
Abstract
Background: Healthy aging is defined as survival to advanced age while retaining autonomy in activities of daily living, high societal participation, and good quality of life. Sarcopenia, insomnia, cognitive impairment, and changes in sensation can be key hinderances to healthy aging, but nutritional supplements may abate their impact. As research advances, an updated review on their efficacy on age-related conditions is warranted. Results: Sarcopenia can be mitigated through proper protein intake, supplements like creatine, and in certain situations Branched-Chain Amino Acids and Vitamin D, in adults over 65. Melatonin supplementation has moderate evidence for improving sleep, while valerian root lacks evidence. Magnesium, tart cherry, and kiwifruits have shown promising impacts on sleep in limited articles. Magnesium, Vitamin D, and B vitamin supplementation have been shown to improve cognition in those with mild cognitive impairment and Alzheimer’s disease but require further study prior to recommendation. The Age-Related Eye Disease Study supplement combination is routinely recommended to reduce risk of progression to advance stages of age-related macular degeneration. Alpha-Lipoic Acid and Folate have been investigated for their roles in mitigating age-related hearing losses. Conclusions: Nutritional supplements and lifestyle changes may mitigate disabilities across multiple domains of age-related illnesses and promote healthy aging.
“Multiple recent reviews have touted whey protein and whey protein isolates as more beneficial as they lead to higher concentrations of Leucine as well.”
Introduction
As the world population continues to age, the burden of age-related disease and degenerative changes increases. 1 These conditions have a higher prevalence in older populations such as sarcopenia, insomnia, cognitive impairment, hearing loss as well as vision changes and can lead to reduced functionality and quality of life.2-4 As a result, people have become increasingly curious about lifestyle choices they can implement to extend healthspan and promote healthy aging. Healthspan is defined as the period of life spent in good health, free from chronic diseases and the disabilities from aging. 5 Fuchs et al defined healthy aging as “survival to a specific age, being free of chronic diseases, autonomy in activities of daily living, wellbeing, good quality of life, high social participation, only mild cognitive or functional impairment, and little or no disability.” 2 There is significant interest from adults regarding nutritional and dietary supplementation strategies that promote healthy aging, but widely available patient-facing content may not be vetted for evidence-based practices. There has been extensive research in this area; however, previous reviews have focused on singular issues or domains of age-related disability. A singular issue approach is not sufficient to describe the concerns associated with the aging process as there are multiple health concerns and body systems that are affected during the aging process. The goal of this paper is to detail the current level of evidence of how dietary supplements promote healthy aging from a multidomain approach and provide recommendations for supplements that promote healthy aging and mitigate risks from age-related degenerative changes.
Methods
In preparing this review, the authors aimed to critically analyze some of the most popular and commonly researched supplements for healthy aging. To accomplish this goal, the authors focused on supplements that allow for continued longevity that are related to the natural course of aging and limit performance for older adults. Therefore, the impact of supplements on critical disease states such as heart disease and cancer were not reviewed as they are remarkably vast with recent reviews that adequately explain the current level of evidence. However, excellent reviews evaluating supplements for heart disease and cancer can be found elsewhere.6,7
Other common age-related conditions of interest including sarcopenia, insomnia, cognitive impairment, macular degeneration, and presbycusis were identified as conditions that drastically impact quality of life and the healthy aging process for older adults. Reviewers [MK and SD] assessed the supplements that impacted the above conditions, focusing on the most established nutritional supplements and those with documented efficacy in humans. The search terms [Supplements Impacting (Condition) in Older Adults] for each condition were used in PubMed. MK and SD discussed the identified supplements and if there were differences between the 2 reviewers in the inclusion or exclusion of a supplement, senior author [MF] performed an independent search to determine whether inclusion or exclusion was warranted.
The supplements included in this review were defined as vitamins and compounds that are commonly used to augment nutrition drawn from the typical diet of adults. With diet and exercise relating so heavily to the impact of supplements and healthy aging, the authorship thought it was crucial to add a brief segment on protein intake and resistance training as well.
Discussion
Promoting Activity, Preventing Sarcopenia
Skeletal muscle is crucial to maintain functional ability. It is maintained through a continual balance of muscle protein synthesis (MPS) and muscle protein breakdown (MPB). 8 Beginning in the fourth decade of life MPB outweighs MPS, resulting in a loss of skeletal muscle mass and strength known as sarcopenia.8,9 The prevalence of sarcopenia varies in different demographics, but a recent study showed that 1%–29% in community-dwelling populations, 14%–33% in long-term care populations and 10% in the acute hospital-care population had sarcopenia, making it a common concern for many older adults regardless of underlying health. 3 In regards to community-dwelling populations, this study cited 4 studies that showed prevalence over 20%, 2 were performed in Italy and 2 in Japan, the remaining 11 studies had prevalence ranging of 1%–14%. 3 The reduction of muscle mass and quality with aging is closely associated with poor health outcomes like mobility impairment, disability, falls, medical comorbidities and overall decreased perceived quality of life. 8 This is a difficult problem to manage as recent studies have suggested that muscle mass decreases approximately 2% every year after the age of 50, and approximately 15% of muscle strength is lost every 10 years after the age of 50. 10 Adequate dietary protein intake and proper dietary supplementation strategies that appreciate the context of comorbidities can help combat sarcopenia and maintain physical fitness and function, particularly when combined with a resistance training regimen.
