
Abstract
Child lifestyle behaviors are influenced by their caregivers. Targeting the caregiver–child relationship can establish healthy habits, especially healthful eating patterns, in both the caregiver and child. The purpose of this study was to identify the context for addressing strategies used to establish nutritious eating for the caregiver and child taken together as a unit (e.g., the caregiver–child dyad), through the perspectives of nutrition-promoting professionals. We performed purposive sampling of professionals who address healthful nutrition. Semi-structured qualitative interviews were conducted to elicit perspectives on caregiver–child eating dynamics and techniques to produce dietary behavior change. Data were coded through the constant comparative method, and subthemes and themes were identified by grouping similar codes and excerpts. We identified four themes relevant to dyadic dietary behavior change: (1) factors to consider when approaching nutrition such as family dynamics, (2) dyad-specific strategies for dietary behavior change, (3) patient-centered approaches professionals implement in interactions with the dyad, and (4) time as a barrier to dietary behavior change. In conclusion, study is novel in eliciting the perspectives of professionals across multiple settings to provide a context for dyadic dietary behavior change. Future studies can focus on developing training for lifestyle medicine professionals to approach dyad-specific behavior modification.
“Our findings could be applicable to broader considerations in lifestyle behavior change science with intergenerational health implications.”
Background
Behavioral modification is a key intervention to achieve any and all pillars of lifestyle medicine. Lifestyle medicine aligns with the American Heart Association framework for optimal cardiovascular health, which states that the first-line strategy to prevent morbidity and mortality is a modification of lifestyle habits, with one of the main pillars of both models being dietary modification toward a vegetable-forward, plant-based diet.1,2 According to the American College of Lifestyle Medicine and the American Heart Association guidelines, a healthy diet is composed of primarily fruits and vegetables, fiber-rich whole grains, nuts and legumes, and limited animal products, sodium, and sugary beverages.1,2 However, it has been shown that up to 90% of children in the United States do not meet healthy eating guidelines. 3
Child eating behaviors are influenced by a multitude of individual, sociocultural, and environmental factors. 4 One of the most crucial pillars of lifestyle medicine and lifestyle behavior change is social connection and relationships. 5 The most influential relationship in a child’s life may be their parent or caregiver, especially when it comes to lifestyle behaviors. For example, numerous studies have established the bidirectional influences between caregiver and child when it comes to eating behaviors, considering the influence of parental food preferences and attitudes toward nutrition and feeding.6-9 One study found that within parent–adolescent dyads, autonomous motivation for health behaviors and fruit and vegetable intake were interdependent and positively correlated. 6 However, another study also demonstrated that the relationship between parent and adolescent eating patterns, including fruit and vegetable consumption, was contextualized and influenced by social, family, and neighborhood-level factors. 9 Parental support has been linked to improvements in children’s dietary habits, and interventions to improve children’s diets often involve parents.3,7 Improving the caregiver and child’s diet simultaneously when establishing healthy eating is important, as parental support enhances healthy eating behaviors, and childhood behaviors track to adulthood. Many professionals seek to promote healthy eating in the dyad, including health care professionals like nutritionists and pediatricians, but also community-based professionals like childcare directors and WIC coordinators.
Multiple studies independently assess child and adult interventions to achieve healthy eating; however, few are targeted at this powerful family unit combined.10-12 Furthermore, studies tend to focus on specific interventions carried out by the dyad, while none have elicited perspectives and experiences from nutrition-promoting professionals who play a role in fostering this behavior change. Limited data exist to inform providers on techniques they can employ to specifically target the caregiver–child dyad relationship to achieve healthy eating in both, despite evidence that improving provider delivery of behavioral interventions leads to better health outcomes. 13 As such, our research question is: What techniques and considerations do nutrition-promoting professionals employ to encourage dietary behavior change in the caregiver–child dyad? We take a unique approach to elicit perspectives from professionals themselves and utilize qualitative analysis to create a thematic understanding of various strategies professionals use to establish dyadic nutritious eating.
