
Abstract
“The development of a gender-specific health education strategy may provide a good basis for smoke-free health promotion.”
Introduction
Smoking is the biggest cause of preventable death and ill health in the developed world. 1 The global health and economic burden of tobacco use is enormous, and is increasingly borne by low- and middle-income countries. 2 Thus, not only could the burden of tobacco dependence be measured in premature deaths due to respiratory, cardiovascular disease, and cancer, but also in economic costs from lost productivity and intensified medical care. 3
A variety of factors have been associated with smoking initiation, including chance, 4 emotional distress, 5 attitudinal issues, 6 and cognitive, emotional, or imagery engagement with characters in mass campaigns. 7 Though a host of factors can contribute to its onset, most adult smokers develop the habit before the age of 18. 8
On the other hand, smoking cessation efforts have benefited from continued pharmacologic developments, increased public awareness of anti-smoking programs, intensive counter-campaigns to illustrate the toll of cigarette smoking (conducted in the context of comprehensive tobacco control programs), and recognition of the many primary and secondary effects of smoking exposure on the general public.3,9 In addition, motivational factors and deep-rooted personal or societal values, such as independence, strength, autonomy, and self-control, seem to influence beliefs and decisions about smoking discontinuation.10,11
Greece is a leading tobacco producing country in the context of the European Union, 12 and touts a 90% rate of population exposure to tobacco smoke (current smoking and secondhand smoke). 13 The present study aimed to identify the potential association between socio-demographic and attitudinal factors with smoking initiation, and cessation, and gain insight pertaining to the main source of information about smoking, and its potential impact. An additional research hypothesis was that smoking is continued, because of ensuing dependence, and stopped, following doctors’ warnings of the possible nearing onset of development of serious illness. Identifying potentially modifiable parameters among these factors could influence smoking rates and maximize the potential effect of anti-smoking campaigns.
Methods
Study Setting and Participants
An internet-based survey was conducted between May 31 and July 31, 2016, in people belonging to the survey registry of AKOS, a non-profit anti-cancer institute in Greece. The registry consists of AKOS supporters and volunteers, who had participated in actions and congresses organized by AKOS, and provided full demographic details, including e-mail addresses, so that registrants could participate in future actions, including on-line surveys. The AKOS institute conducts studies consistent with its founding principles that are of interest to cancer sufferers and to public health. Hence, no Ethical Committee approval was necessary. Nevertheless, all procedures performed were in accordance with the ethical standards of the institutional and national research committee, and with the 1964 Helsinki declaration and its later amendments.
The study questionnaire (Appendix 1), along with a brief explanation of the survey, was e-mailed to a random unweighted sample of 3382 adult participants. The respective e-mails were opened by 1942 people, of whom 1618 responded, yielding a respective rate of 83.3%.
The study questionnaire consisted of four sections: a) a common question for all study participants pertaining to their smoking status (current, ex-, non-smoker), b) a section associated with the specific smoking, ex-, or non-smoking status of each participant (nine, four, and three items, respectively), c) a common question for all study participants pertaining to their main source of information about smoking, and the potential impact of that source of information, and d) socio-demographic data of the participants. These data comprised gender, age group, education, and sector of employment, and were specifically completed in relation to the specific study, and not merely extracted from the AKOS registry.
The design of the study questionnaire, and the selection of the variables included in each section was performed by the senior co-author (D.K.) based on prior knowledge, derived from similar international studies,14-17 along with an intention to explore further the respective parameters in the Greek setting. The smoker category included both regular/systematic (i.e., less than one pack/day, or weekend/social smoker, at least one pack/day, over 2 packs/day), and habitual smokers; the questions regarding the most important reason for continuing to smoke and the most important reason to quit smoking (questions number six and seven, respectively), along with their placement within the questionnaire were original. These questions were conceived and constructed after repeated personal interaction of the senior co-author (D.K.) during nationwide anti-smoking campaigns. Ex-smokers were specifically asked to state the reason for smoking discontinuation, in order to confirm their inclusion in the respective category; this question was also originally created, and additionally served as a means to test the research hypothesis. The never smoking status of non-smokers was also confirmed by their response, as to the reason for never having smoked. The study questionnaire included strictly closed questions, in a multiple-choice answering format.