Protein Intake
Proteins are the building blocks for muscle protein synthesis as they contain the essential amino acids needed for this process. In older adults, protein consumption typically decreases with aging and trends towards 1 protein-heavier meal per day, as opposed to protein consumption at multiple meals throughout the day. 8 This issue is compounded as older adults have decreased absorption of amino acids and require higher levels of protein intake to stimulate MPS. 11
Currently, the recommended dietary allowance (RDA) for protein intake in adults to maintain nitrogen balance is .8 g/kg/day; however, this is likely insufficient for older adults. Recent studies published by the PROT-AGE study group and European Society of Clinical Nutrition and Metabolism suggest that older adults should consume 1.0-1.5 g/kg/day of protein.12,13 The National Health and Nutrition Survey of over 8000 people found that adults over the age of 60 who consumed more than 1.0 g/kg of protein per day had a 22% decreased odds for functional disability. 14 Similarly, this study also showed that consuming .25 g/kg of protein per meal decreased functional deficiencies by 40% for one meal, 52% for two meals, 53% for three meals and 61% for 4 meals. 14 Additional data has suggested that an even distribution of protein consumption across meals with a goal of .4 g/kg per meal 3-4 times per day (resulting in 1.2-1.6 g/kg/day total protein intake) maximizes MPS and supports skeletal muscle health. 8 However, caution should be exercised in patients with pre-existing kidney disease, this level of protein intake may be deleterious. 15 Additionally, a cross-sectional analysis performed in China showed that the amount of protein rather than the protein source (plant vs animal) was the factor that had greater impact on skeletal muscle mass. 16 However, a recent Journal of American Medicine Article found that while plant protein may be better for those with pre-existing risk factors such as obesity or cardiovascular disease, animal protein for those with no pre-existing risk factors decreased all-cause mortality. 17 As with any dietary, lifestyle or supplement change, patients should speak with their physician prior to making a change.
Supplementation
Dietary supplementation strategies involving creatine, vitamin D, omega-3’s and branched-chain amino acids (BCAAs) have been studied in their effects to promote muscle growth and prevent age-related degeneration of muscle tissue. These supplements can augment existing healthy dietary and exercise habits to potentiate muscle protein synthesis.
Creatine, a non-protein amino acid derivative that is naturally produced by the liver and kidneys from essential and non-essential amino acids, has been shown to increase muscle mass, strength, and function in older adults regardless of high or low dosing strategy.9,18 In men ranging in age from 50-71, .1-0.3 g/kg of creatine supplementation paired with supervised resistance training sessions for 32 weeks increased leg press by 30 kg and chest press by 14 kg compared to placebo, regardless of if creatine was ingested prior to or after exercise. 19 Additionally, a recent meta-analysis reported that older adults (age range 48-84 years) had increases in chest press, and leg press strength following creatine supplementation in a range of supplementation protocols over 7.4-52 weeks. 20 Of note within this meta-analysis, only studies where this weight-based protocol dosing lead to participants receiving at least 5g of supplementation per day showed increases in strength or lean mass. 20 These gains in strength and fitness can guard against deconditioning and muscle wasting and decrease the risk of falls, which are a significant source of morbidity in older adults.
Similar to other supplements, research shows that creatine alone without concomitant resistance training is unlikely to improve strength or functional performance. 18 There exists substantial positive evidence supporting creatine usage for older adults, however recent studies have suggested that creatine may have protumor and antitumor effects, and therefore we do not recommend creatine usage in those with cancer. 21 It was previously thought that creatine supplementation was potentially harmful to renal function based on early case reports. However, numerous controlled trials over decades have since demonstrated that creatine supplementation is not harmful to renal function at recommended doses in healthy adults and does not alter urea levels or dampen endogenous production of creatine. 18 That being said, the safety of creatine in adults with pre-existing renal disease is less clear. Isolated case reports of worsening renal function in the setting of pre-existing kidney disease and creatine supplementation exist, while other case reports do not support this, 18 and others have suggested implementing creatine supplementation in hemodialysis patients due to creatine deficiency and protein energy wasting. Due to the complexity and variation amongst renal disease, a blanket recommendation for patients with pre-existing renal disease is outside the possibility and scope of this review. Ultimately, for those with pre-existing renal disease, consultation with a nephrologist is warranted prior to initiating creatine supplementation. However, for healthy adults, a large volume of evidence supports that creatine supplementation is safe and does not cause kidney damage.