Purpose
The purpose of this study is to identify the context for addressing and strategies used to establish nutritious eating for the caregiver–child dyad through the perspectives of nutrition-promoting professionals. In doing so, this study provides a foundational understanding of these seldom-explored topics to generate new questions, hypotheses, and interventions to promote dyadic dietary behavior change.
Methods
Study Design
We performed a qualitative study using semi-structured interviews of nutrition-promoting professionals who work with caregiver–child dyads in low-income families. This study design was utilized to gain a detailed thematic understanding of professionals’ experiences and perspectives related to our research question.
Sampling and Recruitment
We used purposive sampling to recruit nutrition-promoting professionals across clinic and community-based settings. Nutrition-promoting professionals were defined as those who (1) work professionally in a health care or community (e.g., childcare, education) setting, and (2) encourage nutritious eating and dietary behavior change among caregivers and children on a daily basis. Inclusion criteria were: English-speaking, professionals or caregivers working with children directly or indirectly (e.g., with families), background in nutrition, and NYU Langone Health employee or affiliate. Examples include: health care providers who were dieticians or clinicians who practice in primary care, for example, where nutrition is regularly addressed in clinical encounters; childcare professionals who adhere to national standards and guidelines while providing daily meals and related nutrition education to children with the regular involvement of their families; or professionals who work with families in community programs like Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Recruitment occurred through professional networks of investigators, NYU Langone Health listservs, and word-of-mouth. Participants provided verbal informed consent for an audiotaped virtual interview. Participants were compensated with a US$25 gift card. This study was ethically reviewed and considered exempt by the NYU Langone Health Institutional Review Board.
Interview Procedure
The interview guide was created by a multidisciplinary team of investigators specializing in obesity and caregiver–child dynamics. Interview questions were related to the participant’s background and work, perspectives on caregiver–child dynamics associated with dietary behavior, and techniques to elicit dietary behavior change. Three interviewers conducted interviews from 7/2022 – 4/2023 until thematic saturation was reached.
Data Analysis
Audiotaped recordings were professionally transcribed verbatim. We used descriptive statistics to characterize the sociodemographic composition of our sample. Two researchers trained in qualitative research including constant comparative methods performed first-pass coding of manuscripts independently, focusing broadly on techniques for dietary behavior change employed by professionals to develop a preliminary codebook. A codebook of common first-pass codes between the two researchers was defined and labeled with code types. The two researchers then performed second-pass coding independently using both the first-pass codebook as well as codes informed by relevant literature and techniques specifically targeting dyadic dietary behavior change. The constant comparative method was used to identify and iteratively refine codes to devise a second-pass codebook, which was refined until independent coding consistently met >80% inter-reporter reliability, meaning that >80% of excerpts were labeled by the two researchers with the same codes. Once inter-reporter reliability was achieved, finalized coding was performed by the two researchers in Dedoose (version 8.3.35). The researchers then met frequently to identify subthemes and themes that emerged from patterns observed by grouping similar codes and excerpts.
Results
Study Demographics
Participant Characteristics.
