
Abstract
Background: Students’ yearly visits to university counseling centers have increased, concurrent with an increase in diagnosed anxiety and depression. Physical activity (PA) has positive effects on mental health. PA referral may be an option to utilize PA in university mental healthcare. However, clinicians’ perceptions and capacity of PA referral need to be established before implementation. Methods: Using a qualitative descriptive design, 14 licensed mental health professionals across seven southern universities participated in semi-structured virtual interviews to explore perceptions of prescribing PA to patients and referring patients to a PA specialist. Results: Thematic analysis revealed professionals perceived PA to be important for mental health, support prescribing PA to patients, face barriers to prescribing PA, professionals support referring patients to a PA specialist, and professionals face barriers referring to a PA specialist. Conclusions: Professionals agreed that PA was important for mental health and referring to a PA specialist would be the most feasible strategy to incorporate PA in their therapeutic work for patients struggling with physical inactivity and mental health. Future studies should investigate a PA referral system's implementation within university counseling centers and how this system can affect the mental health and PA of college students seeking mental health treatment.
“The clinicians expressed that PA is important for mental health but face barriers for incorportaing PA in their theraputic works.”
Introduction
Mental health symptoms and conditions are prevalent and increasing on university campuses, with anxiety and depression showing the highest increases in prevalence from 2009 to 2015. 1 From 2007 to 2017, university counseling and psychological services experienced a rise in students’ mental health treatment rate from 19% to 34%. 2 In 2020-2021, about 60% of students met criteria for at least 1 mental health problem. 3 Recently, COVID-19 has exacerbated the prevalence of stress, anxiety, and depression on university campuses. 4 One study empirically found that 88% of students reported experiencing moderate to severe stress, 44% experienced moderate to severe anxiety, and 36% experienced moderate to severe depression after the campus shut down in the spring of 2020. 5 As mental health conditions continue to rise on university campuses, remedies to combat deleterious psychological symptoms are necessary.
Physical activity (PA) is any bodily movement generated by skeletal muscle contraction that causes energy expenditure, and exercise is a subset of physical activity that one plans, structures, and repeats to improve or maintain physical fitness. 6 All exercise is considered PA, but not all PA is considered exercise. PA positively influences mental health. 7 Meta-analyses demonstrate that PA decreases both state 8 and trait anxiety. 9 Evidence supports PA to positively affect vital physiological mechanisms of mental health, including neurotransmitter balance, 10 combating oxidative stress, 11 and regulation of the Hypothalmic-Pituitary-Adrenal Axis. 12 Thus, PA may have similar efficacy to standard medications for depression and anxiety while reducing the chances of side effects for depression and anxiety treatment.13,14 Unfortunately, many college students struggle to be physically active.15,16
Guidelines suggest that American adults achieve at least 150 minutes of moderate-intensity aerobic activity (e.g., brisk walking) or 75 minutes of vigorous aerobic activity (e.g., jogging), or an equivalent combination to achieve health-related benefits. 7 Muscle strengthening guidelines include 2 days per week of full body strength training to elicit positive health benefits, including decreased risks of chronic diseases. 7 Using National Health Interview Survey (NHIS) data, current estimates of US physical activity show that only 19% of women and 26% of men meet physical activity guidelines. 17 Similarly, Behavioral Risk Factor Surveillance System (BRFSS) data estimates that 24% of US adults satisfy these physical activity guidelines. 18 Studies demonstrate a range between 46% to 72% of college students who are not getting sufficient PA.15,16,19–21 During COVID-19, physical activity among college students decreased while perceived stress and depressive symptoms increased. 22 However, regular physical activity has shown a negative correlation with psychological distress of college students. 23 Increasing PA among college students is necessary and could provide the extra benefit of improvement in mental health. Thus, universities have developed initiatives or programming to promote PA on university campuses, but the effectiveness of these initiatives on physical and mental health remains unclear. 24
The American College of Sports Medicine began the Exercise is Medicine® On Campus (EIM-OC) initiative in 2009. This global health initiative assesses and promotes PA in student healthcare settings by incorporating PA as a preventive treatment option for students. Health care professionals recommending more PA with an exercise prescription or referring a patient to an exercise professional (also known as an exercise referral scheme (ERS)) may improve PA and health. 25 Few studies have published on ERS in primary student healthcare on university campuses, but ERS in primary student health care have shown to increase physical activity26,27 and self-efficacy for exercise.26,28 College mental health care professionals or clinicians have seemingly been understudied as a target for promotion of PA in students with mental health problems.