Another important supplement to consider for sarcopenia is Vitamin D. Vitamin D supplementation is reported to increase the number and cross-sectional area of type II muscle fibers, improving MPS due to skeletal muscle fiber cells’ expression of vitamin D receptors. 3 Despite this finding, vitamin D supplementation has not been shown to confer strength and influence sarcopenia outcomes once the underlying nutritional deficiency is corrected. 22 Thus, for those with a nutritional deficiency and insufficiency in vitamin D (<20-30 ng/mL), supplementation can improve functional outcomes, but there is little evidence to suggest efficacy beyond that.22,23 One review discusses that older adults with Vitamin D insufficiency (<37-45 nmol/L) experience fewer falls with supplementation, but improving falls is not solely related to increased muscle mass and could relate to bone strength and cognitive improvements as well. 24
See Brain Health Section for Additional Recommendations on Vitamin D
Similarly, omega-3 supplementation has been studied for its role in reducing inflammation and related MPB. 25 In practice however, the current literature does not support that the inflammation reduction from omega-3 supplementation is sufficient to confer functional outcomes in preventing sarcopenia. 26
See Brain Health Section for Additional Recommendations on Omega-3s
BCAAs are the most common supplement used in the United States; however, a recent review published by Plotkin et al stated that “majority of the literature fails to support BCAA supplements as ergogenic aids in the context of strength and hypertrophy.” 27 It is generally accepted that older adults who have adequate protein intake do not need BCAA supplementation. However, amongst older adults, adequate protein intake can be difficult to achieve. It appears that leucine is the rate-limiting amino acid for MPS, and older adults consuming ∼3g per meal over 12 weeks could increase lean body mass by 1.1%.28,29 Additionally, leucine is a key step in phosphorylation of the MTORC1 pathway which overall leads to increased muscle protein synthesis. 30 Other studies at lower concentrations and shorter durations of leucine supplementation have showed no benefit. 31 Leucine can be found in protein rich foods like tuna, chicken, tofu, ricotta cheese or navy beans. Leucine can also be increased through traditional protein supplementation along with whole natural foods. When considering protein supplement sources many consider choosing between Whey and Casein sources of protein. 32 Both are derivatives of cow-milk; however, they differ in their digestion time. Multiple recent reviews have touted whey protein and whey protein isolates as more beneficial as they lead to higher concentrations of Leucine as well. These reviews demonstrate that whey protein supplementation is more beneficial in promoting muscle protein synthesis in older adults with sarcopenia than casein protein.33-35 For those who adopt a pure leucine supplementation strategy, it is important to consider that leucine supplements typically have additives to make them more palatable. Additionally, it is important to consider that whole food forms of protein including whey, casein, soy, or beef protein lead to a greater anabolic response than individual amino acid supplementation strategies. 32
However, it is important to consider, especially in older adults with chronic conditions that BCAA supplementation may be more appropriate than for the general public. Additional research has shown that BCAAs at doses between 4-12g daily can be effective in the setting of certain chronic conditions such as liver disease, rheumatic conditions that are being treated with glucocorticoids, and pre-existing sarcopenia.36-38 In the studies conducted by Ko et al and Tejavath et al, participants had their nutritional status assessed either clinically by investigators or by the Mini Assessment Short Form and stated that they had adequate protein and calorie intake prior to initiating the study.37,38 The other relevant studies did not mention the underlying nutritional status of their participants prior to intervention. In these cases, the human body may be using BCAAs as an additional energy source, and BCAA supplementation may improve muscle mass and functional gains and prevent further deterioration.36,37,39 In a broader sense, when a person’s metabolic demands outweigh their calorie intake, the body will turn to proteins, including BCAAs, for energy, and in turn they cannot be used as building blocks. This highlights the importance of adequate nutrition and calorie intake for everyone, but especially for older adults. 12
Resistance Training
Although the focus of this review is on nutritional supplementation, scientific literature shows that resistance training is crucial to combatting age-related sarcopenia and therefore must be mentioned. There have been previous reviews detailing the extensive data suggesting that resistance training is the most potent non-pharmacologic stimulus for maintenance of skeletal muscle mass, strength, and physical function.8,40,41 These supplement strategies should be used in tandem with healthy lifestyle choices including resistance training. It has been proven through multiple reviews that resistance training potentiates the benefits from supplements.8,40,41 A full analysis of the impacts of exercise on aging and supplementation is outside the scope of this review. To more fully investigate the impact resistance training has on sarcopenia and how it can improve the benefit of supplements, the reviews by McKendry et al, Churchward-Venne et al, and Ahtiainen et al go into further depth.8,40,41
Healthy, Restful Sleep
Restorative sleep can be a key contributor to high quality of life, healing processes and energy. However, for up to the 48% of older adults who experience insomnia, trying to sleep is difficult and can be anxiety provoking and counterproductive. 4 Insomnia is defined by 4 clinical criteria per the International Statistical Classification of Disease and Related Health Problems, 10th revision (ICD-10) 1 : difficulty falling asleep, staying asleep or nonrestorative sleep 2 ; difficulty is present despite adequate opportunity and circumstance to sleep 3 ; this impairment is associated with daytime impairment or distress; and 4 this occurs at least 3 times per week for at least 1 month. 42 This problem is accentuated because older adults have less efficient sleep as well, leading to deficiencies in both quantity and quality of sleep. 43 In addition, in a study of over 6800 patients over 65, insomnia was linked to numerous comorbid conditions such as chronic pain, cancer, chronic obstructive pulmonary disease, cardiovascular disease and most commonly depression.44,45 A recent multicenter study highlighted that late life sleep disturbances were associated with poorer cognition after 3-11 years. 46 Nutritional supplements like melatonin, magnesium, valerian root, and tart cherry and kiwifruit have been studied for their potential benefits for healthy sleep. However, it is important to note that the American Academy of Sleep Medicine does not recommend any specific dietary supplement for the treatment of sleep onset or sleep maintenance insomnia. 47
