
Abstract
The changing needs of our nation’s military veterans call for a change in the healthcare system delivery models providing their primary sources of care. The VA Healthcare System has incorporated a whole health movement emphasizing individualized approaches to healthcare by encouraging complementary and integrative programs. Wheelchair/Adaptive Tai Chi Chuan (W/A/TCC) is such program offering a transformative opportunity to programmatically enhance veteran healthcare services by enhancing the training of VA healthcare providers. This article explores the impacts of a 7-posture W/A TCC instructional training program for healthcare providers that has been facilitated throughout the VA healthcare system since 2016. The purpose is to better understand the impact this training has on healthcare providers, including Recreational Therapists (RTs). A mixed-methods design exploring participant perspectives showed increased confidence levels following training in several key areas and no statistically significant differences between RTs compared to all other healthcare providers. Meaningful impacts described by participants are explored. Overall discussion focuses on this specific training program’s unique applicability for directly influencing VA healthcare providers and the veterans being served. Overall results offer support for wheelchair/adaptive tai chi chuan training as one strategy that can be utilized to increase the success of holistic veteran healthcare.
Keywords
“In order to better understand how veterans can benefit from W/A TCC, we must also look towards the confidence of healthcare providers serving them.”
Introduction
One challenge any healthcare system faces during times of progress is changing demographics, interests, and needs among those they serve. Currently, 17.5% of active-duty military are women, 1 and the largest percentage of living veterans are those who have served since the Gulf War. 2 In addition to demographic changes, it is estimated that approximately 77% of post-9/11 veterans have deployed with 29% deploying three or more times. 3 Fifty-eight percent of pre-9/11 veterans deployed at least once. 3 These statistics do not include longer-term duty assignments where service members are sent overseas to military stations that are not necessarily combat-specific. Deployments and absence affect military families, which in turn influences success rates of veteran reintegration. According to PEW Research Center, 4 61% of post-9/11 veterans who had marital issues while deployed had community reintegration issues when they returned. With these changes, an opportunity exists to explore more holistic opportunities for enhancing provider training to empower healthcare providers in serving a diverse population of veterans with unique disabilities.
For veterans, federal benefits have expanded exponentially since the initial services created after WWI. 5 Programs such as the VHA Transition and Care Management program, 6 the Department of Veterans Affairs (VA) Office of Community Engagement, 7 the Department of Veterans Benefits Affairs (VBA) Solid Start Program, 8 and the Department of Defense (DoD) Office of Warrior Care 9 all have been created to assist military service members and veterans (MSMV) during their transition back into the communities they will now call home. However, even though federal services exist does not mean that MSMV know these benefits exist or how to access the benefits, nor does it mean they will use them. Zoli et al 10 found that 60% of post-9/11 veterans indicated that “navigating VA programs, benefits, and services” (p. ii) was the most significant challenge to their transition from the military.
A recent Whole Health Movement is one of the ways the VA is shifting its perspective on services for military veterans to an individualized approach for overall health and well-being. 11 This movement transitions from a typical medical model that focuses on symptoms to a whole health model that focuses on the team-based development of personalized treatment and health plans holding each veteran’s individualized “values, needs, and goals” at the core. 11 (p. 1) Since implementation in 2018, employees working within the whole health initiative have noted higher motivation, lower burnout and voluntary turnover. 12 Patient satisfaction survey scores were higher, as were overall ratings of hospital performance for facilities where employees were highly involved. 12 All of these findings show improvements are being made through a focus on complementary and alternative therapies (CAT).
Although many professions serving veterans can utilize CAT, there is still an overall negative attitude towards these services among healthcare providers. 13 In addition, there is a limited number of trained therapists who are credentialed to provide these services. 14 Without attitudinal support and an adequate number of trained mentors, it is understandable that a lack of confidence may exist for veteran healthcare providers to branch out into the CAT realm. Confidence is associated with success or failure, performance, trust in relationships, and empowerment. 15 As practice with evidence-based therapies increase, so does the therapist’s confidence in using the practice. 16 Higher confidence in the healthcare workforce results in higher patient experience ratings. 15 The relationship between confidence and CAT exists and can be improved through innovative trainings. CAT training has been associated with increased confidence and self-efficacy for nurses, 14 however, no studies exist to the knowledge of these authors that look specifically at the impacts of a wheelchair based, adaptive CAT.
