
Abstract
Background: Parents play a critical role in their children’s health. We explored the association of children’s perception of their parents’ health behaviors and education level with the health behaviors of middle-school students participating in a school-based wellness program. Methods: Students completed a baseline survey on their dietary, physical activity, and sedentary behaviors, and their parents’ health behaviors and education. Descriptive statistics and generalized linear regression with random intercept analyzed which child-reported parent behaviors, parent education levels, and demographic factors were associated with healthy child behaviors. Results: Among 4607 students, for all behaviors assessed, children who perceived their parent exhibiting a healthy behavior were more likely to display the same healthy behavior. Healthier diet, more physical activity, and less sedentary habits were reported by students who reported their parents had college or higher education, compared to students who reported their parents had some college or less education. Conclusions: These results encourage increased parental involvement in childhood wellness programs. Additionally, these data suggest interventions which target parents with lower educational attainment may also benefit their children’s health behaviors. As we continue to understand how adolescent behavior is shaped, we can increase the effectiveness of targeted health education for parents and children.
“Adolescence offers unique opportunities for child independence, including physical activity and food choices at school.”
Introduction
The prevalence of childhood obesity has risen dramatically in the United States, from 4.0% among children aged 6-11 years in the 1970s to 20.3% in 2018. 1 Obesity has been associated with significant health risks, including diabetes, hypertension, osteoarthritis, sleep apnea, gallbladder disease, some forms of cancer, and cardiovascular disease, 2 with cardiovascular disease being the leading cause of death in the United States. 3
Many factors influence a child’s likelihood of becoming obese, including poor nutrition and lack of physical activity.4,5 Parents and legal guardians, who strongly influence the home environment, given they are the predominate household members responsible for food purchases, cooking, and transportation, are critical in the development of the health habits of their children. Parents serve as role models for children and have the ability to provide or limit access to resources, such as healthy foods or opportunities for physical activity. During adolescence, defined as ages 10-19, 6 children are often obtaining more independence and given more choices regarding food consumption and physical activity (e.g., snacks after school, lunch consumption, sports and after-school activities). Some studies have suggested that parents’ behaviors toward food influence children’s food choices and how they moderate caloric intake, from infancy through adolescence.7,8 In the Australian Healthy Dads, Healthy Kids trial, in addition to fathers’ beliefs about healthy eating mediating their school-aged children’s dietary behavior, co-physical activity of father and child mediated the child’s physical activity. 9
Social determinants of health, defined by the World Health Organization as “the conditions in which people are born, grow, work, live, and age,” greatly impact health outcomes as well.10,11 One such determinant is education, which has been linked to social support, health literacy, employment opportunities and, thereby, income, health benefits, and working conditions. 10 Though not extensively researched, some studies have suggested that parental education also plays a role in their children’s health. Maternal education level has been shown to influence obesity prevalence in infants up to 12 months of age, and higher maternal academic levels resulted in lower rates of obesity in 5 year-olds. 12 Additionally, a study in France discovered higher education levels in both father and mother were associated with lower BMIs and obesity prevalence for children up to 17 years old when compared to children with parents of lower education levels. 13 In many health categories (e.g., smoking, alcohol consumption, and physical activity), each additional year of education has been shown to be associated with fewer unhealthy behaviors and more healthy behaviors. 14 Although these studies were not limited to adolescents, they suggest that parent education level may influence children’s health behaviors throughout childhood.
As discussed, several prior studies suggest parental behaviors and education impact their children’s health and behaviors during adolescence.7-9,13 However, to our knowledge, no studies have assessed the impact of the child’s perception of their parents’ health behaviors and education levels on the child’s health behaviors. This is the objective of our study. We suspect that children in this age group are able to conceptualize what education levels and health behaviors their parents have. We also find it reasonable that adolescents who perceive various lifestyle habits (e.g., eating habits, levels of physical activity) among their parents may be more likely to model these perceived behaviors. We hypothesize that children who perceive their parents to have healthier behaviors will also demonstrate healthier behaviors. Additionally, we hypothesize that higher parent educational levels, as reported by their children, will correspond with healthier behaviors in children. By investigating these factors, specifically children’s perceptions of their parents’ education and health behaviors, we may be able to further understand how adolescent health behaviors are shaped.
Methods
In response to the childhood obesity epidemic, Project Healthy Schools (PHS) was designed to use school-based health education and environmental changes to support healthy behaviors among middle-school children and reduce risk factors for cardiovascular disease and obesity. 15 All PHS program components are designed to promote 5 principal goals: (1) eat more fruits and vegetables, (2) choose less sugary beverages, (3) eat less fast and fatty food, (4) be active every day, and (5) spend less time in front of a screen. The program has been implemented in over 150 middle schools and has reached more than 90,000 students in Michigan since 2004. The schools represent a diverse range of socioeconomic statuses from a variety of locations throughout the state.