Melatonin
Melatonin, or N-acetyl-methoxytryptamine, is an endogenous hormone produced by the pineal gland released exclusively at night and can be taken as an exogenous supplement. 48 Melatonin levels decrease with age, and older adults may be more likely to have lower levels of this hormone. 49 Melatonin supplementation is used at lower doses (.3 mg) to shift circadian rhythms, and is used at higher doses (3 mg) for sleep onset insomnia. 50 A recent systematic review of the over-the-counter sleep medications melatonin, diphenhydramine and valerian root for adults over the age of 65 analyzed mean total sleep duration, sleep latency, efficiency, number of awakenings as well as safety concerns. There were only 3 studies of melatonin meeting criteria for review in adults over 65. The authors found that melatonin had the best evidence for positive impacts on sleep, increasing sleep efficiency and nighttime awakenings, while minimizing safety concerns. 51 Interestingly, there was no significant effect on sleep latency in any of the studies analyzed. In addition, the authors noted that the studies in patients over the age of 65 were very limited in number, small in sample size, and often lacking in robust study design (lacking control groups and using subjective sleep measures such as sleep diaries). 51 Of note, the American Academy of Sleep Medicine does not recommend melatonin as a treatment for sleep onset or maintenance insomnia in adults due to low quality of available evidence. 47 Given these findings, the lowest possible effective dose of melatonin should be used in older adults (.3 to 3 mg), as higher doses carry the risk of prolongation of supraphysiologic melatonin levels through the next day. 52 Similarly, there are limited studies on the efficacy of long-term use of melatonin, and it should not be used for prolonged periods of time.
However, as with most supplements, there are significant safety concerns about the contents of melatonin supplements as they are not regulated by the FDA. One study investigating 31 melatonin supplements for quality and safety found that concentrations ranged from −83% to +478% of the labeled content, and 71% of the supplements studied did not come within a 10% margin of the labeled content. 53 In addition, 26% of these supplements contained serotonin, a natural substrate for melatonin and potent neurotransmitter, which is a controlled substance not available for purchase. 53 While third-party verification websites can be helpful, they are not comprehensive, often clarifying the stated amount contained within the supplement rather than verifying efficacy.
Magnesium
Magnesium has been shown to be a key regulator of sleep as an antagonist of N-methyl-
Valerian Root
Valerian root is a common herbal medication used to improve sleep and reduce anxiety dating back to the 18th century. 58 It is proposed that valerian root allosterically modifies GABA receptors to enhance the neurotransmitter’s sedative effects, acts as a partial serotonin agonist, and modifies adenosine receptors. 58 A current meta-analysis and systematic review of 60 studies highlighted that the current evidence is inconsistent and does not support that valerian root positively impacts sleep. Some studies have suggested that at higher dosages (1800 mg vs the recommended 300-600 mg) valerian root actually increases anxiety. 59 Furthermore, it has been reported that there are a wide variety of chemical properties in different valerian roots, and the different extraction and storage processes can impact the quality of the supplement. 58 Additionally, the active constituents of valerian root are relatively unstable, meaning that it is unclear what ingredients are present by the time it reaches the consumer. 58 The current level of evidence for its efficacy is poor; however, standardization of production and storage practices may influence its feasibility as a sleep aid in the future. 58
Natural Foods
The natural food-based supplements kiwifruit and tart cherry have early evidence to suggest possible benefit for sleep. Kiwifruit is touted to be rich in compounds that promote sleep such as antioxidants and serotonin, which is often at low concentrations for those with insomnia. 60 Tart cherries contain antioxidants, a small amount of melatonin, and tryptophan, a precursor to serotonin. 61 A study in Asia had patients ages 20-55 eat 2 kiwifruits 1 hour before bed for 4 weeks after which, sleep efficiency, sleep onset latency (which were measured using Actigraph logging and the Chinese version of the Pittsburgh Sleep Quality Index), and subjective sleep scores improved significantly. 60 However, this study is unique and the results have not yet been validated. Tart cherry has had 2 placebo-controlled crossover pilot studies where older adults ingested 240 mL of tart cherry juice twice per day, and their sleep was measured using subjective surveys, a polysomnography in accordance with blood tests.61,62 These studies showed increased concentration of melatonin, reduced inflammation and improved subjective sleep measures even after a brief 2-week treatment period.61,62 High inflammation diets, such as those containing processed foods, refined sugars and carbohydrates, as well as red meat, have been linked with insomnia as well, lending credibility to the mechanism of tart cherry. 63 Of note, studies investigating muscle strength recovery, fresh or frozen tart cherry juice was more effective than juice concentrate or powdered tart cherries. This is likely due to lower concentrations of antioxidant capacity in concentrate or processed forms as compared to natural forms, but it remains to be seen if this relationship holds for its effects on sleep. 64 However, there are certainly other ways to reduce inflammation from dietary sources, and a consultation with a registered dietician can be helpful in identifying those types of foods.