Statistical Analysis
Descriptive statistics (mean ± SD) were initially estimated for numeric characteristics, along with a 95% confidence interval for selected variables. Absolute and relative frequencies (percentages) were used to present demographics for categorical data, as well as basic characteristics of smoking behavior. Contingency tables, along with chi-squared test (Pearson’s and Fisher’s exact), were created to investigate relations between categorical variables. Student’s t-test for independent samples and simple ANOVA were specifically used to study the differences in mean values between different levels of categorical variables.
The categorization of the study participants into smokers, ex-, and non-smokers was used as a basic stratification factor. Gender was used as secondary stratification.
Multiple binary logistic-regression models were fitted to investigate the relation of selected result variables with potential predictor factors. Smoking cessation efforts (Yes/No), effect of anti-smoking campaign (Yes/No), and attitude towards other smokers (Positive/Negative) were the basic result variables used in the regression models. Point estimation and 95% confidence limits for the odds ratio were presented.
All analyses were performed using SAS version 9.1. Statistical significance was accepted at the level of .05.
Results
Socio-demographic Characteristics of Study Participants.
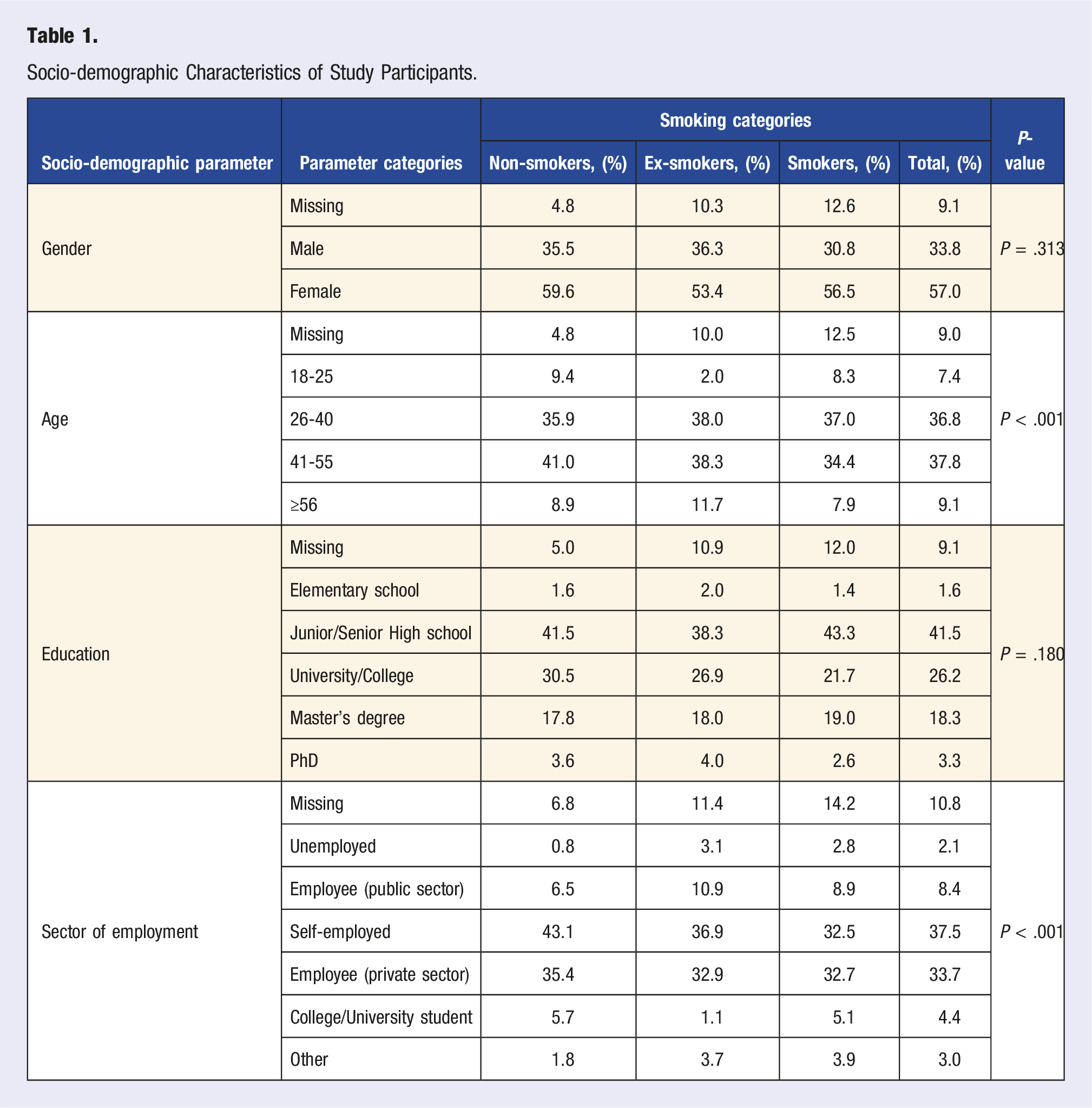
Regarding the duration of smoking, smokers tend to smoke for a longer time period than ex-smokers did (21.2 ± 10.94 vs 17.8 ± 10.1 years, respectively, P < .001), which was not readily expected, as they also tended to be younger (P < .001).
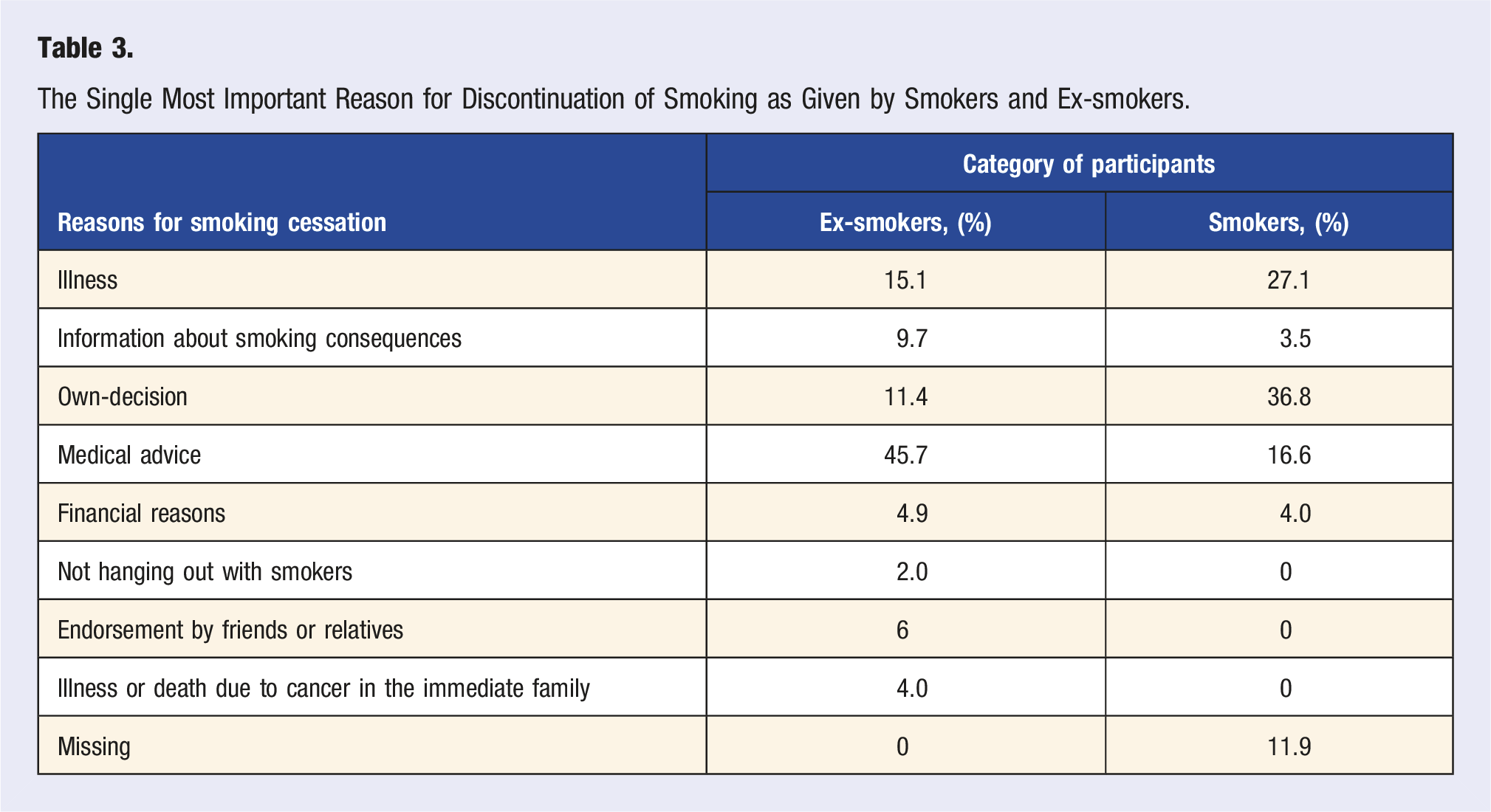
Drawing on the most important reasons for smoking cessation, it is interesting to note that although smokers cite own-decision as the main reason that could lead to smoking discontinuation (36.8%), the reality, as depicted by ex-smokers, is that the main reason to stop smoking had been medical advice (45.7%).