Recreational therapists (RTs) provide a unique perspective for adaptive CAT in the sense that the entire profession focuses on designing adaptive treatments “to restore, remediate and rehabilitate a person’s level of functioning and independence in life activities, to promote health and wellness as well as reduce or eliminate the activity limitations and restrictions to participation in life situations caused by an illness or disabling condition.” 17 Within the VA, RT purposefully facilitates programs focused on supporting “each Veteran’s self-directed, self-determined, and fully independent participation in their chosen life pursuits” 18 and serves as a driving force in evidence-based adaptive programming and CAT. Since 2016, RTs throughout the United States VA healthcare system have been a part of the driving force in making a W/A TCC program benefit Veterans with disabilities.
Wheelchair/Adaptive Tai Chi Chuan (W/A TCC)
TCC is a Chinese martial art that practices the mind over body concept of harmony where physical movements coordinate with breathing awareness and an internal focus on the body’s natural energy flow. 19 TCC can improve depression and mood dysregulation, 20 cognitive functioning,21,22 physical flexibility, 23 quality of sleep,24,25 PTSD symptoms, 24 and can reduce a fear of falling. 21 The martial arts practice was originally created from combat postures or warrior poses 25 combined with controlled breathing and structured movement. With battle movements as its core, the unique quality of “warrior stances combined with calm breathing and the gentle motion of TCC may provide an opportunity for positive associations with warrior identities to emerge and develop.” 25 (p. 2) This association of a warrior identity 25 created through the application of TCC practice makes it an ideal intervention to improve a variety of symptoms relative to military veterans.
Because traditional TCC does require ambulatory ability, its many benefits have primarily been off-limits to people with ambulatory disabilities, even though most of the movements are performed by the upper body and upper extremities. In 2005, Dr. Zibin Guo 26 developed a form of W/A TCC program making TCC practice accessible and beneficial to people with ambulatory disabilities. This W/A TCC program focuses on helping veterans improve physical and mental health by emphasizing relaxation and focusing on that which they can control as mechanisms to control stress and pain sources through adapted physical activity and social interaction. Since its debut at the 2008 Paralympics, this W/A TCC program has received wide recognition from rehab medicine and the disability communities around the world for its broader applications and creative implications. 26 Since this program focuses on modalities that are specifically designed for veterans with disabilities, an overall emphasis on training healthcare providers to be involved and efficient at the specific movements is imperative.
Since 2017, supported by the VA Adaptive Sports grant, the instructional training workshop of this program has been implemented at 76 VA medical centers in 42 states, including Puerto Rico. More than 800 hundred healthcare providers have participated in this training. Healthcare providers are important for presenting new perspectives for their patients by “reframing and reinterpreting their illness.” 27 (p. 1927) Tai Chi itself has been found to reduce work related stress for health care providers, 28 so there is application for this W/A TCC program to be a valuable training in the adaptive sport and fitness rehabilitation realm. Hovick and Provident 16 found that an evidence-based training incorporating “didactic lectures, case studies, and small group work” improved occupational therapists’ confidence in applying evidence-based skills to their patient populations. Hecimovich and Volet (2009) 29 suggest an importance of developing chiropractic students’ confidence in order to improve their practitioner skills and services provided to patient. Other studies have looked at the positive impact confidence has on the patient experience, 15 but none have looked specifically at W/A TCC as an adaptive training for the healthcare providers’ confidence.
This paper examines the impacts of this W/A TCC instructor training through the perspectives of participating VA healthcare providers. Our major research question asks, “what are the perceived effects of this W/A TCC instructional training on healthcare providers’ confidence in prescribing this program to veterans with disabilities?” While we initially hypothesized that confidence would increase following the training, we did not know how or in what specific areas. We also did not know if any differences existed between various healthcare providers but wanted to explore this focusing on RT as our primary adaptive service based on professional expertise in adaptive sport and fitness. A mixed-methods approach analyzed qualitative and quantitative survey data completed by training participants to best explore our research question. Our overall purpose is to better understand the impact this W/A TCC instructor training program has on healthcare providers’ confidence.