Brain Health
Age-associated cognitive decline and impairment is the chief cause of disability worldwide. 65 Cognitive impairment is defined as deficits in memory, executive decision making or ability to make decisions and complete tasks crucial to daily life. It is a spectrum of disorders ranging from mild cognitive impairment to dementia and Alzheimer’s Disease (AD). After human neurodevelopment is complete in the 4th decade of life, brain atrophy begins with variable rate and regionality. 66 Pathologic changes to the brain often occur prior to clinical symptom onset, making primary prevention a crucial aspect of increased healthspan and healthy aging. 65 Interest in the impact of diet and nutrition on cognitive decline has been growing rapidly over the past decade. Nutritional supplements such as magnesium, vitamin D, B vitamins, low inflammation diets with omega-3s and creatine may play a role in prevention of cognitive decline.
Magnesium and Vitamin D
Deficiencies of magnesium and vitamin D are common amongst adults. AD has been correlated with hypomagnesemia and decreased magnesium in brain tissues on autopsy studies. 65 Magnesium has a key role in vitamin D biosynthesis and metabolism, and vitamin D deficiency has also been linked to poor cognition.65,67 Vitamin D is believed to improve cognition by reducing inflammation and potentially by affecting telomere length. 68 In a random sub-cohort of the Reasons for Geographic and Racial Differences in Strokes (REGARDS) study, an inverse relationship between cognitive impairment and magnesium intake was found. 69 Furthermore, when hypomagnesemia (<.75 mmol/L) was corrected to an intermediate level (.75-.81 mmol/L), there was a 41% reduction in relative odds of cognitive impairment. 69 However, there have been no studies to date demonstrating that magnesium supplementation can be therapeutic or preventative in cognitive disorders. Conversely, several double-blind, randomized, placebo-controlled trials demonstrated that 12 months of 800 IU/day vitamin D supplementation improved cognitive function in those with mild cognitive impairment as well as AD.68,70 Vitamin D overall currently has more robust evidence to have a role in improving cognitive performance; however after further research, magnesium may become a viable supplement option.
B vitamins
B vitamins like B6 or B12 are commonly found supplements that are readily accessible that can also impact brain health. B vitamins can lower homocysteine levels in the blood which could plausibly lower the risk of developing AD. It is estimated that 12%–31% of AD cases can be attributed to elevated homocysteine levels. 71 It is thought that older adults are more susceptible to B12 deficiencies because of decreased absorption. Older adults produce less stomach acid production, which activates intrinsic factor, a necessary cotransporter of B12 absorption. 72 As a result, supplementation may mitigate this deficiency and possibly minimize progression to AD. A recent meta-analysis published in 2022 encompassed 95 studies, 46 175 participants, and many different formulations and concentrations of different B vitamins, primarily folate, B6 and B12. This meta-analysis showed that cognitive performance improved (demonstrated by improved Mini-Mental Status Examination scores and slowed progression of cognitive decline compared to placebo) after the 12 month mark of supplementation of folate, B6 and B12 vitamins, however no differences were seen with shorter durations. 71 For those with an established diagnosis of mild cognitive impairment (MCI) and AD however, the efficacy of B vitamins may not be as strong. A recent meta-analysis showed that there were only weak improvements in memory and no improvements in general cognition and executive function. 73 In addition, lower folate levels and higher homocysteine levels were associated with dementia, but no such correlation was seen with levels of vitamin B6 and B12. 71 Of note, a 2008 study in Journal of American Medical Association concluded that high dose supplementation of B vitamins did not slow progression of mild to moderate AD. 74 However, it is certainly plausible that B vitamins may play a role in clinical intervention in the pre-MCI and AD stages of cognitive decline.
Low Inflammation Foods: Omega-3s and the Mediterranean Diet
Inflammation is a key risk factor for cognitive decline. As such, inflammation-lowering agents such as omega-3s and the “Mediterranean diet” have been investigated for ability to slow cognitive decline. Omega-3s are comprised of the 2 fatty acids eicosapentaeoic acid (EPA) and docosahexaenoic acid (DHA) and correlate with global cognitive performance.66,75 However, the overall body of evidence for the efficacy of omega-3s for cognitive performance is mixed. While some studies have suggested that dietary omega-3s play an important role in cognitive decline prevention through fish consumption,75-78 other studies suggest that there is insufficient evidence to make that claim.65,66 The biological plausibility of this argument stems from the fact that Omega-3s consumed in the form of triglycerides or phospholipids are able to cross the blood-brain-barrier to impact local inflammation while supplement forms, typically ethyl-esters cannot. However, it is entirely possible that those who choose to eat fish may make other positive dietary or lifestyle choices that could explain the benefits.
