
Abstract
The study tested the effects of a vegan diet on cardiometabolic outcomes and quality of life among healthcare employees during the COVID-19 pandemic. Overweight hospital employees were enrolled and randomly assigned (in a 1:1 ratio) to an intervention group, which was asked to follow a low-fat vegan diet, or a control group, asked to make no diet changes. However, due to COVID-19 disruptions, all participants remained on their usual diets from March to June (12 weeks), creating a de facto control period, and all (n = 12) started the vegan diet with online classes in June, which continued for 12 weeks. Nine participants completed all final assessments. A crossover ANOVA was used for statistical analysis of differences in cardiovascular health during the control period and during the intervention. Despite the ongoing crisis, body weight decreased (treatment effect −5.7 kg [95% CI −9.7 to −1.7]; P = .01); fasting plasma glucose decreased (−11.4 mg/dL [95% CI −18.8 to −4.1]; P = .007); total and LDL-cholesterol decreased (−30.7 mg/dL [95% CI −53.8 to −7.5]; P = .02; and −24.6 mg/dL [−44.8 to −4.3]; P = .02, respectively); diastolic blood pressure decreased (−8.5 mm Hg [95% CI −16.3 to −.7]; P = .03); and quality of life increased (P = .005) during the intervention period, compared with the control period. A vegan diet improved cardiometabolic outcomes and quality of life in healthcare workers at the height of the COVID-19 pandemic.
“Plant-based diets have a positive effect on individual quality of life both in and out of the workplace.”
Introduction
More than 70% of U.S. adults have excess body weight, 1 which puts them at increased risk for diabetes, hypertension, dyslipidemia, and cardiovascular disease. The incidence of cardiovascular disease is on the rise, and the rate of this increase is similar among hospital workers to the general public.2,3 Healthcare professionals’ health is important to consider and address because it may also affect patient care. For example, physicians with a normal body mass index were found to be more likely than overweight physicians to talk to their overweight patients about weight loss (30% vs 18%). 4
Supporting the cardiometabolic health of healthcare workers has become particularly important during the COVID-19 pandemic because coronary heart disease, obesity, and type 2 diabetes have been shown to contribute to a more severe course of COVID-19. 5 Plant-based diets have been shown to reduce body weight, blood pressure, fasting plasma glucose, and plasma lipids,6,7 and improve quality of life,8,9 and studies testing these benefits of a plant-based diet specifically in healthcare workers are urgently needed.
The aim of this study was to test the effects of a low-fat vegan dietary intervention on body weight, blood pressure, fasting plasma glucose, and plasma lipid concentrations, as well as quality of life and food acceptability, among healthcare employees in a clinical setting.
Design and Methods
Study Design and Eligibility
This study was conducted between January 2020 and September 2020 at Sibley Memorial Hospital in Washington, DC. Hospital employees with a body mass index >25 kg/m2 were enrolled. Exclusion criteria were type 1 diabetes, smoking, alcohol or drug abuse, pregnancy or lactation, and current use of a vegan diet. The study protocol was approved by the Advarra Institutional Review Board. All participants gave written informed consent.
Randomization and Study Groups
Using a computer-generated system, participants were randomly assigned (in a 1:1 ratio) to an intervention group, which was asked to follow a low-fat vegan diet, or a control group, which was asked to make no diet changes. Because assignment was done simultaneously, allocation concealment was unnecessary.
The intervention diet (∼75% of energy from carbohydrates, 15% protein, and 10% fat) consisted of vegetables, grains, legumes, and fruits, without animal products or added fats. The participants were asked to eat less than 30 g of total fat per day and were instructed to favor low-glycemic-index foods. However, no limits were put on refined grains or added sugars. Vitamin B12 was supplemented (500 μg/day). The intervention group was asked to attend weekly classes for detailed instruction and cooking demonstrations. No meals were to be provided. Dietary adherence for the intervention diet was defined as the absence of meat, poultry, fish, dairy, or egg intake, and saturated fat ≤5% and total fat ≤25% of energy, and average daily cholesterol intake ≤50 mg on 3-day dietary records.
For both groups, alcoholic beverages were to be limited to 1 per day for women and 2 for men. All participants were asked to maintain their customary exercise habits and medications, unless modified by their personal physicians.
While the study was planned as a single-center, open parallel design investigation, the arrival of the COVID-19 pandemic necessitated a design modification after study onset.