This lack of research creates a unique opportunity to understand PA’s current role in college mental healthcare since these mental health clinicians are a direct source of support for the positive mental health of college students. Considering the rapid increase in therapy administered and received on university campuses and the benefits of PA for mental health, clinicians effectively promoting PA to patients could significantly combat the crisis of poor mental health on university campuses. A qualitative study investigated how counselors in the UK have used exercise in their therapeutic work and their experiences incorporating exercise into their practices. 29 The study reported that four of the eight counselors assessed exercise at visits, most counselors felt they lacked the competence to prescribe exercise (some were open to referring patients to an exercise professional), and most counselors felt exercise was important. 29 The perceptions of counselors promoting PA in therapeutic work at universities in the US have not been studied. This is a problem since perceptual factors serve as antecedents and reinforcers of individual behavior. 30
Behavioral theory is advantageous for organizing and conceptualizing perceptual and socio-ecological factors that determine behavior.30–32 Social Cognitive Theory (SCT), one of the most frequently applied health behavior theories, 33 utilizes personal, environmental, and behavioral factors to explain behavior. 30 However, researchers have not investigated the personal, environmental, and behavioral factors among college mental health professionals governing PA prescribing or referring to a PA specialist. Thus, it is necessary to investigate perceptual factors that facilitate or thwart PA incorporation as a treatment option in student mental healthcare in the United States. Identifying specific factors at each level of SCT will allow researchers to understand and plan targeted intervention strategies to facilitate the incorporation of PA as a treatment option or adjunct in student psychological healthcare, thereby improving college students' mental and physical health.
Therefore, the purpose of the current study was to explore the specific individual, environmental, and behavioral factors among practicing mental health professionals that serve as determinants for (1) including PA in their therapeutics work, (2) prescribing PA to patients, and (3) referring patients to a third-party specialist for PA. This study is the first Phase 1 (Design Phase) study of the ORBIT Model for Behavioral Treatment Development. 34 This model serves as a framework for turning behavioral scientific discoveries into health-related efficacy testing. 34 This study is the first study in the development of interventions that effectively incorporate physical activity in therapeutic works of university mental health clinicians to help promote PA and improve the mental health of college students.
Methods
The interpretivist paradigm, a framework where researchers use naturalistic approaches (e.g., interviews, focus groups, etc.) to collect and interpret the meanings of data, 35 was selected to allow for the pragmatic comprehension of personal experiences of a phenomenon through exploring people's thoughts, feelings, and emotions. 36 The research employed an exploratory qualitative descriptive study design, 37 frequently used in qualitative healthcare professional studies to answer practical healthcare research questions to answer real-world healthcare problems. 38 A descriptive study design is congruent with the interpretivist paradigm. 39
Participants
The study included a convenience sample of licensed mental health professionals actively counseling college students within student health care. These clinicians were recruited from 7 large southern universities in the United States. Recruitment included calling or emailing different university counseling centers asking them to distribute an email of the study to their mental health professionals. The principal investigator (PI) had no relationship with the mental health professionals before recruitment. Licensed mental health professionals were defined as professionals with one of the following licenses to work with patients in a clinical setting: professional counselor license, clinical social worker license, mental health counselor license, psychologist license, and provisional registered art therapist license. Participants were eligible if they were actively licensed with one of the licenses mentioned previously and were currently working with college students within their respective university healthcare systems.
Ethics
Participation was voluntary, with participants providing written informed consent before the interview. Clinicians remained anonymous and were given a unique participant ID for reporting (e.g., C1). The University of Arkansas’s Institutional Review Board approved the study (Protocol #: 2105332800).
Interview Scripts
Semi-structured interview questions explored personal, environmental, and behavioral factors related to including PA in therapeutic work, prescribing PA, and referring to a PA specialist. Semi-structured interviews are commonly used in qualitative studies and can meaningfully explore participants' perceptions that guide their behavior. 40 The semi-structured interviews allowed standardization for the interview process by ensuring each clinician explored similar critical topics, such as their attitudes on incorporating PA into therapeutic work. But the interviews allowed freedom for the clinicians to expand on their overall personal experience or tendencies. SCT assumes that personal factors (e.g., attitudes, knowledge, self-efficacy), environmental factors (e.g., barriers, facilitators, resources), and behavioral factors (e.g., reinforcement from overt actions, behavioral skills, and behavioral intentions) reciprocally influence one another and provides a framework for explaining the observance of specific behavioral phenomena. 30 Therefore, SCT constructs guided construction of the interview questions. The interview prompts are available in the appendix.
Data Collection Procedures
The PI conducted semi-structured interviews with eligible participants through Zoom video conferencing. The PI and each participant used Zoom in a private, isolated room. The PI transcribed each interview while watching each interview again to ensure the transcripts’ accuracy. To ensure the credibility of the transcripts, the PI then sent them back to participants to confirm that the answers captured the true essence of their thoughts, feelings, and beliefs when answering the questions and to ensure the transcript’s accuracy. The interview duration ranged from 20 minutes to 1 hour, with an average of 40 minutes.