Students are invited to complete a health behavior survey prior to starting PHS during the Fall semester of the academic year (baseline) and at the end of the program during the Spring semester of the same academic year (follow-up). This survey is an abbreviated version of the validated School Physical Activity and Nutrition (SPAN) survey. 16 Demographic information (sex, race) is collected at baseline. Race or ethnicity is self-reported by the students from a list including “White,” “Black,” “Asian,” “Hispanic,” “Native American,” or “Other.” Students further complete 28 questions about their dietary, physical activity, and sedentary behaviors. Dietary question responses range from “none” to “3 or more times” on a 4-point scale. Physical activity question responses range from “0 days” to “7 days” on an 8-point scale. Sedentary screen time habit question responses range from “0 hours” to “6 hours or more” on an 8-point scale. Additional 7 questions ask the children about their parents’ education and health behaviors (dietary, physical activity, and sedentary). Parental health behavior questions are modeled after a combination of the validated SPAN survey and the European ENERGY survey.16,17 Health behavior response options for perceived parental behaviors are the same as the health behavior response options for the students. Questions that ask children about their parents’ education were added to the survey in 2013, and questions that ask children about their parental health behaviors were added in 2015. Over 25,000 students have completed the baseline health behavior survey since the program’s inception; about 14,000 of these surveys were completed after the addition of the parental health behavior questions in 2015. For this cross-sectional study, baseline survey data collected between 9/1/2015 and 3/31/2021 were included in analysis; no follow-up data were analyzed. Student written assent was obtained before collecting survey data. Students were not required to complete the survey and could opt out of any or all portions of the survey. Parental consent was not required to collect student study data, as only survey data and not biometric data were collected. Information on the PHS program, including measurement components, was sent home to the students’ parents/legal guardians. This study underwent full board review and obtained approval for the study, including the waiver of parental informed consent, by the Institutional Review Board at the University of Michigan.
Sixth grade students (aged 11-12 years old in the United States) from Michigan schools participating in PHS who, (1) provided information on at least one parent’s education level, and (2) answered at least one of the 5 questions regarding parental health behaviors, were included in this study. Association of child-perceived parent behaviors was evaluated individually for each of the 5 behaviors. No attempt was made to measure children’s overall health behaviors, perceived parent’s overall health behavior, or to evaluate the association of the overall health behaviors between the children and parents. Over 80% of students reported at least 4 parent health behaviors.
Baseline behaviors of both students and parents, as reported by students, were categorized as “healthier” or “unhealthy” based on recommendations from the U.S. Department of Health and Human Services, the Centers for Disease Control and Prevention, and information from the National Institutes of Health.18-21 Some behavioral criteria were modified to reflect data which indicates that many adolescents are not meeting the current dietary and physical activity guidelines. 19 “Healthier” behaviors were defined as follows: (1) ≥1 time/day eating fruits or vegetables, (2) ≥1 day/week vigorous (for 20 minutes or more) or moderate (for 30 minutes or more) physical activity, (3) ≤1 time/day eating fast or fatty foods (including fatty or fried meats like hot dogs, sausage, or bacon, fried foods or snacks), (4) ≤1 time/day drinking sugary beverages (including regular or diet soda, punch, sweet teas, Kool-Aid®), and (5) ≤2 hours/day of TV, computer, or video game screen time. These parameters were developed and utilized in a previous PHS study, which found that children who reported less “healthier” behaviors were associated with worse cardiometabolic measures. 22
Children were asked to report the highest obtained level of education for up to 2 parents/guardians. We defined parent education level as the higher level of education obtained among the 2 parents/guardians if both were reported by the student. Parent education levels were categorized as “college graduate or higher,” which included options “college degree” and “graduate or professional degree [Master’s degree, PhD, MD, etc.],” or “some college or less,” which included options “less than high school,” “high school or GED,” and “some college.”
Socioeconomic status (SES) was assigned to all participants in a school based on the median household income of homes within the school’s zip code. This was divided into low SES (median household income <$36,180), middle SES ($36,180-$48,240), and high SES (>$48,240) groups. These cutoffs were based on the 2017 federal poverty level (FPL), 23 with $36,180 representing 300% above the FPL and $48,240 representing 400% above the FPL. Households with income up to 300% of the FPL may be eligible for the Children’s Health Insurance Program, 24 while the Affordable Care Act provides subsidies for households with income up to 400% of the FPL. 25
Data Analysis
Categorical variables were reported as frequencies and proportions. Comparisons of the proportions of healthy behaviors were made between the 2 parental educational groups using Fisher’s exact tests. We assessed the agreement between child and perceived parent healthy behaviors based on McNemar’s test.
Descriptive statistics were used to determine which perceived parent behaviors and parent education levels were associated with child behaviors. A literature review on demographic factors associated with child health behaviors was conducted to guide covariate selection for multivariable modeling.26-29 For each of the 5 composite healthy behaviors, we conducted generalized linear modeling with random intercept in which students were clustered within schools. The following were included in each modeling: sex, race, public v. non-public school, SES (low v. middle v. high), community type (urban v. suburban v. rural), perceived parental education attainment (college or higher v. others), and the corresponding perceived parental health behavior. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A 2-tailed P < 0.05 was used to indicate statistical significance.
Results
Student-Reported Demographics, Health Behaviors, and Perceived Parent Health Behaviors; PHS Students With Available Data on Both Student Health Behaviors and Perceived Parental Education and Health Behaviors (N = 4607).