Outcomes
All measurements were to be performed at baseline and 12 weeks. The primary outcomes were body weight, blood pressure, fasting plasma glucose, and blood lipids; the secondary outcomes were quality of life and food acceptability.
At baseline and at 12 weeks, dietary intake data over 3 consecutive days were to be collected and analyzed by staff members certified in Nutrition Data System for Research version 2020, developed by the Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN. 10 All study participants were asked not to alter their exercise habits and to continue their preexisting medication regimens for the duration of the study. Physical activity was assessed by the International Physical Activity Questionnaire. 11
Laboratory assessments were made after an overnight fast. Height (baseline only) and weight were measured using a stadiometer and a calibrated digital scale, respectively.
Blood pressure was measured after participants have rested in a seated position for 5 minutes, using a digital blood pressure monitor Omron M6 Comfort IT (Omron, IL, USA). Three measurements were taken at 1-minute intervals. The first measurement was disregarded, and the mean of the remaining 2 measurements was calculated.
Plasma glucose concentration was analyzed using the Hexokinase UV endpoint method. HbA1c was measured by turbidimetric inhibition immunoassay, and lipid concentrations were measured by enzymatic colorimetric methods. All test kits were made by Roche, Basel, Switzerland.
Quality of life was assessed using the SF-36, which is a brief health survey with 36 questions, developed by the Boston Health Research Institute in the United States. The SF-36 provides a profile of functional health and well-being scores, as well as psychometrically-based physical and mental health summary measures. The SF-36 is a general measure