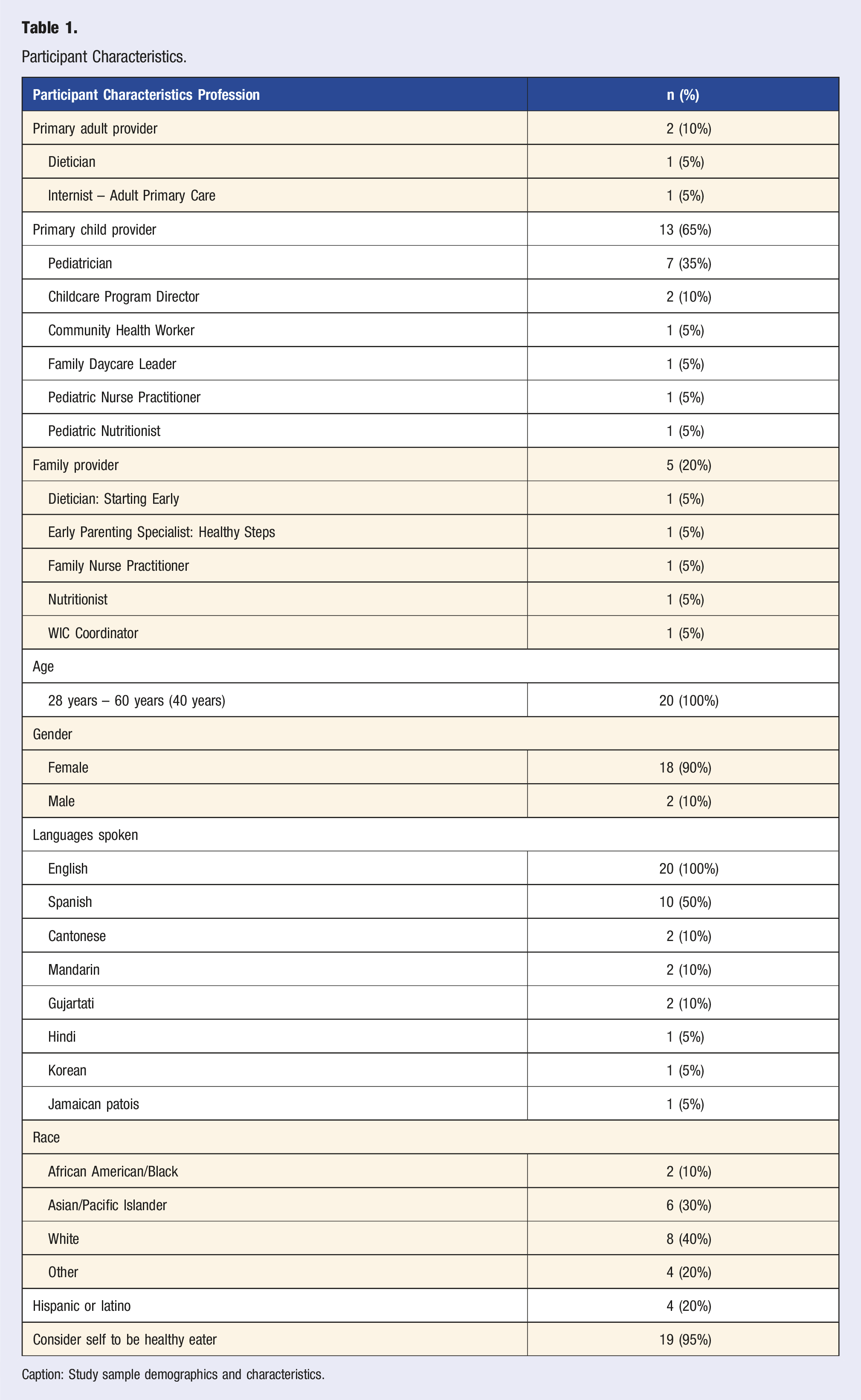
Caption: Study sample demographics and characteristics.
Themes
Themes.