Methods
In order to best understand the perspectives of participating healthcare providers, a mixed-methods design was used to explore the perceived effects of this W/A TCC training program on healthcare providers’ sense of confidence prescribing the program to veterans with disabilities. We were particularly interested in whether or not differences existed between RTs and other healthcare providers. A mixed-methods design was chosen based on its strengths in combining the benefits of both qualitative and quantitative inquiries to reduce limitations imposed by either methodology. 30 This design integrates information from both statistical and thematic analysis driven by the research questions. 31 Statistical, quantitative inquiry within this study explored demographic and confidence level information while thematic, qualitative inquiry sought to better understand participants’ experiences and perspectives. The intentional integration of these various methods was enhanced through a convergent design.31 Quantitative and qualitative data were collected together in the surveys, were independently analyzed, and then compared to each other to determine correlation of findings.
Procedure and Survey Measures
Following IRB approval through the University of Tennessee Chattanooga, data for analyses came from the program’s quality-enhancement web-based survey administered during 2021-2022 to participants immediately before and after completing the W/A TCC training. The pre-training survey link was emailed to participants prior to beginning the training and took approximately 5-10 minutes to complete. These surveys were developed to collect demographics (credentials, gender, race, military service, and previous experience working with Veterans), assess training program quality, and record the unique perspectives of healthcare practitioner trainees. The survey questions were developed by the research team in conjunction with previous healthcare practitioners that had completed trainings in previous years. The research team drafted the initial survey questions and pilot tested with a subgroup of previous healthcare practitioners. Since we were looking at the provider experience with a specific focus on confidence, confidence levels were assessed before and after the training by asking participants, “Using the scale of 0% (not at all confidence) to 100% (highly confident), how confident are you that you can successfully…____” Specific domains of confidence included (1) “explain the purpose and benefits of the program,” (2) “perform the adaptive tai chi movements correctly,” (3) “lead an adaptive tai chi session,” (4) “recruit Veterans to join an adaptive tai chi program,” (5) “maintain an adaptive tai chi program,” and (6) “adapt the program as needed for participants during the session.” Participants selected their level of confidence for each of the above using 10% increments ranging from 0% to 100%. Higher scores indicate higher perceived confidence levels. Open-ended questions were designed to more deeply understand the participant experience. Three open-ended questions were analyzed in this project. Pre-training questions asked: “Why do you choose to work with Veterans? What are your initial thoughts about teaching Tai Chi Chuan in-person? At the end of this training program, what do you hope to have learned?”
The post-training survey link was emailed to participants within 24 hours of completing the W/A TCC training and took approximately 5-10 minutes and re-assessed confidence levels (same procedure as the pre-training survey). Additionally, participants were asked about their confidence to provide exercise modifications to Veterans with disabilities following completion of this training using a “not at all confident” to “extremely confident” scale. Participants were also asked open-ended questions allowing healthcare providers to share personal perspectives and experiences of working with Veterans and completing the W/A TCC training program. One post-training open-ended question was evaluated for this project asking, “From your perspective, what are the greatest needs of Veterans living with disabilities visiting your VA?”
Training
This W/A TCC training program was designed to certify VA healthcare providers to teach this W/A TCC program to veterans with disabilities. Trainings took place over 3-days at various VA medical facilities where participating healthcare providers were introduced or re-introduced to W/A TCC postures and the potential benefits for their veterans. Training locations ranged throughout 11 facilities in 10 states within the United States. The overall goals of this training are to train VA healthcare professionals in this W/A TCC program as an innovative, adaptive service for veterans with disabilities, and to increase healthcare provider confidence in providing adaptive therapy services. With increased confidence, healthcare providers may be more efficient at providing adaptive therapies, in turn increasing both the quality of service provided to veterans with disabilities and the options of services they have to choose from.