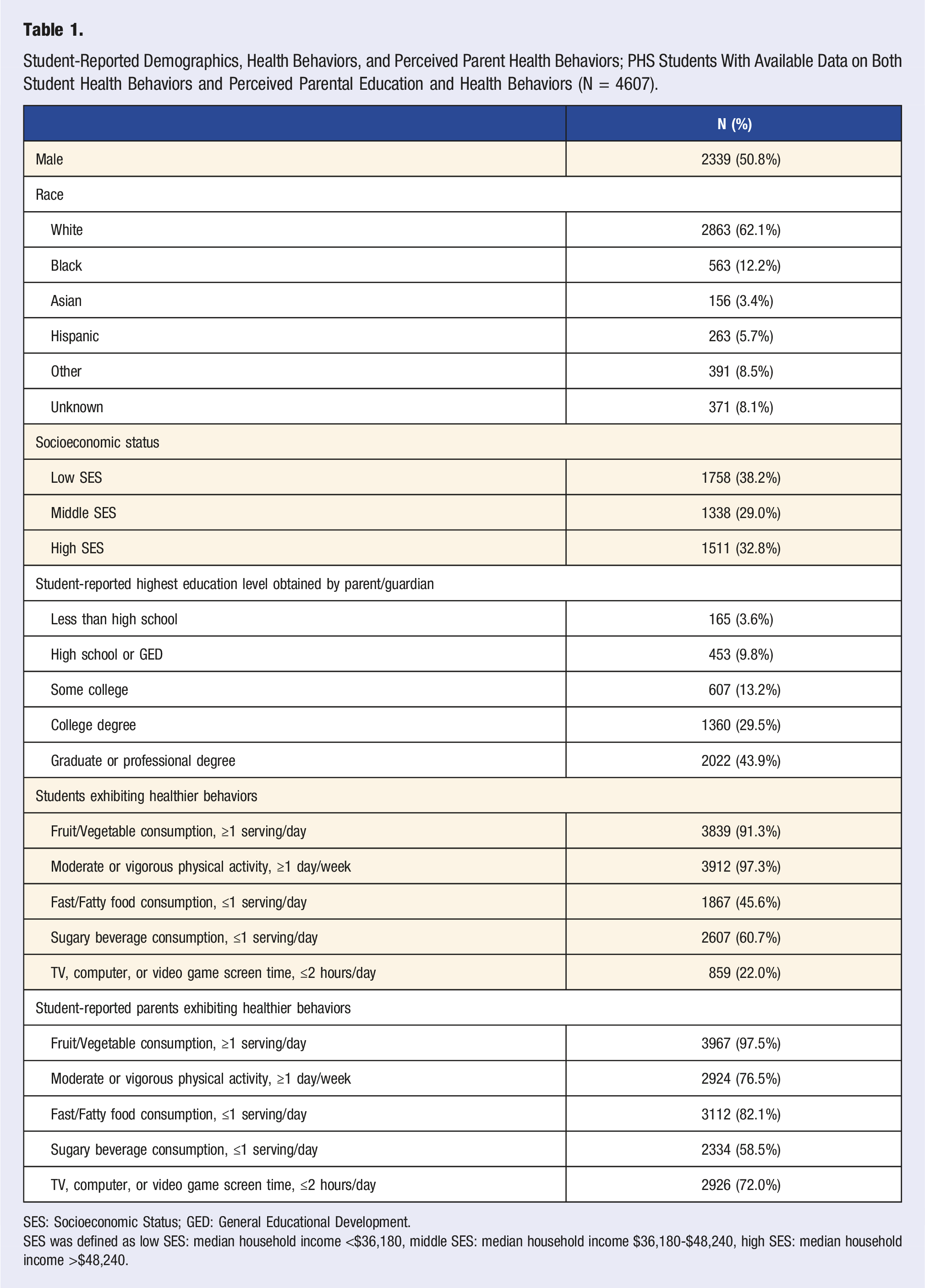
SES: Socioeconomic Status; GED: General Educational Development.
SES was defined as low SES: median household income <$36,180, middle SES: median household income $36,180-$48,240, high SES: median household income >$48,240.
While most students reported “healthier” behaviors for fruit and vegetable consumption (≥1 time/day eating fruits or vegetables) (91.3%), sugary beverage consumption (≤1 time/day drinking sugary beverages) (60.7%), and physical activity (≥1 day/week vigorous [for 20 minutes or more] or moderate [for 30 minutes or more] physical activity) (97.3%), only 45.6% and 22.0% reported healthier behaviors for fast and fatty food consumption (≤1 time/day eating fast or fatty foods) and screen time behaviors (≤2 hours/day of TV, computer, or video game screen time), respectively (Table 1).
Student-Reported Perceived Parent Behaviors in Congruent Categories for Children Reporting Healthier Behaviors.