Data Analysis
For data analysis, the study implemented thematic content analysis to analyze semi-structured interviews effectively. 41 SCT 30 principles guided data analysis to make sense of the data. First, data analysis began with data familiarization by reviewing all transcripts. Then meaningful and similar sentiments were developed into initial codes. Based on the similarity between initial codes and initial themes, subthemes began to form that aligned with the principles of SCT. The PI reviewed the data again to ensure these initial themes and subthemes captured the data set. The PI developed names and clear definitions for the themes. To ensure the reliability and validity of these themes, an independent research assistant separately reviewed and recoded the data based on the definition of the initial theme. Any conflicting codes within themes were reviewed and discussed until the researchers agreed upon explicit inclusion or exclusion of the code. Then the final themes and subthemes were established.
Trustworthiness
To ensure the credibility of the findings, the PI conducted the study using a popular methodological approach, a qualitative descriptive study, which has recognized methodological rigor. 42 To ensure the dependability of the findings, the researcher kept an audit trail across the entire study, which included a bracketing journal and reflective statements and thoughts. The bracket journal allowed recognition of bias by organizing reflective comments and views to minimize these biases when developing codes and themes. An external auditor reviewed the finalized codes, themes, and final audit trail. The external auditor had extensive qualitative research experience but was not involved with the research project besides auditing.
Results
Fourteen licensed mental health professionals who were actively counseling college students at the time of the study from seven different universities across the southern US participated in this qualitative study. Among the clinicians, six practiced in Florida, two practiced in Arkansas, two in Texas, one in Georgia, one in Kentucky, one in Louisiana, and one in Mississippi. Of the participants, 12 self-identified as women, one man, and one non-binary. The average age of participants was 39 years, ranging from 26–67 years. The average years of being a licensed mental health professional were 10 years, ranging from 2–28 years. The average number of years being a licensed mental health professional working specifically with college students was 7 years, ranging from 8 months to 28 years.
From the thematic content analysis of qualitative data, the researchers identified five major themes: PA is important for mental health, clinicians support prescribing PA to patients, barriers to counselors prescribing PA, clinicians support referring patients to a PA specialist, and barriers of clinicians referring to a PA specialist. The text demonstrates exemplar quotes, and the tables show percentages of participants that supported the subthemes within each theme.