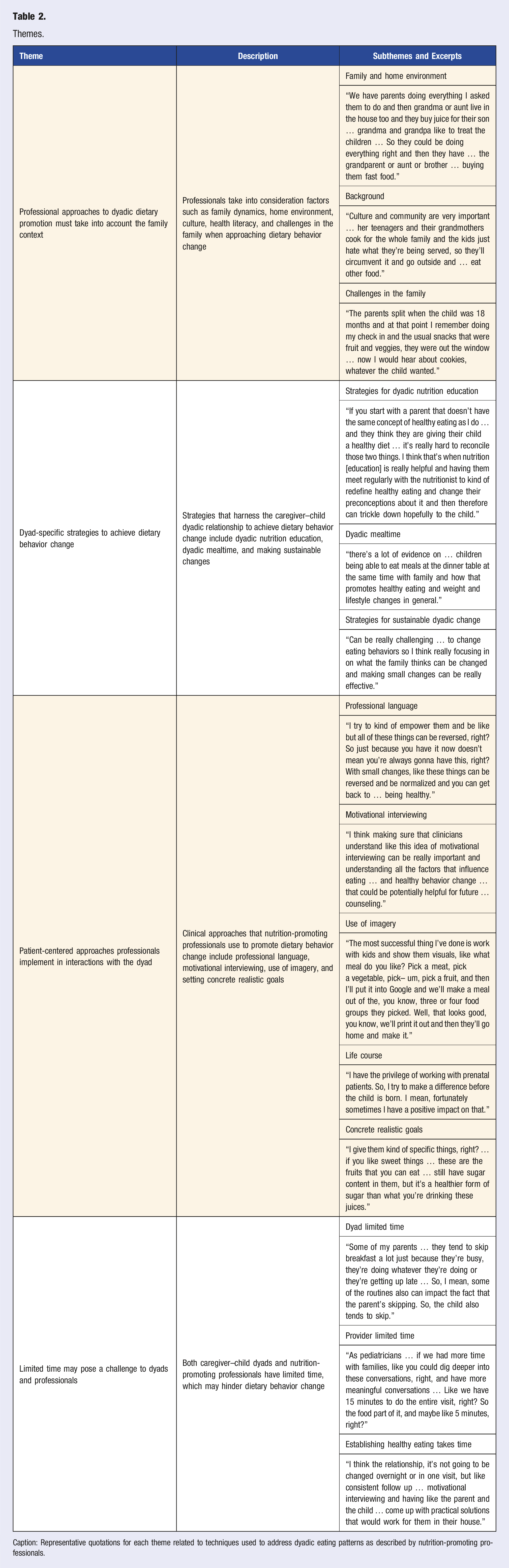
Caption: Representative quotations for each theme related to techniques used to address dyadic eating patterns as described by nutrition-promoting professionals.
Theme 1: Professional Approaches to Dyadic Dietary Promotion Must Take Into Account the Family Context
Nearly all professionals discussed factors that should be taken into consideration when approaching dietary behavior change, such as family dynamics, culture, health literacy, and challenges in the family. Home environment was often explored by professionals in relation to eating behaviors, which is shaped by family dynamics/structure and caregiver feeding behavior. One participant noted the relevance of this consideration to eating patterns, stating that “family dynamics … play a huge role. So who's home for dinner? Is it traditional in the family to have family dinners together?” (Pediatrician). In addition to family eating habits, such as consuming meals together, the family structure must be considered as it impacts who fills a caregiver role. Especially in “families [living in] multigenerational homes … [there is] influence of older caregivers and what they might think is best” (Pediatrician).
Professionals also discussed that the background of the family, including aspects like culture and health literacy, may impact eating patterns. One participant stated that culture influences the type of food caregivers cook and children eat, with Americans tending to eat more fast food: Parents that are … from the Caribbean or … from another country and they're used to cooking food and eating certain types of food. That's exactly what their children eat from young. But … parents that maybe were just brought up here in America it’s a lot of fast food or McDonald's. (Childcare Program Director)
Similarly, another participant raised the consideration of health literacy, defined as the ability to obtain and understand healthcare information to make informed medical decisions and abide by treatments, in relation to dietary change. They stated that “in the US health literacy is kind of defined to a very American population and sometimes that can mean different things for different cultures,” suggesting that patients have varying familiarity with what a healthy diet entails and how to adhere to one based on their health literacy (Pediatrician).
Finally, professionals often mentioned that they explore challenges in the family, which can impact the dyadic diet. Various challenges were commonly discussed, including working parents, financial or psychosocial stressors, and immigration. These challenges must be considered because “it all works together so ignoring one part of it and looking at nutrition in isolation is unrealistic” (Nurse Practitioner). One participant stated that “if something is going on in the family, it will impact the child, it will impact the diet, absolutely … financial, stress, any other factors will impact how they're eating” (Dietician). The specific challenge of being a new immigrant family was discussed by a pediatrician, who recognized that in these families “there's just an underlying … level of stress that affects every decision that they make” (Pediatrician).