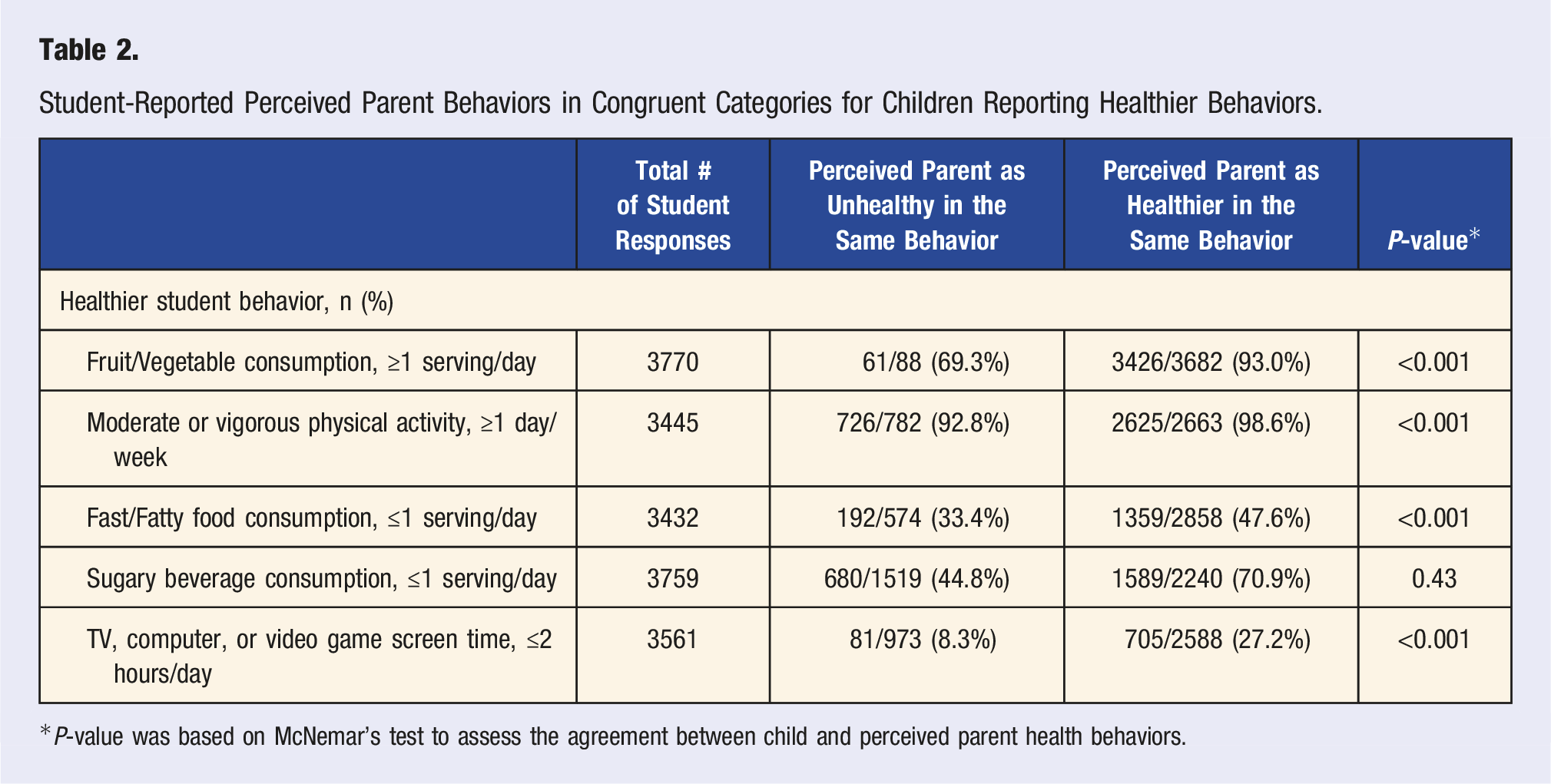
*P-value was based on McNemar’s test to assess the agreement between child and perceived parent health behaviors.
Student Healthier Behaviors by Parental Education Level (N = 4607).