Theme 1—PA is Important for Mental Health
Physical Activity is Important for Mental Health.
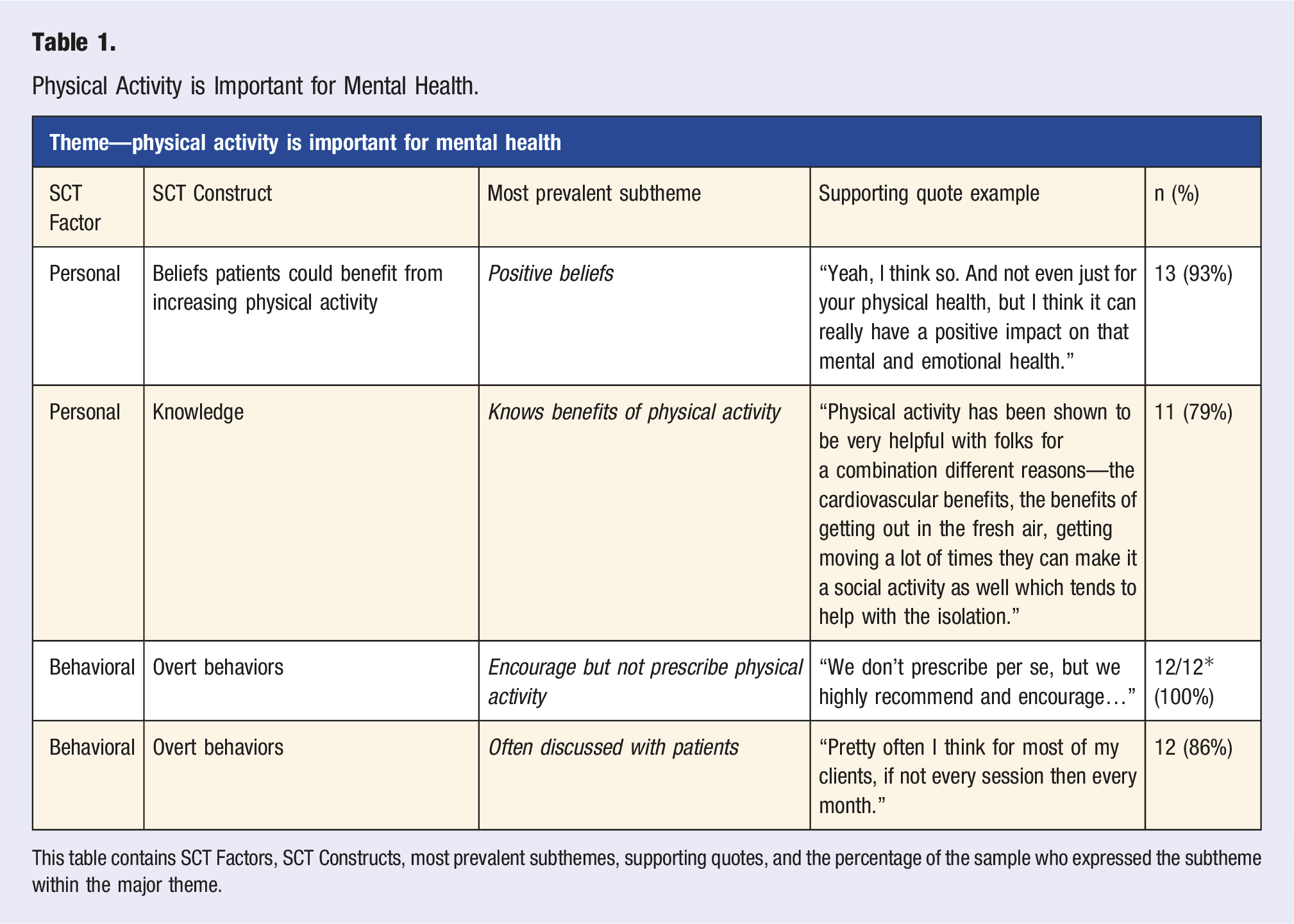
This table contains SCT Factors, SCT Constructs, most prevalent subthemes, supporting quotes, and the percentage of the sample who expressed the subtheme within the major theme.
Theme 2—Clinicians Support Prescribing PA to Patients
Clinicians interviewed in this study expressed support for prescribing PA to patients. The majority of clinicians (64%) had a supportive attitude toward prescribing PA to patients. As C10 reported, “… My attitude is… We should all be doing [it]… We’re really ignoring an important piece of the puzzle for clients if we’re not prescribing. We’re looking at everything else but exercise. I see that as one of those basic self-care things that we all should be doing in some way for ourselves. So, I feel like it’s a necessity for therapists to be including that.”
Outcome expectations of clinicians without having the proper training to prescribe PA reported patients would attempt the PA prescription, demonstrating the perception that patients trust their clinician's advice. C3 iterated, “I definitely think some of them would follow through. You do have to kind of be careful because some of them will do anything you tell them.” An outcome expectation of clinicians prescribing PA to patients after being adequately trained included increased confidence in the clinician. C7 expressed, “If I was properly trained and I have a license to back up my ability to ‘prescribe PA’, then I would feel much more confident.” An outcome expectation the clinician expressed was that if all clinicians across the US were prescribing PA to patients, PA would increase. C5 stated, “Whereas if we’re properly trained, and we’re bringing it up in conversation—whether people do it or not—talking about it more would yield more results in that area [increasing physical activity].” All clinicians (100%) expressed a high sense of locus of control, demonstrating autonomy in their practices to treat patients how they see fit within their scope of practice. C9 reported, “Every counselor does. It’s up to us, it’s up to me. I am the expert with my client.” All clinicians expressed being encouraging but not prescribing PA to patients.
Theme 3—Barriers to Clinicians Prescribing PA
Clinicians Support Prescribing Physical Activity to Patients and Barriers to Prescribing Physical Activity. This Table Contains SCT Factors, SCT Constructs, Most Prevalent Subthemes, Supporting Quotes, and the Percentage of the Sample who Expressed the Subtheme Within these Major Themes.