The internet (in over 50%) and television (in around 30%) represent the main sources of information about smoking and its potential hazardous effects, whilst national or international campaigns against smoking (including pack labels) had adversely influenced only a minority of smokers against it, in comparison with their ex- and non-smoking counterparts (P < .001). Finally, tolerance against smokers is not only extremely low among non-smokers (41.8%), but also quite low among ex-smokers (58%), compared to the smoking subgroup itself (78.7%) (P < .001).
Regarding the effect of gender in the smoking epidemic in Greece, men tend to be heavier and more systematic smokers, than women (P < .001). They also start smoking at a younger age, than women do (P < .001). Indeed, the mean initiation age was 18 (±3.23) years in men, in contrast to 19.2 (±4.25) years in women. Consequently, men smoke longer than women, and this applies both for smokers (P < .001), and ex-smokers (P < .001).
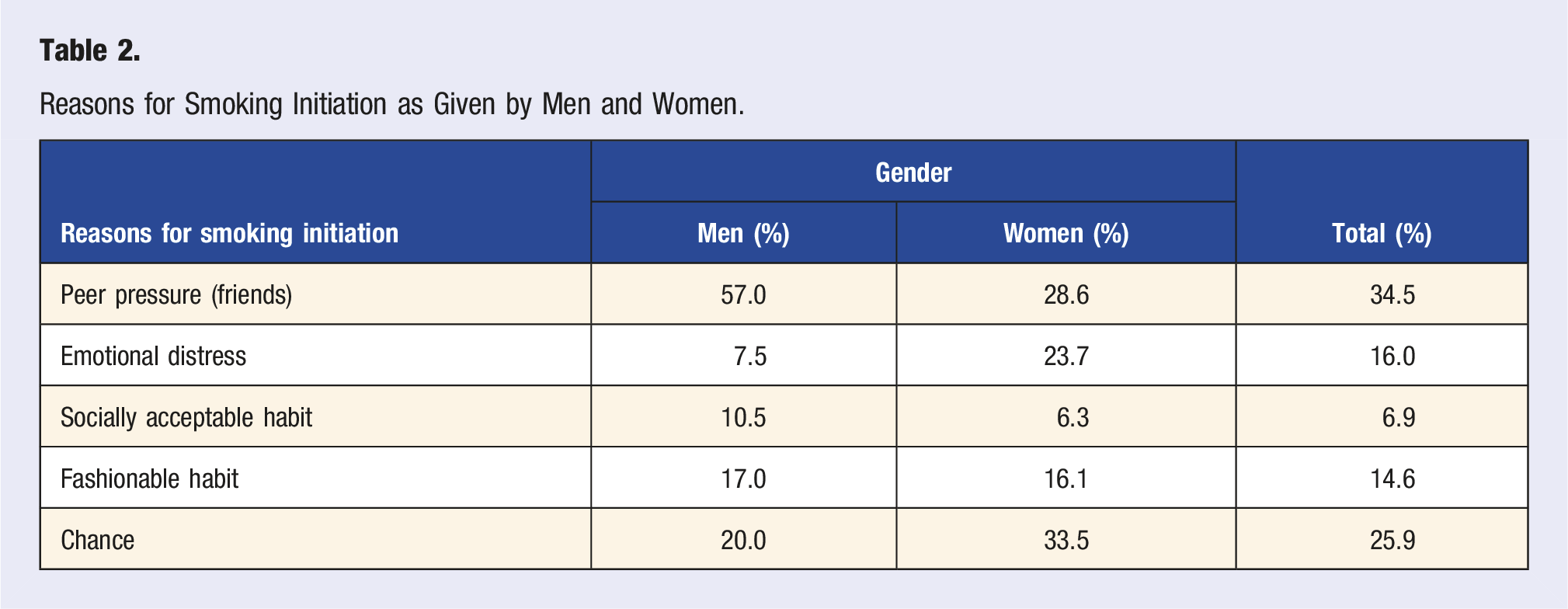
Reasons for Smoking Initiation as Given by Men and Women.