Participants
Participants consisted of VA healthcare providers participating in a W/A TCC training who agreed to participate in the study. Purposeful sampling 31 was conducted to specifically target participants who were present and attending the W/A TCC training. All 168 healthcare providers participating in the training were provided with the email survey. Survey respondents (n = 139) provided information for both quantitative and qualitative evaluation. Age averaged 46.6.9 (10.6) years and participants consisted of 17% male, 76% female, and 7% preferred not to say. Racial breakdown included 4% American Indian or Alaskan Native, 7% Asian, 11% Black or African American, 9% Hispanic or Latino, 55% Caucasian or White, 2% Multiracial or Other, and 9% preferred not to say. Respondents self-reported as RTs (n = 52), Occupational Therapists (n = 35), Physical Therapists (n = 30), Health/Fitness/Wellness Coaches (n = 16), Social Workers (n = 7), Peer Support Specialists (n = 7), and other professions (Counselors (n = 4), Nurse Practitioners (n = 3), MDs (n = 2), DOs (n = 2), and Athletic Trainers (n = 2) (participants were asked to select all that applied). Thirty-three were veterans themselves averaging 7.6 (6.0) years of service.
Analysis
For quantitative data, means and frequencies were calculated to describe demographics and confidence levels. Kolmogorov-Smirnov tests were used to assess normality of confidence levels. Due to non-normality, Wilcoxon Signed Rank tests were used to assess difference between pre- and post-training levels and Mann–Whitney U tests were used to assess differences by profession (RTs vs others). Effect sizes were calculated as η2 = Z2/(N-1) with η2 = .01 indicating a small effect, η2 = .06 indicating a medium effect and η2 = .14 indicating a large effect. 32 IBM SPSS Statistics Windows, Version 29.0 was used for all analyses and statistical significance was set at P < .05.
Qualitative themes were formulated through the evaluation of open-ended survey questions. The four questions analyzed all focused on participants’ perspectives of the training program and the veterans they serve. These answers offered important insight that was explored in seeking to understand any differences or lack thereof with provider confidence. Separate