied by adults with chronic health conditions that could potentially be better managed with their use. These findings may be highly relevant for primary care practice. Indeed, four of the CH modalities (MBSM techniques, prayer/spiritual practice, yoga/Pilates, and vegetarian or predominantly plant-based diet) can be learned through in-person or virtual training, and once learned, are quite inexpensive for patients to implement and sustain, unless they decide to join a fee-for-class group. Healthcare providers, especially those interested in the Lifestyle Medicine first approach that considers Lifestyle Medicine as the foundation for a whole person approach to all healthcare, can play an important role in recommending these CH modalities to their patients. However, they must first become more knowledgeable about how these modalities can help certain conditions and understand where to refer patients who express interest in learning how to use them. Further, while most commercial and government-funded health insurers do not offer coverage for massage therapy or yoga classes as a benefit, patients may be able to get at least partial reimbursement for out-of-pocket costs for these CH modalities from their healthcare reimbursement, healthcare savings, or flexible spending accounts with a form completed by a licensed healthcare provider that recommends a specific CH modality for treatment of a diagnosed health condition. 30
Strengths of our study include the large sociodemographically diverse study population, measurement of multiple CH modalities, and use of comparison data within the same health plan to examine how CH modality use changed from 2014/2015 to 2020. However, we acknowledge some limitations that may affect generalizability of the study results. First, we reported on an aggregated Asian/PI group, which may mask Asian ethnic subgroup differences in CH use. Second, while we were able to estimate use of the five CH modalities among adults with different types of chronic conditions, we were unable to link use of the CH modalities specifically to management of those conditions. Third, the survey was administered only in English, so racial/ethnic differences identified in our analyses are not generalizable to adults who do not read and understand English well. Fourth, post-stratification weighting of the respondent sample to reflect the underlying age, sex, and racial/ethnic composition of the health plan population may not have overcome all sources of survey nonresponse bias. Finally, our study sample was drawn from members of a very large but single integrated healthcare delivery system located in a geographic region where previous national surveys have shown a higher prevalence of CH use compared to other parts of the U.S. 26
Conclusion
The percentages of adults who use complementary health modalities has been increasing, suggesting that many patients may be open to an integrative and Lifestyle Medicine approach to their health care. This positive trend should encourage physicians, especially those in primary care or Lifestyle Medicine clinics, to incorporate relevant evidence-based CH modalities into their practice. The National Center for Complementary and Integrative Health urges a greater focus on implementation science to study how evidence-based CH modalities can be best integrated into clinical settings to improve patient outcomes. 31 Future research is needed to better understand and develop ways to overcome potential barriers to integration of CH into clinical practice, such as reimbursement considerations, provider familiarity with available resources, and patient expectations (i.e., expecting to get prescription medication rather than a referral for CH).
Footnotes
Acknowledgments
The authors would also like to thank the survey team and all the survey participants for participating in the Member Health Survey.
Author Contributions
CQ, NG, and JL conceived and designed the study; NG acquired the data and conducted the data analyses; CQ, NG, and JL contributed to the interpretation of the data; CQ, NG, JL and NR drafted the manuscript; all authors approved the final version for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nancy Gordon received support from the Kaiser Permanente Northern California Community Health Program.
Ethical Statement
Data Availability Statement
The Kaiser Permanente Northern California (KPNC) Institutional Review Board has not provided approval for Member Health Survey data to be placed in a public access repository. However, researchers can request access to use this study data by contacting the corresponding author (NPG).