Theme 2: Dyad-Specific Strategies to Achieve Dietary Behavior Change
Professionals discussed strategies that specifically harness the caregiver–child dyadic relationship to achieve dietary behavior change. These strategies involve education of both individuals within the dyad surrounding nutrition, engaging the dyad in preparing and eating meals together, and encouraging sustainable changes for the dyad. Education of the dyad consists of sharing information about what healthy eating entails. One nutritionist stated that nutrition education of the caregiver is important because it affects the dyadic diet as a whole, since “what we eat is what we're feeding our children … so, if I can have an impact … on the parent, then I know that I've been successful because the parent can understand, okay, so what I'm eating is very important for my child” (Nutritionist). Furthermore, when counseling each member of the dyad, professionals brought up specific considerations. For the caregiver, one professional described that nutrition education should be tailored to their current eating patterns with tangible recommendations for improvement. An example of a specific education point would be “having them build that awareness … oh, I actually need … maximum one teaspoon would be enough salt” (WIC Coordinator). In contrast, education of the child may focus more on why healthy eating is important for their well-being in general. A dietician stated that child education should be about “letting kids know why foods are helpful … for their growth or why nutrients are needed and … giving them knowledge to make healthy choices” (Dietician).
Another commonly discussed topic was strategies to engage the caregiver–child dyad in meal-related activities including grocery shopping, meal preparation, and family dinners. One pediatrician recommended dyads go grocery shopping interactively, suggesting that “maybe every time you go to the grocery store, your mom or dad will let you pick … one fruit or one vegetable that you’re going to try” (Pediatrician). Following grocery shopping, they recommended dyads cook healthy meals together at home, getting the children “involved in what the food looks like and how it's prepared” (Pediatrician).
Another method to engage the dyad in healthy eating is encouraging family dinner. A pediatrician described the various benefits of family dinner, such as caregivers modeling healthy eating behaviors, dyadic bonding time, and nutritious home-cooked meals: When you are able to eat together and sit down together, you can model behavior for your child … or just having it as a time to relax and a bonding time as well, it's cognitive and benefit to the children … and I think when they're eating on the go … you're also more likely to grab faster food that tends to be less healthy than when you sit down like a home cooked meal. (Pediatrician)
Finally, professionals touched on ways the dyad could not only implement dietary changes, but ensure they are sustainable. They emphasized strategies like enforcing dietary changes for the entire family, working as a team with the dyad, and making nutrition a priority and a habit. One pediatrician described that making family-wide changes is often beneficial in that “it's much easier to adhere to diet if everybody in the family is doing it at the same time and it's just what the family meal is” (Pediatrician). To encourage these sustainable changes, one participant recommended that professionals work as a team with the dyad, “[engaging] with the parent and other family” (Nutritionist). Another method to create sustainable change is to refrain from calling healthy eating a diet, and rather to encourage life-long habits. A pediatrician described telling families, “this is how you're going to eat going forward … these are habits that you're going to build now … that will carry you the rest of your life” (Pediatrician).
Theme 3: Patient-Centered Approaches Professionals Implement in Interactions with the Dyad
Apart from strategies the dyad may utilize, professionals also brought up patient-centered clinical approaches they implement in their own interactions with the dyad to encourage behavior change. Professionals discussed various approaches, such as using professional language, motivational interviewing, interactive visuals, harnessing caregiver motivation, and setting concrete realistic goals. They recommended the use of encouraging language to reinforce positive dietary change, “talking about what changed … what have we been doing differently and … encouraging more of it” (Pediatrician). Another technique that professionals frequently mentioned is the use of motivational interviewing to understand the patient and work with them. One participant described the open-ended questions they use to get to know a family: “it's run kind of by them. Like what do you want to talk about today? … What are the barriers to your child eating healthy? So I'll kind of include both of them in that talk … So I'll ask a lot of open ended questions to get them involved in the conversation” (Nutritionist).