line by line coding 33 was the first step in qualitative theme development where researchers reviewed the survey results to create initial themes. Focused coding 33 further narrowed these themes through more explicit comparison to identify the major overall findings. Quantitative and qualitative findings were compared to determine any relevance of findings that either confirmed or disconfirmed resulting theories in gaining a better insight of how the experience impacted healthcare providers.
Results
Quantitative
Prior to this training, 94% (n = 131) had previous experience working with veterans averaging 10.1 (8.1) years of service, 19% (n = 25) had previous TCC training experience, 1% (n = 2) had previous W/A TCC training experience, and less than 1% (n = 1) had previous W/A TCC training with Dr. Guo. Participants saw an increase in confidence levels after completing the training: +44% for explaining (P < .001, η2 = .595), +44% for performing (P < .001, η2 = .570), +44% for leading (P < .001, η2 = .576), +30% for recruiting (P < .001, η2 = .456), +33% for maintaining (P < .001, η2 = .418), and +36% for adapting (P < .001, η2 = .499) (see Figure 1). Healthcare provider confidence levels pre-training vs post-training. Note. Pre-training confidence levels given in black and post-training confidence levels in grey. Practitioners increased confidence across all categories (P <.001) (see Results Section).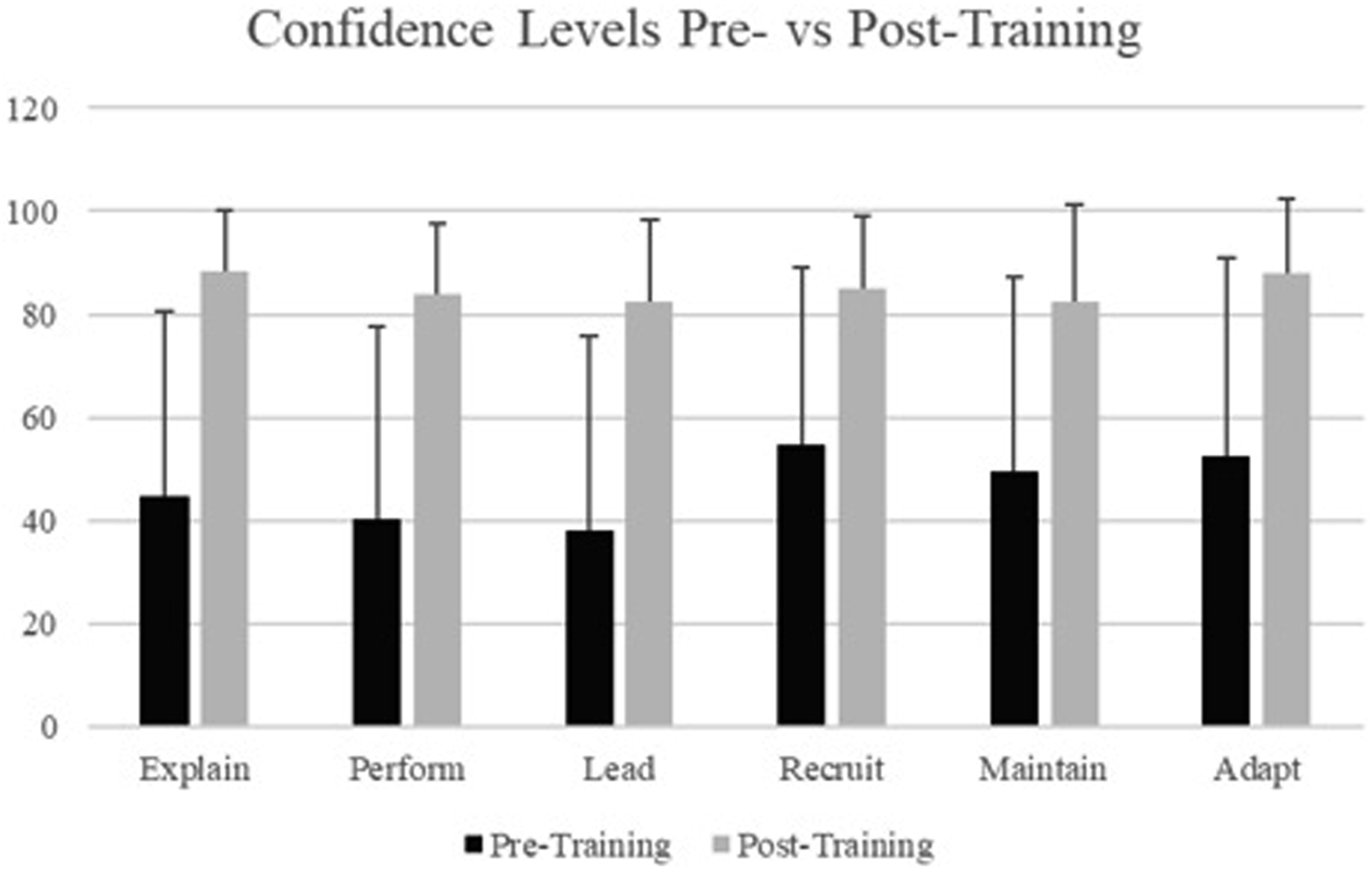
Pre- & Post-Training Confidence Level Comparisons.
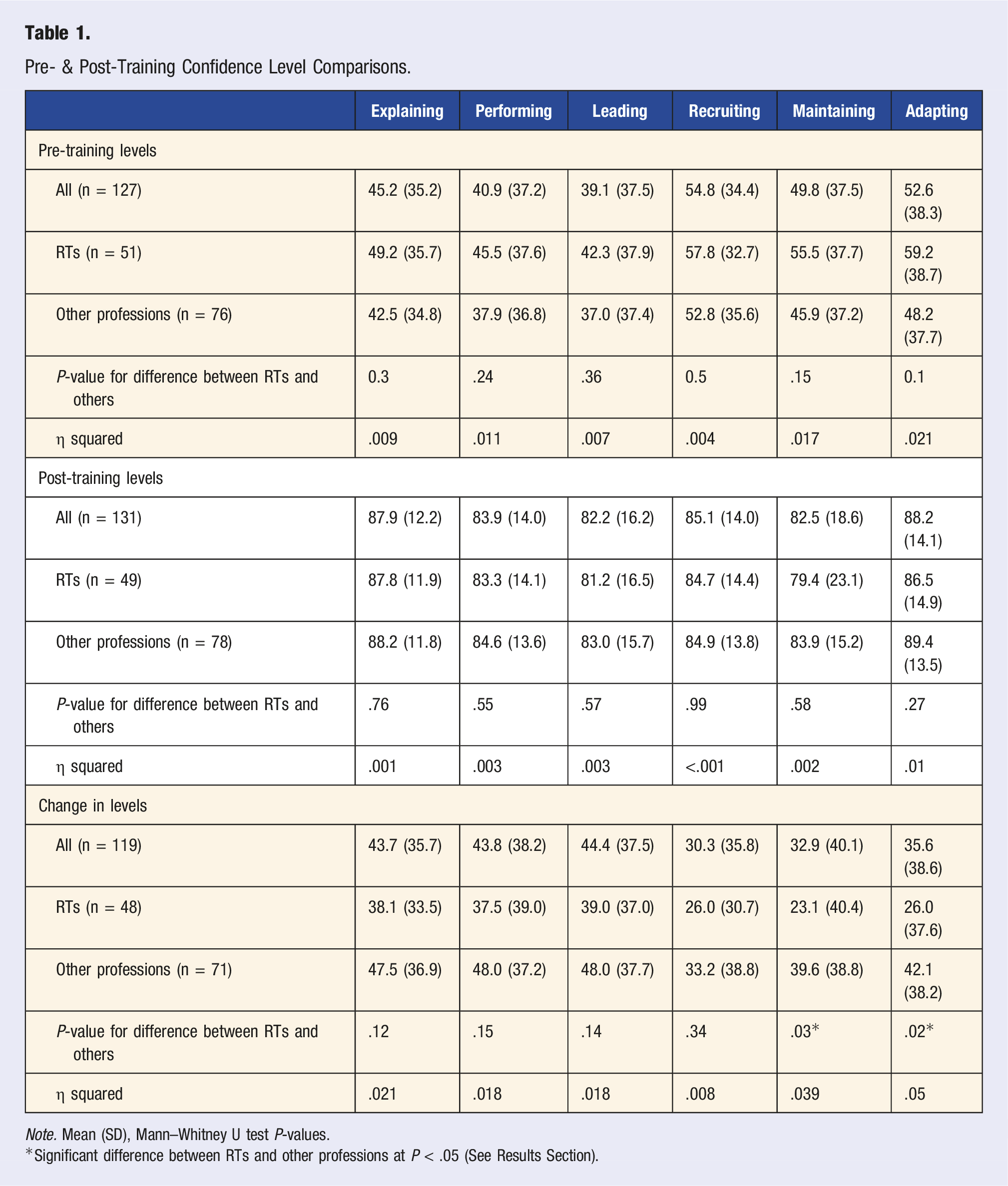
Note. Mean (SD), Mann–Whitney U test P-values.
*Significant difference between RTs and other professions at P < .05 (See Results Section).
Qualitative
In order to further explore the perceived effects of this W/A TCC instructional training on healthcare providers’ confidence, 4 open-ended questions were analyzed alongside the quantitative results to better understand whether or not various perspectives have impact on the results. Not all participants responded to each question, but the numbers of participants of each question still provided a sufficient amount of information to evaluate from a qualitative lens: “Why do you choose to work with Veterans? (n = 116) What are your initial thoughts about teaching Tai Chi