The Single Most Important Reason for Discontinuation of Smoking as Given by Smokers and Ex-smokers.
Finally, there seems to be no gender effect, either regarding national and international campaigns against smoking (including pack labels) (psmokers = .824, pnon-smokers = .075, pex-smokers = .065), or tolerance against smokers (psmokers = .439, pnon-smokers = .225, pex-smokers = .366).
Odds Ratios and 95% Confidence Intervals for Specific Determinants of Successful Cessation Efforts, the Effect of National or International Anti-Smoking Campaigns on the Success of Cessation Efforts, and the Effect of Attitude Against smokers.
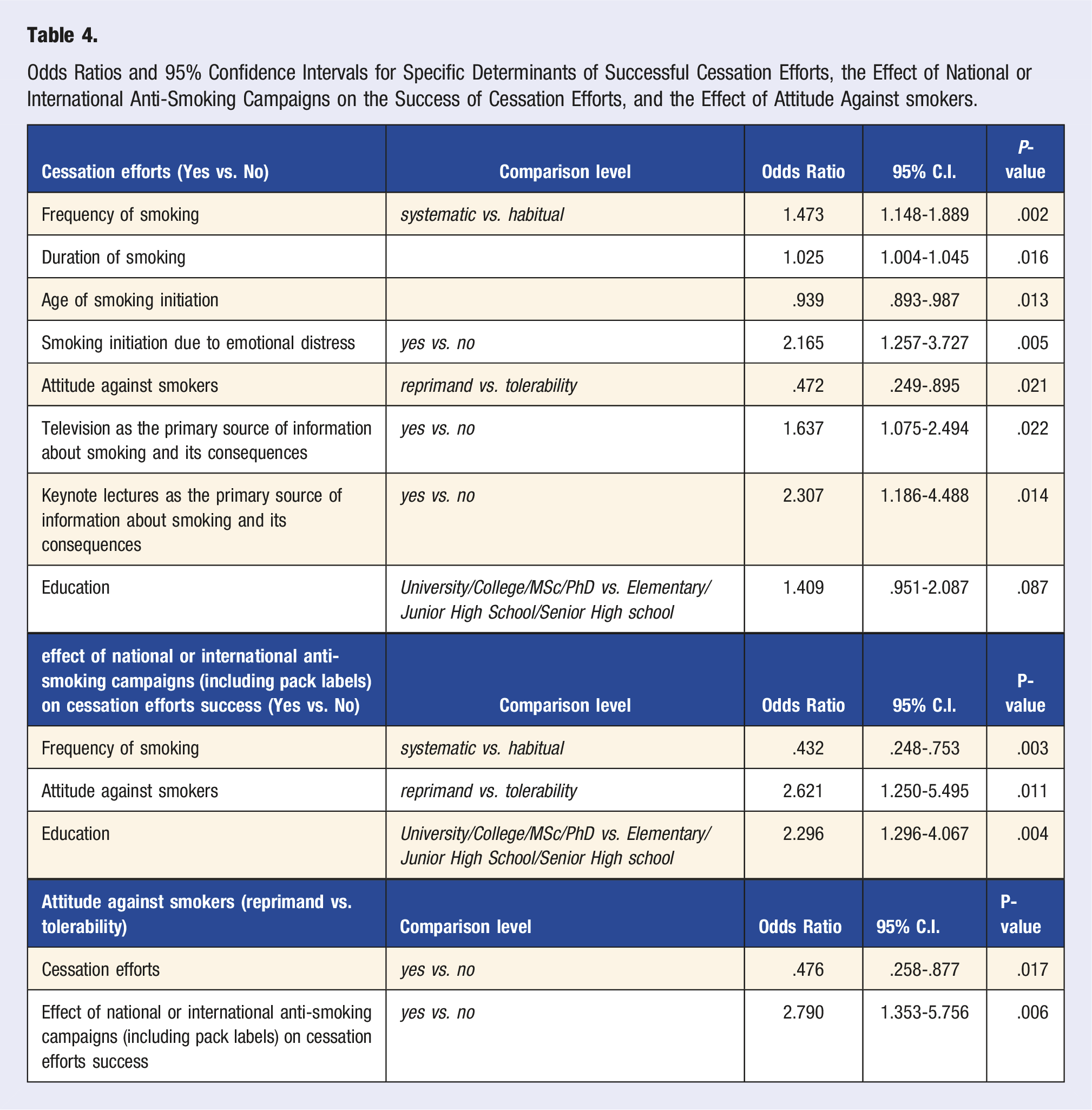
Drawing on the effect of national or international anti-smoking campaigns (including pack labels), this was adversely associated with regular/systematic smoking (P = .003, OR = .432). By contrast, a reprimanding attitude towards smokers (P = .011, OR = 2.621) and higher educational level (P = .004, OR = 2.296) seemed to positively influence the effect of such campaigns.
Finally, smokers, who have attempted to discontinue smoking, are less likely to adopt a reprimanding attitude towards other smokers (P = .017, OR = .476), whilst people, who have been positively influenced by national or international anti-smoking campaigns (including pack labels), are more likely to do so (P = .006, OR = 2.79).
Discussion
Smoking is a systematic disease comprising nicotine dependence and smoking-related illnesses. 13 Smoking directly affects the health of adults and adolescents who smoke in an adverse manner, and has a bystander negative effect in people and fetuses who do not smoke, through secondhand smoking. Hence, smoking represents the most preventable cause of disease, and, of all health interventions, those which can reduce the prevalence of smoking, will have the biggest positive impact on health. 1
The present study confirmed the high prevalence of smoking (40.1%) in Greece, reported in previous studies,18-20 thus highlighting the disappointingly low penetration of anti-smoking health promotion campaigns within the Greek population. However, socio-demographic differences between smokers, ex-and non-smokers in total, and differences pertaining to age, sector of employment, and duration of smoking were also identified (Appendix 1-study questionnaire, Table 1). Indeed, non-smokers were more often private sector employees or self-employed, compared to their smoking and ex-smoking counterparts (P < .001). This finding indicates that a successful movement towards a non-smoking environment in Greece presupposes banning smoking in all state buildings, and not just creating separate smoking areas, a regulation which is often violated in practice, due to the absence of strict control. Indeed, in a study about the compliance and attitudes towards smoking bans among schoolteachers in Attica, 69% of smokers admitted to smoking on school grounds, thus confirming non-compliance with the smoking ban in public places, even those involving a socially sensitive workplace. 21