Professionals recommended the use of eye-catching visuals and interactive models when working with children in particular, such as “food models … visual aids … posters … [and] games also that the little ones can play with, like puzzles” (Nutritionist). With caregivers, professionals advised harnessing motivation to establish life-long changes and set an example for their child, especially during pregnancy and early childhood. One participant stated that “starting [dietary behavior change] earlier … in pregnancy or early childhood is really important because that’s really a time when people are very motivated to make change and can be a really good time to … start instilling these kind of healthier eating habits” (Dietician).
Professionals also discussed methods to help dyads begin implementing recommended changes, such as providing concrete modifications, planning interactively, and setting realistic goals. They advised making specific recommendations tailored to the patient’s original diet. One participant shared an example: “you can still eat a piece of pizza, but you should eat protein and salad with it and walk. And it's not as bad then as eating like three pieces [of] pizza” (Diabetes Educator). Similarly, a nutritionist recommended that when providing these recommendations, one should “work [to] individualize every situation … to work with each family with the resources that they have and with their food preferences” (Nutritionist). Professionals advised that goals be realistic and incremental to make gradual progress. One pediatrician emphasized that it is “important to set realistic goals, because … if you are able to meet one small goal, then it motivates the family, and then you [can] continue to make a little progress, and so on” (Pediatrician). Furthermore, these goals and actions should ideally be patient-driven. Providers can ask patients to “[pick] three SMART goals that are practical and achievable … if they come up with it themselves then … it's more likely to be something that we can practically do” (Pediatrician).
Theme 4: Limited Time May Pose a Challenge to Dyads and Professionals
While professionals discussed many strategies to promote dyadic dietary behavior change, they also brought up factors that make this difficult to achieve. One challenge to both dyads and professionals is limited time, as establishing nutritious eating habits often requires multiple attempts by the dyad and extensive follow-up by professionals. Professionals brought up that limited time is frequently a concern of the dyad hindering healthy eating. For example, one pediatrician described that after a busy work day, caregivers are more likely to rely on fast food to feed their children: The amount of time and energy that the family has after a long work day really affects what … the family eats as a whole … If your dad is … working 12-hour days … just to get by and McDonald's on the way home, right off beside the subway stop … that's what you're getting. (Pediatrician)
Professionals themselves are also limited by time. Short appointment times hinder nutrition counseling, as providers “try [their] best to talk about these things, but a lot of times, because [they] have limited time within the visit [they’re] not able to delve in that much” (Pediatrician). Finally, professionals described that “bringing the family back for follow-up sessions … takes time” (Nutritionist).
Discussion
We conducted interviews with twenty nutrition-promoting professionals to elicit their experiences and perspectives relating to techniques to promote dyadic dietary behavior change. Our findings could be applicable to broader considerations in lifestyle behavior change science with intergenerational health implications. Through an analysis of participant interviews, we identified four themes: Professionals’ consideration of the family context when approaching dietary behavior change, dyad-specific strategies to achieve dietary behavior change, patient-centered approaches professionals implement in interactions with the dyad, and the challenge that limited time may pose to dyads and professionals. This study is novel in eliciting the perspectives of professionals across multiple settings, providing a multidisciplinary viewpoint of the common dietary behavior change strategies used when working with the caregiver–child dyad. While previous studies have utilized a qualitative approach to elicit provider expertise on nutrition behavior change strategies separately in adults and children, our study was the first to explore professionals’ perspectives on the caregiver and child taken together.14,15 Furthermore, our study population was comprised of a variety of professionals, including those not typically considered experts in nutrition such as childcare providers and WIC coordinators.