Chuan in-person? (n = 95) At the end of this training program, what do you hope to have learned? (n = 114) From your perspective, what are the greatest needs of Veterans living with disabilities visiting your VA?” (n = 115). Two major themes emerged from qualitative results that impact confidence in prescribing the program to veterans with disabilities.
Knowledge of Their Veterans
Healthcare providers felt knowledgeable of their veterans. When asked about their perspective of greatest needs for veterans living with disabilities who visit their VA, healthcare providers identified mobility, sense of community, self-determination, and treatment options. In terms of mobility, practitioners felt participants needed more classes that focused on meeting their physical needs, increasing activity, and helping with fears of falling or movement. A need to focus on functional independence and adaptive programs was expressed. For sense of community, practitioners felt veterans needed programs that helped them “get out of their homes, be social, and be more active.” Camaraderie, social inclusion, leisure, and purpose were all described as veteran needs. For self-determination, practitioners described significant veteran needs in terms of encouragement, motivation, empowerment, and “confidence to thrive in life past their challenges.” One participant stated the greatest need for veterans was a “reconnection to the living human condition (the heart, mind, and body) beyond the limitations, boundaries, and disabilities which they may believe is their experience then, now, and/or in their futures.” Improved coping skills, accountability, and strength were also described in terms of self-determination needs. For treatment options, practitioners described the importance in getting veterans out of their homes and into the community through increased awareness of options, alternative treatments, and supportive educational resources. When asked if this W/C TCC program could help with any of the identified categories of needs, 97% (n = 100) answered yes. Of the three who did not say yes, one participant did not directly answer the question, one stated maybe, and one stated “not directly, but once a veteran comes to Whole Health, I believe this would be a popular program.”