that has been administered across various age groups, disease spectra, and treatment regimens. Items on the SF-36 are scored on a scale of 0-100, with a higher score indicating better health-related quality of life. The SF-36 has undergone extensive validity and reliability trials, and published reliability statistics have exceeded the minimum standard of .70, which is recommended for measures used in group comparisons, in more than 25 studies.12,13
The Food Acceptability Questionnaire was used to measure attitudes about the intervention diet, including desire to adhere, likelihood to adhere in the future, and attitudes about accessibility of sustaining the diet, using seven-point response scales. 14
The Eating Inventory is a highly reliable 51-item questionnaire providing quantitative measures of dietary restraint, disinhibition, and hunger. 15 The dietary restraint measure is an index of the extent to which participants feel constrained by their assigned diets. The disinhibition factor indicates overeating in response to stress or other cues. The hunger score assesses the subjective experience of hunger. Its principal use in the current study was a gauge of ease in adapting to the intervention diet, which is indicated by changes in restraint and hunger scores.
Statistical Analysis
Distributions of the data were examined graphically for each outcome to make sure that the criteria were met for the parametric analyses. A crossover ANOVA model was used to evaluate the data. Data from only those with measurements at both time points were included in the ANOVA model.
Results
Participant Characteristics
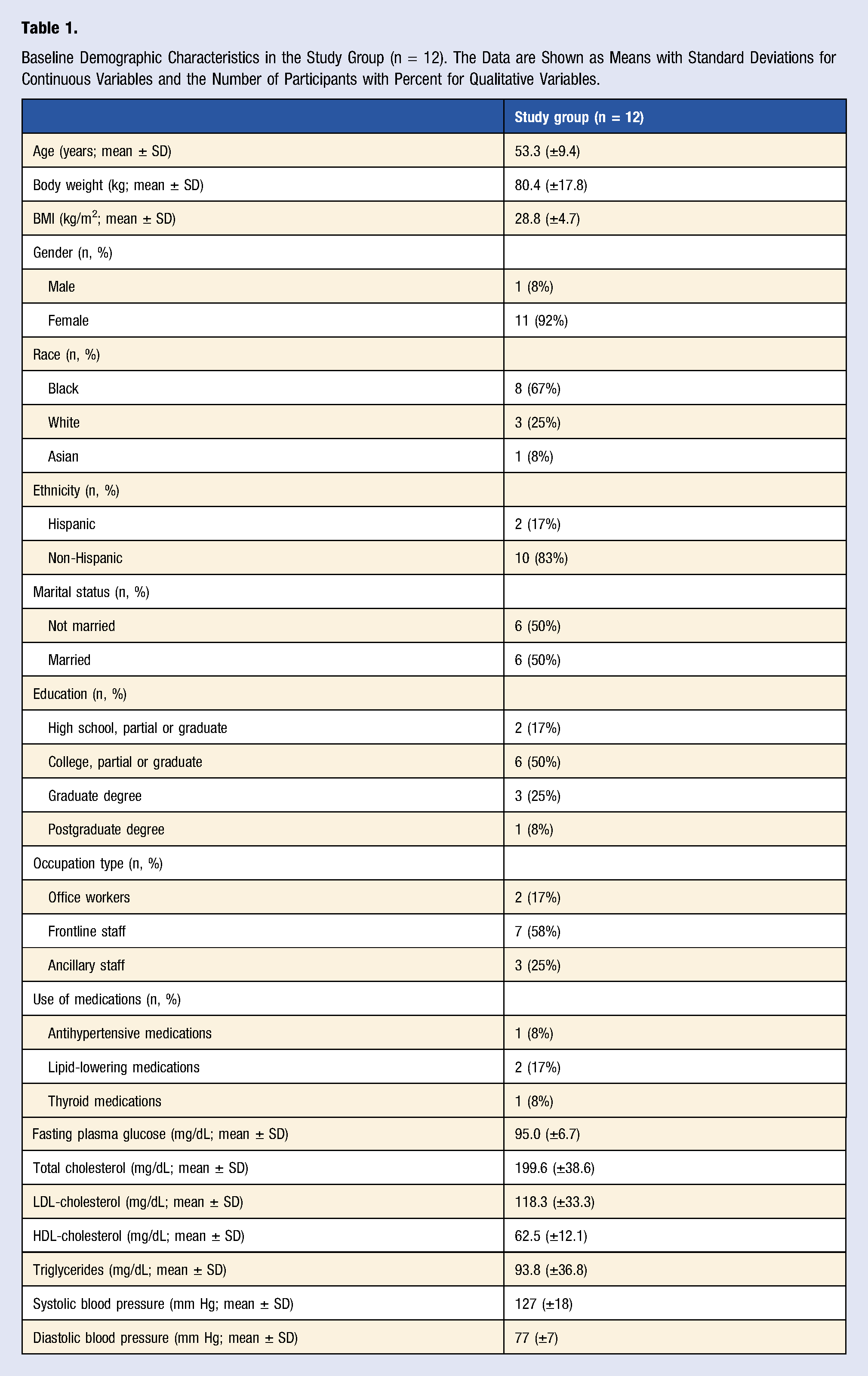