The observation that smokers tended to smoke for a longer time period, than ex-smokers (P < .001), despite their younger age as a group (with more people belonging to the under 25, and less to the 41 and over years of age categories, P < .001), supports the need of bolstering cessation campaigns early in smokers’ lives. And although smoking cessation is a prolonged journey, rather than a single trip, 1 it makes sense that the journey would benefit from an earlier start. Hence, with a view to creating a future smoke-free generation, not only are youth-based smoking prevention interventions warranted,6,18,22 but also are specially-designed campaigns against youth smoking, in addition to adult-focused anti-smoking campaigns, which adolescents also seem to find of certain relevance to them. 17 These would bolster not only health literacy and public awareness, but also the potential success of anti-smoking campaigns.15,23
As far as a gender effect in smoking was concerned, men tended to be heavier and more systematic smokers, than women (P < .001), having started smoking at a younger age (18 (±3.23) vs 19.2 (±4.25), respectively, P < .001). Consequently, men smoked longer than women, and this applied both for smokers (P < .001) and ex-smokers (P < .001). These findings identify male youths as a significantly at-risk population for smoking initiation, and necessitate interventions that would assign realistic values to smoking risks and benefits amongst them, 6 in order for young males to engage in the health-protective behavior of not smoking. In addition, educational interventions targeting parents, especially those who are smokers, could substantially reduce the exposure of adolescents to secondhand smoke at home, which, as an effect, appears to be stronger, than the respective status of close friends. 22
Regarding the main factors of influence for smoking initiation, these were found to differ between genders (P < .001), with friends playing a key role among men, and emotional distress, as well as chance, among women. The results in women are different to some extent from the study by Griffin et al, in which girls were shown to be more strongly influenced by peer smoking, than boys, although this study had rather focused on heavy smoking, and not smoking in general. 24 They reveal, however, the potential existence of an emotion-smoking comorbidity in women, where anxiety-sensitivity, and/or distress intolerance may promote progression across the smoking trajectory, by amplifying the perceived emotional properties of smoking. 5 By contrast, the existence of substantial peer group homogeneity, regarding the initiation of smoking, 25 is confirmed by the central role that friends seemed to play in the respective outset in men.
There also seems to be a gender effect for smoking continuation (P < .001). In addition to the perceived pleasure and habitual smoking continuation cited by both genders, men seem to realize that a primary reason for continuing to smoke is dependence, whilst women attribute their choice on a psychological need. Hence, there is a need for a gender-specific targeted anti-smoking intervention, 26 placing emphasis on appropriately tailoring the message that the real reason behind smoking continuation is dependence, rather than pleasure, and utilizing innovative channels, through which either gender can be effectively reached. The development of a gender-specific health education strategy may provide a good basis for smoke-free health promotion.