Ability to Influence
Healthcare providers expressed an overall ability to influence their veterans by describing reasons and goals for participating in this specific training. Practitioners described an overall sense of fulfillment for their own professional experiences, and a specific respect for the veteran population as a reason why they chose to work with veterans. A sense of satisfaction was described in bringing “healing and well-being to my community,” giving veterans “hope,” returning “back some dignity,” and “helping them get back to doing what they love for their leisure.” Practitioners felt their jobs held a “noble mission” or purpose in serving those who served our country. One practitioner stated “I truly enjoy this population. They are unique in the challenges they face, and the gratitude is given to those that help them.” Respect for veterans was apparent in all responses. Some stated it was an honor or a passion to work with and serve veterans. “Paying it forward” was often described and some veteran practitioners expressed enjoyment in working with “my extended family” where they felt pride in giving back to those they served with or to other veterans. Non-veteran practitioners expressed professional enjoyment in hearing “their [veterans] stories” and giving “back to those who served.”
Practitioners’ goals for participating in this training also described an importance in the healthcare provider’s ability to influence. For practitioners who had a goal of improving their teaching skills of tai chi, many were focused on how they could use this specific intervention for their different veteran populations. An interest was expressed in learning the foundation and principles of Tai Chi as an evidence-based practice. One practitioner described a goal of training participants to help learn about Tai Chi in the sense that “I may feel confident in my ability to begin introducing the practice to the veterans I serve. I recognize that I have a lot to learn and am excited about furthering my skills/practice in order to better facilitate groups in the future.” Practitioners who had goals of learning more about Tai Chi described a desire to learn how this could be “used with Veterans to improve their health and well-being,” to serve as a self-practice to improve overall competencies, and to become proficient in this adaptive tai chi practice. For those who had goals focused on learning adaptive methods, interests focused on learning “appropriate and safe movement and exercise ideas” for different populations. Practitioners identified an interest in adapting modalities to fit unique needs and “how it [W/C TCC] can be adapted for any ability level.”
Discussion
“Veteran” is a heterogenous group in regard to physical and psychological conditions, especially among the veterans who rely on the VA healthcare system. The great diversity in physical and psychological abilities and needs among them make it an extremely challenging task to develop and implement a fitness or rehabilitation program that would be suitable for all. The degree to which this W/A TCC program has thrived within the VA healthcare system in a short span of seven years and the positive responses toward the program received from healthcare providers are extremely encouraging. They suggest not only the significance of considering the social and cultural realities faced by veterans with physical disabilities in the design of any successful fitness intervention, but also the importance of gaining acceptance from healthcare providers and their critical role in implementing a well-designed program for veterans with disabilities.
In order to better understand how veterans can benefit from W/A TCC, we must also look towards the confidence of healthcare providers serving them. Healthcare provider confidence positively impacts patient experiences15,29 and abilities to provide evidence-based services. 16 Our findings indicate that healthcare provider confidence in prescribing this program to veterans with disabilities increased following this training. Seventy-seven percent felt very or extremely confident in providing exercise modifications to veterans with disabilities and 23% felt slightly or moderately confident after completing the training. In addition to changes from pre-training to post-training confidence results, providers initially expressed confidence in their ability to influence veteran patients by wanting to learn the W/A TCC training program as an evidence-based practice, as an intervention they could use, and as an improvement for veteran outcomes. Participants also expressed an awareness of the need to increase veteran socialization, reconnection to self, and adaptive service options. These perspectives helped answer the research question, “What are the perceived effects of this W/A TCC instructional training on healthcare providers’ confidence in prescribing this program to veterans with disabilities?” However, they also left questions that need to be further explored.