Additional low inflammatory foods are those from the Mediterranean diet, a dietary pattern consisting of lean proteins such as fish and chicken, vegetables, berries, olive oil and nuts practiced in Mediterranean countries for centuries. 65 Studies have shown that those with the highest adherence to this diet have a 33% lower risk of developing mild cognitive impairment or AD. 79 These findings have been replicated in numerous studies in the United States and Europe.65,80-82 However, it is critical to note that many of these studies demonstrate correlation and cannot imply causation. In addition, there are other components to the Mediterranean lifestyle that may play a role including exercise and social engagement. 65
Creatine
In addition to its function in skeletal muscle, creatine is also thought to play a role in energy generation in the central nervous system and cognitive processing. 83 Creatine supplementation has thus been studied for its role in cognition, and though its benefit is controversial, some studies demonstrate a positive impact, particularly under conditions of stress such as hypoxia and sleep deprivation. 83 The concentration of creatine in brain tissue has been suggested to decrease with age, but other studies have found similar levels between healthy elderly and young individuals.83,84 Regardless, creatine has been studied for its effects on cognitive performance and in elderly individuals. 83 Evidence for its efficacy is conflicting, with some studies suggesting that creatine supplementation can improve cognition and memory, 85 and others failing to show such an effect. 86 Such studies are limited by the inability to measure creatine concentration in brain tissues. 83 Further studies on the optimal brain creatine concentration and supplement protocol need to be established before making recommendations for supplementation impact on cognitive performance.
See Promoting Activity section for safety considerations for creatine in those with pre-existing cancer or renal disease.
Hearing Loss
Age-related hearing loss (ARHL) or presbycusis is the most common sensory deficit among the elderly. It is reported that roughly two-thirds of those above the age of 70 have hearing loss, with the prevalence doubling every decade of life between after the second decade, however large cross-sectional studies have shown that 100% of those over 80 had presbycusis.87,88 It is defined as hearing loss of sounds (or a hearing threshold) below 25 decibels for mild and 41 decibels for moderate. 89 Presbycusis can impair the ability to participate in society, drastically impact safety, and accelerate cognitive decline in older adults. Numerous studies have suggested a correlation between dementia and hearing loss with 1 significant study showing that even mild hearing loss increased risk of dementia by 1.9x and over 5x for those with severe hearing loss.90,91 Presbycusis is associated with higher frequency hearing loss and difficulty hearing consonants, making it difficult to hear words and properly understand others speech. 89 Numerous risk factors are associated with hearing loss including age, gender, ethnicity, comorbidities including depression, medications, and lifestyle choices including diet.92,93
Alpha-Lipoic Acid
Alpha-lipoic acid (ALA) is an essential cofactor for mitochondrial enzymes that protect against cochlear damage through free radical scavenging and inactivating cell death pathways. 94 It has robust proof in animal studies to attenuate age-related hearing loss. 95 Few studies have been performed in humans, with 1 study demonstrating efficacy in protecting against noise exposure and another showing a decrease in impact from tinnitus or ringing in the ears.94,96 Dosages have ranged between 300-600 mg and Quaranta et al showed that 1 time doses prior to exposure were not protective but a 10 day course of ALA did confer benefit. 94 ALA represents a new frontier for antioxidants impact against hearing loss but further studies are needed prior to formal recommendations.
Vitamins and Folate
Hearing loss may be impacted by the antioxidant properties of vitamins and carotenes. While animal studies of carotenoids as well as vitamins A, C, and E support their efficacy,97-99 human studies overall suggest a mixed picture.100-102 However what seems to be repeated throughout the literature is the inverse relationship between Folate and hearing loss.100,103 Kabagama et al’s study did suggest however, that there might be higher risk of hearing loss in those with elevated levels of erythrocyte folate (∼985 nmol/L), but lowest risk at ∼658 nmol/L. 103 The proposed mechanism is that low levels of folate have been associated with decreased endocochlear potential due to the destruction of the microvasculature of the stria vascularis. 101 It is important to consider that Curhan et al’s study suggest that folate intake should be at least above 600 μg per day and that serum folate may not be a good measure of erythrocyte folate. 100 The goal should be to increase erythrocyte folate rather than serum folate, however at present erythrocyte folate is not a widely used or readily available test clinically. Of note, Curhan et al suggests that Vitamin C and E supplementation was correlated with higher risk of hearing loss as well. 100
Eye Health
Healthy vision is important to maintaining function into older age. In the KORA-Age survey, funded within the German research initiative on “Health in Old Age,” 104 stroke and neurological diseases were strongly associated with disability, but joint and eye diseases contributed most to the burden of disability in this group. 2 Common age-related eye diseases that can negatively impact sight include macular degeneration, cataract, and glaucoma. Nutritional factors supporting and maintaining eye health in older adults are an important and ongoing area of study. The eye may be particularly impacted by oxidative stress due to light exposure and high metabolism, and nutrients with antioxidant function may be important in supporting vision as a part of healthy aging.