Although the present study did not identify any difference between men and women in the number of times they have tried to stop smoking (P = .288), there was a significant difference, regarding their motives for making such an attempt (P < .001). An own-decision seems to be of paramount importance for women, whereas medical advice and potential illness are most important to men. Whilst the latter points of view seem utterly realistic, the former belief tends to dominate the prediction of quitting attempts in many smokers, irrespective of gender. 11 This seems to stem from the perception of quitting as a strictly personal responsibility, which relates interchangeably to a person’s own self-identity, independence, strength, autonomy, and self-control. 10 Although these perceptions should be addressed with respect by the medical professional, they actually tend to raise barriers in the successful implementation of medical treatments for smoking cessation. That is because the reality, which was admitted by the ex-smokers in the present study (Appendix 1, ex-smoker question number two), was that the main reason for them to stop smoking had been medical advice (45.7%), and not own-decision (Table 3). Similarly, a previous European survey demonstrated that adult smokers in Europe seem to quit smoking for two major reasons; becoming ill, or gaining knowledge on smoking-related harm. 27
Drawing specifically on smoking cessation, the results of the present study indicated that discontinuation efforts were most likely to occur in systematic smokers (P = .002), and were also associated with the duration of smoking (P = .016). They were also positively associated with emotional distress, as the primary reason for smoking initiation (P = .005), and anti-smoking campaign through the television (P = .022), as well as keynote lectures (P = .014). The positive effect of anti-smoking television advertising on smoking cessation has been previously acknowledged. 14 That is because television has the potential to reach and to modify the knowledge, attitudes, and behavior of a large proportion of the community. 28 The achievement of sufficient population exposure to anti-smoking campaigns is, therefore, vital, especially for lower socioeconomic status smokers, 7 with each additional channel of exposure to anti-smoking advertising increasing the likelihood of making a quit attempt. 14
However, the results of the present study suggest that the potential existence of an emotion-smoking comorbidity, pertaining to smoking initiation, is not a deterrent factor for discontinuation efforts, despite the clinically significant distress associated with smoking cessation. 29 In addition, keynote anti-smoking lectures hold a far greater significance, than courtesy invitations, as the experts seem to be in a position to positively influence the respective attitude of their audience.