We found connection in the qualitative perspectives of participants to the confidence level increases, but were unable to fully explain how and why confidence changed. Although further studies are needed to support the following theory, one reason this W/A TCC training might have had such an impact on provider confidence could be the influence of the physical activity task within the training. Instead of watching a video or watching someone teach the skills, the providers were actively involved in the program they would be prescribing and/or teaching to future veteran patients. Lobelo and Garcia de Quevedo 34 similarly found that practitioners who were more physically active on their own were more likely to confidently and more frequently encourage physical activity for their patients. These habits were personal habits and not specific to actively participating in the therapeutic modalities they would teach; however, this study did find that these personal habits influenced healthcare providers’ abilities to influence their patients. 34 Similarly, Birkhäuer et al 35 identified patient trust in their healthcare practitioners as positively impacting health-related behaviors, symptom relief, satisfaction with treatment, and quality of life.
When comparing RTs to all other healthcare providers, no statistically significant differences were found. The only differences we discovered were greater increases in confidence of other practitioners (versus RTs) to maintain and adapt the program after completion of the training. One answer to this finding could lie in the fact that the recreational therapy discipline already functions inherently as an adaptive service focused on maintenance and adaptation programs for individualized needs. According to the American Therapeutic Recreation Association, RT services help individuals become more active and informed with their own personal health care. 17 RT has been examined as an integral part of a rehabilitation treatment team 36 and has been included in research regarding veteran whole health services, 37 but limited studies have examined the impacts specifically within the whole health movement and none exist to the knowledge of these writers that look at W/A TCC programs facilitated through RT as employee trainings. Future studies should explore these concepts in looking at how CAT like RT and W/A TCC can benefit the veteran reintegration process through increased provider confidence and efficacy.
This study offers an in-depth evaluation of how one specific W/A TCC training program can promote healthcare provider confidence in providing adaptive programs to veterans with disabilities. No research specific to the impact W/A TCC training can have on healthcare providers is known to these authors; however, an overall conclusion can be made that healthcare professionals who feel confident in their abilities to incorporate adaptive and individualized activities such as this W/A TCC program may have a uniquely positive impact on their veterans’ outcomes.
Conclusions
This study offers a first look at understanding the impact this W/A TCC training program has on healthcare providers and offers insight towards how this adaptive sport & fitness program can be used to improve holistic healthcare for veterans with disabilities. The healthcare needs of military veterans will always be changing, and providers of healthcare services must be proficient at adapting and modifying therapies to fit an individualized, whole health model of healthcare. This study shows that W/A TCC training can act as a unique, adaptive sport & fitness program that enhances confidence for a variety of different healthcare providers. The practice of W/A TCC movement focused on the mind body synchronization, and flow of body, rather than the “ability” of the specific body part. In doing so, it intended to provide a sense of empowerment through transforming the perception of “disabled” body. By proactively combining yielding and redirecting movements of the physical body and wheelchair, a natural transition was encouraged where the perspective of “disability” became one of “ability.” This is important for promoting physical and psychological well-being for veterans. By incorporating this training to VA healthcare providers, veterans gain increased access to an adaptive CAT that has evidence-based results through the provision of services and expertise of trained healthcare providers. With improved confidence in maintaining and adapting a W/A TCC program, healthcare providers may be more likely to continue offering adaptive services, which would result in increased evidence-based options for veterans and a better overall patient experience.
Limitations
A limitation exists in applying findings from this sample population to the greater population of community-based healthcare providers. Although our study is one of the few, if only, study that looks at a broad spectrum of healthcare providers, we focused specifically on healthcare providers within the VA. Veteran healthcare providers in the community may not have the same access to financial support or training for CAT that the VA can offer. It may be more difficult to implement options such as W/A TCC for these providers. Although we can assume the benefits would be similar and can hope these findings will encourage administrators to support such trainings, we cannot assume that the opportunities to participate in this training actually exist on equal levels for these providers. Future studies may want to look at veteran healthcare providers within the community to determine if participation in this training improves confidence to prescribe W/A TCC when supportive resources are limited or non-existent. An additional limitation exists in the fact that this was the first study exploring the perceived effects for VA healthcare providers. Future studies should look at the long-term impacts of this W/A TCC through follow-up looking at how confidence levels and provision of services have been maintained. Our study was also limited to exploring provider training perspectives, not the perspectives of veterans participating in W/A TCC from these providers. Future studies could build on these results by replicating methods with the same W/A TCC program on a greater scale to compare results of veterans being served by the participating healthcare providers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research of this article: This work was supported by the Department of Veterans Affairs VA Adaptive Sports Grant [FAIN# SPORTS-21-055].