Antioxidants, Carotenoids, and the Macula
The human macula provides the fine-detail central visual acuity necessary for many tasks of daily living. Oxidative stress is thought to be a factor in the development of age-related macular degeneration (ARMD), a condition in which yellow deposits called drusen accumulate in the macula and there is progressive loss of central vision. 105 As such, antioxidants such as vitamins C, E, and beta-carotene have been studied as a potential preventative treatment in ARMD. The Age-Related Eye Disease Study (AREDS) found that supplementation with vitamins C and E, beta-carotene, zinc, and copper reduced the risk of progression to advanced ARMD by 25% in patients with moderate dry ARMD (with bilateral large drusen) or large drusen in 1 eye and advanced ARMD in the fellow eye. Subsequently, the AREDS2 clinical trial assessed the addition of lutein and zeaxanthin and/or omega-3 fatty acids (EPA and DHA) to the original AREDS formulation. Lutein and zeaxanthin are carotenoids found in the human macula that are thought to serve a protective role by filtering blue light and providing antioxidant properties. They are not synthesized in the human body and must be obtained through dietary sources such as green leafy vegetables (such as spinach, kale, and broccoli) and orange/yellow fruits (such as orange, papaya, and mango). 105 The AREDS2 trial showed that the addition of lutein/zeaxanthin to the original AREDS formulation resulted in an additional 10% reduction in risk of development of advanced ARMD, with the greatest benefit in the group with the lowest dietary intake of carotenoids. The addition of EPA and DHA did not confer any further benefit. 106 The AREDS2 formulation is now routinely recommended for prevention of progression to advanced ARMD, and includes the original AREDS components (minus beta-carotene due to increased risk of lung cancer in patients with a history of smoking) and with the addition of lutein and zeaxanthin. 107 In addition, several epidemiological studies have suggested an association between dietary carotenoid consumption, higher lutein and zeaxanthin serum levels, and ARMD prevention. 108 Finally, in the Rotterdam Study, high dietary intake of antioxidants (zinc, beta-carotene, lutein/zeaxanthin, and EPA/DHA) was associated with a reduction in risk of development of early AMD in those with genetic risk factors. 109 These include foods like yogurt for zinc, yellow and orange vegetables for beta-carotene, leafy greens like kale and spinach for lutein/zeaxanthin and beta-carotene, and fatty fish for omega-3s.
Antioxidants and the Lens
Age-related cataract, an opacity of the native intraocular lens, is one of the leading causes of blindness and vision loss worldwide according to the World Health Organization. 110 There may be a role of oxidative damage in cataract formation and thus a role for antioxidant supplementation in the prevention of cataract formation. However, several studies of vitamins C, E, and beta-carotene have shown no significant effect on development of cataract. 111 Notably, the AREDS study showed no effect of the original AREDS formulation on progression of cataract or incidence of cataract surgery.135 Similarly, in the AREDS2 trial, there was no significant effect of lutein/zeaxanthin supplementation on rates of cataract surgery or vision loss. However, patients in the lowest quintile of dietary intake of lutein/zeaxanthin did have some benefit. 112 In addition, clinical trials have suggested a benefit of multivitamin supplements in prevention of nuclear cataract. 113 It remains to be seen which ingredients in such supplements contribute to the protective or deleterious effects, and further research is needed. Overall, the existing literature has not demonstrated a convincing benefit of antioxidant or multivitamin supplementation for prevention of cataract and does not support recommending these supplements routinely for this purpose. Further study is needed in this area.
B Vitamins and Glaucoma
Glaucoma is a degenerative disease of the ganglion cells of the optic nerve, which connects the retina to the brain. This disease often (but not always) involves elevation of the intraocular pressure, with most pharmacological and surgical treatments aimed at lowering intraocular pressure. Research into neuroprotective treatments that would protect from ganglion cell damage regardless of intraocular pressure is ongoing. Several dietary supplements have been evaluated for their neuroprotective effects in the prevention of glaucoma. B vitamins have the best evidence, particularly nicotinamide, the water-soluble form of vitamin B3. 114 Nicotinamide is a precursor of NAD+, the level of which decreases in the retina with aging, 115 and serum levels of nicotinamide have been demonstrated to be low in glaucoma patients. 116 Animal models show that nicotinamide prevents ganglion cell death during intraocular pressure elevation, and clinical trials in human suggest improvement in inner retinal function with nicotinamide. 117 An additional clinical trial with nicotinamide supplementation in patients with moderate open angle glaucoma showed some short-term improvement in visual field testing parameters, but it is yet to be seen whether an effect would persist long term, and further study is needed. Other compounds such as flavonoids, carotenoids, curcumin, saffron, and gingko balboa have also been studied but need further investigation. 114 In sum, though the B vitamin nicotinamide shows promise as a neuroprotective treatment for glaucoma, 118 the existing evidence is not strong enough to recommend dietary supplementation in prevention or treatment of glaucoma at this time.