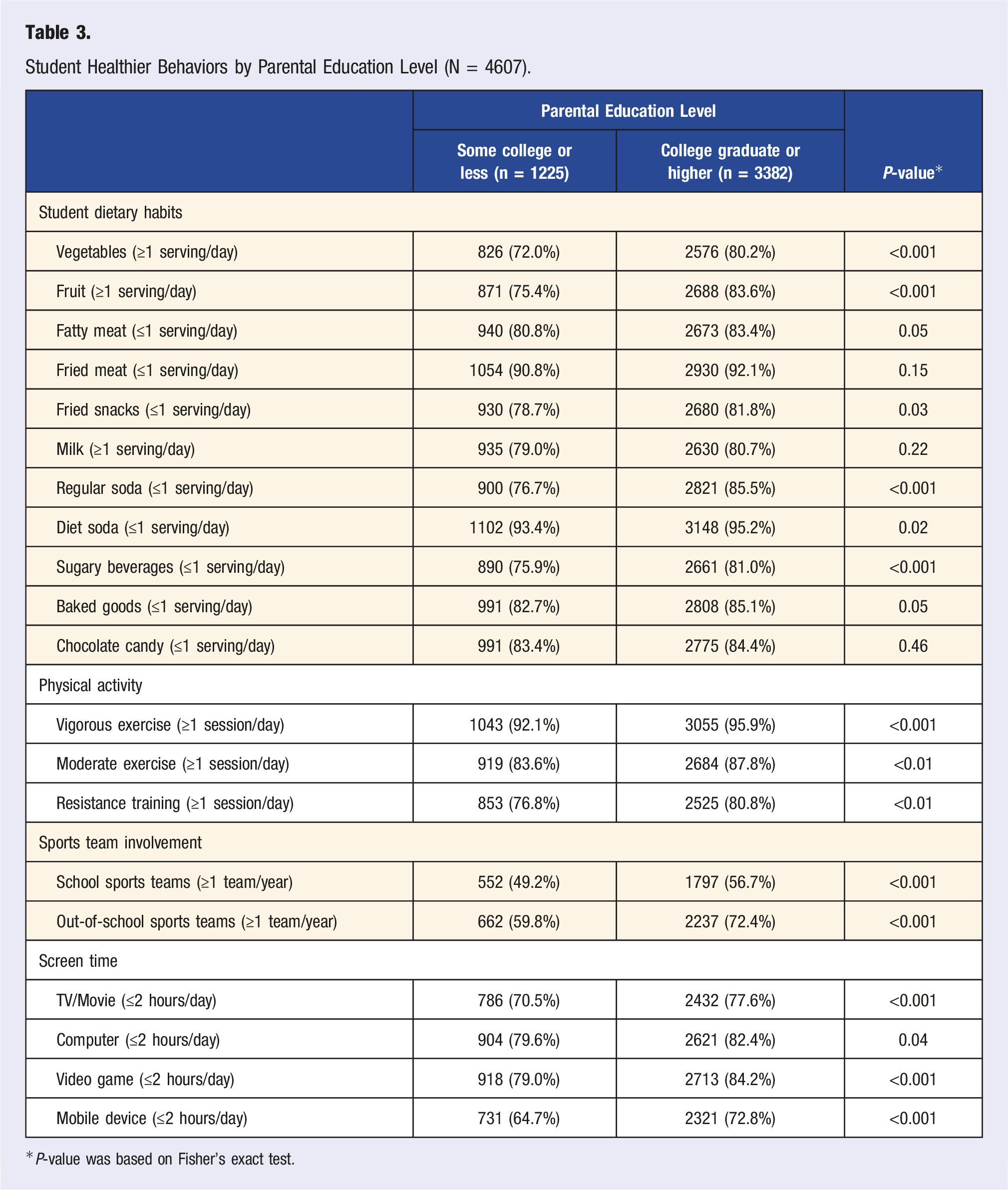
*P-value was based on Fisher’s exact test.
Multivariable modeling was used to assess factors associated with each of the 5 healthier student behaviors. One of these models, for the healthier screen time behavior (≤2 hours/day of TV, computer, or video game screen time), is shown in Figure 1. Odds ratios for all covariates were similar in magnitude and direction for all 5 health behaviors. Female sex was positively associated with healthier (i.e., lower intake of) sugary beverage consumption and screen time behaviors. To examine if student’s sex modified the association of perceived parent behaviors and parent education with student behaviors, we added into the model two interaction terms of sex with one of the two factors. For all five models, the association of parent healthier behavior with student healthier behavior did not vary by the students’ sex. However, the association of student healthier behaviors with parent education level differed by sex in both the physical activity and fast/fatty food consumption models, with female students more likely to exhibit the healthier behaviors if they reported a higher parental education level. Self-reported Black race was associated with unhealthy behavior for fast/fatty food and sugary beverage consumption. Compared to self-reported White students, self-reported Black students were also less likely to demonstrate healthy screen time behaviors (P < 0.001). This unfavorable screen time behavior was consistently observed across all SES groups among Black students (P = 0.029) (Supplementary Table 2). The same finding was observed among Hispanic students only in the middle SES group, compared to White students in the middle SES group (P = 0.029). Higher parental education level, as reported by the children, was associated with healthier behaviors in fruit/vegetable consumption, physical activity, and screen time. Student-reported factors associated with student healthier behavior: screen time (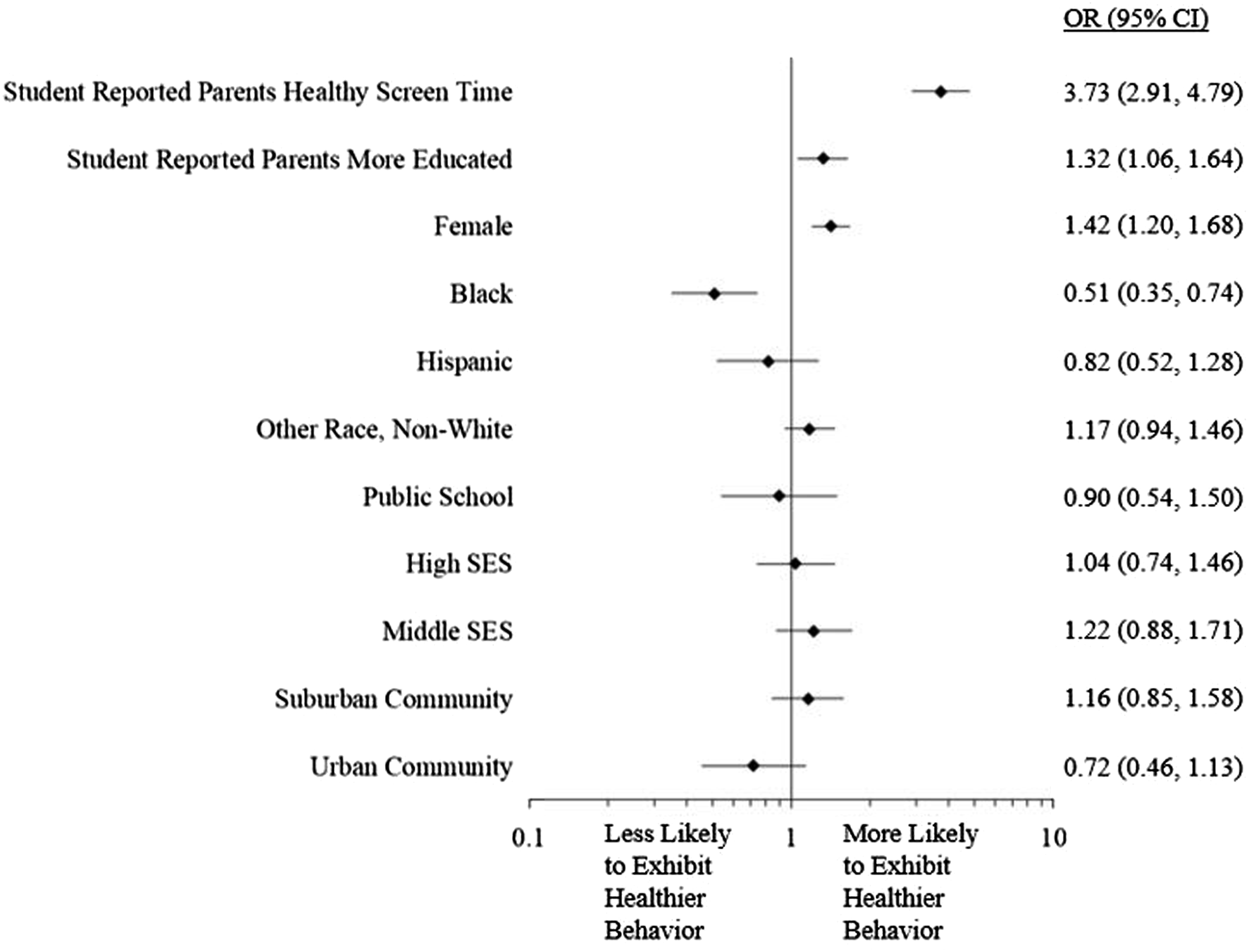