Theme 1 explored the family context that professionals take into consideration when approaching dietary behavior change. Professionals mentioned family dynamics, caregivers and their feeding behaviors, and challenges in the family as factors they consider, rather than viewing nutrition in isolation. This information builds on prior studies showing that child eating behavior is determined by a multitude of factors, including individual, familial, sociocultural, and environmental.4,10,16,17 In particular, one review paper investigates the childhood food environment within community, school, and recreational settings, noting that in the home context, parental support and activities that encourage children to eat nutritiously could prevent childhood obesity. 10 Regarding home context and family influence specifically, one study demonstrated that adolescent fruit and vegetable intake, as well as fast-food consumption, was significantly predicted by their parent’s intake levels and frequency of family meals. 9
Theme 2 encompassed dyad-specific strategies to achieve healthy eating. Multiple studies have shown that the dyadic family unit is a powerful target for behavior change.6-8,18 Focusing on the family, including caregiver/parent–child relationship, rather than any one individual in isolation, is particularly impactful as greater social ties and connectedness amongst the family relate to improvements in BMI, diabetes, cardiovascular disease, and psychological health, amongst others, in both children and adults.5,19 For example, one review paper found that the quality of relationships between parents and young children impacts obesity risk, and recommended targeting the caregiver–child dyad as a component of obesity prevention. 7 While studies have established the importance of targeting the dyad for behavior change, the present study elicits provider perspectives and approaches to implement this in practice. Findings from this study suggest that dyadic nutrition education and a focus on dyadic mealtimes are areas for future work. These recommendations promote caregiver–child interaction and connectedness with regard to healthy eating and may lead to a bidirectional effect impacting both the caregiver and child’s overall health and well-being.
Theme 3 highlighted patient-centered clinical approaches professionals use to promote behavior change. Many approaches discussed by participants in our study were known effective techniques for behavior change such as motivational interviewing and the use of imagery. When discussing goal setting, participants described approaches in line with the SMART criteria [Specific, Measurable, Achievable, Realistic, and Timed-Based] to establish behavior change. 20 However, professionals’ tendency to focus on using established approaches for individual-level behavior change may not be well-suited for dyads.
Finally, theme 4 highlighted the unique challenge to both dyads and professionals of limited time. This is consistent with the fact that professionals tend to be restricted in the amount of time they can allocate to addressing modifiable behaviors, despite these behaviors’ impact on chronic disease and overall health. 21 For the dyad, limited time can manifest as a tendency to purchase fast food for convenience after a long work day. For the provider, the amount of time that can be dedicated to nutrition counseling is limited by short appointment times.
There are several limitations of our study. First, while a diverse number of professionals were recruited and interviewed for the study including those working with adults and children, most of the participants worked primarily with children. Thus, future studies may focus more on the perspectives of professionals working with caregivers or newly formed dyads such as pregnant and postpartum patients. Second, our study was limited to professionals affiliated with NYU Langone Health, meaning that all participants work in an urban environment. As such, challenges and contexts unique to urban families may be overrepresented, such as easy access to fast food by the train home from work.
In summary, our study explored various professionals’ perspectives of and strategies to facilitate dyadic dietary behavior change. Participants discussed the importance of considering the family context when recommending dietary behavior changes to caregiver–child dyads. Strategies to establish healthy eating specific to the caregiver–child dyad were explored, including education of the dyad surrounding nutrition, and encouragement of interactive dyadic mealtime.
Implications
In clinical practice, nutrition-promoting professionals, including those practicing lifestyle medicine, may consider utilizing the dyad-specific techniques discussed in this study as well as adapting individual-level techniques to target the caregiver–child dyad as a unit when approaching dietary behavior change. Policymakers should explore the implementation of either community-based or home-based nutrition programs that promote healthy eating at the level of the caregiver–child dyad. Future research is needed to design and test novel caregiver–child dyadic nutrition and lifestyle medicine interventions and to then establish educational curricula for providers to effectively deliver them. Finally, many excerpts touched on the multitude of barriers unique to the dyad hindering healthy eating, which could be robustly characterized in a separate qualitative study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the KiDs of NYU Foundation.