Of 237 people who expressed interest in the study, 32 met participation criteria, signed the consent form, and were randomly assigned to the intervention (n = 16) or control (n = 16) groups in a 1:1 ratio Enrollment of the participants and completion of the study. Baseline Demographic Characteristics in the Study Group (n = 12). The Data are Shown as Means with Standard Deviations for Continuous Variables and the Number of Participants with Percent for Qualitative Variables. Changes in Outcomes During the Study Comparing a Low-Fat Vegan Dietary Intervention Versus the Control Phase. Data are Means with 95% Confidence Intervals. Listed P Values are Assessed by Crossover ANOVA. *P < .05, ** P < .01 and *** P < .001 for Within-Group Changes from Baseline.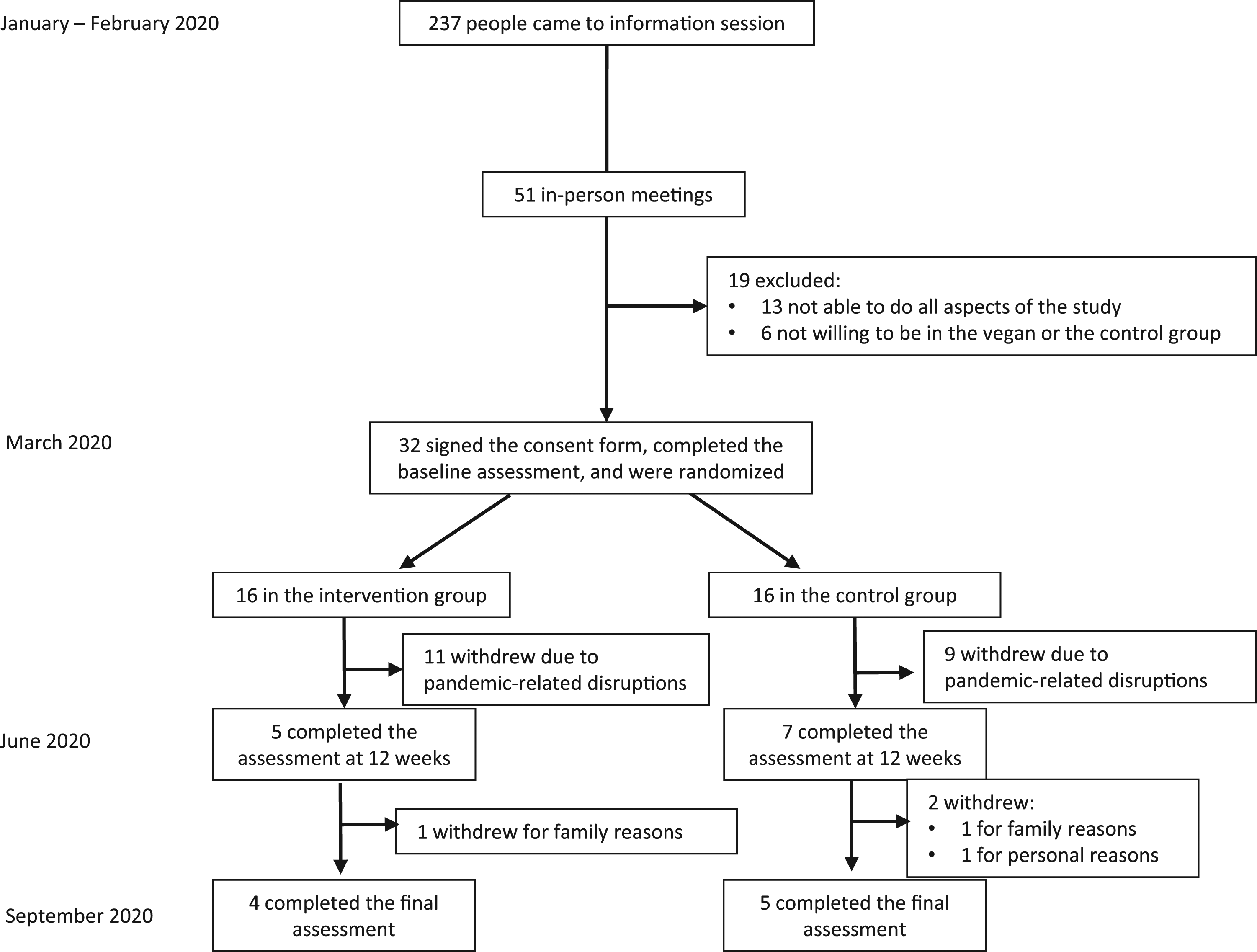
Physical Activity and Dietary Intake
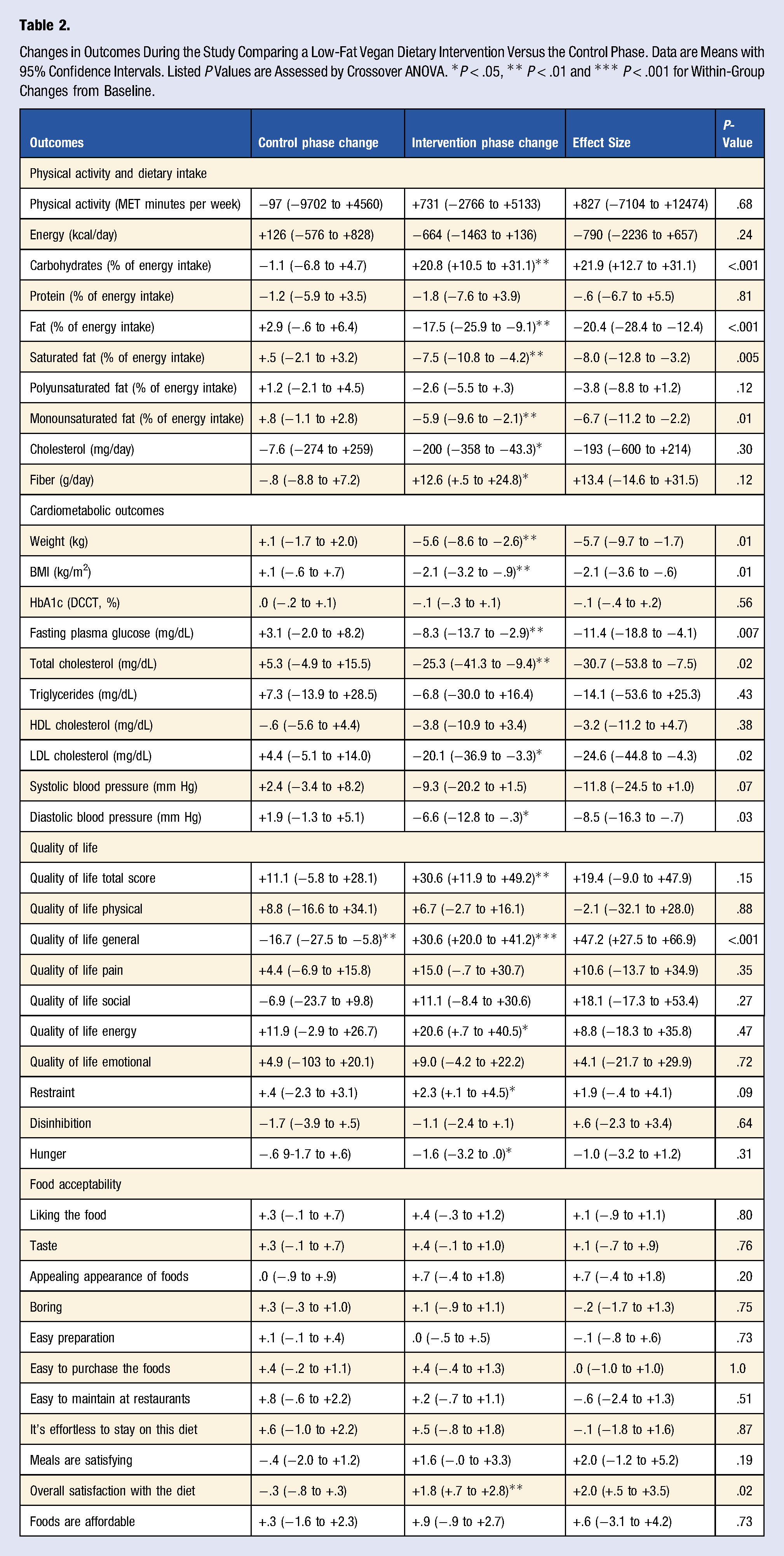
Physical activity and energy intake did not change significantly in either phase. Carbohydrate intake increased during the intervention phase (treatment effect +21.9% of energy [95% CI +12.7 to +31.1]; P < .001) while fat intake decreased (treatment effect −20.4% of energy [95% CI −28.4 to −12.4]; P < .001) and protein intake did not change significantly. Saturated and monounsaturated fat intake decreased during the intervention phase (treatment effect −8.0% of energy [95% CI −12.8 to −3.2]; P < .001; and −6.7% of energy [95% CI −11.2 to −2.2]; P < .001, respectively), while polyunsaturated fat intake did not change significantly.
Adherence to the intervention diet was high. Eight of the nine participants (88.9%) who completed the study reported consuming no animal products and their cholesterol intake was under 50 mg/day. Seven of the nine participants (77.8%) also met the total fat and saturated fat adherence criteria.
Cardiometabolic Outcomes