For all health behavior categories, parents exhibiting the healthier behavior (as reported by the student) was significantly associated with students displaying the healthier behavior. For example, parents exhibiting healthier screen time behaviors was associated with students displaying healthier screen time behaviors (Figure 2). Student-reported perceived parent healthier behaviors associated with student healthier behaviors. OR: odds ratio; CI: confidence interval. Odds ratio for each student-reported perceived parent health behavior was based on generalized linear modeling with student healthier behavior as the dependent variable and the following covariates included: race, gender, socioeconomic status, school type, community type, and student-reported parental education level. Healthier behaviors were defined as follows: Fruits/Vegetables (≥1 time/day eating fruits or vegetables); Physical activity (≥1 day/week vigorous [for 20 minutes or more] or moderate [for 30 minutes or more] physical activity); fast/fatty foods (≤1 time/day eating fast or fatty foods); sugary beverages (≤1 time/day drinking sugary beverages); screen time (≤2 hours/day of TV, computer, or video game screen time).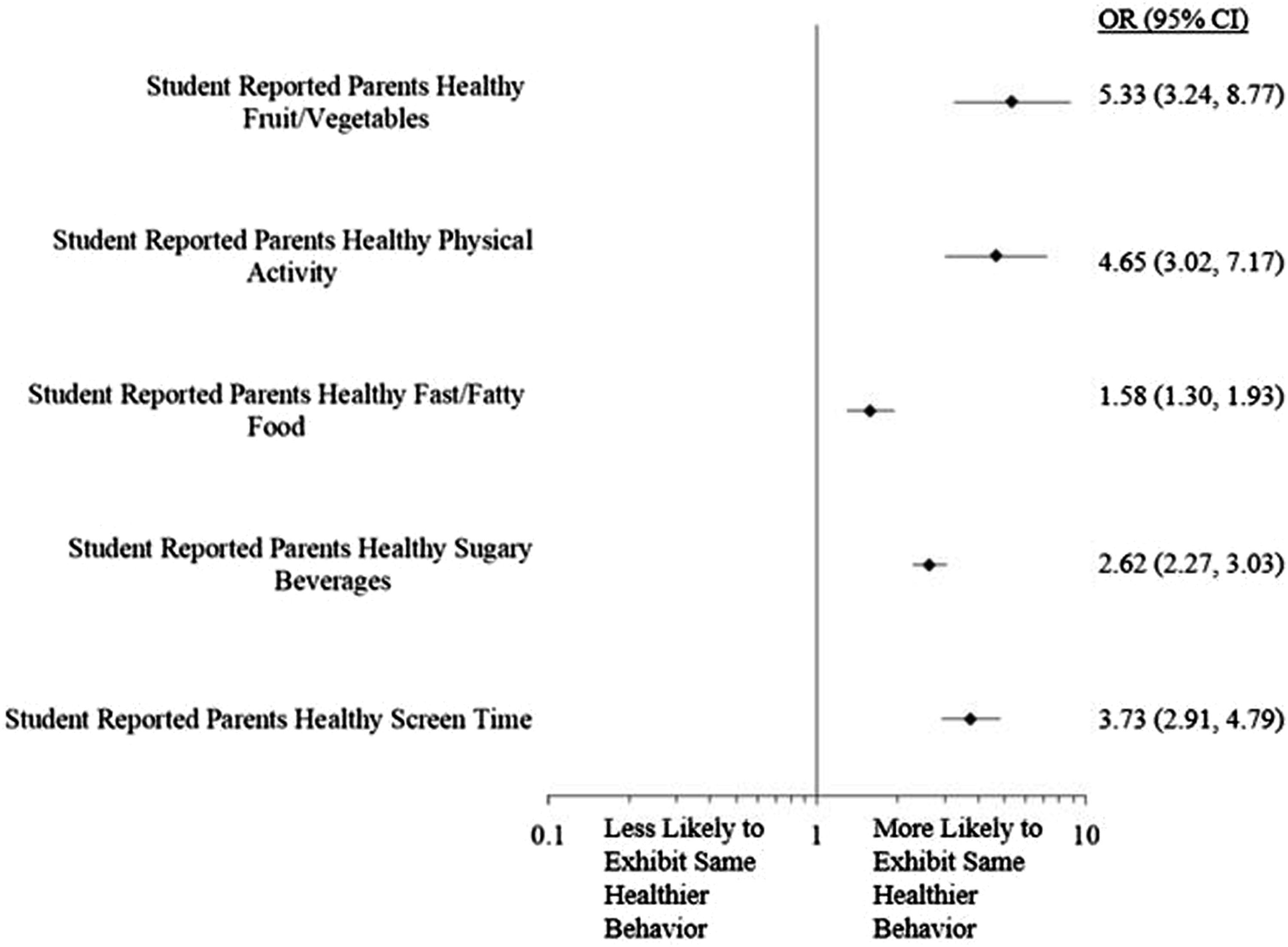
Discussion
Among PHS participants, we observed that middle-school students who reported parental healthy behaviors were more likely to report having healthy behaviors themselves. This study also found associations between higher levels of child-reported parental education and healthier behaviors in children.
Parents play a significant role in shaping the environment and resources made available to their children. The types of food that parents make available to their children, the dietary and physical activity examples set by parents, and parental beliefs about health and nutrition can all influence a child’s health-related behaviors.7-9,30 However, parental influence on children changes as children age. Adolescence offers unique opportunities for child independence, including physical activity and food choices at school. Therefore, middle schools are critical sites for fostering either the maintenance of healthy habits established at home or the development of new healthy habits.