Conclusion
Summary of Supplement Recommendations for Older Adults.
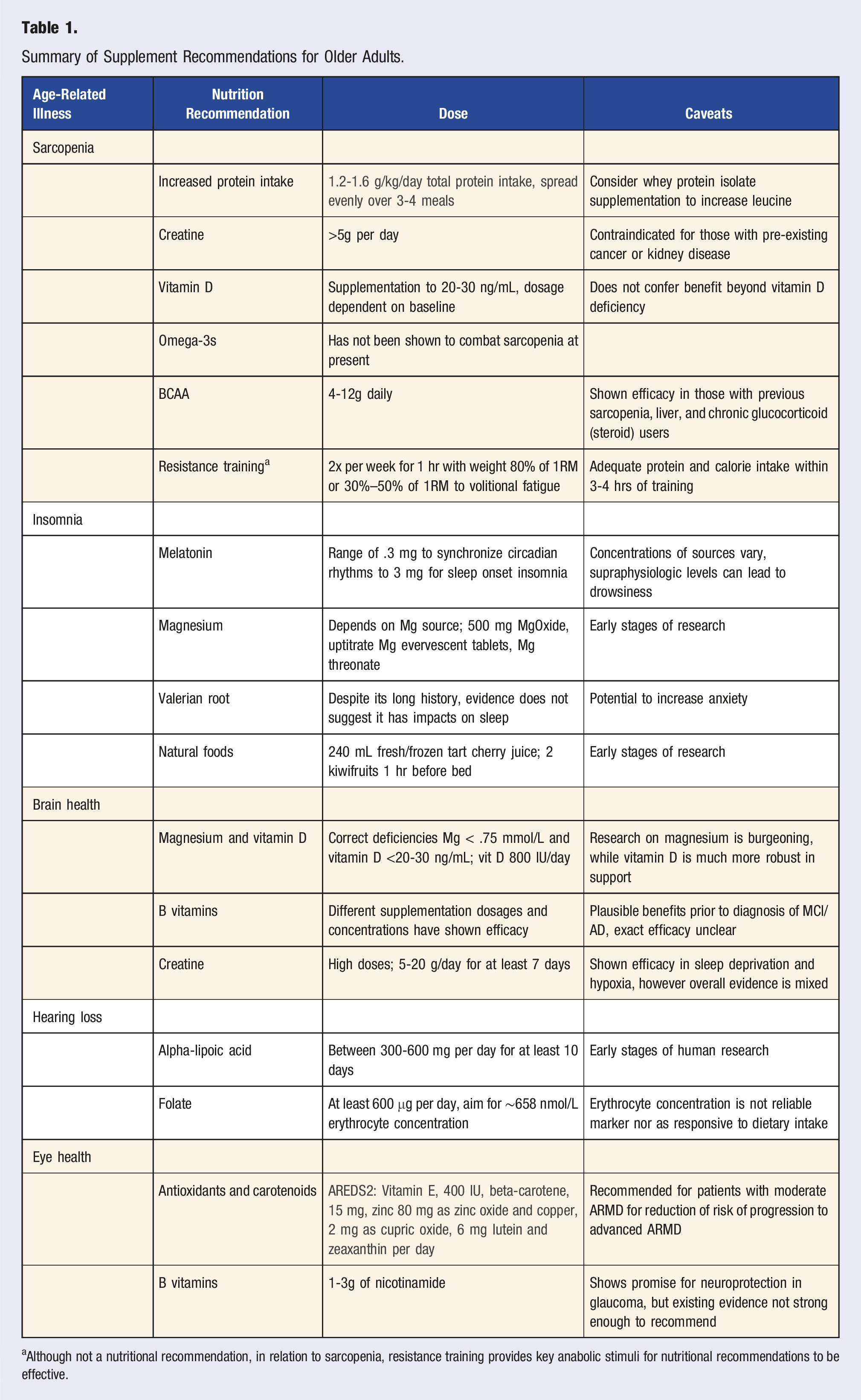
aAlthough not a nutritional recommendation, in relation to sarcopenia, resistance training provides key anabolic stimuli for nutritional recommendations to be effective.
Footnotes
Author Contributions
M.K.- Roles/Writing- Original Draft and Editing, Investigation, Data Curation, Analysis; S.D.- Roles/Writing- Original Draft and Editing, Investigation, Data Curation, Analysis; M.O.- Writing- Editing, Methodology, Supervision, Visualization; C.M.- Writing- Editing, Visualization; M.R.- Writing- Editing, Methodology, Supervision, L.F.- Methodology, Supervision; M.F.- Senior Author, Writing- Editing, Visualization, Methodology, Supervision
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.