Compared with the control period, body weight decreased during the intervention period (treatment effect −5.7 kg [95% CI −9.7 to −1.7]; P = .01). Fasting plasma glucose decreased during the intervention period, with no change during the control period (treatment effect −11.4 mg/dL [95% CI −18.8 to −4.1]; P = .007). Total and LDL-cholesterol decreased in the intervention period, with no significant change during the control period (treatment effect −30.7 mg/dL [95% CI −53.8 to −7.5]; P = .02; and −24.6 mg/dL [−44.8 to −4.3]; P=.02, respectively). Systolic blood pressure did not change significantly during either period (treatment effect −11.8 mm Hg [95% CI −24.5 to =1.0]; P = .07). Diastolic blood pressure decreased in the intervention period, with no change during the control period (treatment effect −8.5 mm Hg [95% CI −16.3 to −.7]; P = .03).
Quality of Life and Food Acceptability
Total quality of life increased during the intervention period (+30.6 points, 95% CI +11.9 to +49.2; P = .005) with no significant change during the control phase. General quality of life decreased in the control phase (−16.7 points; 95% CI −27.5 to −5.8; P = .008) while it increased during the intervention period (+30.6 points; 95% CI +20.0 to +41.2; P < .001). Other quality of life sub-scores (physical, pain, emotional, energy, and social) did not change significantly during either period. Food acceptability was comparable in both phases. The overall satisfaction with the diet increased during the intervention period (+2.0 points; 95% CI +.5 to +3.5; P = .02).
Discussion
This 12-week study in hospital employees has shown that, despite the onset of a major crisis disrupting hospital work, a low-fat vegan diet nonetheless reduced body weight, fasting plasma glucose, total and LDL-cholesterol, and diastolic blood pressure compared with the control phase. Despite the stresses that are routine in hospital work and the greatly added stress of the pandemic, general quality of life and the overall satisfaction with the diet increased during the intervention phase.