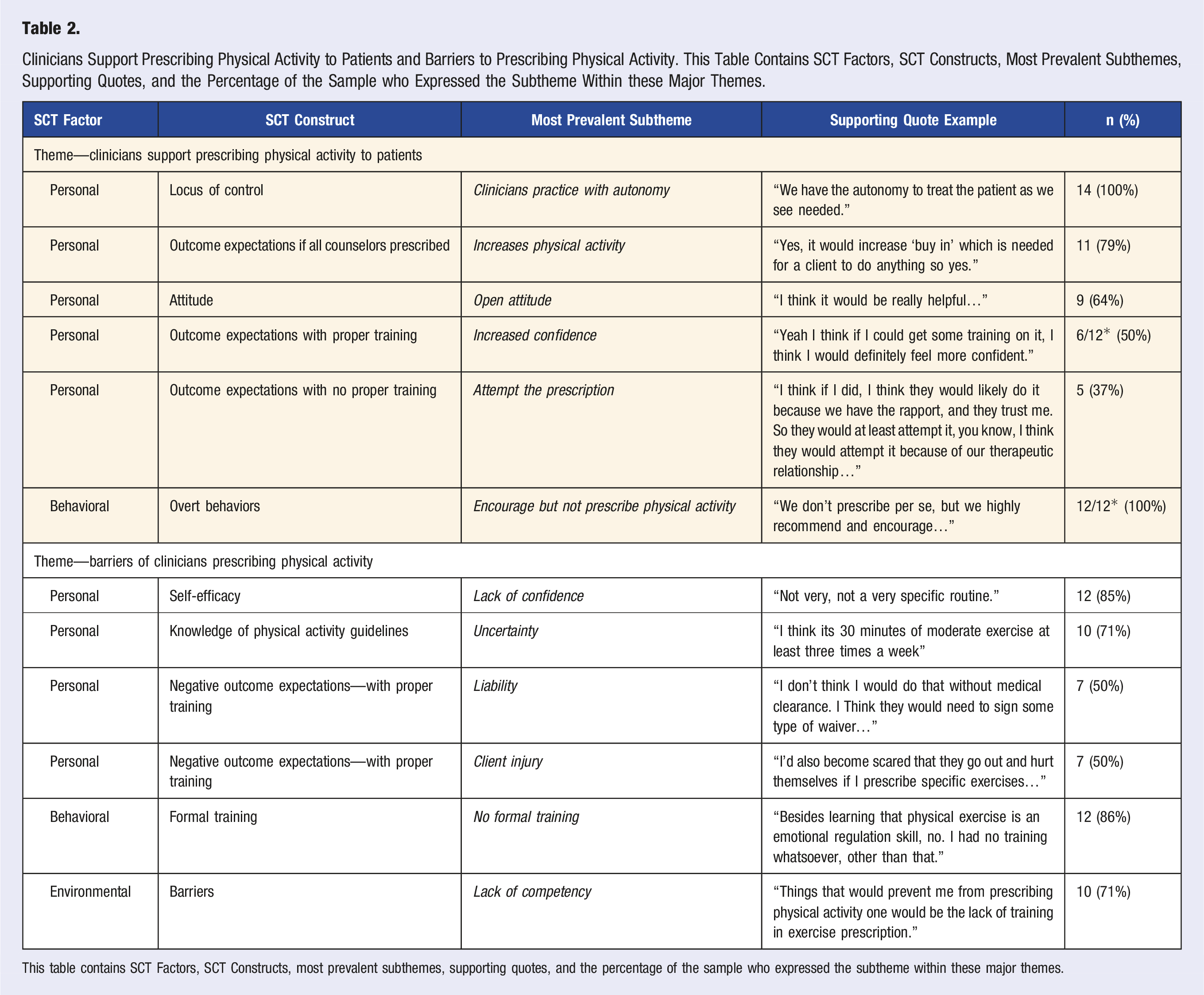
This table contains SCT Factors, SCT Constructs, most prevalent subthemes, supporting quotes, and the percentage of the sample who expressed the subtheme within these major themes.
Clinicians reported a lack of self-efficacy in prescribing PA to patients. C7 responded, “A specific physical [activity] routine, not very confident just because, again, I am not trained in that. That is not what I’m here for. But I do always strongly encourage exercise.” Notably, the majority of clinicians (71%) were uncertain of the PA guidelines and felt they lacked the competency to prescribe PA to patients. C3 stated, “I don’t. I am aware that something like that does exist, but I’m not super aware of what it is.” C6 mentioned, “I would think the only barrier would be just my competency. Like I said, it’s not something that I feel that I could do that I have a breadth of understanding.” Most clinicians (86%) noted they had received no formal training in prescribing PA to their patients in their graduate programs or continued education. C3 said, “Zero. It was just not brought up, you know it was just a general sense that ‘Hey, this is a good thing’. but more than that, not really.”
Theme 4—Clinicians Support Referring Patients to a PA Specialist
Clinicians expressed support for referring patients to a PA specialist. Almost all clinicians (92%) expressed a supportive attitude to referring patients to a PA specialist. C1 expressed, “I think I’d be open to that, especially if I was able to learn more of what that person does or what the specialist would recommend. And again, maybe, just like ideas of what their treatment plans or whatever they might call it, so that I have a better understanding of what that person might recommend to the client.”
Clinicians perceived that referring to a PA specialist would help increase the PA of patients. Clinicians perceived that if all clinicians across the US referred patients to a PA specialist, then the PA of patients would also increase. C11 stated, “I think it could. I think if the students are motivated, it has potential to help them increase their [physical] activity.” The clinicians felt their mental health clinic would be open to working with a PA specialist expressing institutional support. C4 responded, “I see the openness being there. Yeah, just because we do know that physical health is really important to all of the areas of wellness. We use a public health model here, and so physical wellness is a significant part of that public health model.”