It is important to note that less than half of the middle-school-aged children in this study reported ≤1 time/day eating fast or fatty foods (45.6%) or ≤2 hours/day of screen time (22%). This is in line with previous studies. Atkin and colleagues demonstrated in a meta-analysis that, across all studies examined, greater than two-thirds of children reported more than 2 hours of screen time per day. Additionally, some studies included in the meta-analysis reported up to 78.7% of children following this trend. 31 Certain interventions, such as setting clear rules for screen time by parents, have been shown to effectively cut down on children’s screen time. 32 This highlights the importance of empowering parents and caregivers to understand and promote healthy habits regarding screens. Increased screen time and increased fast-food consumption may be linked, with increased TV time and exposure to fast-food advertisements correlated to higher rates of fast-food consumption. 33 Further contributing to an increase in fast-food and unhealthy snack consumption, children often display a preference for unhealthier food options over healthier ones.34-36 Fortunately, rates of unhealthy food choices have been shown to be lower when parents model healthy behaviors and set rules and expectations about healthy eating.37,38
Healthier dietary, physical activity, and sedentary habits were reported in students when the students’ reported parental education at the college graduate or higher level compared to students who reported their parents’ educational attainment as some college or less. Additionally, higher child-reported parental education was positively associated with healthy fruit and vegetable consumption, physical activity, and screen time. Prior research has had similar findings, associating parental education level with the dietary and sedentary habits of their children.39-41 Many factors may contribute to these findings. For example, higher parental education may indicate higher income, allowing better access to proper nutrition and other health care resources. Higher parental education may also indicate increased knowledge and exposure to health education. Other studies support the association between education level and healthier choices among adults, including preventive and risk-control measures (e.g., health screenings and flu vaccinations), healthier dietary habits, less drug use, lower obesity prevalence, and lower probability of smoking. 14 These healthier choices are subsequently being modeled to any children in the household.