Maximizing the cardiometabolic health of healthcare workers is particularly important during the COVID-19 pandemic. In a cohort study of 1590 hospitalized patients with COVID-19, the presence of coronary heart disease increased COVID-19 mortality 4-fold. 16 Obesity and diabetes also increase the severity of the illness.17-19 Therefore, because during the pandemic, healthcare workers are both caregivers and potential patients, improving their cardiometabolic health is crucial.
Plant-based diets have been previously shown to reduce cardiometabolic disease and cardiometabolic risk. 20 In the present trial, the average weight loss was 5.7 kg, reflecting a robust body of evidence showing the efficacy of plant-based diets for weight loss and weight management. A meta-analysis of fifteen randomized controlled trials showed that individuals assigned to a vegetarian diet lost significantly more weight than those assigned to non-vegetarian diets, with a mean weight loss of 3.4 kg in an intention-to-treat analysis and 4.6 kg in a completer analysis. 21
In the present study, the low-fat vegan diet reduced diastolic blood pressure by 8.5 mm Hg on average. This is in line with the findings from previous studies. In 2020, a meta-analysis of fifteen randomized clinical trials with 856 participants found that vegetarian diets lowered systolic blood pressure by 2.7 mmHg and diastolic blood pressure by 1.7 mmHg compared to an omnivorous diet. 22
Fasting plasma glucose was reduced by 11.4 mg/dL on average on the low-fat vegan diet. There is strong evidence from previous studies that plant-based diets improve glycemic control and increase insulin sensitivity.23,24 Insulin resistance is related to lipid accumulation in muscle and liver cells. 25 A recent randomized controlled trial demonstrated that a low-fat vegan diet reduced this lipid content and improved insulin sensitivity in overweight adults. 26
The average reduction in total and LDL-cholesterol was 30.7 and 24.6 mg/dL, respectively. A 2020 umbrella review of systematic reviews and meta-analyses found that a vegetarian diet was associated with significantly reduced plasma cholesterol. 27 Data from clinical studies indicate that for every 1% reduction in LDL-cholesterol, the risk for a major cardiac event, including heart attack and stroke, is reduced by approximately 1%. 28
The increased general quality of life in the healthcare workers in our study is a significant finding.
Plant-based diets have a positive effect on individual quality of life both in and out of the workplace. In an 18-week study in a large U.S. insurance company, a plant-based diet decreased anxiety, depression, and job absenteeism. 29
Acceptability of the low-fat vegan diet was comparable to the participants’ usual diets, confirming the findings of previous studies.29-33 In a 6-month study of 38 individuals practicing 5 new dietary patterns (omnivorous, pesco-vegetarian/semi-vegetarian, vegetarian/vegan), all participants had equal rates of acceptability and adherence pertaining to their diets. In a 74-week study of 99 people with type 2 diabetes, a low-fat vegan diet had similar acceptability to a conventional diabetic diet. These findings suggest no barrier to the use of plant-based diets in medical nutrition therapy. 29
This study has both strengths and limitations. The fact that it occurred during the height of the initial wave of the COVID-19 pandemic is both a strength (ie, taking advantage of an unusual opportunity to investigate a vitally important aspect of health, that of hospital staffers during a crisis) and a weakness, as many volunteers were drawn away and unable to participate. Furthermore, the vast majority of our study participants were women. The final analysis performed, which treats the trial as a crossover study, differs from the originally planned two-arm design. However, our analysis provides a valid assessment of the treatment effect comparing a control to a plant-based diet, and having the same participants on both diets increases statistical power to detect effects in our small study cohort. We note that the order of interventions was identical in all participants, rather than randomized as would have been the case in a prespecified crossover design. The final subject sample was small, with 9 participants completing both an intervention phase and a control phase. Nonetheless, the clinical effects were large, statistically significant, and clinically important, and the study shows that, during a time of crisis, the health benefits of the dietary intervention were nonetheless apparent.
Conclusion
In conclusion, this 12-week study in healthcare workers during a crisis has shown that a low-fat vegan diet reduced body weight, fasting plasma glucose, total and LDL-cholesterol, and diastolic blood pressure, and increased general quality of life and the overall satisfaction with the diet compared with the control phase. These findings are significant due to the impact of the healthcare workers’ health on patient care, particularly in light of the COVID-19 pandemic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Physicians Committee for Responsible Medicine.