The clinicians reported knowledge of resources to recommend to patients to help increase PA, which included the campus recreation center. All clinicians (100%) expressed high self-efficacy in being able to make a referral. C7 reported, “I’ve done it, so pretty confident.” Again, all clinicians (100%) felt autonomy in their practices to treat a patient how they see fit within their scope of practice. Clinicians believe referring to a PA specialist is the most feasible behavior compared to clinicians prescribing PA or a hybrid model of both behaviors. C9 expressed, “I will say referring someone out to a third-party specialist because it’s just not my area of training and expertise. It's outside the scope of my training.” Most clinicians (86%) reported making referrals in the past. C6 confirmed, “I think so…. When we think about third party people, we collaborate with people on the campus all the time.”
Theme 5—Barriers to Clinicians Referring to a PA Specialist
Clinicians Support Referring to a Physical Activity Specialist and Barriers Referring to Physical Activity Specialist.
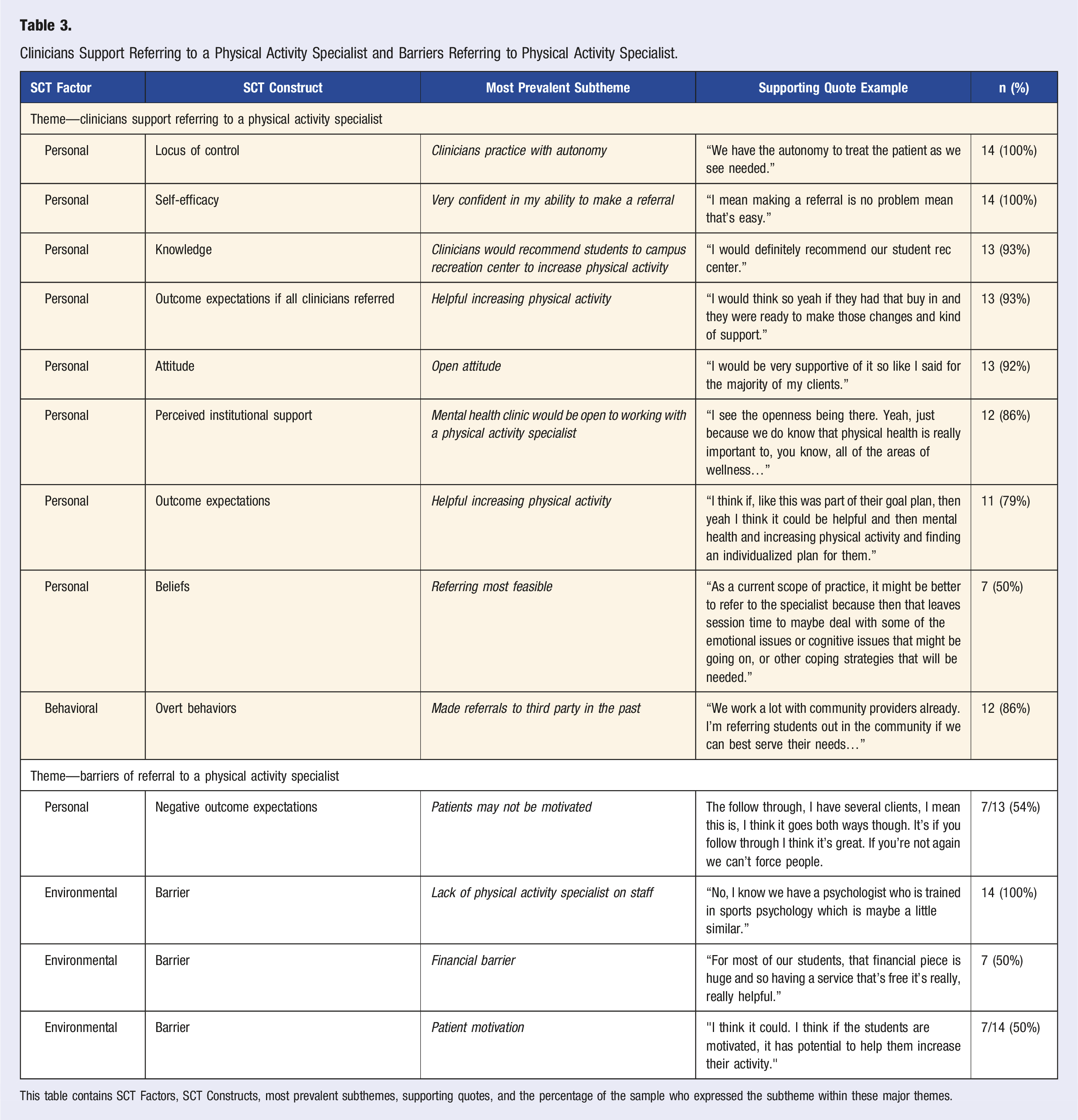
This table contains SCT Factors, SCT Constructs, most prevalent subthemes, supporting quotes, and the percentage of the sample who expressed the subtheme within these major themes.