By contrast, younger age of smoking initiation (P = .013) and a reprimanding attitude towards smokers (P = .021) seem to influence cessation efforts in an adverse manner. Nevertheless, it is important to recognize that in everyday life many young people are not systematic decision-makers; their intentions are extremely volatile and context-dependent, and, as such, highly spontaneous. 30 Hence, bolstering attitudinal factors during youth, might counteract immature risk assessment, and play a role in protection against youth smoking. 6 Furthermore, comprehensive tobacco control programs are more likely to promote quitting and reduce adult smoking prevalence, 31 rather than rowdy reprimanding attitudes, towards smokers.
Regarding the effect of national or international campaigns against smoking (including pack labels), these had adversely influenced only a minority of smokers against it, in comparison with their ex- and non-smoking counterparts (P < .001). This disappointing result comes in stark contrast with previous reports, 2 and could only be viewed in the context of the observed lack of political willingness in Greece to implement a comprehensive tobacco control program. Despite former legislative provisions, 32 indoor smoking has only recently been officially prohibited. 33
Regression analysis revealed that the effect of national or international anti-smoking campaigns (including pack labels) was adversely associated with regular/systematic smoking (P = .003), which was not surprising, taking into account the afore-described reality in Greece. Interestingly, however, a reprimanding attitude towards smokers (P = .011), and higher educational level (P = .004), seemed to positively influence the effect of such campaigns. Hence, although reprimanding smokers seems to influence their cessation efforts in an adverse manner, it appears to enhance the penetration of anti-smoking campaigns, probably counteracting the aforementioned political inactivity, towards implementing the law. The opposite also seemed to be true; people, who had been positively influenced by national or international anti-smoking campaigns (including pack labels), were more likely to adopt a reprimanding attitude towards smokers (P = .006). These findings appear to confirm the lack of respective tolerance, caused by years of ineffective smoking regulation.
Finally, the positive association between the effect of national or international anti-smoking campaigns and higher educational level can be explained by the idea that having more formal education generally helps people to acknowledge the core messages of such campaigns. Perhaps such people therefore search for additional information about smoking risks and/or discontinuation methods through the internet, 34 cessation helplines, and similar sources. It also supports the notion that a lower overall prevalence of current smoking, especially in higher educational classes, is to be expected in Greece, should systematic anti-smoking health promotion campaigns be implemented. 18
Limitations of the present study include the use of an unweighted sample, based on responses received through the internet. Nevertheless, this modern approach resulted in a high response rate, and a large, but balanced sample size, whilst avoiding common methodological problems (i.e., underrepresentation of women or certain age groups, lack of experience from the interviewer, imputation of data). The possibility of selection bias cannot be completely excluded, as the AKOS registry may attract a population already interested in cancer control. However, the survey registry could serve as a means for future research, and comparisons with the results of the present study.
Conclusion
The necessity of implementing comprehensive tobacco control programs in conjunction with the appropriate political willingness, the added value of endorsing campaigns against youth smoking, and the importance of medical advice as the main reason leading to smoking cessation need to be acknowledged by health professionals, health policy makers, and politicians in order to address the smoking epidemic in practice.
Supplemental Material
Supplemental Material - Attitudes and Parameters Influencing the Smoking Epidemic in Greece: What is Important?
Supplemental Material for Attitudes and Parameters Influencing the Smoking Epidemic in Greece: What is Important? by Petros V. Vlastarakos, MD, MSc, PhD, IDO-HNS (Eng.), Angeliki Gkouvali, BSc, MSc, Evangelia-Filothei Tavoulari, MD, MSc, PhD, and Despoina Katsochi, MD, PhD in American Journal of Lifestyle Medicine.
Ethical Statement
Ethical Approval
All procedures performed were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was conducted under the aegis of AKOS, a non-profit anti-cancer institute, based in Athens, Greece.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.