Female students reported lower consumption of sugary beverages and reduced screen time in comparison to male students. Female students also reported more “healthier behaviors” if their parents were college graduates than male students. Similar results have been previously reported,42,43 although the reason for these results remains unclear. Girls in one study were more likely to report that TV and computer screen time was “bad” or “not useful” in comparison to boys. 43 Separately, Bjelland and colleagues reported that their school-based health intervention was effective at reducing screen time and sugary beverage consumption in girls, but not boys. 44 A proposed explanation for this was the increased parental awareness noted among the parents of girls compared to the parents of boys, 44 consistent with prior studies of gender differences in parent-child communications.45-47
Furthermore, it is concerning that self-reported Black students reported more unhealthy behaviors regardless of SES levels. Increased screen time habits among Black and Hispanic students have been seen in other studies,39,48-50 sometimes regardless of household income. 48 As noted above, 33 increased screen time results in increased exposure to processed food and beverage advertisements. Black adolescents have been found to be less likely to distrust these advertisements 51 and more likely to engage with fast-food and sugary beverage brands on social media, 52 compared to their White counterparts. Other studies have also reported increased sugary beverage consumption among Black adolescents,49,53 as was seen in our study. One study found that Black adolescents perceived higher consumption of sugary beverages among their peers and saw these beverages as less unhealthy. 51
While the behavioral mechanism of these observations has not been proven, social determinants of health beyond education, including structural racism, should be examined. Racism permeates American culture and has far-reaching effects; it is highlighted by some as a driving force for many other social determinants of health (e.g., socioeconomic status, access to health resources, neighborhood environments). 54 For example, racial and ethnic minorities are less likely to live in neighborhoods with a chain supermarket (i.e., a “food desert”), and more likely to live in a neighborhood with a high density of fast-food restaurants and “junk food” (i.e., a “food swamp”).55,56 Unsurprisingly, this built environment leads to poor dietary habits and increased prevalence of obesity.55,56
Demographics, education, and other social determinants affect health directly, and some studies have reported an impact on the effectiveness of school-based interventions.57,58 As health behaviors during adolescence often track into adulthood, 59 interventions targeting this population have the potential to improve the overall health of the community. Creative solutions are necessary to tailor interventions, like Project Healthy Schools, to reduce disparities and improve effectiveness for all children, including those who are socially disadvantaged.
The PHS program currently focuses on student health education, and this has resulted in physiological and behavioral improvements.60,61 Additional focus in this program on parental involvement and health education may have an even larger impact on students’ health.
Limitations
Project Healthy Schools is a school-based health intervention, which is non-randomized and observational in nature. It is therefore subject to inherent limitations and biases. This study did not collect data regarding intra-family dynamics, including the number of parents per household, parenting styles, or household income. Socioeconomic status was not student-specific and was instead assigned to all students within a school, greatly limiting our ability to draw conclusions based on SES.
Parental education and habits were based on student reporting, and these measures were not psychometrically validated, a major limitation. Students may have misrepresented their parents’ health behaviors, especially considering survey questions did not specify which parent(s) should be included in the reporting. Students may have over- or under-estimated their parents’ education or misunderstood the questions or response variables. A high percentage of students reported parents with “college graduate or higher” education, which may reduce the generalizability of the study, as 2021 census data suggests less than 40% of United States residents over the age of 25 are college graduates. 62 Further limiting the generalizability of the study, nearly two-thirds (62.1%) of the study population was White. Additionally, the use of a health behavior survey lends itself to potential reporting and recall biases of the students’ own health behaviors.
Conclusions
Parents play a critical role in their children’s health. In our study, perceived parental education levels and health behaviors were correlated with children’s health behaviors. We hope, with lessons learned from this study, to increase parental involvement in PHS. As we continue to understand how adolescent behavior is shaped, we can increase the effectiveness of targeted health education for parents and children alike.
Supplemental Material
Supplemental Material - Associations Between Perceived Parental and Michigan Middle-School Students' Lifestyle Characteristics
Supplemental Material for Associations Between Perceived Parental and Michigan Middle-School Students' Lifestyle Characteristics by Ryan Rogers, Kayla Marcotte, Rachel Krallman, Chih-Wen Pai, Daniel Montgomery, Jean DuRussel-Weston, Eva Kline-Rogers, Kim A. Eagle and Elizabeth A. Jackson in American Journal of Lifestyle Medicine.
Supplemental Material
Supplemental Material - Associations Between Perceived Parental and Michigan Middle-School Students' Lifestyle Characteristics
Supplemental Material for Associations Between Perceived Parental and Michigan Middle-School Students' Lifestyle Characteristics by Ryan Rogers, Kayla Marcotte, Rachel Krallman, Chih-Wen Pai, Daniel Montgomery, Jean DuRussel-Weston, Eva Kline-Rogers, Kim A. Eagle and Elizabeth A. Jackson in American Journal of Lifestyle Medicine.
Footnotes
Acknowledgments
Since its inception in 2004, Project Healthy Schools’ (PHS) wellness efforts have been generously supported by a multitude of individuals, foundations, corporations, and health systems. PHS is grateful to these organizations and individuals; their partnership has played a significant role in the remarkable success of the program.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Jackson reports research funding from NIH and Amgen; editorial board membership: Circulation: Cardiovascular Quality and Outcomes; consulting: American College of Cardiology and McKesson, Inc.; Expert witness for DeBlase Brown Everly LLP.; and royalties for UpToDate. The remaining authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
This study underwent full board review and obtained approval by the sponsoring Institutional Review Board.
Disclosure
The remaining authors have nothing to disclose.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.