Clinicians reported a financial barrier for patients or the university to fund a PA specialist. C10 expressed, “And I guess to the other piece might be financial I haven’t talked about that too much, but yeah just financially. You know, one of the benefits of having someone in-house at the university is that a lot of our services are covered, or at least partially covered, so if it was someone in the community, it might be a little more challenging if there wasn’t an affordable place for that person to go.”
Another barrier included the lack of a PA specialist on staff within the counseling center. C9 stated, “You know what, no. No, I don't know anybody.”
Discussion
Overall, this study identified specific personal, environmental, and behavioral factors that may influence the incorporation of PA counseling and referral for mental healthcare professionals in a university setting. The findings of these interviews show that most clinicians expressed that PA is important for the treatment of the mental health needs of their patients. Clinicians had supportive attitudes and presented specific barriers to prescribing PA to patients and referring patients to a PA specialist. The clinicians expressed that PA is important for mental health and recognize the wide range of PA benefits, including physical, mental, and emotional health. Therefore, the clinicians mention discussing PA frequently in sessions with patients and offer general encouragement but not a specific exercise prescription for PA. This finding is similar to a study in the UK, where most clinicians in the sample felt PA or exercise was important and would generally encourage exercise but not provide a prescription. In primary healthcare, a systematic review investigated the effectiveness of PA promotion through advising and counseling participants on multiple occasions, demonstrating that self-reported PA measures increased after 12 months of follow-up. 43 This supports general encouragement of PA can be effective, but within the interventions, variability existed in giving individualized PA advice, general recommendations based on guidelines, and general encouragement of PA. Recent evidence suggests that written prescriptions for exercise are more effective than standard PA counseling in primary health care. 44 The current practice of mental health professionals offering general or vague encouragement of PA may not be the most effective therapeutic practice to increase the PA of mental health patients.
Mental health professionals supported the idea of prescribing PA to patients. However, a lack of perceived competency in prescribing PA, low self-efficacy in prescribing PA to patients, and fears of client injury and subsequent injury liability (all personal factors of SCT 30 ) stop clinicians from prescribing PA. The clinicians’ knowledge of the PA guidelines was comparable to the general American population, as only 33% of Americans knew the dose recommendations for PA, 45 and 29% (n = 4/14) of the counselors in the current study could recite the guidelines. This lack of PA knowledge is similar to other health care providers. A study noted that a lack of organized education in PA counseling and lifestyle medicine during residency training is a barrier to PA counseling from physicians. 46 Other previously reported barriers included a lack of knowledge on creating individualized plans to meet PA guidelines and overcoming barriers patients face. 47 Another potential barrier that was not assessed includes the PA level of each clinician. A systematic review demonstrated a positive relationship between physicians and healthcare providers' PA levels with PA counseling. 48 One study showed that 46% of healthcare providers do not meet the recommended physical activity guidelines. 49 Future studies should investigate mental health clinicians’ PA levels and how frequently they utilize PA counseling or encouragement during visits. Helping inactive mental health clinicians increase their PA may help them promote PA to patients. Despite recognizing the importance of PA, many mental health clinicians are not receiving formal education about PA, and they may not be physically active themselves. Thus, they lack specific confidence to prescribe PA to patients. However, perceptions, confidence, and knowledge are all modifiable personal factors.
Formally educating mental health professionals on PA, including the benefits, modalities, prescription, and ethics of PA may be the best strategy to overcome the mentioned barriers. Training is a critical strategy to enhance intervention uptake and implementation. 50 As clinicians must obtain continuing education credits to renew their licenses, developing an approved continued education training could help increase the available capacity of PA for counselors. Evidence-based training or education strategies such as Interactive Learning Education, 51 Audit and Feedback, 50 Collective Efficacy, 52 and Discussion and Application 50 can increase PA capacity. 53 Training can increase clinicians’ self-efficacy to prescribe PA. Although the barrier of liability and client injury remains, prescribing PA may be comparable to prescribing medication. For example, as a medical doctor does not act outside of negligence or unethically, doctors are not held liable for the patient’s mishandling of medical prescriptions. Appropriately trained mental health clinicians may not be responsible for client injury. Regardless, mental health care professionals promoting the National Physical Activity Guidelines to patients may be more effective than general encouragement and more feasible than becoming certified to provide PA prescriptions for now. Clinicians iterating specific benefits of PA, adequate dosages and intensities of PA, and encouraging different modalities to achieve the National Physical Activity guidelines may be more likely to get patients to increase PA levels.
Overcoming barriers to PA prescription, such as lack of PA education and liability concerns, may be focal longer-term strategies for incorporating PA into mental health care practice. More clinicians reported positive factors when referring patients to PA specialists. Thus, the referral-based approach may provide a more effective immediate solution to incorporating PA into practice. A certified professional (accredited strength and conditioning coaches, personal trainers, etc.) who understands the benefits of PA and exercise and who can prescribe individually tailored PA programs to students was the definition of a PA specialist. University counseling centers may address these barriers by designing and implementing an ERS. An ERS has been recognized as one of the four most common methods to increase poor PA. 54 As mental health counselors lack PA knowledge to prescribe PA, an ERS may help overcome barriers in incorporating PA into therapeutic works. ERS typically involves a health professional determining a patient to be physically inactive, referring the patient to a PA specialist, and then consulting with the patient about increasing PA. 54 Despite its effectiveness in increasing PA,55-57 few ERS have attempted to improve PA and mental health outcomes for patients seeking mental health treatment.58,59 In mental health treatment, one study found that increased self-reported PA was sustained after a year but the ERS did not improve depression outcomes or decrease the use of antidepressants. 58 Another study found lower levels of anxiety/depression in the intervention group but no effect on self-reported PA. 59 EIM-OC promotes developing ERS on university campuses. Although, few studies have published on ERS in primary student healthcare on university campuses through EIM-OC. Studies that did utilize ERS through EIM-OC had primary care physicians refer students to physical activity specialists within the campus and showed an increase in PA26,27 and exercise self-efficacy.26,28 These studies have been limited by small sample sizes and self-reported PA measures. In the current study, none of the clinicians have been involved with an ERS or mentioned EIM-OC. Mental health professionals could be novel health care providers to refer to an ERS scheme on university campuses and could be key stakeholders for EIM-OC. However, there is no current literature on the implementation or effectiveness of an ERS within a university counseling center utilizing EIM-OC, and previous findings from an ERS in mental health treatment are unclear, necessitating further investigation of ERS implementation. In following the ORBIT Model for Behavioral Treatment Design, 34 a future study will address the barriers clinicians faced when referring to a physical activity specialist and continue the design and piloting of a feasible ERS within a university counseling center through EIM-OC.
Limitations
One limitation of the study includes using a convenience sample, limiting the transferability of findings to other samples, including clinicians who serve non-university populations or mental health professionals not located in the southern US. Self-identified females made up nearly the entire sample (85%). This percentage is just slightly higher than a national estimate of mental health therapists, where 71% are estimated to be women. 60 Also, only people actively counseling at large southern universities participated in the study. Therefore, clinicians from smaller universities with fewer resources may not share similar perceptions of benefits and barriers to prescribing and referrals for PA. This inclusion criterion increased internal validity by having a more homogenous sample. Next, the lack of direct observation of participants with patients is also a limitation. For example, the researchers never observed clinicians during appointments, so it was unclear how clinicians included PA in their therapeutic works in actual appointments. However, clinicians were encouraged to be transparent and honest with each question. Finally, with qualitative research, themes can be influenced by a researcher’s bias and experiences. Therefore, necessary trustworthiness methods (e.g., bracketing journal, member checks, and auditing) attempted to limit biases.
Conclusion
Overall, the study explored personal, environmental, and behavioral factors influencing university mental health clinicians' inclusion of PA into therapeutic work, prescribing PA to patients, and referring patients to a PA specialist. Clinicians agreed that PA was important for mental health but lacked knowledge on PA. Formally educating mental health clinicians on PA, including the benefits, modalities, prescription, and ethics of PA may help clinicians prescribe PA. Training options could include workshops from exercise scientists or an EIM-OC leadership team on their respective campus. Mental health clinicians also expressed that referring to a PA specialist would be the most feasible strategy to incorporate PA as part of their therapeutic work for patients struggling with physical inactivity and mental health. This finding highlights the openness to developing an ERS for assisting clinicians in implementing PA in their therapeutic works. EIM-OC can be a helpful resource for developing an ERS on a college campus. Future studies are necessary to investigate the implementation or reach of an ERS within a college counseling center and the effects an ERS can have on the mental health and PA of college students seeking mental health treatment. Physical inactivity15,16,19,20 and poor mental health 1 are highly prevalent on university campuses. Incorporating PA in the therapeutic works of mental health professionals may be a critical strategy for a university to promote PA and the mental health of a vulnerable population.
Footnotes
Acknowledgments
We, the authors, would like to thank the participants for their time and efforts. We also like to thank Nicole Doyle, Ph.D., for her time and efforts as the external auditor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.